
Abstract
Molecular radiotherapy (MRT) with radiolabeled molecules has being constantly evolving, leading to notable results in cancer treatment. In some cases, the absorbed doses delivered to tumors by MRT are sufficient to obtain complete responses; in other cases, instead, to be effective, MRT needs to be combined with other therapeutic approaches. Recently, several studies proposed the combination of MRT with external beam radiation therapy (EBRT). Some describe the theoretical basis within radiobiological models, others report the results of clinical phase I–II studies aimed to assess the feasibility and tolerability. The latter includes the treatment of various tumors, such as meningiomas, paragangliomas, non-Hodgkin's lymphomas, bone, brain, hepatic, and breast lesions. The underlying principle of combined MRT and EBRT is the possibility of exploiting the full potential of each modality, given the different organs at risk. Target tissues can indeed receive a higher irradiation, while respecting the threshold limits of more than one critical tissue. Nevertheless, clinical trials are empirical and optimization is still a theoretical issue. This article describes the state of the art of combined MRT and EBRT regarding the rationale and the results of clinical studies, with special focus on the possibility of treatment improvement.
Introduction
The use of combined treatments is most applied in cancer therapy. Different techniques such as surgery, chemotherapy, and radiation therapies can have a synergic effect to eradicate or reduce tumoral lesions. The most recent literature offers interesting examples of studies combining different radiation therapy modalities, such as external beam radiation therapy (EBRT) and molecular radiotherapy (MRT) with radiopharmaceuticals. 1 –7 The potential benefits of this strategy are (1) to increase the efficacy of the treatment by a higher irradiation of the same solid tumor lesion, fulfilling the threshold limits of more than one critical tissue (both modalities aim at the same target volume but have different organs at risk (OARs); (2) to target solid tumors and disseminated disease; this offers the possibility to combine a local effect (from EBRT) to the effect of a systemic therapy (MRT), which is also potentially able to irradiate microscopic lesions not yet documented at imaging 2,4,7 ; (3) to deliver a high dose to subvolumes of a large solid tumor having an heterogeneous uptake of radionuclide, allowing an intensity-modulated radiation therapy (IMRT) plan to be made accordingly. The IMRT plan could cover the tumor volume receiving an inadequate absorbed dose or give a boost absorbed dose to volumes with high metabolism. 8
Considerations for a combined treatment may also apply to patients coming to MRT after other treatment options, including EBRT or vice versa. 2,9
Several authors have described the theoretical approach for a combined EBRT and MRT that includes radiobiological considerations about the normal organ tolerability and tumor control. 10 –13 This should represent a rigorous methodology for treatment optimization. 1 –7,9 –13 In contrast, to date, the majority of clinical studies aim to assess feasibility and toxicity and are not based on such theoretical rationales yet, but rather on empirical approaches. 2,4 –7,9 These approaches are, however, a source of relevant information for future perspectives.
The present work offers an overview of the rationale guiding the combination of EBRT and MRT and summarizes the main results of interesting clinical trials.
Methods
The implementation of combined therapies has to rely on the accuracy of each among several steps. Many factors contribute to the final quality of the dosimetric data, which is crucial in the attempt of relating the outcomes with the patient-specific therapy schedule. Image coregistration, which is necessary to correlate the information deriving from the two modalities, should be as accurate as possible to avoid any error propagation to the combined result.
EBRT planning and absorbed dose estimation are a common clinical practice characterized by a very high accuracy compared with MRT. In selected cases, information deriving from diagnostic SPECT or PET studies is used. 14 As opposite to this, 3D image-based dosimetry in MRT is not yet routinely applied in daily practice, although it is feasible.
Once acceptable accuracy of MRT dosimetry is assumed, the major issue becomes how to convert the MRT information into EBRT information or vice versa, given the very different characteristics of the two radiation modalities. MRT delivers the absorbed dose with a continuous decreasing absorbed dose rate, as a result of activity distribution and biological and physical decay, whereas EBRT delivers the absorbed dose in the time frame of few minutes in multiple fractions. As a result, the absorbed dose delivered by MRT can be much more heterogeneous than the one delivered with EBRT. Consequently, different biological effects are expected to occur for the same absorbed dose delivered with either modality.
The linear quadratic (LQ) model has been proposed in several studies to combine the absorbed doses from these two techniques through the biological effective dose (BED) concept.
10,11,13
Not only does BED take into account the amount of absorbed dose delivered, but also the time dependency of the delivery, in relation to the tissue response to the radiation injury. Thus, according to the hypothesis of the LQ model, the same biological effect is expected to occur for the same BED delivered with either modality.
3,12
The principal equations (eq.) of the radiobiological method are summarized as follows:
where SF is the fraction of cells surviving after irradiation; α/β relates the intrinsic radiosensitivity α to the potential sparing capacity (β); DEBRT is the absorbed dose delivered with EBRT in N fractions (absorbed dose per fraction: DEBRT/N), and DMRT is the absorbed dose delivered with MRT. G(∞) is the Lea-Catcheside factor
16
that accounts for a protracted radiation where repair of sublethal DNA damage can occur during irradiation. G(∞) is a function of the monoexponential repair constant μ:
where t and w are integration time variables.
