
Abstract
Purpose:
Single-step iodination is often performed in preference to use of a radiometal label for initial animal biodistributions. Yet loss of iodine occurs in vivo so that it is important to measure uptake (%ID/g) differences between radiolabels.
Methods:
Murine biodistributions of four radioiodinated and 111In-labeled cognate anti-carcinoembryonic antigen antibodies were compared. Uptakes were obtained in athymic mice out to 96 hours for diabody, minibody, scFv-Fc, and intact humanized (M5A) versions of the T84.66 antibody. Tissues included liver, spleen, kidneys, lungs, and human LS174T colorectal xenografts. Ratios (R) of iodine uptake to indium uptake were calculated.
Results:
For all cognates, no significant differences were found in the blood uptakes between the two labels. In normal solid organs, iodine was generally cleared more rapidly with decreasing molecular weight (MW). In liver and spleen by 24 hours, the R value was 5% for diabody and minibody, whereas a value of 50% was seen for the intact mAb. Renal differences were even more marked for the two lower MW species. Tumor losses, however, were found to be essentially independent of MW and were modest; 50% by 48 hours. To test the generality of the results, comparisons were then made for normal organs and tumors of the R values found above for M5A and MN-14 intact antibody literature results. Good agreement, within estimated errors in R, was seen between these two cases, although 111In and 88Y were the respective radiometals.
Conclusions:
Loss of iodine from labeled antibodies can be marked in normal organs and that correction (by 1/R) of the iodine biodistribution to estimate the associated radiometal result may be possible. Explicit differences between the two types of biodistribution also imply that separate uptake results need to be considered when evaluating the impact on imaging and therapy using various possible radiolabels.
Introduction
After establishing the targeting of a novel protein to relevant normal or tumor cells in vitro, a critical next step in preclinical evaluation is an animal biodistribution study. In analyses involving tumor-seeking agents, one would typically utilize athymic mice, bearing human cancer xenografts. In such studies, organ uptakes u(t) are measured in percent injected dose per gram of tissue (%ID/g). Time (t) intervals are generally on the order of 0≤t≤96 hours during which five to eight time points are measured.
The importance of biodistributions cannot be overemphasized. It may be that the proposed agent has sequestration issues with one or more nonspecific sites such that targeting to the organ or molecule of interest is greatly inhibited. If this were the case, the investigator would probably want to shift attention to another possible targeting agent and cease the production of the product under test. Yet limited amounts of material may make such initial animal studies difficult if a radiometal were used as the label. This follows from the typical two-step approach used for metal labeling: first attaching a chelator and then adding the radioactive ion to the chelated protein. By experience, metal conjugation requires a minimum of several milligrams of protein, whereas radioiodination can be achieved with hundreds of micrograms. Thus, there is a necessary emphasis in the literature on single-step iodine labeling of any new protein for this initial biodistribution. This strategy, however, has two specific limitations.
First, while iodine has a number of useful imaging and therapy isotopes, including 123I, 124I, 125I, and 131I, the user of the successful putative agent may wish to consider a metal as a more flexible choice as radiolabel. Since approximately 70% of the Periodic Table is made up of metals, the number of possible options is thereby enhanced. Additionally, because of its decay scheme and emitted particles, a radiometal might permit better imaging or therapy using the protein of interest. Thus, the investigator may choose to use a label that unfortunately requires relatively large amounts of the novel protein. If such amounts are not yet available, the evaluation of the metal-based biodistribution would not be possible.
The second limitation of an iodine-based biodistribution is that the results differ significantly from those obtained using a radiometal label. 1 Generally, the former show more rapid loss from all normal organs in the test animal. It is not clear if malignant tissues exhibit similar action—although this outcome may be expected to some degree as tumor cells have an origin in normal tissues. In vivo catabolism and subsequent iodine loss are assumed to contribute to this effect. 2 Additionally, one may postulate the persistence of water-soluble metallic ions remaining inside the cell while the iodine metabolic compounds may be soluble in the cellular lipid membrane so as to more readily exit from a given tissue. 3,4 The authors have used the rubric dehalogenation to cover these various iodine-loss processes in the following.
Thus, while obtaining an iodine biodistribution may be expedient, it may not be indicative of radiometal measurements with the same protein. It would be useful if a method was at hand to help predict the metal-based biodistribution UIn given these initial iodine results UI. In the following, such a method is outlined for a group of proteins designed to target carcinoembryonic antigen (CEA). Radioiodine and 111In results are compared for four representative anti-CEA antibodies, and functions are determined, which allow transforming the more-accessible iodine results into the corresponding indium biodistributions. It is important to measure the magnitude of these labeling differences over time and to relate these variations to both the protein's molecular weight (MW) and the organ or tissue in question. With such information, the analyst may, at least, make estimates of the changes that may be expected when converting the radiolabel from iodine to metal.
