
Abstract
Carcinoembryonic antigen (CEA) is an attractive target molecule of radioimmunotherapy (RIT). To enhance RIT's therapeutic efficacy, the fractionation of radiolabeled antibody doses is an attractive strategy. In this study, a fully human anti-CEA monoclonal antibody (mAb) C2-45 was selected by virtue of its lack of immunogenicity, and the effectiveness of fractionated RIT with yttrium-90 (90Y)-labeled mAb C2-45 was evaluated. In LS180 tumor-bearing mice, indium-111 (111In)-labeled mAb C2-45 showed high and persistent tumor accumulation. Therapeutic studies were performed with single doses of 90Y-mAb C2-45 (100 or 200 μCi) or double doses of 100 μCi 90Y-mAb C2-45 at different intervals (5, 10, and 15 days). All 90Y-mAb C2-45-treated mice showed inhibition of tumor progression, while the time to tumor progression was much longer in both the 200-μCi-treated group and the double 100-μCi-treated group than in the single 100-μCi-treated group. The therapeutic effect of the double 100 μCi administration at days 0 and 15 lasted significantly longer than that in the other treatment groups. These findings indicate that 90Y-mAb C2-45 may be a promising agent for the treatment of CEA-positive cancer and that the fractionation of 90Y-labeled antibody doses could enhance the therapeutic effect if performed according to an appropriate protocol.
Introduction
Radioimmunotherapy (RIT) targeting CD20 has been widely used for non-Hodgkin's lymphoma therapy and has shown significant therapeutic efficacy in clinical practice. 1,2 Many other molecules have also been studied as a target of RIT for the treatment of solid tumors. Among them, carcinoembryonic antigen (CEA) is an attractive target molecule of RIT. CEA is a well-known cancer-associated biomarker in the blood and is expressed in many types of tumor, such as colorectal cancer, gastric cancer, and lung cancer. 3,4 Thus, RIT targeting CEA has great potential for the treatment of various types of cancer. A large number of radiolabeled anti-CEA monoclonal antibodies (mAbs) have been studied, and some of them have been used in clinical practice. 5,6 However, since the therapeutic efficacy of radiolabeled anti-CEA mAbs is not sufficient, combining RIT with anticancer drugs or pretargeting RIT has been undertaken to enhance therapeutic efficacy. 7 –9
Fractionated RIT is an attractive strategy to enhance therapeutic efficacy. Since the fractionation of radiolabeled antibody doses could decrease normal tissue toxicity, fractionated RIT enables us to increase the total dose of radioactivity, and thus to enhance therapeutic efficacy. 10 –12 Furthermore, fractionation doses were also reported to enhance therapeutic efficacy even when their combined dose was the same as a single dose. 13 Meanwhile, one problem with fractionated RIT is antibody immunogenicity arising from multiple doses. To reduce the immunogenicity of antibody drugs, not only the chimerization process, but also technologies to make fully human mAbs have been developed. 14 –16 Recently, several fully human mAbs have already received approval and have been used in clinical practice. Thus, fully human mAbs should be used as a carrier of fractionated RIT.
In this study, mAb C2-45, a fully human anti-CEA mAb established by Kuroki and colleagues 17 was radiolabeled, and binding assays to CEA-expressing tumor cells and biodistribution studies in tumor-bearing mice were performed. The therapeutic efficacies of various treatment protocols of yttrium-90 (90Y)-labeled mAb C2-45 in tumor-bearing mice were compared (a single dose or double doses at various intervals). Based on the results, the potential of 90Y-mAb C2-45 for CEA-positive cancer therapy and the effectiveness of dose fractionation of 90Y-labeled mAb on therapeutic efficacy were evaluated.
Materials and Methods
General
A human anti-CEA antibody C2-45 was kindly given by Kyowa Hakko Kirin Co., Ltd. A colon cancer cell line expressing a high level of CEA, LS180, 18 was purchased from the American Type Culture Collection. Other reagents used for preparation of radiolabeled antibody were of reagent grade and used as received.