17
More in detail, the term after the second integral sign refers to the first of a pair of double-strand breaks (DSB) required to produce a lethal lesion—the exponential term describing the reduction in numbers of such DSB through repair. Similarly, the term after the first integral sign refers to the second DSB, which can interact with DSBs produced earlier that still remain after repair. For MRT with monoexponential absorbed dose rate with an effective rate constant λeff, eq. 3 simplifies as:
The radiobiological parameters included in eq. 1 –5 are specific for the tissues and the effects. Typically, α/β ranges are 7–20 Gy and 0.5–6 Gy for acutely and late responding tissues, respectively. For example, α/β was estimated to be 2.96 Gy for prostate cancer, 18 15±2 Gy for liver cancer, 19 and 4±0.9 Gy for the lungs. 20 Most often, α/β values are assumed to be 10 Gy for tumors and 3 Gy for normal organs. The repair constant μrep can be, for example, 0.46 hour−1 (Trep=1.5 hours) for normal tissues and 1.3 hour−1 (Trep=0.54 hour) for tumors. 10
A generalized expression of BED for tumors includes the effect of repopulation that occurs during treatment and that concurs with cell kill, wasting some of the delivered absorbed dose.
21
Considering an exponential clonogen proliferation with doubling time Tav and an effective time of treatment T, a biological repopulation factor is being considered, so that eq. 3 becomes:
where T represents the time when the tumor cell killing rate equals the repopulation rate, so after T, the contribution to the BED from repopulation overcomes the BED from the radiopharmaceutical and the therapy is no more effective. 22
In case of spatial absorbed dose nonuniformity, the equivalent uniform biological effective dose (EUBED) has been defined for tumors and organs with parallel structure to represent the uniform biological absorbed dose, which would produce the same number of surviving cells. 23
It can be calculated to assess the possible radiobiological effect, according to the following equation:
where P(BED) represents the probability density function of BED and exp(−αBED) expresses the fraction of surviving cells SF. This applies in case of tumors or in case of functional subunits of parallel organs.
24
In practice, eq. 7a is often applied in a discrete form, dividing the volume of interest into subvolumes (voxels), to evaluate the absorbed dose at the voxel level. Eq 7a becomes eq 7b:
where N is the total number of voxels and BEDi represents the BED value within the voxel i.
In some cases of MRT, the equivalent uniform dose (EUD) can be a useful parameter.
3
It represents the absorbed dose given uniformly that will lead to the same effect as the actual nonuniform absorbed dose distribution and can be extrapolated by solving the following equation
3
:
This equation mirrors eq. 5 but accounts for nonuniformity. Similarly, EUD for EBRT can be derived as the solution of:
For a certain tumor BED (or EUBED in case of nonuniform absorbed dose distribution), the tumor control probability (TCP) is defined
25
for an initial number of clonogenic cells N0 as:
Concerning the risk of toxicity associated with MRT schedules, the phenomenological curves of normal tissue complication probability (NTCP)
26
derived from the EBRT experience can be used according to the following passages. The expression proposed to fit the EBRT absorbed dose–response data for a uniform irradiation of the whole organ is:
where D is the total absorbed dose, m is a parameter representing the steepness of the dose–effect curve, and TD50,5 is the absorbed dose value for which 50% of the population exhibited complications within 5 years for a uniform whole-organ irradiation.
When the organ is irradiated with a nonuniform absorbed dose distribution, with fractions of volumes vi uniformly irradiated with an absorbed dose Di (identifying the series {vi, Di}), the effective volume method is applied in EBRT for reducing the dose volume histogram (DVH) data to the unique parameter EUD.
27
The NTCP associated to the nonuniform absorbed dose distribution can thus be calculated from eq. 11 and eq. 12 assuming that the whole organ is uniformly irradiated with an absorbed dose equal to EUD. The parameter EUD is defined as:
where n is the volume–effect parameter (e.g., n=0 for serial organs, 0<n<1 for serial-parallel organs).
To apply the same model in case of uniform MRT irradiation, the BED values from MRT need to be converted into the EBRT absorbed doses yielding the same biological effect (EQDX). 28
Such values are the suitable input data for eq. 11 and 12. When performing the above conversion, the same EBRT fractionation schedule must be considered as the one applied to the absorbed dose data used to derive the experimental NTCP curve. For example, in case of 2 Gy/fraction scheme, the EQD2 parameter can be calculated according to eq. 14:
Similarly, in case of nonuniformity, the {vi, BEDi} series derived from MRT can be converted into a series {(vi, EQDXi)}, which is the input for eq. 13 to derive EUD and then apply eq. 11 and eq. 12.
A summary of the studies describing a combined therapy with MRT and EBRT is reported in Table 1.
MRT, molecular radiotherapy; EBRT, external beam radiation therapy; LQ, linear quadratic; 131I-mIBG, 131I-metaiodobenzylguanidine; 153Sm-EDTMP, 153Sm-ethylene diamine tetramethylene phosphonate; IMRT, intensity modulated radiation therapy; OAR, organs at risk; 90Y-IT, 90Y-ibritumomab tiuxetan; PPRT, peptide receptor radionuclide therapy.
Examples Where the LQ Model Is Applied
The methods described above propose a useful guide to integrate different radiation modalities. To date, these have been applied to show a theoretical advantage from a combined approach or when a rationale was preferred to empiricism to build a clinical protocol. In the following section, the most representative examples from the literature, in which the LQ model is applied, are illustrated. It must be considered that these methods still remain theoretical models that need to be validated with clinical trials.