Materials and Methods
Anti-CEA proteins
Only a limited number of antibodies have been evaluated with regard to both iodine-labeled and radiometal-labeled biodistributions. Literature examples include the diabody, 5 minibody, 6 the I253A scFv Fc fragment, 7 and intact humanized M5A antibody. 8 MWs for the four cognates were 55, 80, 105, and 150 kDa, respectively. In the examples, 131I and 125I were iodination labels using the Iodogen method. The Iodogen technique led to high protein-specific activity (1–2 μCi/μg) and limited damage due to oxidation. Thyroid tissue was blocked using a saturated solution of KI in the drinking water (10 drops of SSKI/100 mL every 24 hours). Total activity per animal was between one and three μCi.
In these studies, 111In was used as the radiometal; modified DOTA molecules 9 being used as the chelator. Activity levels and concentrations were similar to values cited above for iodination. Both radiopharmaceuticals were purified using HPLC columns. All athymic mice had subcutaneous 100 to 300 mg LS174T human colorectal tumors (ATCC, Manassas, VA). Tissues taken for the biodistributions included the liver, spleen, kidneys, lungs, and tumor. Blood samples were also drawn.
Modeling approach
A modeling approach is proposed whereby loss of iodine is initially described in analogy with radioactive loss from the organs of interest. By this, we mean that, at a given time t, the measured ratio of tissue uptakes is represented by a quotient:
where a number of normal organs as well as LS174T human colorectal xenografts are studied in the athymic mouse model. If, in Equation (1), the ratio were that of uncorrected tissue uptake divided by uptake corrected for radiodecay, the result would be exp(-λt) with λ being the label's physical decay constant. By analogy, one may represent R by one of two lowest-order forms:
where r 0, r 1, and r 2 are amplitudes, while k 1 and k 2 (h−1) represent rate constants. It is seen that Equation (2) has two adjustable parameters, while Equation (3) has four. Notice that the set of equations is a nested one; Equation (2) being a special case of Equation (3). The latter represents the physical situation whereby the iodine loss is not monodirectional (as in the case of radiodecay) but may come back to the tissue of interest; for example, via the circulation. One would anticipate that the longer the biodistribution is carried out, the more likely a multiexponential is required to fit tissue data.
For each organ and tumor uptake ratio R, the ADAPT II algorithm 10 was used to obtain a fit of each of the two ratio equations. The Akaike information criterion 11 was used to decide which equality gave the better result for a given data set. This indicator combines residual sum of squares with the total number of free parameters in the model of interest. In using this index, the more negative Akaike values are to be preferred over less negative values. Notice that the iodine-based data are to be corrected by a factor of 1/R to obtain the comparable indium results. Thus, given measured iodine-biodistribution results and a relevant R value, one could predict the radiometal results—at least for indium. This is one possible application of the analysis presented here.
If we wish to compare one organ or tissue with another with respect to the rapidity of dehalogenation, a single parameter is preferred rather than the two or four parameter combinations of Equations (2) and (3), respectively. In the following, we use a mean residence time (MRT) approach.
12
Here, the derived R (t) function is used to determine a single characteristic time (in h) via:
Using Equation(4), one can readily compare, using the single MRT parameter, one protein's iodine loss with another's in a particular tissue or, given a tissue, to compare across a set of cognate proteins. If a MRT is relatively small, the conclusion is that the iodine is being rapidly cleared compared to another example with a longer residence time. Analyses outcomes in terms of fitting and resultant MRT values are shown below.
Results
Using Equations (2) and (3), biodistribution data were analyzed for the kinetic parameters of the R ratio. An example for liver analysis involving minibody and the intact mAb is given in Table 1. In both cases, the Akaike index was more negative for the double-exponential model, that is, the Equation (3) representation was preferred over that of Equation (2). Notice, however, that the MRT was approximately the same for both models indicating that the MRT concept was relatively stable with either one- or two-exponential fits.
N is the number of data points, M is the number of model parameters, and MRT is the mean residence time from Equation (4). For each antibody, the first row represents a single exponential fit; the second row represents the two-exponential fit.
Blood
By comparing blood curves for the four antibodies against CEA, it was found that no significant differences were seen between iodine-label and indium-label outcomes. This result proved useful as it allowed the rest of the analysis to go forward directly. If there had been a significant difference between these curves, one would have had to consider deconvolution of the various organ results before finding their iodine to indium uptake ratios (Fig. 1).

Value of the uptake ratios (R) in blood for the four cognate anti-CEA antibodies. Error bars represent one standard deviation. Some variation is seen, but the results are consistent with no dependence on the label. Because of relatively large errors, diabody blood curves are not shown beyond 6 hours.
