
Abstract
Objective:
Few studies describe peptide receptor radionuclide therapy (PRRT) using 90Y- or 177Lu-labeled peptides in patients with recurrent meningiomas. No clinical data about 111In-Pentetreotide in such patients are available. We report on 111In-Pentetreotide therapy in patients with inoperable meningiomas and review the literature about PRRT of meningiomas.
Methods:
We reviewed clinical records of 8 patients with meningioma/meningiomatosis showing high 111In-Pentetreotide uptake on pretherapy scintigraphy who were treated with at least one cycle of 111In-Pentetreotide. In 2 patients, a cocktail of 111In-Pentetreotide and beta-emitting radiolabeled peptides had been administered.
Results:
No patient experienced acute toxicity, neurological or renal function impairment. Mild transient bone marrow toxicity was observed in 4 patients. Objective partial response was observed in 2 patients, stable disease in 5 and disease progression in one. There were no statistically significant correlations between objective response and patient age, tumor WHO grade, baseline Karnofsky performance score, 111In-Pentetreotide tumoral uptake grade, tumor/nontumor ratio, disease state at baseline, and cumulative dose.
Conclusions:
In consideration of its efficacy and the lack of significant toxicity, PRRT of meningiomas using 111In-Pentetreotide could be proposed even nowadays when the use of 177Lu- or 90Y-labeled peptides seems unsafe, namely in patients with renal impairment/toxicity.
Introduction
Meningiomas, the most frequent benign intracranial lesions, are well differentiated vascular tumors that usually grow slowly and have a low potential to be invasive; nevertheless, benign meningiomas could have an aggressive behavior and malignant subtypes can occur. 1,2 Meningioma recurrence is not rare—ranging between 2% (benign meningioma) and 78% (malignant meningioma) in patients with apparently complete surgical resection 3,4 ; moreover, complete resection is impossible in several cases because of the involvement of critical structures. Treatment options in patients with subtotally resected or recurrent meningiomas include external-beam radiation therapy (EBRT), stereotactic radiosurgery (SRS), boron neutron capture therapy (BNCT), chemotherapy, immunomodulation therapy, somatostatin therapy, and targeted molecular therapy.
In the last two decades, peptide receptor radionuclide therapy (PRRT) has gained greater importance as an alternative or complementary tool in the treatment of neuroendocrine tumors (NETs) and other somatostatin receptor-positive (sstr+) tumors. 5 With their high sstr density and location outside the blood-brain barrier, meningiomas represent ideal targets for treatment by radiolabeled somatostatin analogues. Few studies have been performed using 90Y- or 177Lu-labeled somatostatin analogues in meningioma patients showing recurrence after standard treatments. 2,6 –8 On the other hand, to the best of our knowledge, no clinical data are currently available about the use of 111In-Pentetreotide. The aim of this study is to report our experience with 111In-Pentetreotide therapy in patients with inoperable sstr+ meningiomas. Moreover, we reviewed the literature about PRRT of meningiomas.