Radiolabeling antibody
Iodine-125-labeled mAb C2-45 (125I-mAb C2-45) was prepared according to standard protocols for the chloramine-T method. Briefly, 740-kBq/2 μL of Na125I (MP Biomedicals, Inc.) and 1 μg of chloramine-T in 3 μL of 0.3 M phosphate buffer were added to 10 μg of antibody in 100 μL of 0.3 M phosphate buffer. After incubation for 5 minutes at room temperature, the labeled antibody was purified using a Bio-Spin 6 Column (Bio-Rad Laboratories) according to the manufacturer's protocol. For labeling with indium-111 (111In) or 90Y, 2-(4-isothiocyanatobenzyl)-diethylenetriaminepentaacetic acid (SCN-Bn-DTPA; Macrocyclics) was conjugated to mAb. Typically, SCN-Bn-DTPA in dimethylformamide was added to mAb at 5–10 mg/mL in 50 mM borate-buffered saline (pH 8.5) at a molar ratio of 5:1. After incubation at 37°C for 20 hours, DTPA-mAb was purified using a Bio-Spin Column. The number of DTPA attached per molecule of mAb was calculated to be 2.0, according to the procedure described previously 19 with slight modifications. Briefly, 10 μL of 111InCl3 (Nihon Medi-Physics) was incubated in 15 μL of 0.25 M acetate buffer (pH 5.5) for 5 minutes at room temperature, then added to the 5 μL of unpurified reaction mixture. After being left to stand at room temperature for 1 hour, protein-bound radioactivity was determined by ITLC (Gelman Science, Inc.) developed with saline. For the preparation of the 111In-labeled antibody (111In-mAb C2-45), 40 μL of 111InCl3 was incubated in 60 μL of 0.25 M acetate buffer (pH 5.5) for 5 minutes at room temperature followed by incubation with 10 μg of DTPA-mAb for 1 hour at room temperature. The labeled antibody was purified using a Bio-Spin Column. For the preparation of the 90Y-labeled antibody (90Y-mAb C2-45), 80 μL of 90Y solution (nuclitec GmbH) was incubated with 100 μL of 0.25 M acetate buffer (pH 5.5) for 5 minutes at room temperature, followed by incubation with 1 mg of DTPA-mAb for 1 hour at 37°C. The labeled antibody was purified using a PD-10 column (GE Healthcare Biosciences AB) according to the manufacturer's protocol. The radiolabeling yield of 90Y-mAb C2-45 was 92.2%±3.3%, and the specific radioactivity of 90Y-mAb C2-45 after purification was 4.08±0.62 mCi/mg mAb (mean±S.D. of seven experiments).
Binding assay
A solution of 125I-mAb C2-45 (containing 0.01 μg of antibody) was added to 100 μL of cell suspension (containing 1×106 cells) with various amounts of nonlabeled antibody. After incubation for 1 hour at room temperature, the cell suspension was centrifuged at 3000 rpm for 5 minutes. After the supernatant was removed, the radioactivity of the cell fraction was measured with a well-type γ counter (ARC7001; Aloka Co. Ltd.) and compared with the initial radioactivity. Bmax (antigen expression level) was determined by Scatchard plot analysis.
The immunoreactivity of DTPA-conjugated mAb C2-45 was evaluated as the inhibitory activity toward 125I-mAb C2-45 binding to the cells relative to that of mAb C2-45.
Biodistribution study
The animals were cared for and treated in accordance with the guidelines of the animal care and experimentation committee of Gunma University. BALB/c nude mice were purchased from CLEA Japan. Tumor-bearing mice were prepared by implantation of LS180 tumor cells (1×106 cells) in 100 μL of PBS into the flanks of BALB/c nude mice. When the tumors were fully established (about 8–10 mm in diameter, 2–3 weeks after implantation), biodistribution experiments were performed by intravenously administering 111In-mAb C2-45 (protein dose: 20 μg). Animals were killed at 1, 24, and 48 hours after administration, and tissues of interest were excised and weighed. Their radioactivity was then measured with a well-type γ counter. To evaluate the specificity of tumor accumulation, biodistribution studies of 111In-mAb C2-45 with increasing amounts of unlabeled antibody (20, 100, or 500 μg/animal) were performed.
Therapeutic study
For the therapeutic studies, LS180 tumors were grown in BALB/c mice in the same way as described above. When the tumors were fully established (0.52±0.25 cm3, 2–3 weeks after implantation), animals were randomly assigned to each treatment group (four to seven mice per group). There was no significant difference of the average tumor size between groups. The mice were intravenously administered 100 or 200 μCi of 90Y-mAb C2-45 (protein dose: 20–30 μg/100 μCi) or nonlabeled mAb C2-45 (100 μg). On the selected day (at day 5, 10, or 15), some of the 100-μCi-treated mice were readministered 100 μCi of 90Y-mAb C2-45. Untreated mice were used as a control. Three therapeutic studies with different protocols were performed. Study 1: a single dose of nonlabeled mAb C2-45 (100 μg) (n=4), a single dose of 90Y-mAb C2-45 (100 μCi) (n=5), double doses of 90Y-mAb C2-45 (100 μCi) at days 0 and 10 (n=5), or untreated (n=5). Study 2: a single dose of 90Y-mAb C2-45 (100 μCi) (n=5), double doses of 90Y-mAb C2-45 (100 μCi) at days 0 and 5 (n=5), double doses of 90Y-mAb C2-45 (100 μCi) at days 0 and 15 (n=5), or untreated (n=5). Study 3: a single dose of 90Y-mAb C2-45 (100 or 200 μCi) (n=6 and n=7, respectively), double doses of 90Y-mAb C2-45 (100 μCi) at days 0 and 15 (n=5), or untreated (n=5). Regularly, the mice were weighed and the tumor diameters were measured by calipers. Tumor volumes were determined using the following formula: (length)×(width)×(height)×0.5, then the relative tumor size was calculated by dividing each initial tumor volume.
Statistical analysis
Data are expressed as mean±standard deviation where appropriate. Statistical analysis was performed by using the unpaired t-test for comparing differences between two groups, and by using one-way ANOVA followed by the Tukey's honestly significant difference (HSD) test for comparing differences between multiple groups. Differences were considered statistically significant when p-values were less than 0.05.
