
Abstract
Purpose:
The aim of the study was to retrospectively evaluate the potential benefit on survival outcomes of selective intraarterial radionuclide therapy (SIRT) with Yttrium-90 microspheres as a salvage therapy in liver metastasis of different tumors.
Material and Methods:
Sixty-one patients who had unresectable liver metastases from colorectal carcinoma (n=23), neuroendocrine tumor (NET; n=12), cholangiocarcinoma (n=9), and others (n=17) received yttrium-90 microspheres. All patients were treated in a salvage setting with an 11-month mean follow-up. Early metabolic treatment response was evaluated by 18F-Fluorodeoxyglucose positron emission tomography (FDG PET-CT) in the sixth week after treatment.
Results:
Of the 61 patients, 32 were alive at the end of the study; median overall survival (OS) was 17.0±2.5 months (95% confidence interval: 11.9–22.0). A subset analysis of colorectal and noncolorectal groups demonstrated median OS rates of 14.0±5.8 and 17.0±4.8 months, respectively (p=0.543). The mean OS for patients with NET and cholangiocarcinoma was 29.0±3.1 months and 17.7±3.2 months, respectively (p=0.010). According to the early metabolic treatment response, the mean OS of responder and nonresponder groups was 32.0±5.6 months and 11.4±2.1 months, respectively (p=0.054). Eastern Cooperative Oncology Group performance status <1 (p=0.018) and chemotherapy-naive patients (p=0.008) showed significant correlation with survival.
Conclusion:
SIRT is an effective treatment option for patients with metastatic liver disease in a salvage setting with acceptable toxicity.
Introduction
Metastatic disease to the liver is the most common location for solid organ metastasis. Liver failure secondary to hepatic tumor burden is major cause of death in patients with cancer. Primary malignancies that commonly metastasize to the liver include gastrointestinal, breast, neuroendocrine, pancreas, stomach, and melanoma. For patients who present with metastatic liver disease, the prognosis is poor, except for a minority who are eligible for curative resection. 1 Liver directed local therapeutic options are available in clinical practice for palliative care, including transarterial chemoembolization (TACE), embolization, and radiofrequency ablation (RF), which have enabled significant improvements in patient survival. Unfortunately, these treatments are restricted to a limited number of patients, as they depend on the size, number and site of the liver tumor. Therefore, advances are ongoing in the development of new therapeutic options to ameliorate the survival of those patients who have disseminated metastases and remain unsuitable for alternative therapies.
Selective intraarterial radionuclide therapy, also known as radioembolization, with Yttrium-90 microspheres has been recognized as a promising therapeutic option for patients in salvage settings. The efficacy of SIRT for the treatment of metastatic disease to the liver has been evaluated most extensively in colorectal cancer and revealed encouraging outcomes. 2 –6 Recent findings suggest that selected patients with other malignant processes may benefit as well, but conclusive evidence is limited. 7–8
A retrospective study was conducted to evaluate the efficacy of SIRT in the salvage treatment of unresectable metastatic liver disease.
Materials and Methods
Patients
This study was a single-institution retrospective analysis of patients with liver metastases from various primary malignancies treated by SIRT. Consent of the local ethics committee was obtained before the retrospective collection of all data. Between September 2008 and June 2012, 61 patients with unresectable liver metastases from various primary malignancies [colorectal carcinoma (CRC) (n=23), neuroendocrine tumor (NET; n=12), intrahepatic cholangiocarcinoma (ICC; n=9), pancreatic adenocarcinoma (n=3), gastric adenocarcinoma (n=3), breast cancer (n=2), leiomyosarcoma (n=1), malign melanoma (n=1), bladder cancer (n=1), nasopharynx cancer (n=1), primary unknown (n=5)] were treated at our institution. The median age of the patients was 59 years, and there were 36 men and 25 women.