Patients and Methods
We retrospectively reviewed clinical records of 8 patients (6 female and 2 male, mean age 58.5 years, range 50–81 years) who had been referred in the past years to the section of Nuclear Medicine of our University Hospital with a diagnosis of meningioma (6 patients) or meningiomatosis (2 patients) and had been treated with at least one cycle of 111In-Pentetreotide. Patients had been treated with 111In-Pentetreotide since other radiolabeled peptides were still unavailable or patients' conditions seemed incompatible with other treatments 9 ; in 2 patients, a cocktail of 111In-Pentetreotide and beta-emitting radiolabeled peptides had been administered. Patients' characteristics are summarized in Table 1. All patients had grade 2 to 3 tumoral uptake at 111In-Pentetreotide scintigraphy planar images (images acquisition procedure was in accordance with guidelines for 111In-Pentetreotide scintigraphy) 10 using the following four-point scale: lower than (grade 1), equal to (grade 2), or higher than (grade 3) normal liver tissue; or higher than normal spleen or kidney uptake (grade 4). 11 Visual analysis revealed tumor uptake clearly above skull uptake. More interestingly, median tumor/nontumor ratio (i.e., tumor/brain tissue ratio), evaluated by a standard ROI method on the 24 hours scan 12 in all patients, was 5.7 (range 2.9–9.1). Normal pituitary gland was not clearly visualized in any patient. Patients started PRRT no more than 30 days after 111In-Pentetreotide imaging (range 14–30 days, mean 22 days). Prerequisites for treatment were hemoglobin ≥5 mmol/L (≥8 mg/dL), white blood cells ≥3×109/L, platelets ≥75×109/L, creatinine ≤150 mmol/L (≤1.70 mg/dL), creatinine clearance ≥40 mL/min, in accordance with recent guidelines 13,14 ; Karnofsky performance status (KPS) in our patients was ≥40. For a better evaluation of renal function, glomerular filtration rate (GFR) value was estimated by renal dynamic scintigraphy before the beginning of PRRT; baseline GFR values in our patients ranged between 50 and 91 mL/min (median: 70 mL/min).
1=grade 1, lower than liver; 2=grade 2, equal to liver; 3=grade 3, higher than liver; 4=grade 4, higher than spleen or kidneys.
The patient died.
First and second cycles consisted of 111In-Pentetreotide (1.1 GBq)+90Y-DOTATOC (1.1 GBq) and 111In-Pentetreotide (3.7 GBq)+90Y-DOTATOC (1.1 GBq), respectively.
One cycle of 111In-Pentetreotide (4 GBq)+two cycles of 111In-Pentetreotide (3.7 GBq)+177Lu-DOTATATE (1.8 GBq) each.
F, female; M, male; PD, progression of disease; PR, partial response; PRRT, peptide receptor radionuclide therapy; RT, radiation therapy; SD, stable disease; Surg, surgery; WHO, World Health Organization.
Lesion volume evaluated by magnetic resonance (MR) imaging ranged between 1 and 70 cm3.
All patients had been treated with high therapeutic activities of 111In-Pentetreotide (two to four cycles, median three cycles, activity per cycle 1.1–7.4 GBq, median activity per cycle 7 GBq, cumulative activity range: 4.8–29 GBq). The therapeutic doses of 111In-Pentetreotide were obtained by adding, under aseptic conditions, 7.4 GBq of ultrapure 111InCl3 in a vial containing 30 μg of Pentetreotide. The average specific activity obtained was 247 MBq per μg Pentetreotide (i.e., 345 MBq/nmol). Labeling yields of more than 99% were routinely achieved. Patient #4 had been previously treated with six cycles of 90Y-DOTATOC (cumulative activity: 13.3 GBq) maintaining a condition of stable disease (SD); the patient had shown a mild impairment of renal function. 111In-Pentetreotide was associated with 90Y-DOTATOC in patient #5, and with 177Lu-DOTATATE in two PRRT cycles of patient #8 (Table 1). The interval between treatments was 6–10 weeks (average interval between treatment cycles: 8 weeks). To reduce the radiation dose to the kidneys, an infusion of aminoacids (25 g arginine and 25 g lysine in 2 L saline) was started 30 minutes before the administration of the radiopharmaceutical and lasted 4 hours. The radiopharmaceutical was administered via a second pump system in 30 minutes.
KPS evaluation was performed before each PRRT cycle and at follow-up visits every 2–3 months. Blood samples were evaluated every 15 and 30 days for 2–3 months following each cycle, to assess bone marrow, kidney, and liver toxicity. GFR value was estimated by renal dynamic scintigraphy every two treatment cycles. Toxicity was defined according to WHO criteria. 15
MR examinations were performed within 1 month before the beginning of therapy and every 2–3 months during and after PRRT.