Results
Binding assay
High binding of 125I-mAb C2-45 to LS180 cells was observed without a nonlabeled antibody, and this binding was inhibited by mAb C2-45 in a concentration-dependent fashion (Fig. 1). These results indicated the high and specific binding of mAb C2-45 to LS180 cells. The CEA expression level was calculated at about 825,000 molecules per cell by using Scatchard plot analysis. DTPA-mAb C2-45 inhibited the binding of 125I-labeled mAb C2-45 to LS180 at almost the same concentration as with mAb C2-45, indicating that DTPA conjugation has little effect on the immunoreactivity of mAb C2-45.
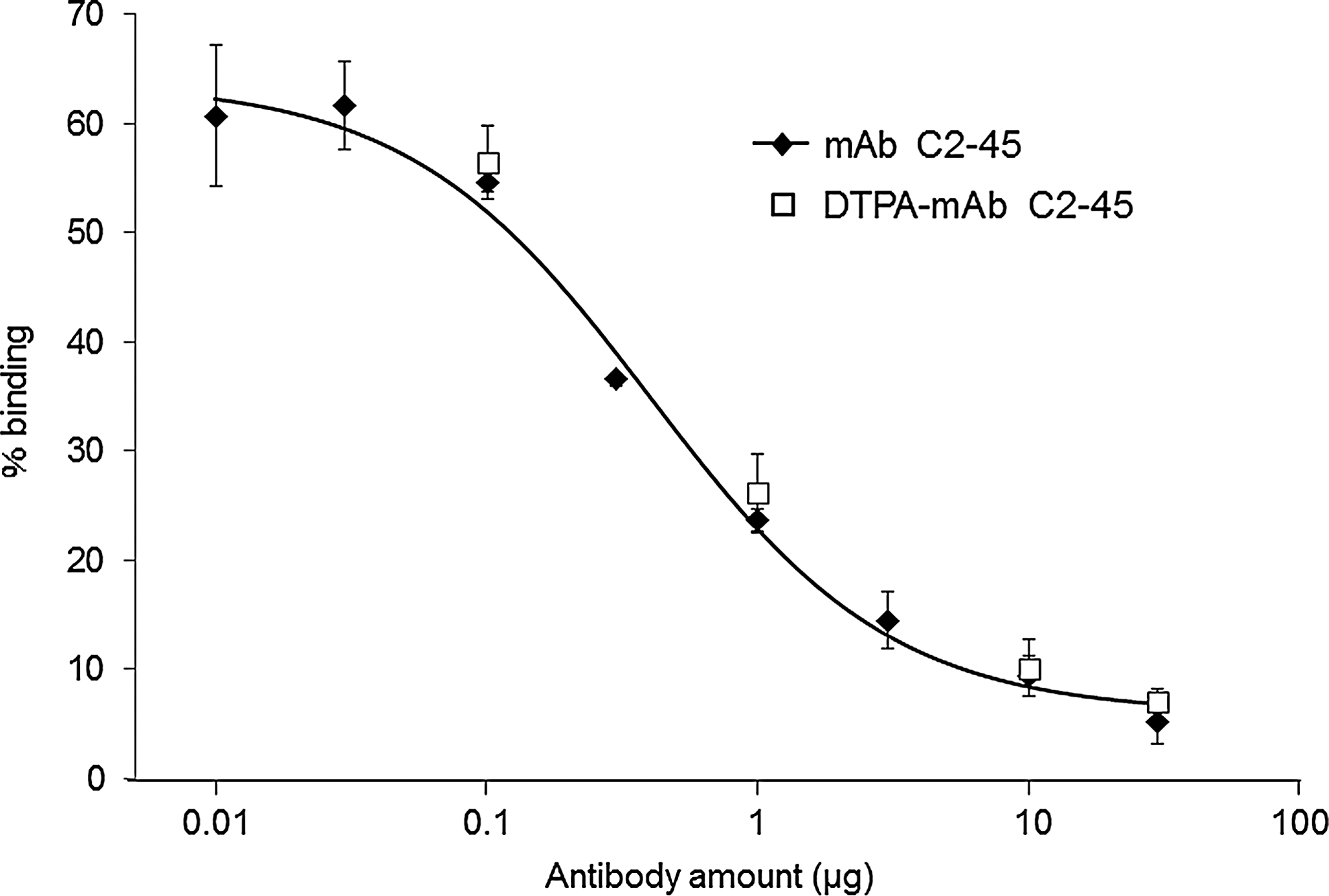
Binding of 125I-mAb C2-45 to LS180 cells. Each amount of nonlabeled antibody or DTPA-conjugated antibody was added. mAb, monoclonal antibody; 125I-mAb C2-45, iodine-125-labeled mAb C2-45.
Biodistribution study
Tumor accumulation of 111In-mAb C2-45 was high and persistent (16.2%±2.6% and 19.8%±3.6% ID/g at 24 and 48 hours after administration, respectively) (Fig. 2). The tumor-to-blood ratio and the tumor-to-muscle ratio were 2.5±0.7 and 22.0±6.9 at 48 hours after administration, respectively. This tumor accumulation level was significantly reduced with increasing protein dose and became to about half by coadministration of 500 μg of mAb C2-45, indicating the specific accumulation of 111In-mAb C2-45 in the tumor (Fig. 3). Renal accumulation was also significantly reduced by coadministration of excess amount of mAb C2-45. Blood clearance was significantly delayed and lung uptake was significantly increased by coadministration of mAb C2-45. Accumulation in the bone was less than 3%ID/g at all time points after administration.