Liver
From Figure 2, the R factor for liver decreased by essentially 50-fold by 24 hours in the minibody study. Similarly, relatively large hepatic corrections were seen for other cognates, including diabody, scFv-Fc, and M5A. The intact mAb, however, showed a loss of only a factor of three by 96 hours and was consistently higher than the ratio for the other three anti-CEA proteins.
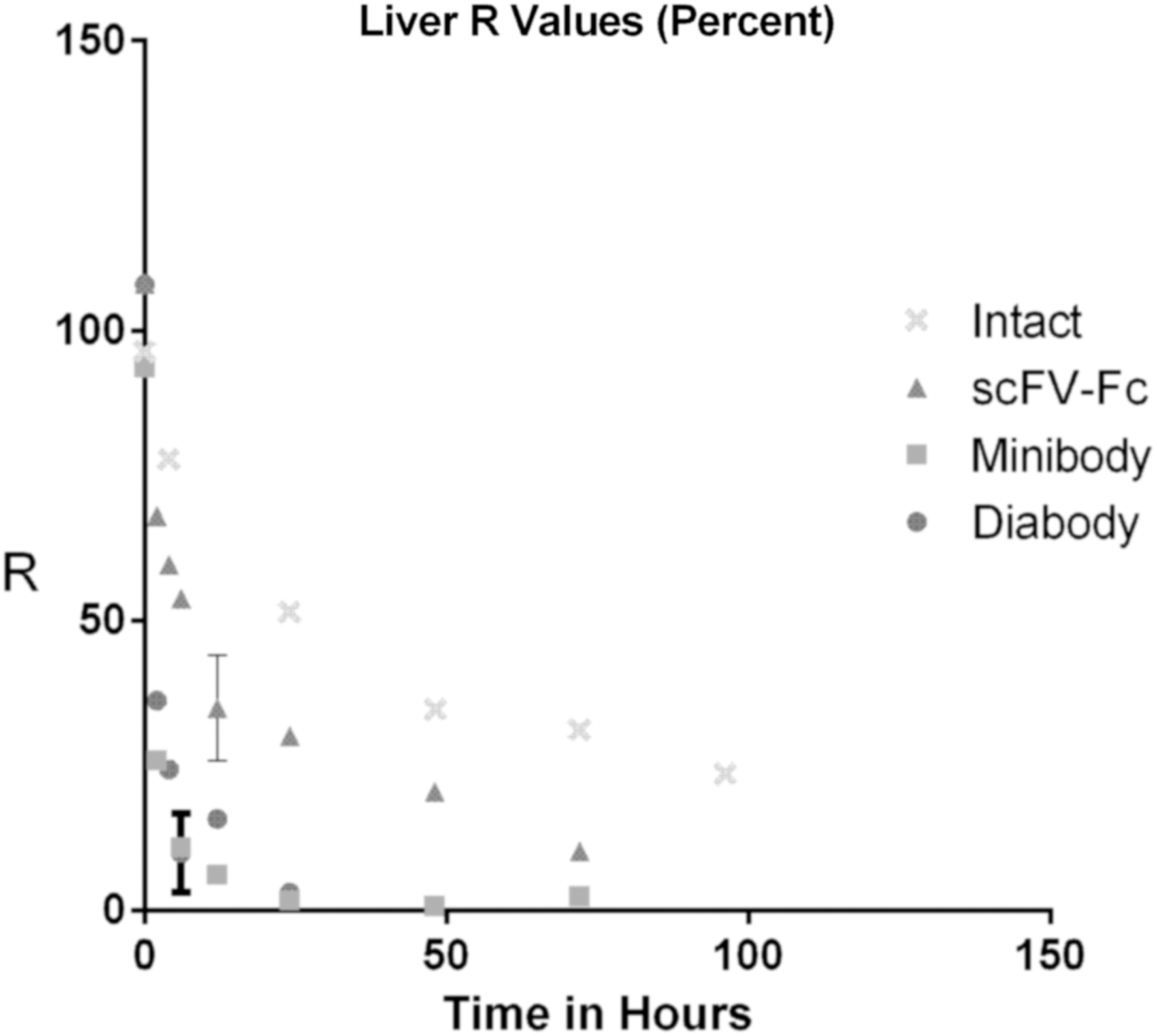
Value of the ratio of uptakes (R) in the liver for four cognate antibodies to CEA. Lower MW cognates showed increased iodine loss compared to intact M5A.
Spleen
Splenic results (Fig. 3) were similar to those in the liver. Again, the intact mAb showed the least loss of iodine (approximately one third) over a time frame of 96 hours. Lower MW cognates, such as the minibody, showed factors of 50-fold loss by 24 hours into the biodistributions.