Response was evaluated according to the Southwest Oncology Group (SWOG) criteria 16 : complete response (CR) was complete disappearance of all measurable lesions' diameters; partial response (PR) occurred when the sum of products of all lesions decreased by ≥50% for 3 to 6 weeks with no new lesions appearance; SD occurred when the sum of the products of all lesions decreased <50% or increased <50% for 3 to 6 weeks; and progressive disease (PD) occurred when there was a ≥50% increase in the sum of the products of all measurable lesions, or new lesions appeared.
Written informed consent was obtained from all patients before each procedure. Ethic Committee approval was not requested for this retrospective study.
Statistical analysis
The Mann–Whitney test and the Fisher's exact test were used to analyze statistical relevance of patient age, tumor WHO grade, baseline KPS, 111In-Pentetreotide tumoral uptake grade, tumor/nontumor ratio, disease state at baseline, and cumulative dose in determining better results. A p–value <0.05 was considered significant. Statistical analysis was performed using SPSS software version 12 (SPSS, Inc., Chicago, IL).
Results
No patient had acute toxicity or neurological impairment. No short- or long-term renal function impairment was observed. Mild bone marrow toxicity (transient leucopenia and/or thrombocytopenia grade I WHO) was observed in 4 patients (50%).
In 4 patients (50%) a significant improvement of clinical conditions (i.e., KPS) was achieved (Table 1). As far as objective response is concerned, PR was observed in 2 patients (25%) and SD was observed in 5 patients (62.5%), whereas PD occurred in 1 case (12.5%); namely, PR (Fig. 1) or SD was achieved by PRRT in 3 patients presenting with PD. One patient with poor clinical condition that had not responded to PRRT died a few months after, whereas in the other 7 patients, median follow-up duration from end of PRRT was 12 months (range 5–50 months). There were no statistically significant correlations between objective response and patient age, tumor WHO grade, baseline KPS, 111In-Pentetreotide tumoral uptake grade, tumor/nontumor ratio, disease state at baseline, and cumulative dose (all p>0.05).
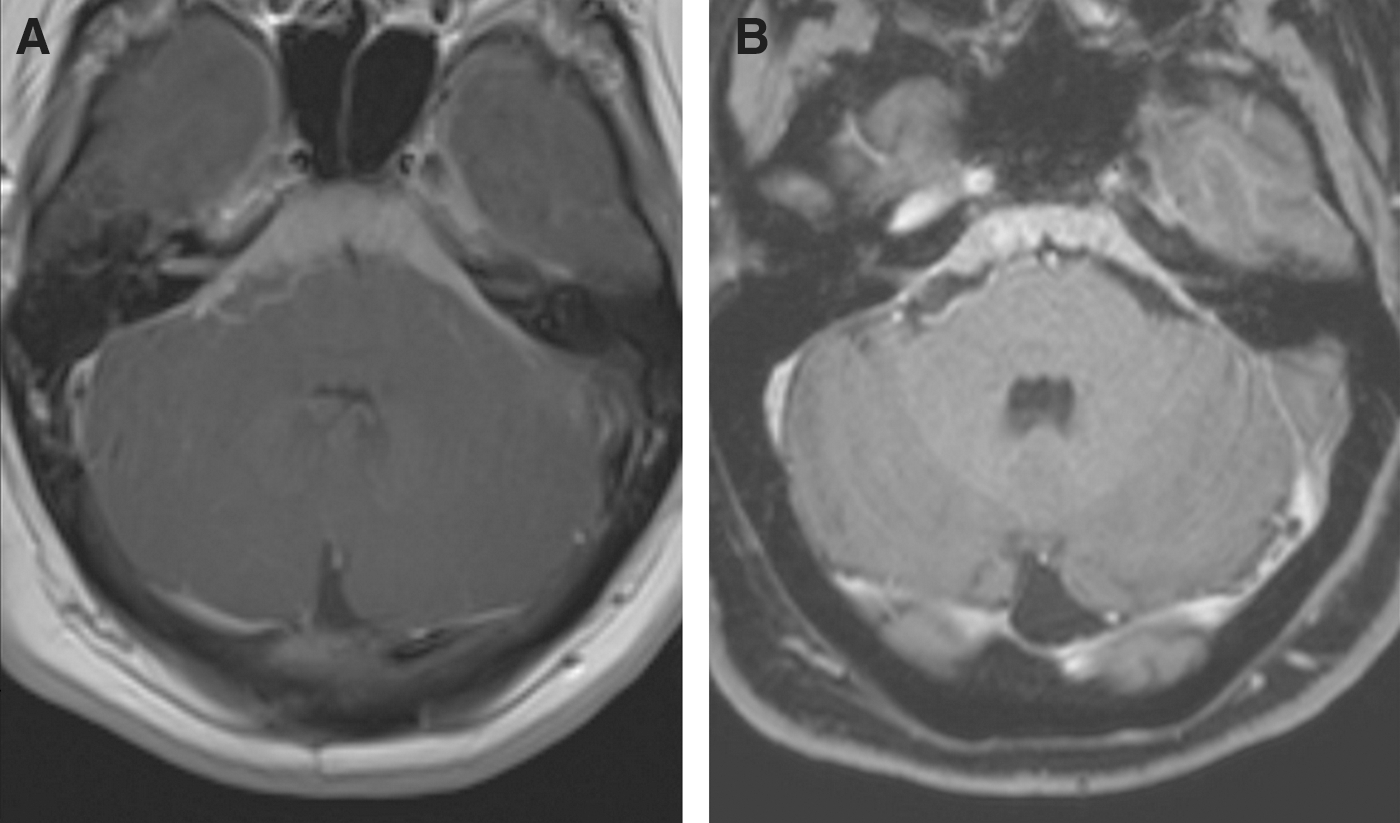
Contrast enhanced T1-weighted magnetic resonance images obtained before
Discussion