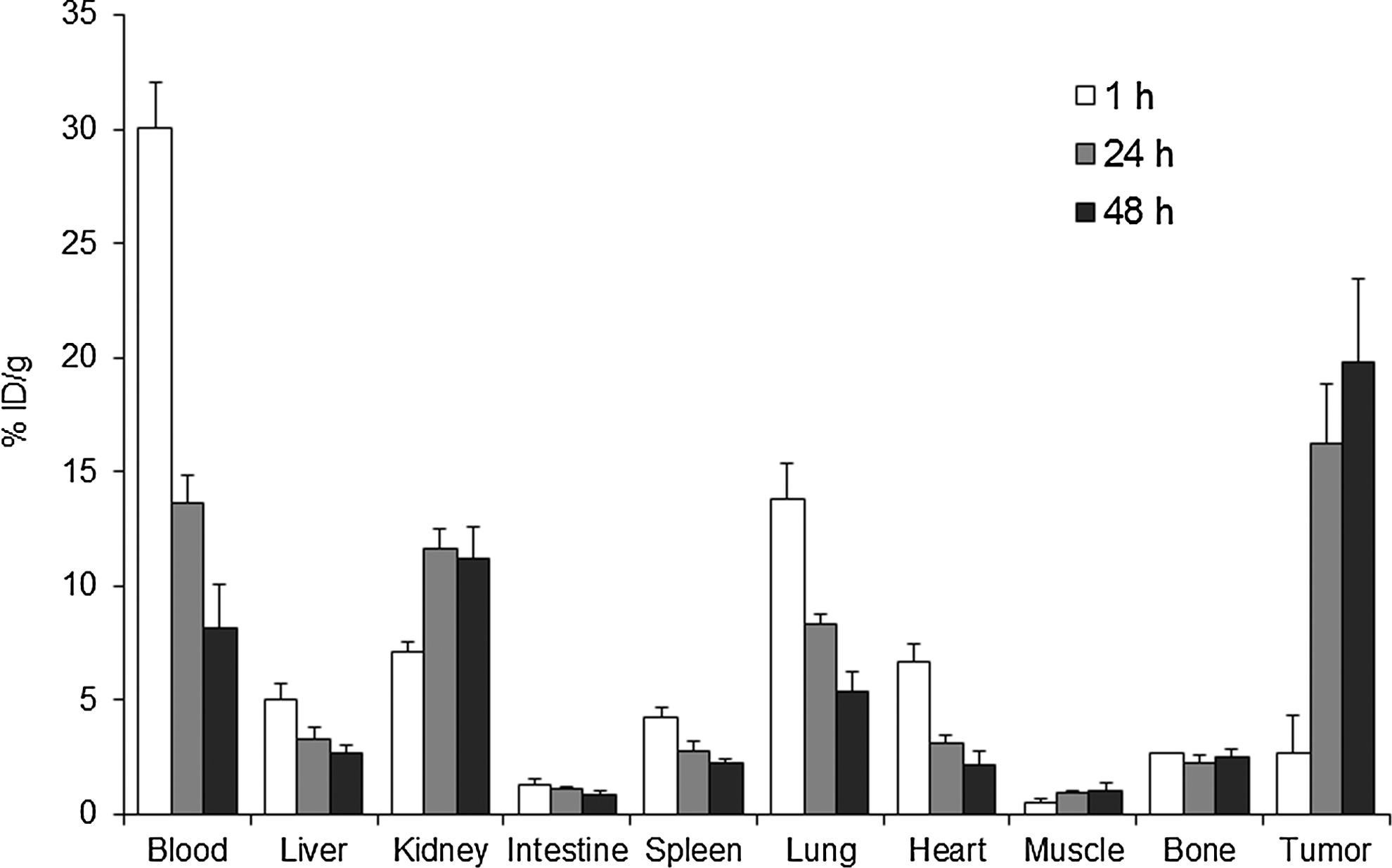
Biodistribution of radioactivity after intravenous administration of 111In-mAb C2-45 (protein dose: 20 μg) in LS180 tumor-bearing mice. Each value represents the mean±S.D. of five mice. 111In, indium-111.
