
Abstract
Background:
The addition of bevacizumab (BEV) to cytotoxic chemotherapy regimens (CTX) was believed to be effective; however, its magnitude of benefits is still controversial. So a meta-analysis and systematic review seems to be necessary.
Methods:
PubMed and the Cochrane library were systematically searched. All relevant citations comparing CTX with/without BEV were considered for inclusion. Sensitivity and meta-regression analysis were performed to identify potential confounders. All pooled estimates were performed using a random-effects model. All statistical analyses were performed by StataSE 12.0.
Results:
The search strategy identified 10 eligible random control trials (RCTs) (n=1366). In our pooled estimates, the additional benefits of BEV to CTX were identified in overall survival (OS) hazard ratio (HR, 0.76; 95% CI, 0.69 to 0.82) and progression-free survival (PFS) (HR, 0.56; 95% CI, 0.51 to 0.60), and prolonged survival duration were also identified for OS (18.2 vs. 16.3, p=0.0003) and PFS (8.9 vs. 6.5, p<0.001). Subgroup analyses stratified by CTX was also performed, evident benefits of additional BEV in OS and PFS can be identified in all subgroups, except for the CTX containing capecitabine in OS. Moreover, the increased rate of incidence was also identified in hypertension, thrombosis, proteinuria, gastrointestinal perforation, and fatigue.
Conclusion:
BEV, acting as a targeted agent to CTX, its additional benefit to CTX is at the cost of increased toxicity.
Introduction
Colorectal cancer (CRC) is the third common and fourth leading cause of deaths among cancer sufferers throughout the world. 1 Since intravenous Fluoropyrimidine therapy was first found to be efficacious for the treatment of metastatic CRC (mCRC), two other cytotoxic drugs (Irinotecan [IRI] and Oxaliplatin [OXA]) and targeted monoclonal antibodies (Bevacizumab (BEV), Cetuximab, and Panitumumab) had been gradually discovered over the last decades. 2 OXA-based chemotherapy and 5-fluorouracil (FLU) plus Leucovorin (LEU, also known as folinic acid, acting as a biochemical modulator of FLU) based chemotherapy have become the standard treatment for mCRC. 3 –5 Moreover, Capecitabine (CAP) is an oral Fluoropyrimidine that has similar efficacy with the combination of FLU and LEU in the first-line treatment for mCRC. 6 –8
Acting as a humanized variant of anti-VEGF monoclonal antibody, BEV has been evaluated as an antiangiogenic cancer therapy in many tumor types. 9 The primary mechanism of BEV is the inhibition of tumor growth rather than cytoreduction. 10 It has antiangiogenic effect which could decrease local vascular density, and finally reduces the blood supply which is critical to the rapid growth of transplanted tumors. 11 However, in addition to its direct antiangiogenic effect, BEV may also alter tumor vasculature and decrease the elevated interstitial pressure in tumor, such improves the delivery of chemotherapy. 10,12,13 Additionally, BEV is well tolerated as a single agent, and also in combination with chemotherapy, 10,14 but it does not have significant activity as monotherapy. 15
However, with the gradually updating evaluation performed, the magnitude of additional benefits derived from BEV is still controversial. The present meta-analysis and systematic review has been performed with the purpose of assessing the feasibility and safety of BEV when adding to cytotoxic chemotherapy regimens (CTX) in the treatment of CRC.
Methods
Selection criteria
Studies were potentially eligible for inclusion in this meta-analysis if they involved a randomize comparison of CTX with/without additional targeted agent-BEV in the treatment of CRC patients (age >18), and CTX in both compared groups should not be confounded by additional chemotherapeutic, adjuvant agents or interventions. Prior surgical cancer therapy was permitted. Exclusions were considered if: abstract reports of RCTs presenting preliminary or interim data only, results of RCTs were reported in letter or editorials. Other reasons for exclusion were illustrated in Figure 1. Major selective criteria of patients, and details of chemotherapy regimens for each trial were shown in Table 1.
