
Abstract
Genetic predisposition has been shown to affect the severity of skin complications in breast cancer patients after radiotherapy. Limited data exist regarding the use of a genetic risk score (GRS) for predicting risk of tissue radiosensitivity. We evaluated the impact of different single-nucleotide polymorphisms (SNPs) in genes related to DNA repair mechanisms and oxidative stress response combined in a GRS on acute adverse effects induced by breast radiation therapy (RT). Skin toxicity was scored according to the Radiation Therapy Oncology Group (RTOG) criteria in 59 breast cancer patients who received RT. After genotyping, a multilocus GRS was constructed by summing the number of risk alleles. The hazard ratio (HR) for GSTM1 was 2.4 (95% confidence intervals [CI]=1.1–5.3, p=0.04). The other polymorphisms were associated to an increased adverse radiosensitivity, although they did not reach statistical significance. GRS predicted roughly 40% risk for acute skin toxicity per risk allele (HR 1.37, 95% CI=1.1–1.76, p<0.01). Patients in the top tertile had a fivefold higher risk of skin reaction (HR 5.1, 95% CI=1.2–22.8, p=0.03). Our findings demonstrate that the joint effect of SNPs from oxidative stress and DNA damage repair genes may be a promising approach to identify patients with a high risk of skin reaction after breast RT.
Introduction
Breast radiation therapy (RT) after conservative surgery is widely accepted as a standard of care for patients with early breast cancer. As a result, adverse side effects may develop in the co-irradiated normal tissue. From a biological and clinical point of view, adverse reactions to RT are commonly classified in early (acute) and late effects. 1 Acute normal tissue toxicity is generally a transient phenomenon, with symptoms settling within months after treatment but can affect the therapeutic program and worsen patients' quality of life. 2 Late complications are especially important, as they are progressive and appear to be associated with a lifelong risk. 3 Furthermore, it has been suggested that there may be an association between the occurrence of early reactions and the risk of subsequent late effects in a number of organs. Thus, markers for the acute response should be predictive for consequential effects. 4
Both acute and late tissue effects are known to differ considerably between patients treated with identical schedules. Only 30% of this clinical variation can be attributed to changes in treatment-related parameters. 5,6 It has been suggested that these variations not only mainly result from differences in individual factors, such as age or body–mass index (BMI) 5,7,8 but are also genetically determined. 9 As a matter of fact, great interest is currently directed toward the use of genetic markers, such as single-nucleotide polymorphisms (SNPs), as parameters for the individual risk of experiencing radiation-induced tissue toxicity. Several studies have been performed but the results obtained are heterogeneous and, often, conflicting. 10 –13 In particular, the vast majority of SNPs studied so far are assumed to have no or a small effect on the individual skin radiosensitivity. Thus, the simultaneous investigation of many SNPs, each one associated with a small effect, could increase the possibility to develop molecular markers able to predict radioresponse. Accordingly, the purpose of this study was to assess the joint effect of different SNPs combined in a genetic risk score (GRS) on early adverse effects induced by RT in normal tissue of a population of breast cancer patients. Such risk scores can easily be created by adding the number of risk alleles per patients and correlating the resulting numerical value with the severity of the normal tissue toxicity. Since it is well known that ionizing radiation (IR) therapy exerts its cytotoxic effects that damage the DNA directly or indirectly through the production of reactive oxygen species, we investigated selected SNPs located in genes which are involved in oxidative stress (GSTM1 and GSTT1) or DNA damage signaling and repair (XRCC1, XRCC3, and H2AX), previously associated with early radiation-induced side effects and DNA repair capacity.