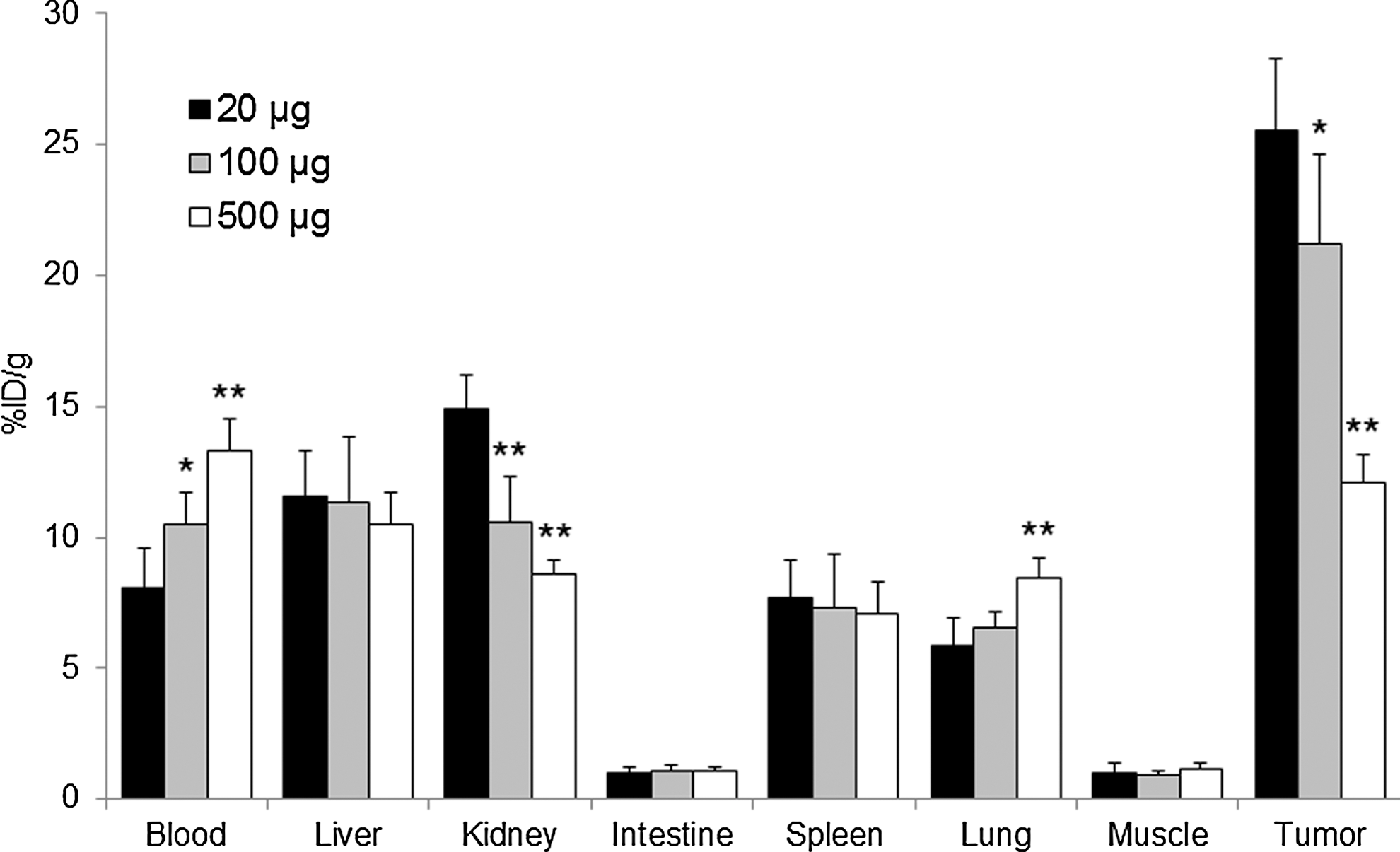
Biodistribution of radioactivity 48 hours after administration of 111In-mAb C2-45 containing different amounts of unlabeled mAb C2-45 (20, 100, or 500 μg/animal) in LS180 tumor-bearing mice. Each column represents four or five mice, and significant differences compared with the 20 μg injected group were determined (*p<0.05, **p<0.01).
Therapeutic study
Therapeutic studies with different protocols were performed in tumor-bearing mice. Tumor progression was inhibited by 90Y-mAb C2-45 treatment, while tumors grew rapidly in mice treated with nonlabeled mAb C2-45 at almost the same rate as those of untreated mice (Fig. 4A). The duration of the effect of the 200-μCi-treated group and that of the all double 100-μCi-treated groups were much longer compared with the single 100-μCi-treated group (Fig. 4A–C). Tumor regrowth in the single 100-μCi-treated group, the 200-μCi-treated group, and the all double 100-μCi-treated groups was observed at about 15 days, more than 25 days, and more than 25 days after treatment, respectively. Figure 5 summarizes the time to tumor progression, as defined by tumors reaching 2.5 times the baseline size, in accordance with a previous report. 20 The average time to tumor progression was significantly longer in the 90Y-mAb C2-45-treated groups than in the untreated or nonlabeled mAb C2-45-treated group (p<0.01). Among the treatments with 90Y-mAb C2-45, the average time to tumor progression of the 200-μCi-treated group or of the double 100-μCi-treated groups was significantly longer compared with the single 100-μCi-treated group (p<0.01). In comparison between the all double 100-μCi-treated groups and the 200-μCi-treated group, tumor progression was significantly slower and the average time to tumor progression was significantly longer in tumors with double 100 μCi administration at days 0 and 15 than in those with double 100 μCi administration at days 0 and 5, at days 0 and 10, or in tumors with single 200 μCi administration (Tukey's HSD test; p=0.016, p=0.002, and p=0.001, respectively). No mice died from toxicities in the all treatment groups. Although body weight transiently decreased (by less than 20%) after administration with 100 or 200 μCi of 90Y-mAb C2-45, it returned to normal levels within 3 to 4 weeks after the last treatment. The weight loss of the 200-μCi-treated group or of the double 100-μCi-treated groups was larger compared with the single 100-μCi-treated group (Fig. 6). In comparison between the all double 100-μCi-treated groups and the 200-μCi-treated group, the rate of weight loss was similar, but the shape of the body weight curves was different. Body weight loss of mice with double 100 μCi administration at days 0 and 15 occurred at a slower rate than those with double 100 μCi administration at days 0 and 5, at days 0 and 10, or in tumors with single 200 μCi administration.