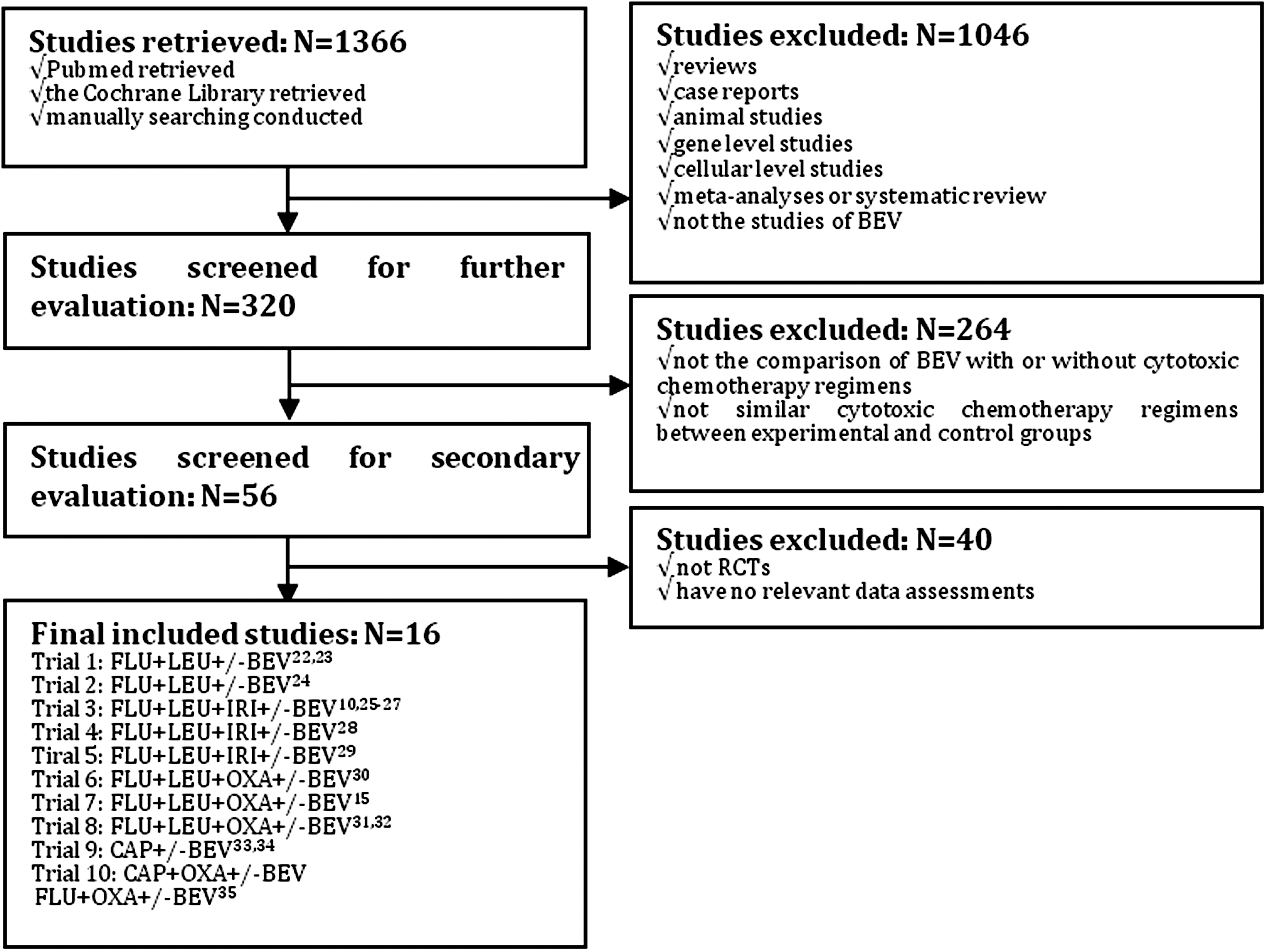
Flow chart of included trials.
an approximate estimate; 1, random sequence generation; 2, allocation concealment; 3, blinding of participants and personnel; 4, blinding of outcome assessment; 5, incomplete outcome data; 6, selective reporting; 7, other bias.