(1) In an article by Bodey et al., 10 hypothetical EBRT treatment planning was prepared for 3 patients who underwent MRT. Absorbed dose and BED distribution maps were obtained for each therapy separately (MRT and EBRT) and for their combination. The absorbed doses from MRT were converted into corresponding absorbed doses for EBRT schedule, using the LQ model. The DVHs of EBRT alone or of the combined therapies were compared for the tumor and the OARs. For example, for a patient affected by retroperitoneal neuroblastoma and treated with 131I-metaiodobenzylguanidine (131I-mIBG) (33 GBq), the EBRT treatment planning with three isocentric wedged fields was considered, delivering an absorbed dose of 60 Gy to the isocenter. For the combined therapy, the EBRT contribution was scaled to deliver, overall, the same minimum absorbed dose to the clinical target volume (CTV) as with EBRT alone. In this patient, the OARs was the left kidney. The analysis of the DVHs (Fig. 1) highlighted the advantage of the combined solution for both the CTV and the kidney. The mean absorbed dose ratio between kidney and CTV was 0.40 versus 0.16 for the EBRT alone versus the combination.
(2) Another study by Hobbs et al. 1 applies the equations of the LQ model in search of therapy optimization for a patient with osteogenic sarcoma enrolled in a protocol of high-dose 153Sm-ethylene diamine tetramethylene phosphonate (153Sm-EDTMP). Although the patient did not receive the treatment, the treatment planning of 153Sm-EDTMP and subsequent IMRT was studied as interesting case. A baseline IMRT (with 2 Gy/fraction) treatment plan was designed to deliver an absorbed dose of 30 Gy to 90% of the paraspinal tumor voxels while minimizing the absorbed dose to the spinal cord. For MRT, the tumor volume was delineated on CT images. SPECT images were corrected for attenuation, scatter, collimator detector response, partial volume effect, and coregistered with CT. These were input of the 3DRD software for dosimetry evaluations with the Monte Carlo simulations. BED maps for MRT were converted into absorbed dose maps of EBRT, and the relative contribution of EBRT was established by a factor such that the highest voxel total absorbed dose in the spinal cord involved fulfilled the constraint of 50 Gy. With the administered activity of 16.7 GBq, the average absorbed doses from MRT were 22.6 Gy to the tumor and 3.9 Gy to the spinal cord. For an IMRT treatment plan obtained by scaling the baseline plan to the maximum tolerable absorbed dose (MTD) of 50 Gy, the average absorbed doses were 54.6 Gy to the tumor and 18.6 Gy to the spinal cord, respectively. The evaluations revealed the advantage of the combined treatment, with an average value of 71.5 Gy to the tumor and 20.6 Gy to the spinal cord.
(3) A new procedure called IART® (intraoperative avidination for radionuclide therapy) was recently used in patients with early breast cancer undergoing conservative surgery. 29 The purpose of this therapy is to irradiate the residual mammary gland immediately after the surgery to give an anticipated boost to the tumor bed. It consists of the administration of 3.7 GBq of 90Y-biotin to be combined to a shortened course of EBRT. On the basis of planar imaging data, the LQ model was used to calculate the equivalent effect of that administered activity compared to the EBRT fractions replaced by IART. A phase I–II study assessed the tolerability on 35 patients treated with IART followed by an EBRT treatment (40 Gy, 2 Gy/fraction). 29 In this cohort, only 1 patient relapsed at 5 years post-treatment, but larger series should be considered to conclude the equivalence of IART plus EBRT versus standard EBRT. The study by Ferrari et al. 3 retrospectively performed a 3D voxel dosimetry analysis in 14 IART patients, according to the methods described in the Methods section, to investigate the possibility to improve the integration with the EBRT modality. Dose–volume and BED–volume histograms were generated to derive EUBED and EUD values for IART. The number of EBRT fractions that would cover the same EUBED produced by IART was calculated, and a median value of 9.5 (7.2–13.3) fractions was found. This indicates that the IART procedure allows to spare about 2 weeks of EBRT at 2 Gy/fraction. Following this methodology, a patient-specific evaluation can be performed to calculate the number of subsequent EBRT fractions needed to deliver a prescribed total absorbed dose. 3 Moreover, it was possible to compare the TCP curves as a function of time (eq. 11) for the combined treatment of IART followed by reduced EBRT (40 Gy to the mammary gland, 2 Gy/fraction) versus standard EBRT (40 Gy to the mammary gland plus a boost of 20 Gy to the tumor, 2 Gy/fraction). Figure 2 shows the advantage of a boost delivered immediately after the surgery. From the graphs, it is expected that the combined therapy would offer the same, even anticipated, tumor control of the standard treatment, with the advantage of avoiding ∼10 sessions of EBRT.
Feasibility Studies
Besides the previous studies, the literature offers several clinical trials that are of great interest despite the fact that they do not rely on a robust rationale but rather on empirical background. They are essentially studies of feasibility and/or tolerability or retrospective studies, which use standard and/or empirical protocols for EBRT and MRT. Typically, they include a limited number of patients. MRT is provided with fixed activities (the “one fits all” concept), or activities corrected per body weight or per body surface area, so that the resulting absorbed doses from MRT are not personalized. Dosimetry evaluations for MRT are not always performed, and radiobiological models are not considered. Nevertheless, these studies represent a rich source of information for future individualized planning. The examples that follow show the wide range of potential applications and open the way to prospective optimized studies.