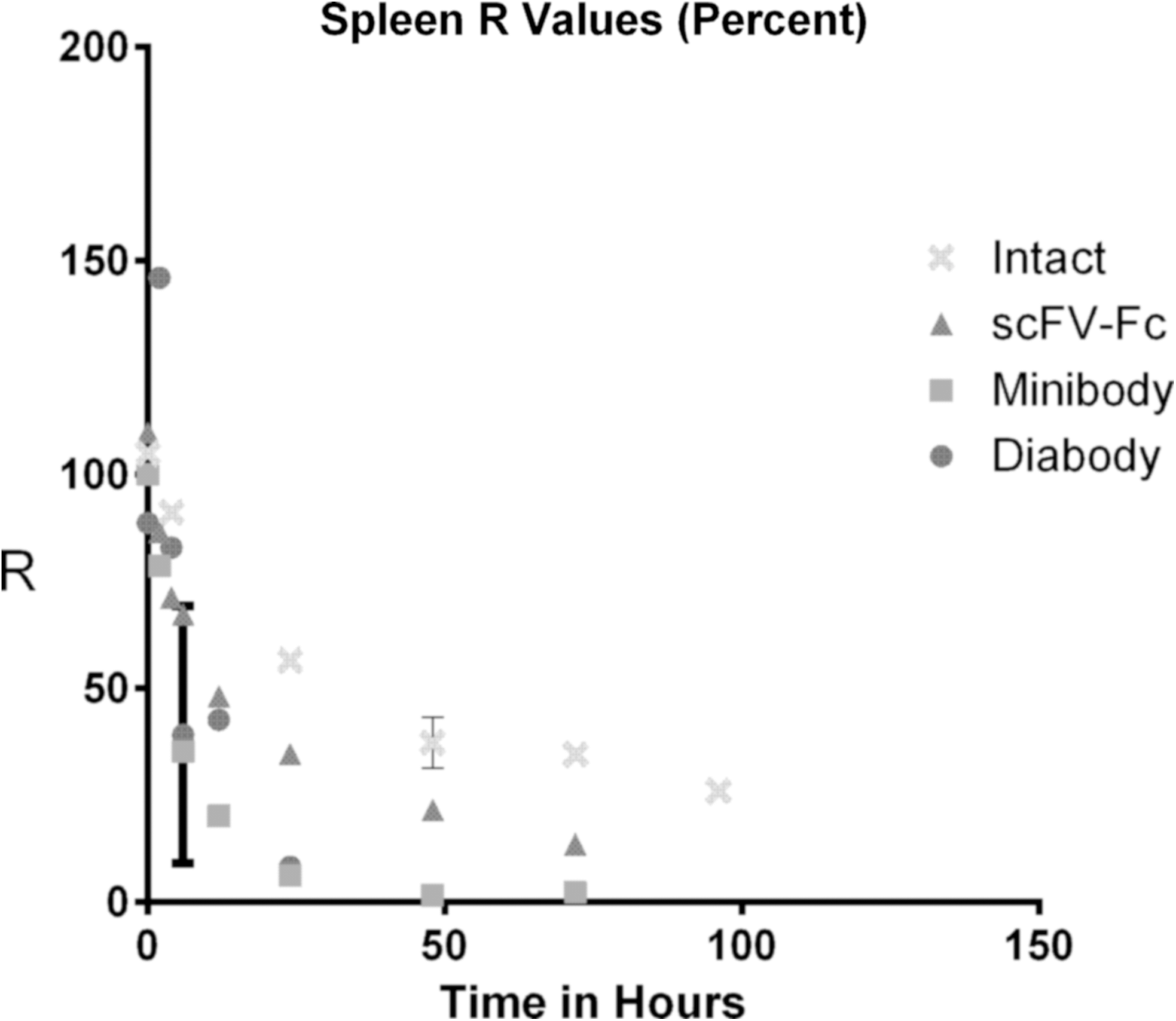
Value of the ratio of uptakes (R) in the spleen for four cognate antibodies to CEA. Notice that lower MW cognates show increased iodine loss compared to intact M5A.
Renal
The diabody and minibody showed the most rapid iodine clearance from the kidneys (Fig. 4). The former result is presumably associated with filtration of the diabody by the kidneys. Much longer times were observed for the scFv-Fc molecule I253A and intact M5A antibody. Larger MWs allowed the iodine to remain with the renal tissue. In this organ, the intact mAb had reduced iodine loss than that observed in liver and spleen; for example, iodine-labeled renal uptake being lower than the indium-based renal uptake by only 20% at 48 hours into the study.