The indication for Y-90 microsphere treatment was driven by an institutional board of specialists that included oncologists, hepatologists, surgeons, interventional radiologists, and nuclear medicine physicians. The therapy indications were as follows: (1) chemorefractory or progressive liver-dominant metastases; (2) nonsurgical candidates; (3) not considered suitable for alternative transarterial therapies; (4) not greater than 70% hepatic parenchymal involvement; (5) Eastern Cooperative Oncology Group (ECOG) performance status of 0–2; (6) noncompromised pulmonary function; (7) the ability to undergo angiography and selective visceral catheterization; (8) adequate hematologic parameters (granulocyte count ≥1.5×109/L, platelets ≥50×109/L), and renal function (creatinine level ≤2.0 mg/dL; (9) adequate liver function (bilirubin level ≤2.0 mg/dL, albumin level ≥3 mg/dL, INR ≥1.2, aspartate transaminase, alanine transaminase, and alkaline phosphatase levels less than five times the normal upper limit); and (10) limited extrahepatic disease.
Baseline imaging studies (CT or MR and FDG PET/CT imaging) were obtained and evaluated for the percentage of tumor burden in the liver and presence of extrahepatic metastases. After being chosen as the candidate, pretreatment angiography was performed to evaluate anatomy and identify vessels that required intervention, such as embolization. At the end of the angiography, a 150 MBq dose of Tc99m-MAA was administered through the catheter in an attempt to detect extrahepatic shunts. Planar whole body and abdominal SPECT images were obtained with a dual head gamma camera (E.cam; Siemens Medical Solutions, Erlangen, Germany) and low-energy high-resolution collimators. Regions of interest were drawn around the liver and lungs in anterior and posterior planar images, and the pulmonary shunt was calculated. In an attempt to detect shunts from the hepatic arterial system to the gastrointestinal tract, Tc99m-MAA SPECT images were coregistered with the pretherapeutic CT images and evaluated by two experienced nuclear medicine specialists.
All of the patients provided written informed consent regarding the procedure and its associated risks.
Selective intraarterial radionuclide therapy
Depending upon the extent of tumor burden, patients received either segmental or lobar treatment. For bilobar treatment, the first lobe treatment was followed by the second lobe treatment approximately 4 to 6 weeks later. No whole liver infusions were performed. In this study, patients were treated by Y-90 resin-microspheres (SIRSpheres-Sirtex Medical Limited, Lane Cove, Australia) (in 50 patients) or Y-90 glass microspheres (Thera-Sphere, MDS Nordion, Ottawa, Canada) (in 11 patients). The activity was calculated as per the manufacturer's instructions.
PET/CT imaging
FDG PET/CT imaging was performed within 4 weeks before SIRT and 6 weeks after SIRT. The patients fasted for a minimum of 6 hours before imaging, and their blood glucose levels were less than 150 mg/dL at the time of the tracer injection. The patients received an intravenous injection of 370–550 MBq of 18F FDG, and then rested for approximately 60 minutes before undergoing imaging. First, low-dose CT was performed (140 kV and app. 50 mAs) without any specific breathholding instructions. The scanning from the top of the skull to the upper thighs was performed in a single step with the patient in a supine position on a 6-slice PET/CT (Biograph TruePoint, Siemens Medical Solutions). CT data were used for attenuation correction. The PET images were iteratively reconstructed with 5-mm thick slices (TrueX option, subsets=21, iterations=3). Immediately following the CT, a PET emission scan was acquired using the whole-body mode. Six to eight bed positions were used, with an acquisition time of 3 minutes for each bed position. The PET data were reconstructed using 3D PET reconstruction with a system matrix derived from point source measurements.
Evaluation of treatment response
Early metabolic treatment response was evaluated by FDG PET-CT in the sixth week after treatment in 47 patients. FDG PET-CT was not used in patients with neuroendocrine tumors and low FDG uptake for evaluation of treatment response. Additionally, 2 patients who had hepatic failure after therapy could not undergo the FDG PET-CT after treatment. To assess metabolic response using the FDG PET-CT images, we measured the maximum standardized uptake value, corrected for body weight (SUVmax) of the hepatic metastases. For this response assessment, we summed the SUVmax measurements of up to five of the most notable hepatic metastases and calculated the percentage change on the follow-up scan relative to the baseline measurements. Any decrease exceeding 25% of the summed baseline SUVmax was taken to indicate a therapy response (responder), whereas any lesser decrease or any increase in SUVmax or appearance of new hepatic lesions were considered as lack of response (nonresponder).