153Sm-EDTM, bone metastases
A prospective clinical trial described by Baczyk et al. 6 compared the analgesic effectiveness and toxicity of monotherapy with 153Sm-EDTMP to combined therapy of 153Sm-EDTMP followed by EBRT. Eighty-eight patients affected by metastatic prostate cancer with at least three bone lesions were included. The administered activity of 153Sm-EDTMP was 37 MBq/kg, and different EBRT schedules were applied after 3–14 days (8 Gy×1 fraction; 4 Gy×5 fractions; 3 Gy×10 fractions). Unfortunately, dosimetry was not performed, and the impact of the different EBRT and 153Sm-EDTM absorbed doses could not be taken into consideration. The results indicated that combined therapy did not intensify the toxicity (irrespective of the EBRT absorbed dose) and was more effective than radionuclide therapy alone.
Peptide receptor radionuclide therapy, meningiomas
In a study by Kreissl et al., 4 the feasibility and tolerability of a combination of peptide receptor radionuclide therapy (PRRT) with EBRT was assessed in 10 subjects affected by unresectable meningioma, previously studied with 68Ga-DOTATOC/DOTATATE PET to confirm a high expression of somatostatin receptors. For safety reasons, patients were administered with one cycle of 177Lu-DOTATOC/DOTATATE with an activity of 7.4±0.3 GBq. Two to 9 days after MRT, EBRT with IMRT technique was delivered, with a schedule individualized according to clinical considerations to avoid possible toxicity. The median tumor absorbed dose from MRT was 7.2 Gy (0.2–30.6 Gy). The median tumor absorbed dose (D95) from EBRT among patients was 53 Gy, ranging from 40 to 60 Gy with 1.8–2 Gy/fraction, and a limit of 54 Gy was set to the optic organs. In 4 patients, the EBRT absorbed dose to the target was reduced because of concerns to the optical nerve due to the summation of absorbed doses. It is to be noted that absorbed doses were simply summed without considering DVH or the BED formalism. However, this study showed the feasibility and tolerability of PRRT and EBRT combination, as well as the typical large variability of absorbed doses delivered with PRRT. The choice of 177Lu instead of 90Y spared the cranial nerves.
131I-mIBG, pheochromocytomas and nonhead and neck paragangliomas
The role of EBRT in the management of patients with malignant pheochromocytoma or nonhead and neck paraganglioma is controversial. Fishbein et al. 5 have described sequential 131I-mIBG (2 mCi/kg per two treatments) and EBRT in 5 patients affected by these tumors. The 131I-mIBG scan was used to assist the EBRT planning. The dose-limiting toxicity for 131I-mIBG was hematologic while IMRT was used to spare the peritumoral normal tissues (bone marrow and bowel in the cases considered). Two to 6 Gy/fraction schemes were applied for a total EBRT absorbed dose ranging from 30 to 54 Gy. Areas irradiated with EBRT showed durable objective response, whereas out-of-field systemic progression required other treatments. The results showed that EBRT can be highly effective in local management of malignant paraganglioma and can be used with 131I-MIBG due to nonoverlapping toxicities with excellent control of locally bulky tumors.
Radioimmunotherapy, follicular lymphoma
The strategy of combining EBRT with radioimmunotherapy (RIT) with 90Y-ibritumomab tiuxetan (90Y-IT) was applied by Burdick et al. 2 in patients with relapsed or refractory bulky (>5 cm) follicular lymphoma. This was done in the attempt to improve therapeutic response, as bulky disease is known to be resistant to RIT. In a group of 11 patients, a shorter regimen of 24 Gy given in 8 fractions (vs. a standard of 40 Gy delivered in 2 Gy/fraction) was planned to reduce the time interval before 90Y-IT, which was set after complete recovery of standard hematologic functionality. As a result, with α/β=10 for lymphoma, the BED was 31.2 Gy compared with the standard 48 Gy. 90Y-IT (11–15 MBq/kg) was administered after the recovery of blood counts (median: 55 days) and after the biodistribution analysis with 111In-IT. However, no dosimetry evaluations were reported for RIT. An overall response rate of 64% with no relapse within the EBRT field confirmed the efficacy of EBRT to pretreat bulky sites before 90Y-IT. EBRT followed by 90Y-IT did not show any relapse of bulky disease, thus reaching 100% local control, with a median progression-free survival of 18 months. It was concluded that the combined treatment might improve clinical outcomes and extend survival. Whether the short regimen of EBRT and the time interval between 90Y-IT and EBRT were appropriate remains to be established.
RIT, brain metastases
RIT with 131I-L19SIP (4.1 GBq/m2) in addition to whole-brain radiotherapy (30 Gy in 10 fractions) has been proposed by Poli et al. 7 in 6 patients affected by multiple brain metastases from solid cancer, who received whole-brain irradiation with 10 fractions of 3 Gy each. Patient eligibility was decided based on a previsional dosimetry evaluation with 124I-L19SIP to guarantee that absorbed doses to the red marrow remained within 2 Gy. RIT showed a wide variability of absorbed doses to the brain lesions (median 0.38; range 0.10–1.37 Gy/GBq) as well as to extracranial lesions (median 1.41; range 0.15–5.38 Gy/GBq), leading to 2.4 Gy (0.7–8.1 Gy) and 7.3 Gy (1.1–35.8 Gy), respectively. The study evaluated the tolerability of the treatment and posed the basis for future optimization of the combined therapy, also in consideration of the variability of the absorbed doses from RIT that could lead to exclude patients with too low uptake.