L, indicate low risk of bias; H, indicate high risk of bias; U, indicate uncertain risk of bias; IV, intravenous injection; FLU, 5-fluorouracil; LEU, Leucovorin; IFL, bolus 5-fluorouracil/folinic acid/irinotecan; IRI, Irinotecan; BEV, bevacizumab; CAP, Capecitabine; CRC, colorectal cancer; mCRC, metastatic colorectal cancer; ECOG, Eastern Cooperative Oncology Group; AC, adjuvant chemotherapy; RT, radiation chemotherapy; SG, surgery; OXA, oxaliplatin.
Identification of trials
Deadline for trials publication and/or presentation was March, 2012. Updates of RCTs were systematically searched through PubMed ( #1 colon* #2 rect* #3 colorect* #4 ((#1) OR #2) OR #3 #5 carcinoma #6 neoplasm* #7 tumor #8 cancer #9 (((#5) OR #6) OR #7) OR #8 #10 bevacizumab #11 Avastin #12 (#10) OR #11 #13 ((#4) AND #9) AND #12
Appropriate modifications were made and identical search was performed through the Cochrane library during the same period, but did not identify any additional articles. Researches were also performed so that both completed and current trials could be identified. All titles and abstracts identified by search strategies were assessed for relevance. Full papers were obtained if potential relevance could be confirmed or uncertainty existed. Additionally, no language or date limitations were imposed. Unpublished trials were sought through electronic searches, but none could be identified. The literature search, inclusion and exclusion criteria establishment, identification of relevant articles were all performed and verified by both of the two investigators (D.Z., Y.L.W.) independently. Any uncertainty or discrepancies about the eligibility of a trial or particular treatment groups within trials were resolved by discussion with the involvement of a third investigator (C.L.), and final consensus was made.
Data collection and quality assessment
The data presenting the most comprehensive results comparing CTX with/without additional targeted agent-BEV was extracted into a form, which was made by one investigator and modified by other investigators. For studies that had more than one published reports, each eligible outcome was collected into the identical trials, then the outcome from most recent reports was used where there was a possibility of overlapping data. The primary outcome measure was overall survival (OS), which was defined as the time from randomization until death by any cause. Data for survivors were censored on the date of last follow-up. The secondary outcome was progression-free survival (PFS), which was defined as the time from randomization until progression or death by any cause. Data for survivors without progression were censored on the date of last follow-up. Trials presenting OS and/or PFS were considered for inclusion. Overall response rate (ORR) and several adverse events were also taken into consideration.
Quality assessments for eligible trials were evaluated when referring to the Cochrane collaboration's tool for assessing risk of bias within the Cochrane handbook 5.1.0 (available on
Analysis and statistics
To investigate the targeted adjuvant effects of BEV when adding to CTX, all results were then combined to give overall hazard ratios (HRs, for OS and PFS) or odds ratios (ORs, for ORR, or other adverse events) for all of the chemotherapy regimens. Subgroup analyses were also done for each specified category basing on the CTX, for example, FLU+LEU, IFL, FOLFOX and CAP-based chemotherapy, to further evaluate the additional benefits of BEV to each specified CTX.
We analyzed data by using a random-effects model due to the anticipated clinical heterogeneity across the included trials to provide more conservative estimates. Statistical heterogeneity was evaluated using the X 2 test, and the I 2 describing the percentage of total variance across trials due to heterogeneity rather than chance. A probability level for the X 2 statistic ≤10% (p≤0.10) or an I 2 ≥50% were considered indication of statistical heterogeneity. The possible existence of publication bias was explored by funnel plots through the trim and fill method. 16 The recorded heterogeneity and presenting funnel asymmetry was identified by performing subgroup analyses with matching for CTX, and subsequently sensitivity analyses. AS for one or more study-level variables explaining the heterogeneity of related regimens were then explored in meta-regression models for all studies combined. 17,18 In addition to subgroups based on CTX, we took sample size of each individual trial, dosage of BEV, percentage of surgery before chemotherapy as confounding factors.
Survival curves for OS and PFS are presented as simple (non-stratified) Kaplan-Meier curves, which were performed by combining relevant data extracted from the original Kaplan-Meier curves.
19
–21
Engauge Digitizer 4.1 (available on
All statistical analyses were done with StataSE 12.0.