Meningioma recurrence is not rare, especially for WHO grades II (atypical meningioma) and III (malignant meningioma): in major clinical trials reporting patients with apparently complete surgical resection, 5-year recurrence rates for benign, atypical, and malignant forms were 2%–3%, 33%–50%, and 38%–78%, respectively. 3,4 When complete resection is impossible because of the involvement of critical structures (vascular or neural ones), clinical outcomes are less favorable. 2 If complete excision is not possible, options include definitive EBRT and partial excision followed by adjuvant radiotherapy. SRS has become an alternative option to EBRT for recurrent or partially resected meningiomas and for patients in whom surgery is not an option because of the tumor's location or patient comorbidities. 17 –21 BNCT is a binary radiotherapy that selectively and maximally damages tumor cells without harming the surrounding normal tissue: in a recent experience, malignant meningiomas seem to be good candidates for BNCT. 22
Various chemotherapeutic agents and immunomodulating therapy have been used, especially for recurrent atypical or anaplastic meningiomas, with no significant results. 23 Namely, multiple studies have investigated a variety of cytotoxic agents, including temozolomide, dacarbazine, adriamycin, ifosfamide, and irinotecan, all with disappointing results, 23 whereas treatment with hydroxyurea, an oral ribonucleotide reductase inhibitor, has shown contrasting results in the treatment of meningiomas refractory to surgery and radiation. 24 –28 In a recent retrospective study dealing with 60 patients, Chamberlain and Johnston reported very limited benefit from therapy with hydroxyurea: 35% of patients showed SD and 65% of them showed PD. 27 Moreover, a study evaluating combination therapy of hydroxyurea and radiotherapy provided no clear results to state whether this approach is better than radiotherapy alone. 29 Using immunomodulation therapy with interferon-α (IFN), a leukocyte-produced cytokine exerting antiangiogenesis effect and direct tumor cell inhibition, 30 Kaba et al. 31 and Muhr et al. 32 reported positive response, mainly SD, in 5/6 (83%) and 9/12 (75%) patients, respectively, without significant treatment toxicity. Moreover, in a recent prospective phase 2 study involving 35 patients with recurrent meningioma who started IFN therapy after radiology imaging had shown PD, Chamberlain and Glantz 33 reported that no patient had CR or PR [26 patients (74%) demonstrated SD and 9 patients (26%) had PD; median time to tumor progression was 7 months]. Furthermore, although no treatment-related deaths occurred, 3 patients went off study because of toxicity and 7 patients required a dose reduction.