Statistical analysis
The Kaplan-Meier survival analyses using log-rank methods were used to estimate overall survival (OS) of the entire sample as well as to test differences in survival between groups. Mean and median survival was reported (with 95% confidence intervals). Covariate adjustment was performed via Cox regression modeling. Variables studied in the univariate analysis included gender, age (>65 and <65 years), tumor burden, presence of extrahepatic disease, prior liver-directed local therapy, chemotherapy or hepatic resection, ECOG performance status, hepatopulmonary shunt (>10% and <10%), pretherapy liver function tests and administered dose of Y-90 microspheres. Survival was calculated from the time of first SIRT to the time of death. All statistical analyses were performed using the IBM SPSS Statistics version 20.0 package (IBM Corporation, Somers, NY).
Results
Patients
Eleven patients had solitary tumors, while 50 had multifocal disease. Tumor volume was between 50% and 70% of liver volume in 19 patients, between 25% and 49% of liver volume in 33 patients and ≤24% of liver volume in 9 patients. The ECOG performance status was 0 in 41 patients (67%), 1 in 14 patients (23%), and 2 in 6 patients (10%). Of the 61 patients, 56 (92%) had previous treatments included systemic chemotherapy in 43 patients, surgery in 7 patients, TACE in 5 patients, and RF in 1 patient before SIRT.
The study population underwent a total of 66 treatments in which 49 patients received lobar (48 right lobar and 1 left lobar) treatment and 12 patients received bilobar treatments. The calculated mean percentage of hepatopulmonary shunting on 99mTc-MAA scans was 7.9%±5.6%. Thirteen patients had a reduction in the calculated dose due to over 10% lung shunting of the Y-90 microspheres. In 3 patients, the intended dose could not be completely administered because of intrahepatic arterial stasis. Therapeutic doses of these patients were recalculated after therapy (74% and 82% of the targeted activity) and used in the analysis. The mean dose administered was 2.0±0.9 GBq (range: 1.0–2.5 GBq).
Toxicity
The most common acute toxicity was fatigue (54%) followed by nonspecific self-limiting abdominal pain (32%), nausea (24%), vomiting (16%), and fever (3%). None of these symptoms lasted longer than 7 days. Four patients had grade 3 bilirubin toxicity. Two deaths were observed within 3 months following the procedure. The patients who had hepatic failure after therapy died 8 and 12 weeks after SIRT. These patients had multiple metastatic lesions in the liver and were treated in the initial stage of our experience. Since both patients' liver functions were in normal limits before therapy and they had progressive hepatic failure after therapy, it was thought that the hepatic failure was caused by radiation-induced liver disease. SIRT-induced gastric or duodenal ulcerations were not observed. This resulted in a 3% incidence of significant complications on a per-patient basis and a 3.3% incidence on a per-procedure basis.
Response
Early metabolic treatment response was evaluated by FDG PET-CT in the sixth week after treatment in 47 patients. According to early metabolic treatment responses, 29 patients were classified as responders and 18 patients as nonresponders. The mean pretreatment SUVmax values of responder and nonresponder groups were 16.15±10.12 and 10.3±10.6, respectively. The mean post-treatment SUVmax values of responder and nonresponder groups were 9.5±5.9 and 13.0±11.1, respectively.
Survival analysis
Mean clinical follow-up was 11 months (range: 2–48 months). Of the 61 patients, 32 (52%) were alive at the end of the study. Thirty-one of the 61 patients (51%) eventually had progression of the disease. Seven patients had only extrahepatic progression, while the remainder had intrahepatic progression with (n=17) or without (n=7) extrahepatic disease. Among these, 29 patients died and 2 patients were still alive at the end of the study.
The median survival for all patients groups was 17.0±2.5 months (95% confidence interval: 11.9–22.0) (Fig. 1). A subset analysis of CRC and non-CRC groups demonstrated median survival rates of 14.0±5.8 months and 17.0±4.8 months, respectively (log rank test, p=0.543). Median OS was not reached for patients with NET and ICC; the mean OS was 29.0±3.1 months and 17.7±3.2 months, respectively (Figs. 2 and 3). According to the early metabolic treatment response, the median OS was not reached for the responder group and the mean OS was 32.0±5.6 months. The median and mean OS of the nonresponder group were 9.0±1.9 months and 11.4±2.1 months, respectively (p=0.054) (Figs. 4 and 5).