Radioembolization, liver lesions
The safety of the radioembolization (RE) of liver lesions with 90Y microspheres in 31 patients who came for RE after previous EBRT has been retrospectively studied by Lam et al. 9 No particular details of the EBRT techniques used were described, but the DVHs for the EBRT planning were analyzed. RE using resin or glass spheres was administered with empirical methods according to the manufacturer's protocols. No DVHs for RE were considered. For EBRT, the mean absorbed doses to the nontumoral liver was 4.4 Gy (0–23 Gy); for RE, the mean absorbed dose to the liver was 58 Gy (27–149 Gy). Patients who experienced hepatotoxicity (grade II or higher, 39% of cases) received higher EBRT absorbed doses to the liver, with also a trend of higher cumulative (EBRT+RE) absorbed doses. Two patients, who had fatal RE-induced liver disease (REILD), received the highest absorbed doses for EBRT (21, 23 Gy) and RE (92, 149 Gy). A multivariate analysis indicated the EBRT absorbed doses as the only independent predictor of toxicity. The fraction of liver exposed to at least 30 Gy (V30) was, in fact, the strongest predictor of toxicity, with a threshold for hepatotoxicity at a volume of ∼10% and a threshold for fatal REILD at a volume of ∼30%. Nevertheless, definite thresholds for safe RE after EBRT were not established. It is concluded that the dose–response relationship for hepatotoxicity after RE remains unclear, owing to the uncertainty of the RE absorbed dose distribution in comparison with EBRT and that the liver tolerates a much higher mean absorbed dose from RE in comparison with RT, likely because of the inhomogeneity of microsphere distribution. However, it has to be pointed out that the authors' conclusions could be strongly influenced by the unbalance between dosimetry information deriving from EBRT and RE. In any case, this article gives evidence that accurate dosimetry is indispensable also in RE and is a precious information for subsequent analysis.
Other Interesting Applications: Combination of Radionuclides in MRT
Although methodologically different from schedules integrating EBRT and MRT, the combination of two different MRTs has some merit in relation to the aim of this article. The basal concepts are the same as those presented in the Methods section for EBRT+MRT, but the in-depth analysis suggested by some authors illustrates the possible optimization. The rationale is to use more than one radionuclide, labeled to a single agent or to two different agents, to increase the efficacy of the treatment itself. The combination of two radionuclides may, in fact, target a wider range of tumor diameters (e.g., ∼1 mm with 131I and 177Lu, ∼3–5 mm with 90Y), 30 and two different radiopharmaceuticals can have orthogonal toxicity (as often occurs for MRT and EBRT combinations). Clinical trials are emerging especially for PRRT. 31 –33 However, the activity ratios are still chosen on an empirical basis. Other studies have been proposed as theoretical models, 15,34,35 with the primary aim of leading to an optimization of the administered activities of the two radiopharmaceuticals, A1 and A2, to maximize the TCP, without exceeding the MTD and BED to the OARs.
In particular, the study by Hobbs et al. 15 for the myeloablative treatment of non-Hodgkin lymphoma (with 131I-Bexxar and 90Y-Zevalin) and the study by Walrand et al. 34 for the treatment of neuroendocrine tumors (with 177Lu- and 90Y-DOTATATE) are here considered for their “complementary” nature. Indeed, the first one develops the mathematical framework to calculate, for a fixed absorbed dose or BED to one or more OARs, the maximum injectable activity of two radiopharmaceuticals that ensures the maximum absorbed dose to the tumor; the second develops a challenging tumor model to simulate homogeneous and heterogeneous radionuclide uptake. The principal take-home messages are here summarized.
Focus on the OARs
Considering two radiopharmaceuticals, and indicating with d1,OAR1 and d2,OAR2 the absorbed doses per unit injected activity for the corresponding OARs, and with MTDoar1 and MTDoar2 the corresponding MTD values, the following system of linear equations should be solved for A1 and A2:
Moreover, indicating with (d1,tum, d2,tum) the absorbed doses to the tumor, for all the couples A1, A2 that are solutions of the above system, the absorbed dose to the target is derived by:
The maximum Dtum provides the most effective combination of A1 and A2. A counterintuitive result is found: the activity providing the highest safe absorbed dose for the OARs does not necessarily deliver the highest absorbed dose to the target.
Focus on the tumor
In PRRT, tumor radionuclide distribution depends on the receptor density distribution and on the vascular tumor system and is generally far from homogeneous. The spectrum of the radionuclide could play a major role in determining the tumor control. To get more quantitative insight, Walrand et al. 34 depicted tumors as small radioactive-filled spheres (ø 1–25 mm), containing smaller cold spheres (ø 1–7 mm) representing heterogeneities, that is, areas that do not take up activity. They supposed to have one single OAR, the kidneys, and two radionuclides, for example, 177Lu and 90Y to label a peptide, as it is common in PRRT for neuroendocrine tumors. The situation is the same as described by eq. 16 and 17. For each couple A1, A2 and each tumor, the authors calculated the EUD and the TCP, using published parameters for the radionuclide kinetics into the tumor and the kidneys, and fixed the tumor/nontumor specific activity. Some of the interesting findings that emerged are as follows: 177Lu alone cannot even control 1 mm heterogeneities, irrespective of the tumor-specific activity; 90Y alone cannot even control homogeneous tumors smaller than 6 mm in diameter. With the typical kinetics and uptake considered, an injected activity according to the proportion 80% of 177Lu-peptide, 20% of 90Y-peptide would constitute the best balance because it allows controlling homogeneous tumors down to 2 mm in diameter and cold areas up to 3 mm in diameter.