Materials and Methods
Study population and data collection
We enrolled 59 patients (mean age, 58.4; range, 35–80 years) who underwent RT after conservative surgery for breast cancer (Stage I–III) at the Radiation Oncology Unit of Brindisi Hospital “A. Perrino.” A detailed anamnestic history was collected from all patients, and blood sampling was performed for each of them. The acute side effects of RT developing in the skin within the radiation field of the breast were used to measure clinical radiosensitivity. For the assessment of the severity of skin reactions, we used a classification system based on a scoring system according to the Radiation Therapy Oncology Group (RTOG) criteria. 14 Grade 1 acute toxicity was defined as follicular, faint, or dull erythema, dry desquamation, and epilation and grade 2 was defined as tender or bright erythema, patchy moist desquamation, and moderate edema. Patients with acute skin reactions of RTOG grade ≥1 were referred to as the radiosensitive group and compared with patients with no or minimal skin reactions (RTOG grade 0). The occurrence and severity of acute skin reaction were determined within 30 days after RT treatment.
RT
The planning target volume (PTV) dose prescription ranged from 40.05 Gy (55 patients), 45.00 Gy (1 patient), and 50.00 Gy (3 patients). In most cases, the PTV irradiation was followed by a boost phase of 10.00 Gy to the tumoral bed (47 patients). Conventional (200 cGy/day) and accelerated fractionations (250 or 267 cGy/day) were used. Computed tomography images were acquired with a fixed step size of 5 mm. In accordance with the International Commission on Radiation Units and Measurements (ICRU 50), 15 the PTV was generated by expanding the clinical target volume, that is, the entire breast for approximately 5 mm from the body contour, of 7 mm in all directions but in the direction of the skin surface, to compensate for set-up uncertainty. In the skin direction, the distance between the body and PTV was left at 5–6 mm so as to not excessively penalize the dose–volume histogram calculations. Ninety-five percent isodose included PTV so this dose was at 5 mm under the skin. All PTVs were contoured by the same radiation oncologist, and a single physicist individually performed all treatment plans. The linear accelerator used was a Varian 2100 (Varian Medical Systems), which has an enhanced dynamic wedge. The treatment planning system (Varian Eclipse version 7.3.10; Varian Medical Systems) used a calculation pencil beam algorithm with the modified Batho power law as tissue inhomogeneity correction method; the grid calculation dose was 2.5 mm for the dose calculation for all patients. The optimized plan had isocentric photon beams with 6 or 15 MV energy, and the beam separation angle was approximately 174°±5° so as to align the beam's internal divergence and to avoid involving the contralateral breast.
Sample collection, DNA extraction, and genotyping
Genomic DNA was extracted from peripheral blood leukocytes using EuroClone Kit (EUROGOLD Blood DNA Mini kit; EuroClone) according to the manufacturer's instructions. XRCC1 Arg399Gln (rs25487) and XRCC3 Thr241Met (rs861539) were assessed by polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) method using primers and restriction enzymes as previously described. 16 GSTM1 and GSTT1 was carried out in a multiplex PCR with the albumin gene as an internal positive control to verify the correct DNA amplification. 13 The −1420G>A (rs8551) and 1057C>T (rs7350) variants in H2AX gene were determined by real-time PCR and high-resolution melting (HRM) analysis. Primers for H2AX gene polymorphisms were designed using program PRIMER 3 and the sequences were as follows: forward 5′-TGGTGCTTAGCCCAGGACTTTCAG-3′, reverse 5′-AGAAGGGGCGCCAGACCGTGATC-3′ for 1057C>T genetic variant and forward 5′-ATCCTGGGCGTTTCTTGCCCTGT-3′, reverse 5′-ATGGAGAGGGAGAGAGTAGCAAG-3′ for −1420G>A genetic variant. PCR amplification was performed with initial denaturing at 98°C for 2 minutes, followed by 49 cycles of denaturing at 98°C for 2 seconds, annealing/extending at 63°C for 5 seconds, and subsequent melting that consisted of a continuous fluorescent reading from 60°C to 90°C at the rate of 0.2°C per seconds. Allelic discrimination was analyzed using the Bio-Rad Precision Melt Analysis Software (Version 1.2; Bio-Rad).