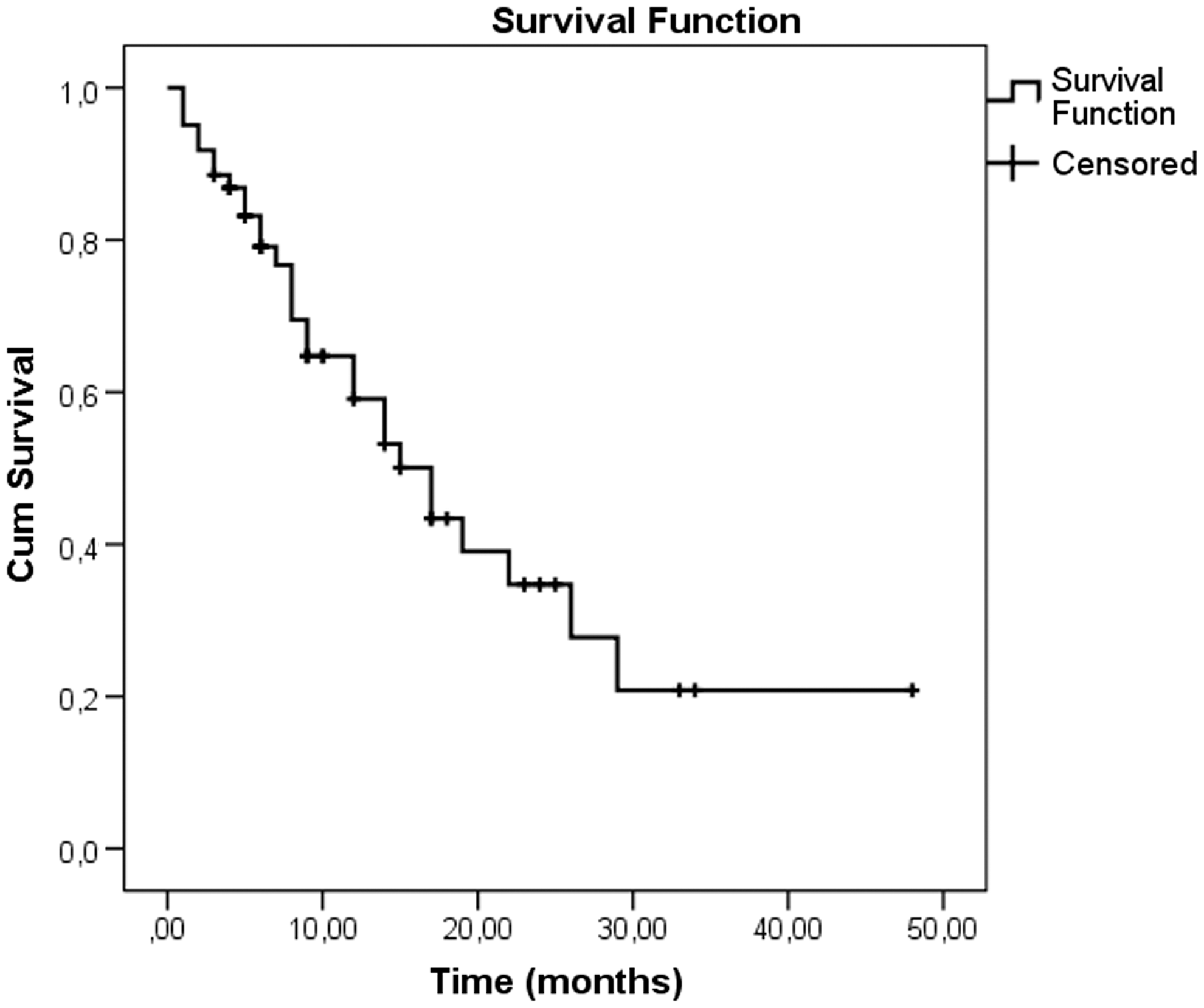
Median overall survival (OS) of all patients treated using the Kaplan-Meier method. Median survival for this cohort was 17.0±2.5 months (95% confidence interval: 11.9–22.0) from the date of SIRT.