Discussion
The review of the literature highlights that combined treatments of EBRT and MRT are rapidly evolving and represent a new promising option. Many applications have already been proposed, embracing the treatment of meningiomas, paragangliomas, bone lesions, osteosarcomas, non-Hodgkin's lymphomas, brain, hepatic, and breast lesions, all showing tolerability and improved outcomes. Two main results emerge from the analysis of the body of information described.
The first one is that combined treatments can be more advantageous than a single radiation modality, delivering higher absorbed doses to the target and minimizing the irradiation of critical organs. Since different therapies usually have different OARs, the properties of each treatment modality can be fully exploited. The implementation of special EBRT techniques (such as IMRT) can be designed to complement the typical inhomogeneous absorbed dose distribution of MRT and the wide variability of patient activity uptake, thus potentially increasing the efficacy of the combined result. 3 Moreover, the systemic action of MRT can treat possible microscopic lesions.
The second finding of this analysis is that clinical trials to date are phase I–II studies, in the majority of cases based on empirical approaches. Since EBRT and MRT combination is a rather new approach, the exploration of the toxicity profile seems a correct initial approach. However, optimization is possible and should be incorporated in future steps. In some cases, the potential of combination has not been fully exploited because of the low administered activity (activity escalation concept). This is the case of the study by Kreissl et al. 4 where, to preserve safety (empirically established), only one cycle of 7.4 GBq of 177Lu-DOTATATE/DOTATOC has been conceived (vs. the usual four cycles). Regarding optimization, difficulties rise from the fact that only a few studies report MRT dosimetry, while details of EBRT dosimetry are always available in the centers. This applies, for instance, to the study by Burdick et al., 2 where 90Y-IT is regarded as a sort of chemotherapy (i.e., no absorbed doses reported). Therefore, an estimation of the relative contribution from MRT and EBRT to the 100% local control reached is not possible. In an article by Lam et al., 9 there is an imbalance between the accurate 3D data from EBRT dosimetry, with DVH analysis, and the simple evaluation of mean absorbed doses in RE, where no distinction between tumor and nontumoral liver is adopted. The inclusion of the absorbed dose distribution of RE and considerations from radiobiological models could have offered, instead, important information that would have possibly led to different conclusions about thresholds for toxicity. A discrepancy between EBRT and MRT 3D absorbed dose evaluations plays against a better understanding of the therapy outcomes.
The encouraging results of the trials here mentioned the improvements of internal dosimetry accuracy, and the mathematical framework already identified (see examples by Bodey et al., 10 Hobbs et al., 1 and Ferrari et al. 3 ) requires future prospective studies to pursue optimization. Clinical trials must include an accurate 3D MRT dosimetry to be integrated with EBRT dosimetry. This would allow verifying the predictivity of the proposed models or the need of specific corrections. Reading the articles by Baczyk et al. 6 (88 patients, no MRT dosimetry) and by Hobbs et al. 1 (MRT dosimetry, only 1 patient), it is easy to imagine the excellence of a study that incorporates both the clinical setting by Baczyk et al. and the rationale by Hobbs et al. The article by Fishbein et al. 5 (5 patients treated with 131I-mIBG and EBRT) plays in favor of the rationale presented by Bodey et al. 10 in the example reported (Fig. 1).
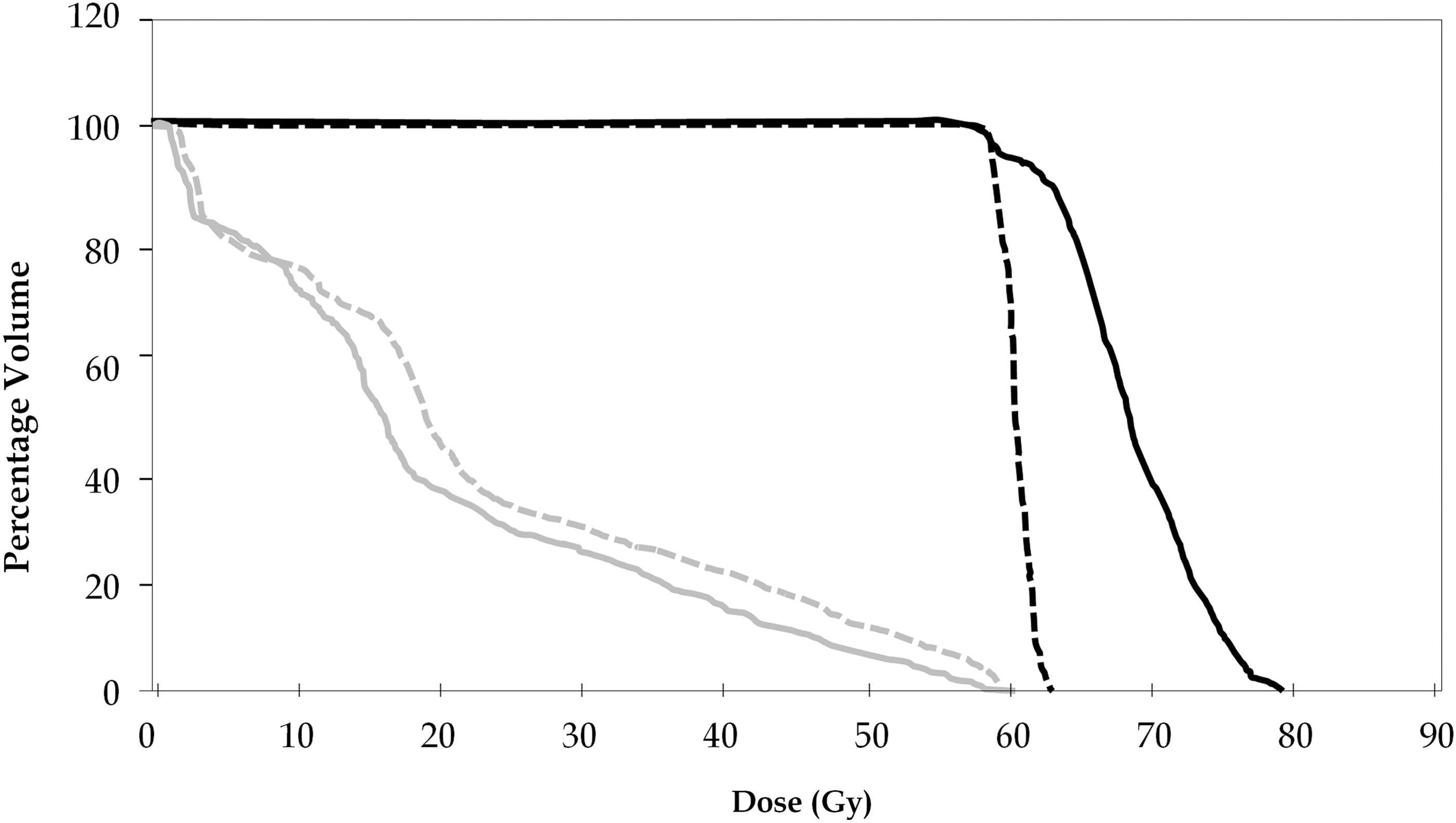