Statistical methods
Statistical analysis of the data were performed with the StatView statistical package, version 5.0.1 (Abacus Concepts). Data are expressed as the mean±standard deviation. Differences between categorical variables, genotype/allele frequencies, and Hardy–Weinberg equilibrium (HWE) were tested by χ2 analysis. Differences between continuous variables were evaluated using Student's t-test. Data for three or more independent groups were analyzed by analysis of variance, and significant differences among pairs of means were tested by Fisher's exact test. The probability of development of the maximum grade of skin toxicity in the 30 days after RT was determined by the Kaplan–Meier analysis with the statistical significance of the difference between curves determined by the log-rank test (Mantel-Cox Test). High-risk alleles were used to generate a GRS that was calculated as follows: 2 units if the patient was homozygous for the high-risk allele, 1 unit if the patient was heterozygous, and 0 if the patient was homozygous for the low-risk allele. The GRS was modeled as a continuous variable and as tertiles. Cox proportional hazard models were used to assess hazard ratios (HR) with confidence intervals (CI) that were 95% of SNPs and of GRS adjusted for potential confounders.
Results
Demographic and clinical characteristics of the study population stratified according to the RTOG grade are reported in Table 1. Specifically, 24 (41%) patients experienced faint to moderate acute skin toxicity, while 35 (59%) had no acute skin reactions. A significant difference was found in the BMI value (p=0.02) between the two groups. No difference was observed for the other clinical variables.
BMI, body–mass index.
All subjects were successfully genotyped for all selected SNPs. The genotype distribution between patients according to RTOG grade 0 and RTOG grade ≥1 showed that GSTM1 distribution was significantly different between the two groups (p=0.02). Conversely, the genotype distribution of other polymorphisms was not significantly different from that observed in radioresistant and radiosensitive groups (Table 2).
SNP, single-nucleotide polymorphism.
The Kaplan–Meier curves for the GSTM1 polymorphism showed a significant difference in the development of acute skin toxicity test according to the genotype. Indeed, the GSTM1 null allele was associated with an increased risk for acute skin reaction (HR 2.4, 95% CI=1.1–5.3, p=0.04). In addition, after controlling for baseline confounding variable, BMI, the GSTM1 null allele remained independently related to acute side effects (HR 2.4, 95% CI=1.1–5.5, p=0.03).