Survival of patients according to primary malignancy. Median survival for patients with colorectal carcinoma (CRC) was 14.0±5.8 months. Median OS was not reached for patients with neuroendocrine tumor and intrahepatic cholangiocarcinoma (ICC). The mean OS was 29.0±3.1 months and 17.7±3.2 months, respectively.
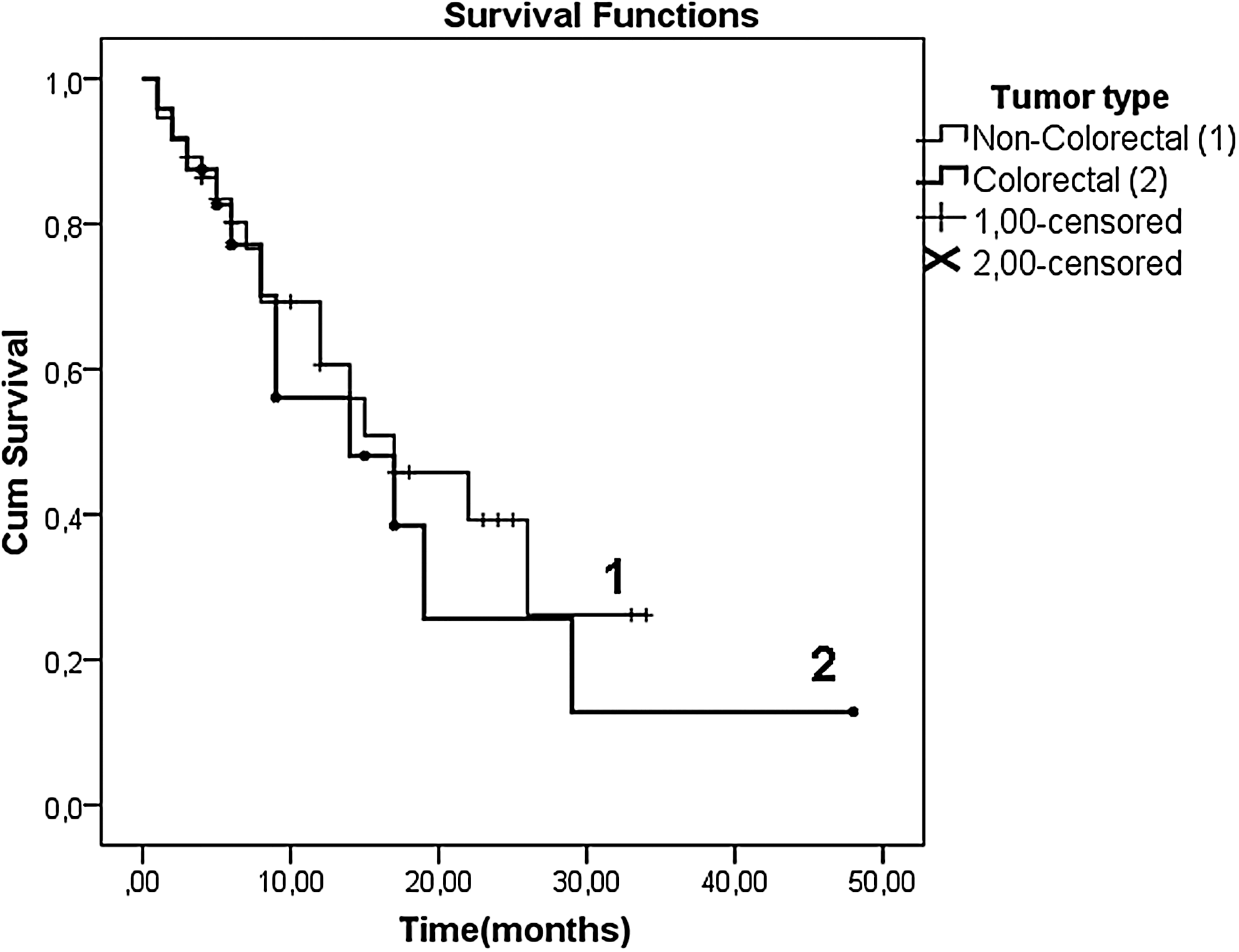
Median OS for patients with CRC or non-CRC primary. Median survival for patients with CRC was 14.0±5.8 months versus 17.0±4.8 months for patients with non-CRC (p=0.543).