Results
Up to March, 2012, 16 reports 10,15,22 –35 compared the combination of CTX with/without targeted agents-BEV. Several data were reused within several reports separately, for example, trial 1, trial 3, trial 8 and trial 9, which were described in Figure 1. The details of extracting eligible citations were also described in this Figure, with 7,127 people having CRC involved into final meta-analyses. Two trials 22,23 underwent FLU+LEU based chemotherapy, with 349 patients involved; 3 trials 10,25 –29 underwent IFL-based chemotherapy, with 1,249 patients involved; 3 trials 15,30 –32 underwent FOLFOX based chemotherapy, with 3,834 patients involved; 1 trial underwent CAP based 33,34 chemotherapy, with 313 patients involved; 1 trial 35 underwent both CAP+OXA based and FOLFOX based chemotherapy, with 700 patients involved, respectively. Seven trials 10,15,22 –27,30 –32 were completed in USA, the other three trials were completed in Greece, 28 China 29 and Australia, 33,34 respectively.
In meta-analyses done for OS and PFS when comparing targeted agent-BEV added to CTX versus CTX alone in the treatment of CRC, BEV is associated with evidently decreased HR [Fig. 2(a) showed overall effect for OS and Fig. 3(a) showed overall effect for PFS). And significant heterogeneity between trials could be identified (I 2 =43.5%, p=0.060 for OS; I 2 =61.6%, p=0.004 for PFS]. The results for both outcomes remained much the same when the above analyses were repeated with fixed-effects models.
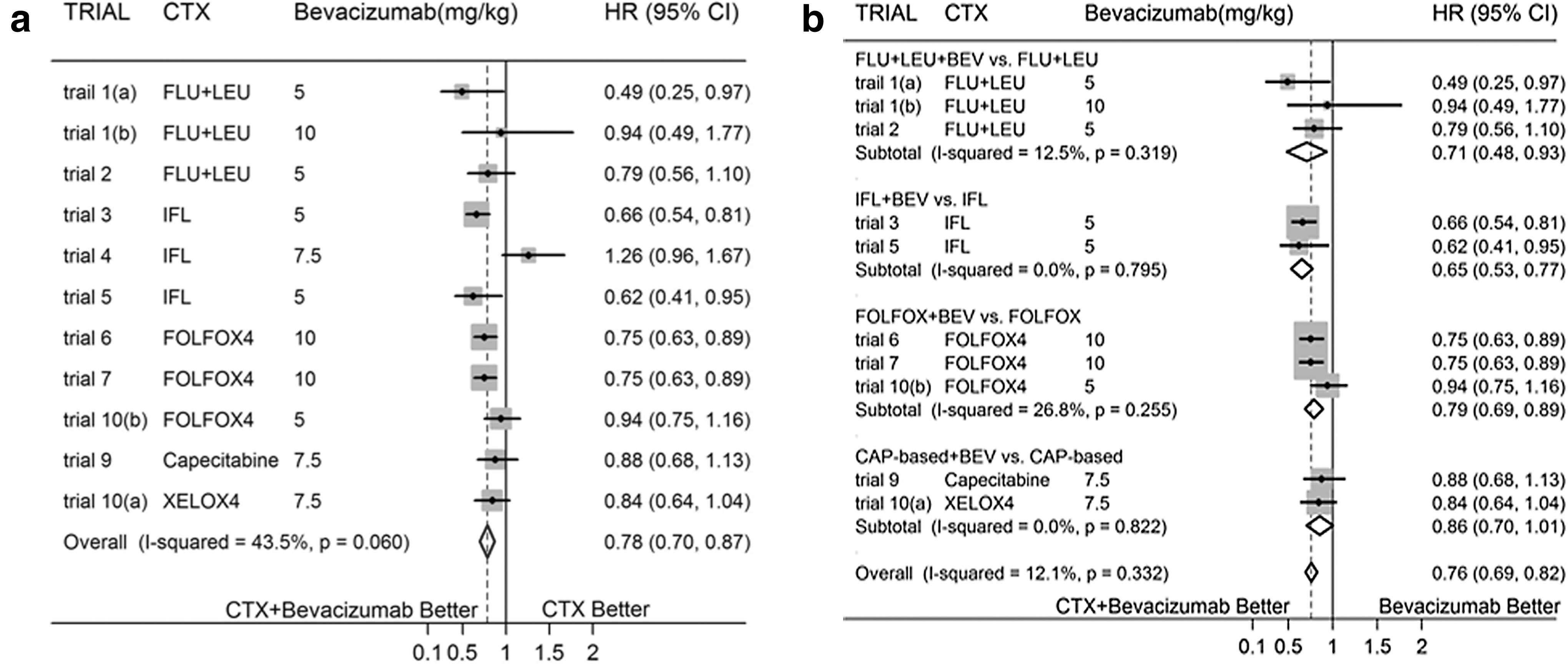

There were evidence of funnel-plot asymmetry for both outcomes about OS (p=0.020) and PFS (p=0.001). Subgroup analyses were done basing on different CTX, significantly decreased HRs for subtotal effects in OS were identified in the regimens about FLU+LEU based and FOLFOX based chemotherapies with/without BEV, with no evidence of statistical heterogeneity; while no significant differences were identified between CAP based chemotherapy with/without BEV (with no heterogeneity was identified) and IFL based chemotherapy with/without BEV, but with evidence of statistical heterogeneity (I 2 =80.1%, p=0.007) in IFL group. Sensitivity analyses were performed, and statistical heterogeneity disappeared after eliminating trial 4, 28 which led to funnel-plot asymmetry. Additionally, subgroup analyses for PFS were done basing on similar CTX, with evident decreased HRs for all of the subgroups; but significant heterogeneity was found in FOLFOX group (I 2 =81.9%, q=0.001). Sensitivity analyses were performed, and then statistical heterogeneity disappeared after eliminating trial 831,32 which led to funnel-plot asymmetry.