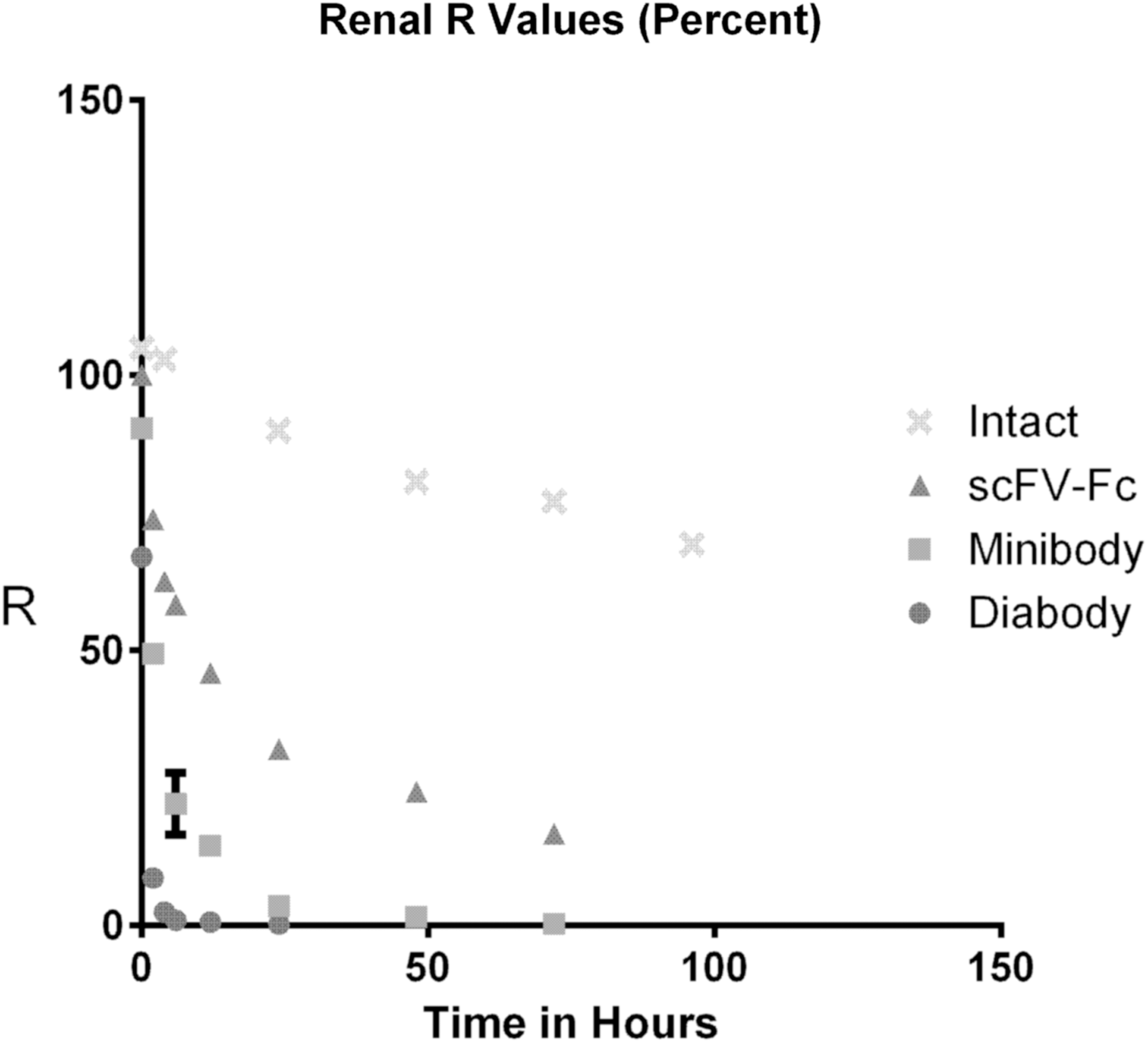
Value of the ratio of uptakes (R) in the kidneys for four cognate antibodies to CEA. The lower mass proteins showed increased iodine loss compared to intact M5A. Iodine loss in the case of the diabody is particularly marked; at 6 hours, iodine-labeled diabody uptake in the kidneys was only 1% of the indium-labeled renal uptake.
Lung
Figure 5 demonstrates the loss of iodine relative to indium in lung tissue. Both the I253A and intact mAb demonstrated iodine retention, in the intact case, only 15% of the label was lost out to 96 hours. Both diabody and minibody results showed relatively rapid clearance of the iodine label.