In the last years, preclinical studies suggested that somatostatin, antiangiogenic drugs and mammalian target of rapamycin (mTOR) inhibitors may be of utility in the treatment of meningiomas. 34 –36 In the pilot in vivo prospective study, somatostatin achieved a significant radiologic response in patients demonstrating somatostatin receptor positivity on 111In-Pentetreotide scintigraphy (among 16 patients with recurrent meningioma, 31% of patients showed PR, 31% SD, and 38% PD) 37 whereas, in a recent phase 2 study, among 11 patients with recurrent or progressive meningioma enrolled without performing 111In-Pentetreotide scintigraphy and treated with subcutaneous octreotide, no patient experienced a radiographic response 38 ; namely, 11/12 showed PD. In 2010, Puchner et al. 39 first reported about a patient with substantial regression of an anaplastic meningioma after bevacizumab therapy; on the other hand, further studies on larger series showed less satisfactory results and the occurrence of serious toxicity (intracranial hemorrhage, intestinal perforation, and pneumonia/sepsis) in about 20% of patients. 35,40
In the last two decades PRRT acquired greater importance as an alternative or complementary tool in the treatment of NETs and other sstr+ tumors. Many experiences of PRRT using different radiopharmaceuticals, mainly 90Y and 177Lu (β-emitters) labeled peptides are reported in the literature and are very encouraging in terms of tumor regression, self-assessed quality of life, and overall survival. 5 With their high sstr density (especially subtype 2A), 2,41 –46 and location outside the blood-brain barrier, meningiomas also represent ideal targets for PRRT. Namely, meningiomas have been uniformly found to be positive for sstr, the receptor density reaching even more than 400 fmol/mg protein. 47 Moreover, a prominent expression of subtype 2 sstr also in endothelial cells of peritumoral blood vessels, 43 suggesting that PPRT may exert its action also through an antiangiogenic effect, and a correlation between sstr2A expression and the entity of neo-angiogenesis 48 have been demonstrated in meningiomas.
Only a few studies have been performed using radioactive somatostatin analogues in meningiomas treatment. Sabet et al. 8 reported the case of a 62-year-old female affected by intracranial anaplastic meningioma with pulmonary metastases presenting with progressive facial pain and treated with PRRT (three cycles of 177Lu-DOTATATE, cumulative activity: 691 mCi): the patient had no serious side effects and experienced a dramatic reduction of facial pain together with a significant improvement in quality of life; at 3 months follow-up she was considered in SD. Van Essen et al. 6 described 177Lu-DOTATATE therapy in 5 patients (cumulative activity up to 29.6 GBq) with high grade cranial or cervical meningiomas (2 patients had extremely large, exophytic, cranial tumors—1 of them also had cervical metastases—1 patient had a large, exophytic, cervical meningioma with rapid progression; 2 patients had a cavernous sinus meningioma) reporting PD in 3 patients and SD in 2. They proposed 177Lu-DOTATATE therapy in cases in which the disease is slowly progressive and other options are absent or are not considered effective. Moreover, they stated that if 177Lu-DOTATATE is given earlier in the course of the disease or in combination with other therapies, results could possibly be better. 6 Bartolomei et al. 2 reported about 29 patients with inoperable (n=3) or recurrent (n=26) meningiomas (14 grade I, 9 grade II, and 6 grade III) treated with 90Y-DOTATOC (cumulative activity up to 15 GBq); 20 patients had a single lesion whereas 9 patients had multifocal meningiomas. The authors reported SD in 19/29 patients (66%) and PD in 10/29 (34%), 3 months after PRRT. Better results were achieved in patients with grade I meningioma than in patients with grade II or III meningioma; namely, median time to progression (i.e., from PRRT) was 61 months in patients with grade I meningioma and 13 months in patients with grade 2 or 3 meningioma.