In meta-regression analyses for OS, the associations between additional targeted chemotherapeutic agent-BEV and HRs were not substantially altered by sample size of each individual trial, dose of BEV, and CTX. However, they did depend on the percentage of prior surgery for CRC (p=0.012). In multivariate meta-regression analyses, after adjusted for these variables, percentage of prior surgery and CTX could explain 100% of between-study variance (p=0.0184), but with a stronger association with percentage of prior surgery than CTX (p=0.009). As for meta-regression analyses for PFS, the associations between BEV and HRs were not substantially altered by dose of BEV, and CTX. However, they did depend on the sample size of each individual trial (p=0.001) and the percentage of prior surgery for CRC (p=0.001). Both of these two confounding factors could explain 100% of between-study variance.
Subgroup analyses were reconfirmed after eliminating trial 4 in OS and trial 8 in PFS which were attributable to evident between-study heterogeneity. All subgroup analyses for both OS and PFS identified significantly decreased HR, excepting for CAP based CTX for OS [Fig. 2(b) and Fig. 3(b)].
The OS and PFS endpoints were also described with Kaplan-Meier curves, with median survival duration prolonged approximate 1.9 months in OS (18.2 vs. 16.3, p=0.0003) and 2.4 months in PFS (8.9 vs. 6.5, p=0.0000), which were described in Figure 4(a) and Figure 4(b).

Pooled estimates of ORs for ORR and several common grade 3 or 4 adverse events were also performed, and shown in Table 2. BEV tended to be associated with significantly higher OR when added to CTX (OR, 1.79; 95% CI, 1.28–2.50).
GI, gastrointestinal; exp, experimental group; con, control group; CI, confidence interval; ORR, objective response rate; OR, odds ratio.
As for study about the incidence of adverse events, the addition of BEV to CTX tended to be associated with significantly higher OR for any adverse events when compared with CTX alone (OR, 2.14; 95% CI, 1.71–2.69). The addition of BEV may also increase the incidence rate of grade 3 and 4 adverse events in hypertension, thrombosis, proteinuria, gastrointestinal perforation, and fatigue, with evident differences in ORs. But no evident between-group differences could be identified in the adverse events for bleeding, diarrhea, and leukopenia. Details were described in Table 2.