Comparison of the DVH curves in a patient administered with 33 GBq of 131I-mIBG, hypothetically undergoing EBRT delivering an absorbed dose of 60 Gy to the isocenter (2 Gy/cycle). The continuous lines represent the combined MRT+EBRT treatment, with the DVHs of the tumor (black curve) and of the OARs (gray curve). The dotted lines represent the EBRT, with the DVHs of the tumor (black curve) and the OARs (gray curve). The graph highlights the advantage of the combined solution for both the CTV and the OAR (the left kidney). Adapted from Bodey et al.10 DVH, dose volume histograms; 131I-mIBG, 131I-metaiodobenzylguanidine; EBRT, external beam radiation therapy; MRT, molecular radiotherapy; OAR, organs at risk; CTV, clinical target volume.
The availability of MRT dosimetry may have an important impact also on the inclusion criteria. The study by Poli et al., 7 with absorbed doses from 131I-L19SIP ranging from 1.1 to 35.8 Gy, and the study by Kreissl et al., 4 with absorbed doses from PRRT ranging from 0.2 to 30.6 Gy, point out the need to narrow the recruitment for MRT based on diagnostic scans (124I-L19SIP and 68Ga-DOTATOC, respectively), to avoid useless treatments with negligible absorbed doses to the tumor. In the study by Ferrari et al., 3 where the procedure cannot include a diagnostic scan and, therefore, fixed activities were administered, the dosimetric results from IART enhanced the possibility to compensate for interpatient differences by adapting the subsequent number of EBRT fractions.
The LQ model remains at the moment the most considered method to compare EBRT and MRT. This model can be regarded as a fascinating guiding tool, preferable to activity escalation strategies, especially in the safety assessment of innovative therapies. In any case, there are several pros and cons in the use of a radiobiological model to plan combined treatments, and the pertinence of the LQ model for the integration of two radiation therapies should be definitely proved by the analysis of large experimental data sets.
Regarding advantages, the LQ model can be applied in the comparison of TCP curves as a function of time. This can help in deriving the capacity of tumor control of different therapies and in establishing adequate time intervals between therapies, therefore balancing tumor proliferation and damage recovery. This point is highlighted in Figure 2, where TCP curves versus time show the advantage of a boost delivered immediately after the surgery with IART compared with the standard EBRT. The time schedule of combined therapies should be deepened specifically for each therapy, as it could be a strong point. The use of diagnostic PET or SPECT provides information that is useful for treatment planning in EBRT and MRT as well. On the other hand, PET or SPECT examinations performed during MRT document the radiation actually delivered in the area of interest. If EBRT is performed first, the diagnostic examinations can guide the planning, while if MRT is first, both the available examinations can be integrated to optimize the subsequent EBRT treatment. In the studies described, the standard approach for the disease has been proposed as the first treatment. For instance, 131I-mIBG is administered first, followed by EBRT. 5 In some cases, restrictions related to the need to recover from toxicity 2 or from surgery exist, 3,29 but further investigation is warranted. In other cases, the time interval could be reduced and/or the order assessed in virtue of the orthogonal toxicities, clinical and radiobiological considerations, such as the time dependency of the TCP curve. 36

Comparison of the TCP curves versus time for the combined IART+EBRT therapy (IART, 20 Gy+EBRT, 40 Gy at 2 Gy/fraction) and for the standard EBRT (40 Gy to the mammary gland plus a boost of 20 Gy to the tumor, at 2 Gy/fraction). The continuous line represents IART+EBRT and the dotted line represents the standard EBRT. The curves were evaluated considering the following radiobiological parameters: α/β=10 Gy; α=0.30 Gy−1; Teff=38 hours; Trep=1.5 hours; Tav=40 days; number of clonogenic cells N0=106. The graphs show the advantage of a boost delivered immediately after the surgery (in this case by IART). It is expected that the combined therapy IART+EBRT would offer the same, even anticipated, tumor control of the standard treatment, with the advantage of avoiding about 10 sessions of EBRT. TCP, tumor control probability; IART, intraoperative avidination for radionuclide therapy.