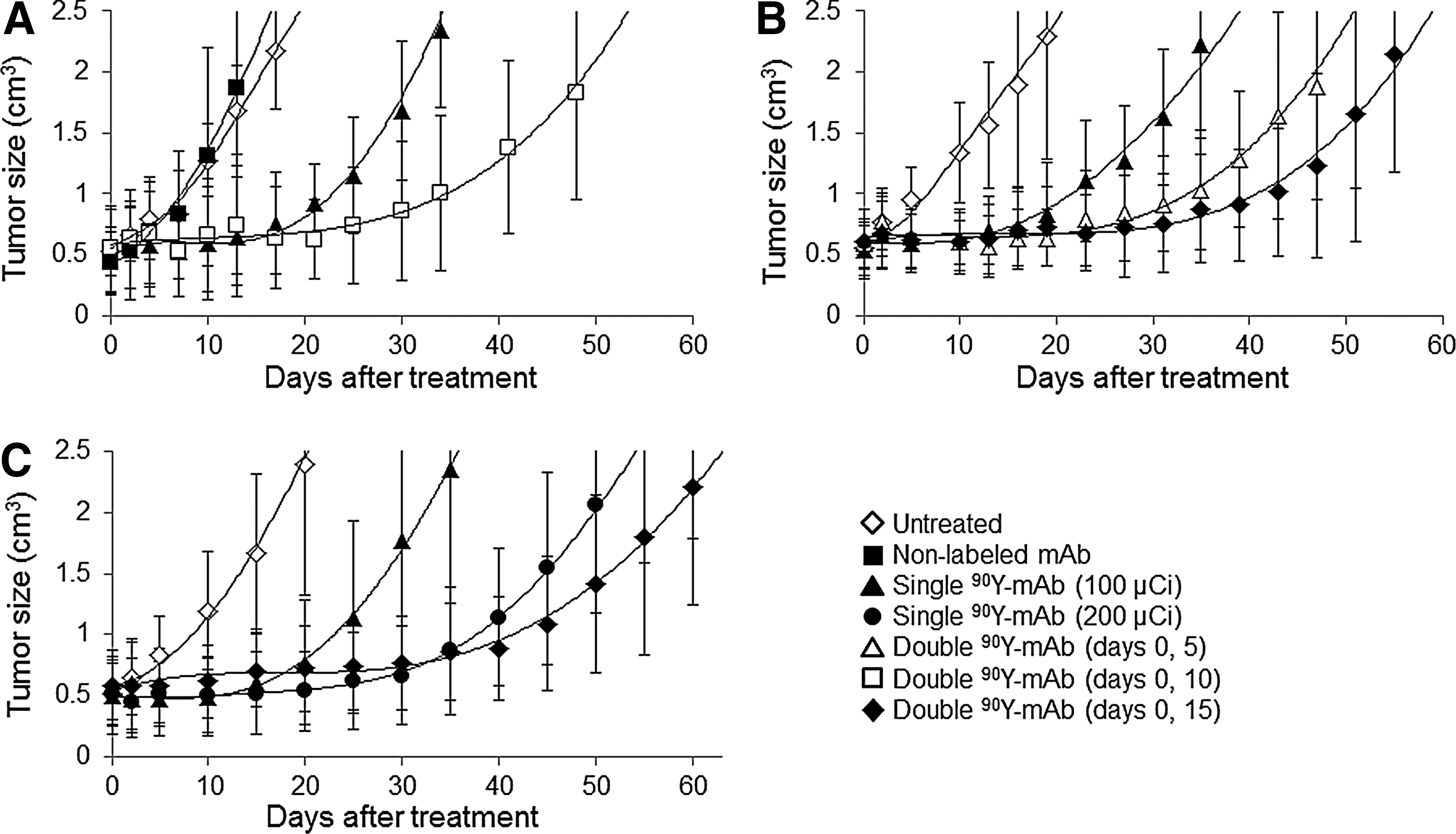
Radioimmunotherapy with 90Y-mAb C2-45 in LS180 tumor-bearing mice. Mice were intravenously administered with
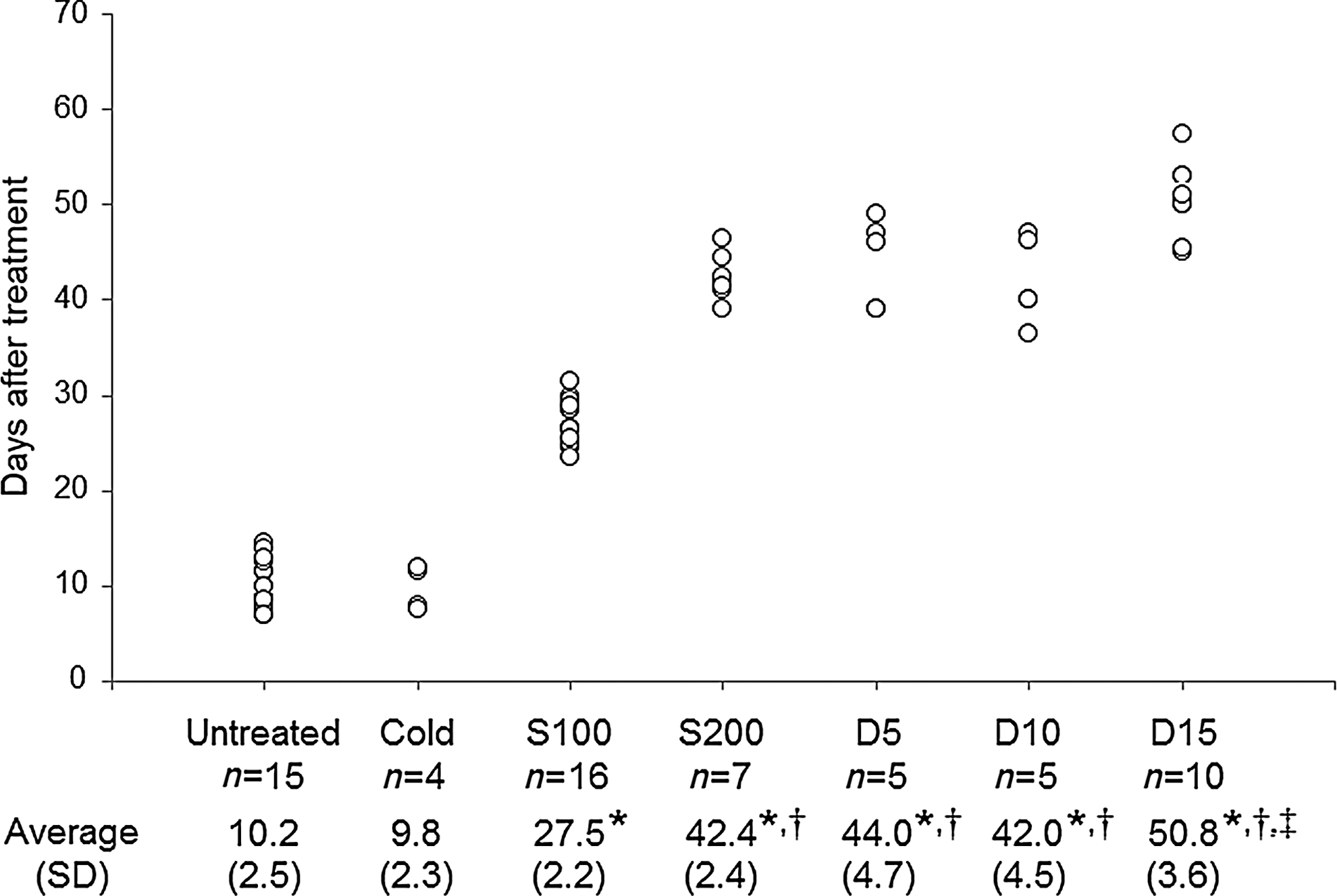
Time to tumor progression after initial treatment. The results of three different studies were unified. Each circle represents the day by which tumor volume had increased 2.5-fold from the baseline of individual mouse. The mean values (SD) of each group are shown below. Cold, nonlabeled mAb (100 μg); S100, single dose of 90Y-mAb (100 μCi); S200, single dose of 90Y-mAb (200 μCi); D5, double doses of 90Y-mAb (days 0, 5); D10, double doses of 90Y-mAb (days 0, 10); D15, double doses of 90Y-mAb (days 0, 15). Significant differences from untreated group (*p<0.01) and 90Y-mAb (100 μCi)-treated group († p<0.01), and comparison between the all double 100-μCi-treated groups and the 200-μCi-treated group (‡ p<0.05).

Relative body weight change after 90Y-mAb C2-45 treatment. Each value represents the mean relative body weight±S.D. of more than five mice.
Discussion
Human anti-CEA antibody mAb C2-45 binding was reported to be high and specific to CEA-expressed tumor cells. 17 Our binding studies also showed high and specific binding to the CEA-expressed tumor cell line LS180. DTPA conjugation showed little effect on the affinity of mAb C2-45, and 111In- or 90Y-labeling would not have an effect on the affinity since 111In or 90Y form complex only with DTPA and these complex formations would not induce conformational change of antibody. Thus, 111In- or 