Discussion
Acting as a targeted antiangiogenic therapeutic agent for cancer, BEV provides little clinical benefits as a single agent, 15 and its additional benefits to CTX varied among each individual trial in the treatment of CRC. This meta-analysis of individual trials identified that the addition of BEV to CTX was more effective comparing with CTX alone in improving the rate of survival in terms of OS and PFS, which may confirm the feasibility of adding targeted agents to CTX when treating CRC. And the median survival duration approximately prolonged 1.9 months in OS, and 2.4 months in PFS. The pooled estimate for ORR also identified improved response rate of BEV after adding CTX compared with CTX alone. It has a major prognostic effect on the survival of patients. 36 The duration of BEV therapy is likely to be important, and treatment until disease progression may be necessary to maximize the clinical benefit derived from BEV therapy. 35
However, the rate of any adverse events also increased, especially for hypertension, thrombosis, proteinuria, gastrointestinal perforation, and fatigue is grade 3/4. It was consistent with the controversy that the achievement of OS and PFS benefit with the addition of BEV to chemotherapy is at the cost of a significant increase in toxicity. 37,38 Though grade 3/4 bleeding event was not evident in this meta-analysis, several reports had identified it. 15,30,37 Moreover, Saltz et al. 35 pointed out that neurotoxicity, gastrointestinal disorders, and hematologic events are the most common reasons for treatment discontinuation, which were attributable to CTX rather than BEV. Some trials had specified cerebral metastases, advanced atherosclerotic disease, or proteinuria as contraindications to the use of BEV. 37
Additionally, frequent monitoring of blood pressure is necessary, and it is manageable with oral antihypertensives when hypertension occurs. 37 The use of low-dose aspirin (≤325 mg/day) can also reduce the incidence of arterial thromboembolic events in high-risk patients treated with BEV, 39 but no increased bleeding risk in patients receiving BEV and anticoagulation therapy. 35
As aforementioned, the additional benefits of BEV were not consistent across trials. As for OS, no efficacy of additional BEV to CTX could be identified in several trials, including FLU+LEU, 22,23 IFL, 10 FOLFOX4, 30 and CAP 29,30 based chemotherapy regimens. However, after being stratified based on the CTX, the addition of BEV to FLU+LEU and FOLFOX based chemotherapy showed evident efficacy; its additional benefit was also evident in IFL-based chemotherapy after ignoring the trial 10 leading greatly heterogeneity, suggesting that prior surgery treatment for CRC maybe a main confounding factor; as for CAP-based chemotherapy regimens, both trials 29,30 identified no additional benefits of BEV. As for PFS, the additional benefits of BEV to CTX were identified in all trials except trial 1(b) and trial 8. The additional benefits were evident in all subgroups, after stratified basing on the CTX. And no alteration was identified after eliminating trial 8, which led to greatly heterogeneity mainly due to prior surgery treatment for CRC. Its largest sample size maybe also a confounding factor. Though adding BEV to CAP significantly improved PFS, but did not improve OS. It should be considered as a first line therapy option for patients with mCRC, especially when considering the benefits of controlling caner with limited adverse events, especially for those who are unfit for, or also do not require initial IRI or OXA. 33
Some studies have also indicated that the benefit of BEV is independent of age, and that toxicity is not excessive either in older patient groups, 33 or higher dose of BEV. 10,22,24 However, cautions should be exercised in IRI contained regimens, since advanced age, prior pelvic radiation therapy, impaired performance status, and low serum albumin have all been reported to increase IRI-associated toxicities 40 –43 ; cautions should also be exercised in FOLFOX regimens, since the association of increasing age with excess toxicity, 31,44 despite BEV was not associated with major additional toxicity except for a modest increase in rates of arterial thrombosis events in the older patient group. 33
Additionally, predictive markers in relation to the treatment effects with/without BEV were also explored, and the survival benefit with the addition of BEV in the treatment of mCRC is independent of the status of biomarkers, such as K-ras, b-raf, and p-53. 26 –28,34 But D-dimer may represent a useful biomarker for patients treated with antiangiogenic agents, though strongly correlated with OS, but not PFS. 23
In conclusion, BEV, acting as a targeted and antiangiogenic cancer therapeutic agent, is of efficacy and feasibility in adjuvant to CTX. However, the pros and cons should be considered since the generation of benefits is at the cost of toxicity. Further exploration should be considered to find out more directed prognosis predictors on the basis of additional efficacy of BEV to CTX, especially for each specific chemotherapy regimens.
Footnotes
Disclosure Statement
No competing financial interests exist.