Although the difference did not reach statistical significance, clear differences in Kaplan–Meier curves were also observed for the other genetic variants (H2AX 1420G>A and 1057C>T, XRCC1 Arg399Gln, and XRCC3 Thr241Met) according to a recessive or co-dominant model of inheritance (Fig. 1 and Table 3). The integrated effect of six SNPs was evaluated by calculating a GRS representing the sum of the high-risk alleles. The resulting GRS was significantly associated with the risk of early acute effects (HR 1.37, 95% CI=1.1–1.76, p<0.01). The highest HR for early acute effects was found in patients in the top tertile (HR 5.1, 95% CI=1.2–22.8, p=0.03) of the GRS compared with those in the bottom tertile (Fig. 2).
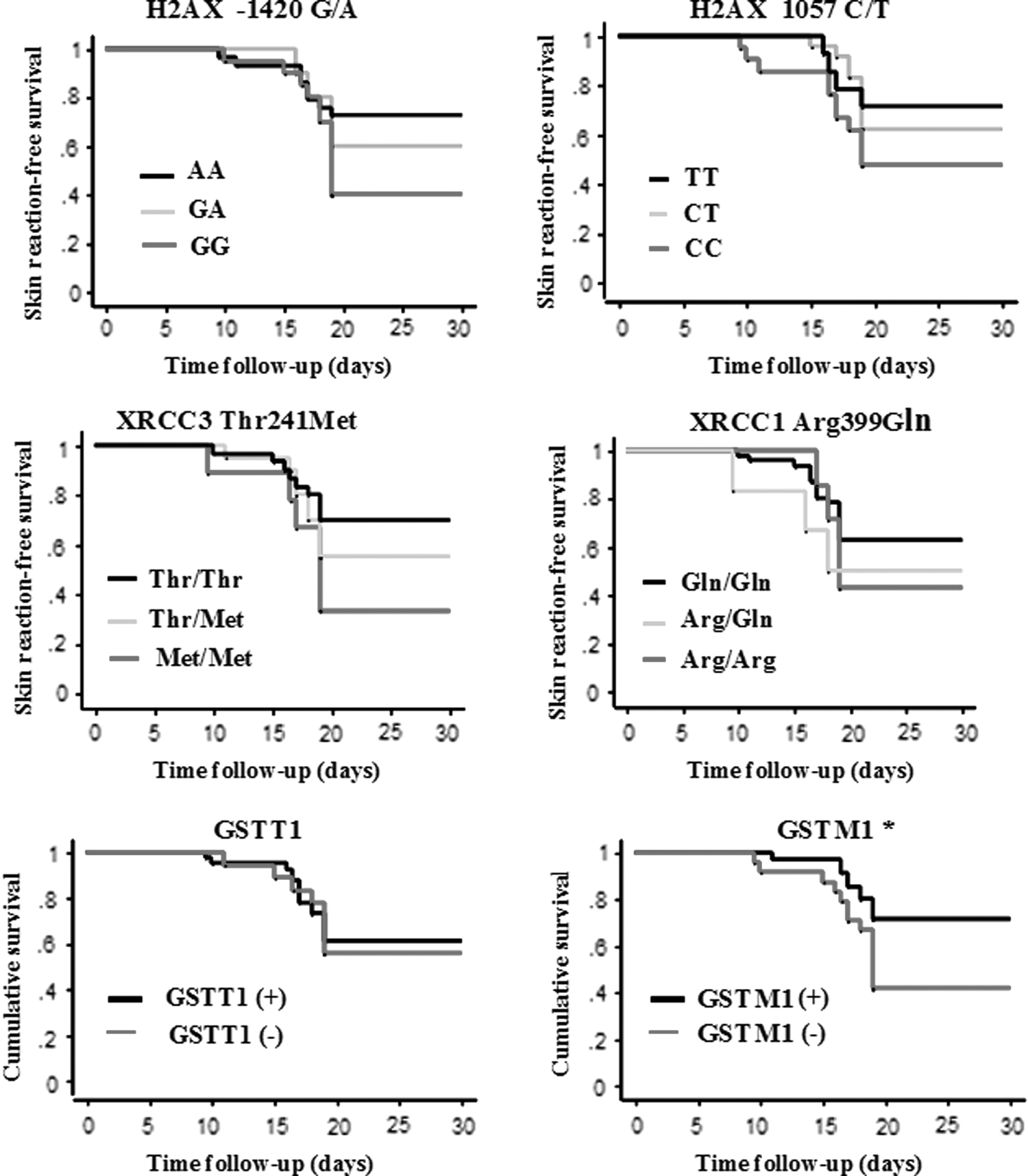
Kaplan–Meier survival curves according to different genotypes.*p<0.05.

Kaplan–Meier curves for patients according to tertiles of high-risk alleles.
Adjusted for BMI.
CI, confidence intervals; HR, hazard ratio.
Discussion
This study evaluated the impact of genetic variants linked to oxidative stress (GSTM1 and GSTT1) and DNA damage signaling and repair (XRCC1 Arg399Gln, XRCC3 Thr241Met, and H2AX 1420G>A and 1057C>T) in relation to the development of acute skin side effects after RT in breast cancer patients.
During the last years, a number of studies have shown mainly positive associations between certain genetic variants in enzymes involved in oxidative metabolism and detoxification and DNA repair and the risk of tissue toxicity after RT. 10 –13 In particular, glutathione S-transferases (GSTs) enzymes are recognized as one of the key mechanisms of cellular protection against oxidative stress. 17 Structural deletion polymorphisms in GSTM1 and GSTT1 genes lead to loss of enzyme activity and may result in a greater risk for radiation-associated toxicity. 18,19 Furthermore, previous studies reported no association between GSTM1 and GSTT1 null allele and the development of early skin complications. 13 –20
XRCC1 protein plays a pivotal role in DNA single-strand break repair in the base excision repair pathway. Several variants of XRCC1 have been described, including one affecting codon 399 in exon 10 that results in arginine (Arg) to glutamine (Gln) change.