90Y-DTPA-mAb C2-45 would be expected to have high and specific binding to CEA-expressed tumor cells similar to DTPA-mAb C2-45. In a biodistribution study, 111In-mAb C2-45 showed high and persistent accumulation in LS180 tumors, and this accumulation was significantly reduced by coadministration of mAb C2-45. Since more than 10 μg of mAb C2-45 was required to completely inhibit 125I-mAb C2-45 binding to 1×106 cells in vitro, 500 μg of mAb C2-45 would not be enough to completely inhibit specific accumulation of 111In-mAb C2-45 in the tumor, and nonspecific accumulation of mAb C2-45 in the tumor would be much lower. These in vitro and in vivo results indicated that 90Y-mAb C2-45 should specifically accumulate in CEA-positive tumors, since the biodistribution of 111In-labeled mAbs is similar to that of 90Y-labeled mAbs. 21,22
Our therapeutic studies of LS180 tumor-bearing mice showed that 90Y-mAb C2-45 treatment significantly inhibited tumor progression. Since the administration of nonradiolabeled mAb C2-45 showed no therapeutic effect, we can infer that this therapeutic effect was due to irradiation from 90Y. In clinical practice, nonradiolabeled mAb C2-45 may show a therapeutic effect, since the human antibody is expected to have ADCC and CDC activity in human beings. Even so, 90Y-mAb C2-45 is a promising drug for the treatment of CEA-positive cancer. Since CEA is known to be expressed not only in colorectal cancer but also in other types of cancer, RIT with 90Y-mAb C2-45 has great potential to treat various types of cancer.