The main advantage of the BED is the possibility to quantitatively compare the different radiation modalities in terms of cell surviving fractions for tumors and functional subunits for parallel organs. Indeed, it is well known that absorbed doses of EBRT and MRT are not directly comparable. This was observed for instance on clinical data of kidney toxicity after therapy with 90Y-DOTATOC. Absorbed doses converted to BED allowed to derive an NTCP curve that was nearly overlapping the corresponding curve from EBRT data. 24 In this case, absorbed dose values (or absorbed dose distribution maps) from both treatments have been converted into BED values (maps), and comparisons made in terms of BED. However, to predict toxicity and efficacy, it seems most convenient to convert MRT absorbed doses distribution into BED distribution and then into absorbed dose map in terms of EBRT. 1,3,10 This is because of the large amount of experimental data available in EBRT in terms of dose–effect correlations (phenomenological curves) and DVH characteristics compared to the shorter experience of MRT. Such a conversion allows familiarizing with some of the radiobiological approaches already used in radiotherapy, which help to correlate doses with effects and to analyze the DVHs in the perspective of dose–volume effects.
The fact that any conversion depends on the value assigned to the radiobiological parameters included in the model reflects the limitations of the model itself, pointing out the main disadvantage of the questioned adequacy of the LQ model for the comparison of different radiation modalities. The impact of the radiobiological parameters remains an open issue of the model, and the influence of a possible variation should always be taken into account. For example, in the study by Ferrari et al., 3 if the α/β value of 4.6 Gy for the breast target tissue obtained in more recent studies 37 would replace the α/β of 10 Gy considered, 3 one more fraction (2 Gy) of EBRT should be added after IART to compensate the lacking effect.
Also the use of EUD parameter, in case of highly heterogeneous radionuclide uptake, deserves further investigation, especially if it is used for comparison with EBRT clinical data (NTCP curves), which refer to a small degree of dose heterogeneity. In addition, in case of MRT, such parameter is heavily affected by the noise of the functional images used for dosimetry. Generally, all the factors contributing to MRT dose uncertainty could impact on the validity of the radiobiological modeling. It is well known that tailored dosimetry in radionuclide therapy is still challenging and affected by a considerably higher uncertainty than EBRT (∼20% vs. ∼2%). 38 –42 Such dose uncertainties could be amplified when converted to radiobiological parameters or used as input data for the NTCP and TCP models. Efforts should be made to improve MRT dose evaluation: nuclear medicine images need to be properly reconstructed and corrected for scatter, attenuation, and response of the system. 1 Moreover, proper correction for partial volume effect should be implemented. If these requirements are fulfilled, 3D dosimetry methods can be recommended based on convolution methods or direct Monte Carlo simulations.
From a practical point of view, the combination of EBRT and MRT can be conceived based on a prescribed absorbed dose to the tumor or a constraint to the absorbed dose to the OARs. When toxicities are not of concern, the combination can be planned imposing the same minimum absorbed dose to the tumor in the combined treatment as with EBRT alone. This is the case of 131I-MIBG shown in a theoretical example by Bodey et al. 10 and in the clinical study by Fishbein et al. 5 As opposed to this occurrence, when the OARs are irradiated by both EBRT and MRT, the threshold for toxicity has to be preserved, and methods like the one proposed by Hobbs et al. 1 should be applied. In a serial organ, the highest voxel total absorbed dose must be lower than the absorbed dose constraint, while for parallel organs, the mean absorbed dose or the EUD could be set lower than the constraint.
Finally, considerations concerning the combination of two MRTs 15,34,35 could better interpret the effects of combined EBRT and MRT. In fact, the equations set by Hobbs et al. 15 concerning the MTD to different OARs and the absorbed dose to the tumors can be also adapted to combined EBRT and MRT, which usually have complementary OARs. The analysis by Walrand et al., 34 showing the impact of tumor heterogeneity and the choice of the radionuclide for MRT, is relevant also if MRT is associated to EBRT, which may need to compensate for heterogeneity and/or fulfill proper constraints to the OARs. 8 This emerges in the treatment of meningiomas, where 177Lu instead of 90Y is selected for PRRT to avoid the irradiation of cranial nerves. 4 With 177Lu, the MTD condition for cranial nerves involves only the contribution from EBRT, while MRT imposes a MTD condition to the kidneys and the red marrow.
Conclusions
Treatments combining EBRT and MRT are a promising option that can be applied in many different clinical scenarios and may be more advantageous than a single radiation modality. Different therapies have usually different OARs, so the properties of each therapy can be fully exploited, with the result of increased irradiation of the target and reduced irradiation of critical tissues. To date, clinical trials of combined therapies are based on empirical approaches but offer key information. The mathematical framework to integrate the effects of different radiation modalities has already been proposed with the LQ model. Despite some possible limitations, this model represents a starting point to derive information for future verification and improvement. The present body of data justifies the development of prospective clinical studies with radiobiological personalized imprint and aimed at optimization.
Footnotes
Disclosure Statement
There are no existing financial conflicts.