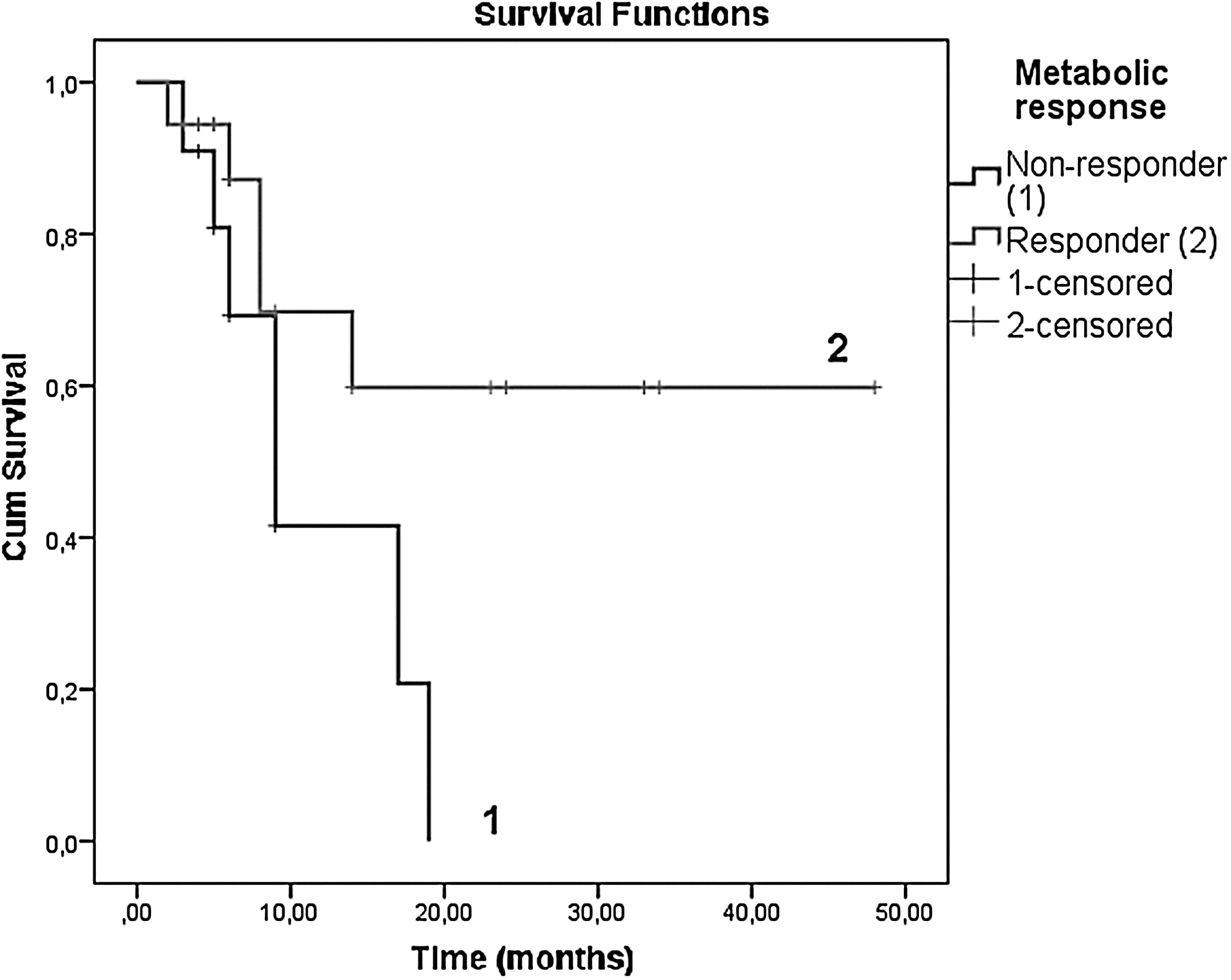
The Kaplan-Meier survival curves as a function of FDG-PET-CT metabolic response. Responders had a significantly (p=0.054) longer survival than nonresponders.