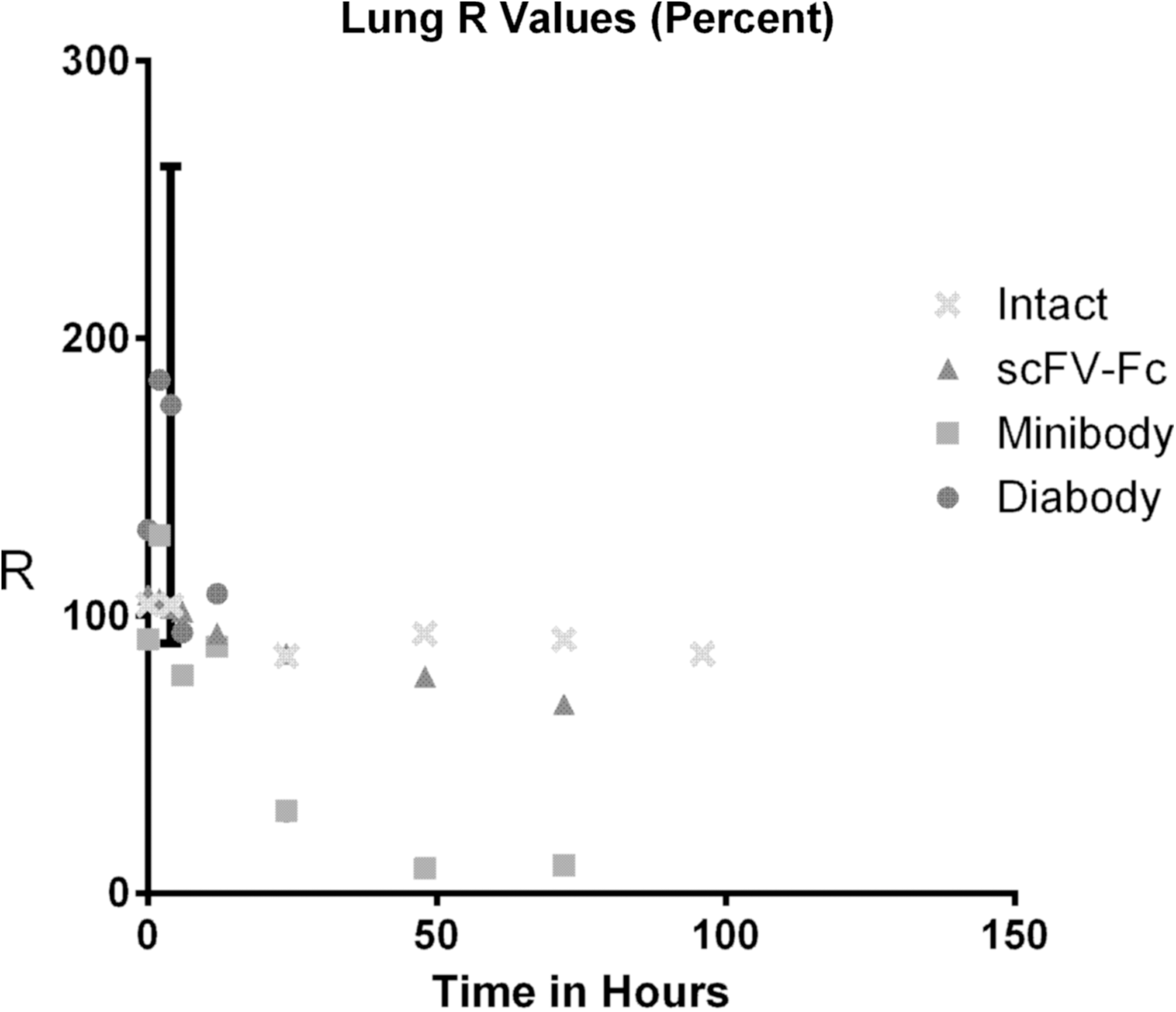
Value of the ratio of uptakes (R) in the lungs for four cognate antibodies to CEA.
Some evidence is seen for enhanced lung uptake (R>100%) of the iodine-labeled diabody protein at short times (t<24 hours). A similar result could be seen in the tumor data shown below. As both these results were the ratios of small numbers, the associated error bars were correspondingly large and the statistical significance reduced.
Tumor
Uptake in human colon tumor (LS174T) showed the most consistent difference between the two labels for all four cognate anti-CEA agents. By 48 hours, the R value approached 50%, that is, the iodine-based biodistribution uptake was approximately half that of the indium-based value for these lesions. This result was unlike any normal organ in that cognate MW did not have a demonstrable impact on accumulation in this tissue. Notice that the M5A dehalogenation was similar to that seen above in the normal organs (Fig. 6).

Value of the ratio of uptakes (R) in LS174T human colon xenografts for four cognate antibodies to CEA. All cognates demonstrated comparable iodine losses.
To relate the four cognates to each other and also over the normal and tumor tissues, a summary of MRT values is included in Table 2. Generally, the table shows that the R value increased with MW in any given tissue—including the LS174T tumor. For example, in the liver, MRT(R) went from several hours in the cases of diabody and minibody, increased to 23 hours for scFv-Fc and was 65 hours for the intact mAb. This variation was approximately a factor of 20-fold over the MW range of 56 to 150 kDa. In the colon tumor, the change in MRT was much less marked; going upward only by a factor of five over the same range of cognates. Thus, the dehalogenation process is dependent on cognate, tissue, and time.
Optimal least-squares fit to the R data were done with a single exponential, that is, Equation (2). Values in parenthesis indicate one standard deviation for representative calculations.