The inhibitory effects of 100 and 200 μCi of 90Y-mAb C2-45 treatment on tumor progression did not differ in the early phase, but the 200-μCi-treated group had a much longer effective period than the 100-μCi-treated group. Since the tumor size is not reduced in the early phase after treatment, 23,24 the enhancement of therapeutic efficacy would be apparent only in the duration of the effect. Since the proportion of surviving tumor cells in the 200-μCi-treated group would become smaller than that in the 100-μCi-treated group, it would take longer to form a tumor mass again.
It would be not easy to compare therapeutic effects between different experiments since time to tumor growth might vary from one experiment to the other. However, since there was no significant difference of the time to tumor progression between each untreated group or each single 100-μCi-treated group of three studies, comparison of the all double 100-μCi-treated groups and the 200-μCi-treated group could be acceptable. Among the three administration protocols of fractionated RIT, only the double administration of 100 μCi at days 0 and 15 inhibited tumor progression significantly longer than the single administration of 200 μCi did, which is also significantly longer than the double 100 μCi administration at days 0 and 5, at days 0 and 10 did. These results indicated that not only the fractionated RIT of the same total dose could prolong the therapeutic effect of 90Y-mAb C2-45, but also the administration protocol affects the therapeutic efficacy of fractionated RIT. It was reported that fractionated RIT with 131I-labeled anti-CEA mAb at a dosing interval of 2 or 3 days was less effective compared with the same total radioactivity of a single dose. 25 Additionally, the therapeutic efficacy of fractionated RIT with 131I-labeled anti-TAG-72 mAb was reported to be affected by the administration protocol. 13 Thus, designing an appropriate administration protocol would be critically important for successful fractionated RIT. Meanwhile, although the fractionation doses did not suppress the body weight loss of mice in our studies, since fractionation doses have been reported to increase the total amount of radioactivity that can be administered, fractionated RIT with 90Y-mAb C2-45 is expected to further enhance the therapeutic effect if it is performed with an escalating dose.
In our studies, a second administration just before regrowth (about 15 days after the first administration) showed better results; this protocol was successfully performed by Parry et al. 26 However, the appropriate protocol of fractionated RIT would vary depending on the radiolabeled antibody or on the tumor type. For example, a second administration earlier than regrowth would accelerate the therapeutic effect in cases where the tumor shrinks. 27 Thus, a schedule of fractionation doses is needed to optimize each RIT agent. However, after optimization, it would be possible to perform a second administration at an appropriate time for each patient, since the therapeutic response to RIT could be monitored by positron emission tomography with fluorine-18 (18F)-fluorodeoxyglucose (18F-FDG). 28,29
Since the immunogenicity of the antibody would be fatal to the clinical application of fractionated RIT, reducing it is necessary. Although chimeric or humanized mAb have been used to reduce immunogenicity, 111In-labeled chimeric anti-CEA mAb was reported to develop high immunogenicity in the clinical trial, 30 and radiolabeled humanized mAbs were also reported to exhibit immunogenicity in many clinical cases. 31,32 Although several clinical studies of radiolabeled fully human mAb are needed, the use of a fully human antibody would be an optimal approach for fractionated RIT due to its minimal immunogenicity. In that sense, the 90Y-labeled fully human antibody 90Y-mAb C2-45 would be a promising agent of RIT.
In biodistribution studies, relatively high renal accumulation was observed and this accumulation was significantly inhibited by coadministration of excess amount of mAb C2-45, indicating a specific accumulation. Blood clearance was significantly delayed by coadministration of mAb C2-45. The decreasing of the accumulation in the tumor and in the kidney by coadministration would be one of the factors to delay blood clearance of 111In-mAb C2-45. Another factor is that the excess of cold antibody would bind to the circulating CEA in the blood and therefore the 111In-mAb C2-45 would not form mAb-CEA complexes that are cleared from the blood. The accumulation in the liver was relatively low in Figure 3, however, the liver uptake in the inhibition study was higher (Fig. 4) in spite of the protein dose of these studies being the same 20 μg. The characteristics of mAb C2-45 or the different amounts of circulating CEA in the blood might be involved in these difficult results. Since mAb C2-45 is a fully human antibody, biodistribution in human would be different from that in murine, and clinical studies are warranted.
Conclusions
111In-labeled human anti-CEA antibody 111In-mAb C2-45 showed high and specific accumulation in the CEA-expressed LS180 tumor, and 90Y-mAb C2-45 showed a significant therapeutic effect. Thus, 90Y-mAb C2-45 is a promising agent for the treatment of CEA-positive cancer. Fractionation of the dose of 90Y-mAb C2-45 could significantly enhance the therapeutic effect if performed according to an appropriate protocol, indicating the effectiveness of fractionated RIT with the 90Y-labeled human antibody.
Footnotes
Acknowledgment
We are grateful to Kyowa Hakko Kirin Co., Ltd., for kindly providing the C2-45 human anti-CEA antibody.
Disclosure Statement
No competing financial interests exist.