Coronal slices of a pretherapeutic fused
Age, gender, tumor burden, extrahepatic metastases, hepatopulmonary shunt, surgical resection, or local liver directed therapies before SIRT, pretherapy liver function tests, and administirated dose showed no significant correlation with survival according to the Cox proportional hazard model. Univariate analysis identified two significant prognostic variables associated with an improved OS: ECOG performance status <1 (p=0.018) and chemotherapy-naive patients (p=0.008) showed significant correlation with survival. Table 1 demonstrates the significance of clinic and treatment related prognostic factors for OS.
Discussion
Clinical studies have shown significant improvement in outcomes with the use of SIRT for hepatic metastases in the salvage setting, as demonstrated by the increased survival times for a substantial proportion of patients. 2 –8 In line with these studies, the present retrospective analysis revealed that SIRT which enabled a significant median OS of 17.0 months with acceptable toxicity profile is an effective salvage therapy option in metastatic liver disease. While multiple types of primary tumors were present in our analysis, CRC represented the largest number of primary tumors. We have found median survival of 14 months with SIRT as a second or subsequent line of therapy in unresectable, chemorefractory CRC liver metastases. The median survival is similar to that previously reported by others. 2 –5 In concordance with our findings, Nace et al. reported a mean survival of 14.4 months after failure of all current chemotherapeutic regimens in a cohort of patients consisting of CRC liver metastases. 3 Sato et al. also reported a median survival of 15.2 months in their subgroup analysis of 51 patients with chemorefractory CRC liver metastases. 4 Most of the published data on salvage SIRT in CRC has been generated from retrospective or single-center studies. 2 –8 Cosimelli et al. reported first prospective evaluation of SIRT of patients with CRC liver metastases who failed previous oxaliplatin and irinotecan based on systemic chemotherapy regimens. 9 The median survival in this multicenter Phase II clinical trial was 12.6 months with SIRT, which is consistent with our findings. Numerous studies have also reported cases of patients with unresectable liver metastasis refractory to chemotherapy that was downstaged to allow resectability after SIRT, which resulted in prolonged survival. 10 –12 Although these encouraging results suggest that SIRT may offer a real clinical benefit to this population with dismal prognoses, questions remain regarding its use earlier in the course of the disease. Randomized controlled trials in which SIRT has been combined with systemic chemotherapy or hepatic arterial infusion for the first or second-line treatment of CRC liver metastases have been published. These studies generally show an improvement in OS compared with salvage patients; the reported survival times range from 10.5 months to 29.4 months. 13 –17 However, results from the ongoing Phase III trials are needed before this treatment can be recommended more widely as a first-line treatment for CRC liver metastases.
In this study, the difference between median OS times for colorectal and noncolorectal group (14 months vs. 17 months) is not significant (p=0543). This finding may suggest that selected patients with various primary malignancies may benefit from SIRT in salvage settings as well. Not surprisingly, one of the subgroup's most favorable survival (mean: 22 months) is found in patients with NET, likely because patients with NET have a much better prognosis. In line with our findings, Rhee et al. observed that 92% and 94% of patients treated with glass and resin microspheres, respectively showed either a partial response or stable disease at six months, and the median survival was 22 and 28 months, respectively. 18 King et al. reported the mean survival time of 27.6 months in 34 patients treated with resin based microspheres. 19 Furthermore, Kennedy et al. reported a retrospective review of 148 patients with hepatic metastases of NET. The median survival was 70 months, and the authors stated that one of the largest benefits of this treatment is the stabilization of extensive disease allowing for longer survival periods. 20 This promising finding suggests that SIRT has the potential to be a promising new tool in the management of patients with unresectable hepatic metastasis of NETs.