The most dramatic variation in R occurred for renal tissue where the diabody had a MRT value of essentially 1 hour, whereas the comparable intact mAb value was 300 hours. Variation in the lungs showed a similar behavior with low MW cognates having approximately 300 times faster clearance of the iodine label compared to the intact antibody. This difference may reflect a tendency for the intact mAb to have relatively little dehalogenation in the pulmonary system. Notice that the MRT of M5A in the lungs exceeded 6000 hours; this was the largest MRT value in the table.
Application and Discussion
Measurements have been made of the variations between iodine-based and indium-based biodistributions of four cognate anti-CEA proteins. It was found that the intact antibody showed the least difference between labels compared to its diabody, minibody, and scFv-Fc cognates. Using the MRT calculation, the ratio R of the iodine to indium uptake results was relatively more rapidly decreasing in the liver and spleen compared to kidneys and lungs. Renal clearance was, however, very rapid for the two lowest mass cognates (diabody and minibody) so as to produce MRT values on the order of only a few hours for the R ratio.
One important outcome of the R analysis was that the human LS174T colon tumor xenografts showed similar, relatively minor, dehalogenation results for all four cognates. Losses were only on the order of 50% by 48 hours. Without further investigation, it is unclear if this result was a consequence of the colonic origin of the tumor, malignant changes in the tumor itself or a combination of these and other factors. It was found that iodine loss in LS174T lesions for the intact antibody (M5A) was comparable to that seen in some of the normal organs, such as liver, spleen, or kidneys.
Investigators may assume that radiolabel is relatively unimportant in the determination of animal biodistribution results. From the above analyses, it is apparent that the choice of radiolabel type has a direct impact on any resultant (radiodecay-corrected) biodistributions. In a given normal organ, uptake differences of an order-of-magnitude or more could be seen between an iodine-labeled anti-CEA cognate and the same protein with an indium marker. These variations were also a function of time.
Given its manifest loss of radiolabel, it may be tempting to consider that any iodine-based biodistribution is inherently inferior to metal-based results. For example, it was seen that of the four normal tissues sampled, all demonstrated loss of iodine relative to indium. Yet the dehalogenation found in the tumor was relatively weak implying that the contrast between lesion and normal background tissues may be more striking for an iodine label. Thus, using iodination may lead to improved imaging and/or therapy of tumor sites. 13,14 The investigator may need to carefully investigate the differences between the two uptake results before making any final conclusions as to optimal labeling in a given application.
Using these measured uptake ratios, it may be possible to correct iodine-based murine biodistributions so as to estimate indium—or other radiometal based—results for cognate antibodies to CEA. Specifically, R values determined in the Figures 2 to 6 can conceivably be used to predict indium uptakes given a radioiodine-based result in a particular tissue. We therefore applied our technique to another intact anti-CEA antibody described previously by Koppe and co-workers. In that case, the label was 88Y for the metal-based results 15 and 131I for the iodinated MN-14 antibody. 16 Results at the same time points (24, 48, 72, and 96 hours) as the M5A data are shown in Figure 7 for four normal organs and LS174T colorectal tumor. Note that this is the same xenograft as examined above.