Moreover, the combination of EBRT and PRRT has been used in advanced cases, which is feasible and well-tolerated. Namely, Kreissl et al. 7 described 10 patients with inoperable or recurrent meningioma who have been treated with either 177Lu-DOTATATE (4 patients) or 177Lu-DOTATOC (6 patients) and external beam radiotherapy. EBRT dose was 42–60 Gy whereas the median tumor dose at each PRRT was 7.2 Gy (specific dose: 30–3890 mGy/GBq). CR occurred in 1 patient, SD in 8 patients, and PD in 1 patient. Moreover, authors reported that lesion volume after therapy, as estimated by PET/CT imaging, became 81%±21% of the baseline volume; mean time to progression was 13.4 months.
Our results are significantly better than those reported by both van Essen et al. and Bartolomei et al. and are comparable with results by Kreissl et al. The effectiveness of 111In-Pentetreotide in the treatment of intracranial benign tumor is not entirely new, since, recently, the first demonstration has been reported of the effectiveness of PRRT with 111In-Pentetreotide in a giant prolactin-secreting pituitary adenoma resistant to conventional treatments. 49 It can be related to the high and homogeneous expression of somatostatin receptors in meningiomas that allows Auger and conversion electrons (characterized by extremely short penetration range and high linear energy transfer) to obtain cytotoxic effect. Moreover, the higher specific activity of 111In-Pentetreotide than that reached by 90Y- or 177Lu-labeled DOTA-peptides and a lower injected mass of peptide 2,6,50,51 may be additional favorable features. In fact, increasing the mass dose of ligand or radioligand (i.e., the injected mass of peptide) will eventually result in a saturation of the receptors, since, in vivo, high affinity sstrs may be expressed at low capacity. 52 As a consequence, less of the administered radioactivity will bind to receptors and become internalized by receptor-expressing tissues and tumors. 53,54 Actually, the uptake expressed as percentage of the administered dose is a bell-shaped function of the injected mass. This finding might be the result of two opposing effects, (1) a positive effect of increasing ligand concentrations on the rate of internalization by ligand-induced receptor clustering and (2) a negative effect due to saturation of the receptor at increasing ligand concentrations. 54
Our retrospective analysis shows that PRRT with 111In-Pentetreotide is safe, well tolerated and effective on disease control in patients with meningiomas. Moreover, our results are better than that obtained in the majority of the reported series by using hydroxyurea, IFN, somatostatin, or bevacizumab.
It has been demonstrated that 90Y-labeled somatostatin peptide analogues may be responsible for development of severe permanent renal toxicity in a significant percentage of patients 55 and renal toxicity is one of the main limiting factors in treatment with 177Lu-labeled peptides 56 ; moreover, risk factors such as hypertension or diabetes represent further limitations in PRRT using 90Y- or 177Lu-labeled peptides. 57 On the other hand, no significant renal toxicity has been reported for111In-Pentetreotide even using high activities 58 –60 ; furthermore, limited or no renal toxicity was observed in published trials of 111In-Pentetreotide therapy without coinfusion of aminoacids. 59 Because of the lack of late toxicity reported for high cumulative activity of 111In-Pentetreotide, dose escalation studies in meningioma patients could be performed.
In consideration of its efficacy and the lack of significant toxicity, we think that 111In-Pentetreotide PRRT of meningiomas showing high 111In-Pentetreotide uptake on pretherapy scintigraphy could be considered even nowadays at least when the use of 177Lu- or 90Y-labeled peptides seems unsafe.
Other clinical experiences are needed to confirm our data; we are planning a dosimetric study on patients with meningioma/meningiomatosis treated by PRRT to evaluate specific doses to the tumor and to the surrounding structures to compare the different treatment regimens of PRRT.
Footnotes
Disclosure statement
No competing financial interests exist.