While ICC is primary liver cancer, its clinical management is similar to metastatic liver tumors rather than primary. There is no recognized standard palliative treatment for advanced or metastatic ICC and long-term survival is poor. Therefore, nine cases were included with ICC to our retrospective analysis, and we found a mean of 11.4 months of OS. Preliminary studies have shown similar responses of ICC to SIRT. 21 –24 This outcome is also comparable to the results of the first randomized Phase III clinical trial with current standard chemotherapy regimen consisting of cisplatin and gemcitabine (median survival was 11.7 months). 25 Furthermore, most patients (98%) in this large cohort were chemotherapy naive, whereas our small patient series consisted of chemorefractory liver metastasis from ICC. In line with our findings, Hoffmann et al. reported a longer survival in the chemotherapy naive subgroup (14.2 months) than in the group of patients previously treated with chemotherapy (11 months) in 33 patients with unresectable ICC. 24
It is of critical importance in the planning of SIRT to identify those patients likely to have a less favorable outcome. By so doing it is possible to avoid treating patients with an expensive therapy that carries with it the potential risk of harm. Our study identified two factors associated with increased survival. First, patients with an excellent performance status (ECOG performance status 0) had a significantly better prognosis than patients with an impaired performance status, depending upon whether they had an ECOG 1 or ECOG 2 performance status. This result correlates positively with the results published by Dunfee et al., which reported that compromised performance status is the most powerful negative prognostic factor in the population with liver malignancies. 26 Second, the results of the present study suggest a longer survival in the chemotherapy naive subgroup than in the group of patients previously treated with chemotherapy (p=008). This finding is confirmed by previous studies, in which chemotherapy-naive patients with various primary malignancies survived significantly longer after SIRT than patients previously treated with chemotherapy. 7,22 –24
While the current standard for assessment of response to therapy in solid tumors, the RECIST, requires a response to be assessed by using cross-sectional imaging, we used FDG PET-CT for evaluating early metabolic response. This was because of the published data which supports the inadequacy of RECIST to accurately assess early responses in this setting. 6 18F-FDG PET has shown promising results in assessing early response to therapy and survival outcome. 18,27 –29 Our data indicate that patients who had early metabolic treatment response had an improved prognosis (p=0.054). Similar findings were reported by Kucuk et al. in 124 patients with various primary tumors. 30 The mean OS time of responder and nonresponder groups was 25.63 months and 20.45 months, respectively (p=0.04).
Even though SIRT is restricted to intrahepatic tumors, we did not observe that the occurrence of limited extrahepatic metastases worsened survival. Rafi et al. reported similar findings in an ICC group consisting of those who were at risk of a shorter survival. 31 In contrast to our findings, there are numerous studies which reported that the presence of extrahepatic disease resulted in shorter OS. 6,31 Nace et al. reported that the absence of extrahepatic disease at the time of treatment with SIRT was associated with an improved survival, compared to those with extrahepatic disease at the time of treatment with SIRT (median survival: 17.0 months vs. 6.7 months). 3 According to clinical experience, there is a trend toward a poorer prognosis in patient with extrahepatic metastasis. On the contrary, patients with NETs classically have prolonged survival rates despite significant extrahepatic disease. Therefore, it is important to note that patients with limited extrahepatic metastases cannot be excluded when hepatic metastases was deemed to be the predominant and life-limiting disease.
Other factors included in our univariate analysis, such as age, gender, tumor burden, hepatopulmonary shunt, surgical resection, or local liver directed therapies before SIRT, pretherapy liver function tests and administrated dosages did not have an impact on patient outcome. Overall data available to date are conflicting and in contrast to our findings. Numerous published studies have found a significant correlation among many of these factors and patient outcomes after SIRT. 4,21 One explanation for this could be that the different results of studies may reflect the differences in the studied patient population. A relatively small number of patients and a heterogeneous patient group did not allow for a strict conclusion regarding which of the potential risk factors are independent predictors of less favorable outcomes. However, it can be argued that further investigations to optimize patient treatment strategies and treatment selection are needed.
Toxicities were consistent with previously published data and were generally mild, easily managed with supportive care and reversible. radiation was generally well tolerated, with a low incidence (3%) of radiation-induced liver disease. 7,13,16 –18 The incidence of radiation-induced liver disease increases with age, whole liver treatment, and increased baseline bilirubin levels. 32,33
The present study has several limitations, including the small patient population studied, its nonrandomized nature and its retrospective construct. Due to this retrospective nature, we could not assess progression free survival of patients. The treatment cohort was also a heterogeneous population, which limits the ability to generalize the findings. Despite these limitations, the results of the present study support that the use of SIRT provides therapeutic benefits in the salvage setting for metastatic liver disease.
Conclusion
These initial results indicated that SIRT in salvage patient population suffering from hepatic metastasis was found to provide a satisfactory OS, while having an acceptable toxicity rate.
Footnotes
Disclosure Statement
The authors declare that they have no conflicts of interest.