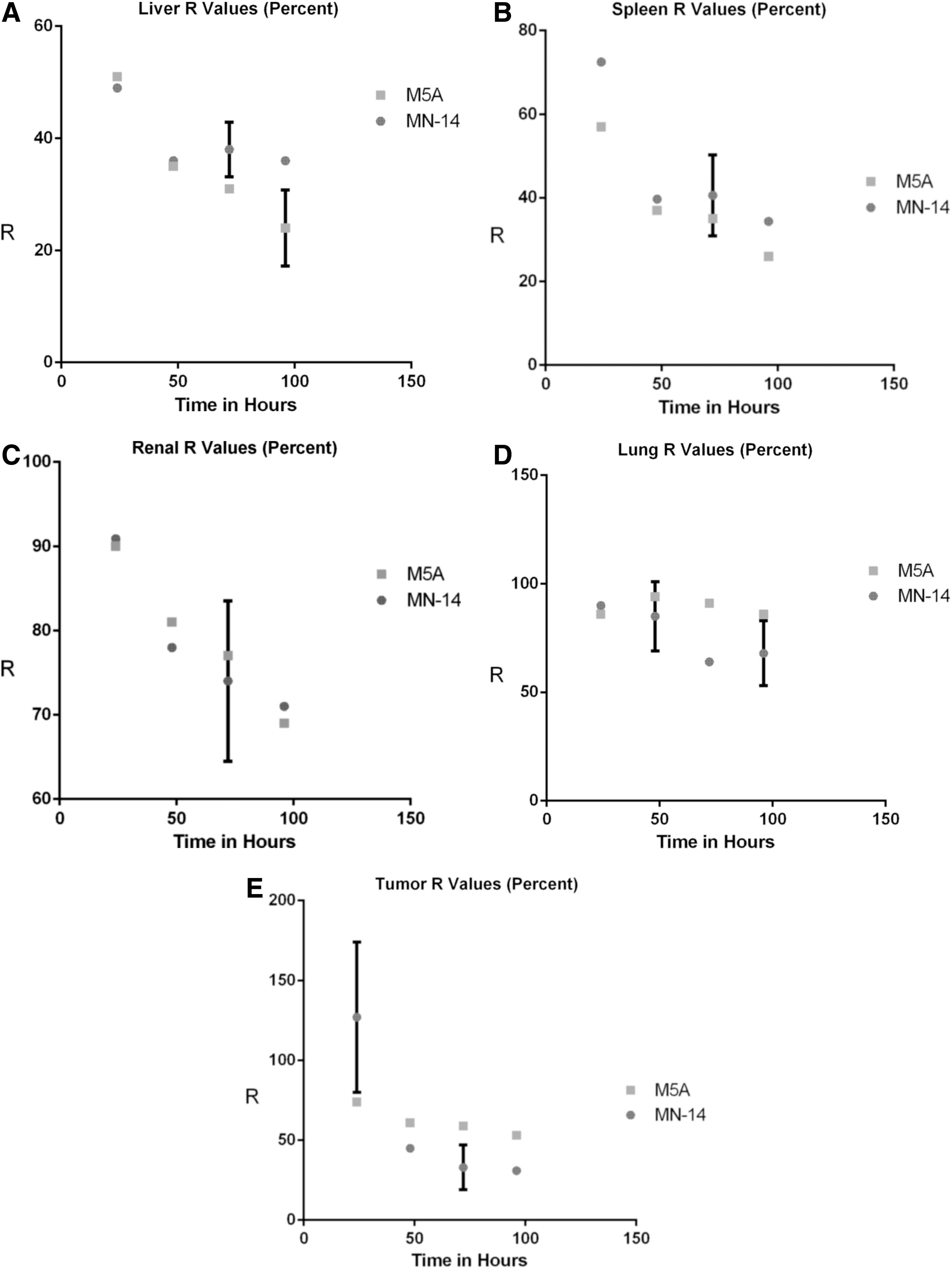
It was seen that the R value predicted by the corresponding organ or tumor M5A data sets was generally a reasonable estimate of the independently measured MN-14 R results. Notice that no adjustable parameters were used in these calculations. Agreement was particularly good for the kidneys with some divergence being seen at short times (24 hours) for tumor and for longer times (t>72 hours) for liver and lungs. In these cases, error bars were relatively large due to R being the ratio of small—and relatively uncertain—numbers. Other disparities between the Koppe et al. 15,16 and our M5A-based predictions could be due to variation in the chelate used as well as differing radiometal labels (88Y and 111In, respectively).
Conclusions
Ratios of iodine-based to metal-based biodistributions in athymic mice were measured for a set of four cT84.66 anti-CEA cognate antibodies. Normal organs, including liver, spleen, kidneys and lungs, were evaluated along with human LS174T colorectal tumor. Ratio values were found to be a function of MW, organ, and time. Generally, the smaller the MW, the faster the iodine label was seen to clear relative to the 111In label. Particularly rapid clearance occurred for the two lowest MW antibodies (diabody and minibody) for renal tissue. Tumor showed an R value that was essentially independent of MW and indicated a relatively slow dehalogenation process. Using our R ratios, we were able to predict, generally within errors, the corresponding uptake ratios for the same four normal organs and implanted human tumor for the MN-14 intact anti-CEA antibody. Thus, there is some confidence that the ratio method may be applied—at least to other intact mAbs in normal organs and in LS174T colorectal cancer xenografts.
It may also be possible to predict R values for proteins having MW values not directly observed in these analyses. The relatively continuous changes seen in the figures as the MWs varied imply that such interpolations may be reasonable predictors of the result for intermediate MW values. These results, however, depend on future experiments.
One other implication of the above analysis is worth mentioning. In some antibodies, there is the possibility that unlabeled (“cold”) agents can also effect tumor size reduction. Therapy in such cases generally involves giving a combination of both cold and labeled antibody. For example, tositumomab (Bexxar) 17,18 is known to reduce the number of B-lymphoma cells without recourse to radiation effects. If one were to model this therapy process using the iodine-based biodistribution of the material, it is important to recall that the radioiodine is being cleared in time as shown above. Thus, the actual amount of cold antibody at the tumor site and elsewhere would probably be better determined using 1/R. If the analyst were to look simply at the UI as seen by counting iodinated samples for radioactivity, the amount of unlabeled material being recorded would be underestimated. Those modeling therapy using such antibodies with iodine labels will need to take this effect into account.
Footnotes
Disclosure Statement
No competing financial interests exist.