The presence of the polymorphic variant (Arg399Gln) in XRCC1 gene leads to an amino-acid change that deeply affects the protein function, thus influencing its ability of DNA repair capacity. 21 –23 The association between Arg399Gln polymorphism and radiation-induced toxicity has been extensively investigated. 24 –26 However, studies performed till now have shown conflicting evidence of this association. A recent meta-analysis reported an association between the XRCC1 399Gln allele and a trend toward an increased risk of high-grade radiation-induced toxicity when a dominant model is used to analyze the data. 27
XRCC3 participates in DNA double-strand break via homologous recombination repair breaks caused by normal metabolic processes and/or exposure to IR. 28 The common polymorphism Thr241Met in exon 7 affects the enzyme function and/or its interaction with other proteins involved in DNA damage and repair. 29 Regarding this SNP and acute skin radiotoxicity, the previous results are conflicting. For instance, no significant association between XRCC3 polymorphism and radiosensitivity has been reported by earlier studies, 11,30 while an increased rate of toxic skin effects was subsequently demonstrated in patients carrying the XRCC3 Met allele. 13 Similarly, a further study documented a link between the wt allelic variant of XRCC3 Thr241Met and a lower rate of erythema. 31
Finally, the H2AX is known as the “histone guardian of the genome.” In fact, histone H2AX phosphorylation (γ-H2AX) is essential for the initial recognition of DNA double-strand breaks through a specific and efficient coordination of DNA repair mechanisms. A major role of γ-H2AX in the stabilization of DNA repair proteins has been recognized as well as its major involvement in both NHEJ and HR repair pathways. 32 The selected 1420G>A and the 1057C>T H2AX polymorphisms are located, respectively, in promoter and in 3′UTR of gene. Recently, several studies demonstrated that H2AX promoter polymorphisms may alter susceptibility to cancers, including breast cancer. 33 This finding provides support for the hypothesis that SNPs in the H2AX promoter region are biologically important. Anyway, the possible role of genetic polymorphisms in the H2AX promoter region has not yet been studied in the toxicity after RT. In our study, no significant association was found with any individual SNP except for GSTM1. However, the power to detect a significant association with radiation toxicity may be limited due to the relatively smaller sample size of cases. In fact, the associations for the other SNPs were in the expected direction but statistically not significant. To combine the relatively small effects of individual genes and to better capture the complex relationship between genetics and radiation toxicity, genotypes at multiple SNPs may be included into a genetic score calculated according to the number of risk alleles carried. Importantly, the analysis of the joint effects of the six SNPs demonstrated that the resultant GRS predicted a roughly 40% risk for acute skin toxicity per risk allele. In particular, patients in the top tertile of GRS had a fivefold higher acute skin effect than patients in the bottom one, supporting the utility of a genetic score in order to provide a greater predictive value than any single variant. To date, a few studies have examined the utility of genetic scores to identify subjects at an increased risk for early side effects after RT showing that combining multiple loci with modest effects into a global GRS may improve the predictive value better than any single variant. 24,34,35 Accordingly, we were able to support the notion that radiation side effects depend on multiple and not on single polymorphisms as well as to show that a GRS may improve identification of individuals at an increased risk of developing acute reactions.
However, our finding should be interpreted while bearing in mind some limitations such as the modest sample size that makes statistical estimations less robust. Furthermore, though the candidate gene approach has been widely used to study normal tissue radiosensitivity, the usefulness of this approach is largely limited by an a priori knowledge of possible gene candidates and, unfortunately, the molecular dissection of the “radiosensitive phenotype” remains largely unknown.
Over the next few years, indeed, it is expected that SNPs associated with adverse effects resulting from RT will be identified from several large-scale genome-wide associations. 36 Larger prospective studies involving multiple and novel genetic variants are needed in order to find the optimal set of genes able to predict adverse responses to radiation therapy as well as to permit personalization of the treatment plan on an individual basis.
Despite these limitations, our findings demonstrate that the combination of specific polymorphisms might be a feasible and promising approach to identify patients at a high risk of radiation-induced adverse effects.
Footnotes
Acknowledgment
The authors thank all the patients who participated in this study.
Disclosure Statement
There are no existing financial conflicts of interest.