
Abstract
Introduction:
Although several studies have shown that the presence of acellular mucin pools in surgical specimens with rectal carcinomas examined after preoperative chemoradiotherapy indicated complete response to therapy, the proper meaning of these pools has yet to be elucidated. The aims of this study were to analyze the immunoprofile of acellular mucin pools and to review the relevant literature.
Methods:
In 30 consecutive rectal cancers that were preoperatively treated with chemoradiotherapy, the clinicopathologic features were correlated with the immunoexpression of AE1/AE3 keratin and carcinoembryonic antigen (CEA).
Results:
Acellular mucin pools were present in all the cases, independently by their preoperative histological aspect. In remnant tumors (n=20), they were present at the invasion front and were marked by CEA. In cases without remnant tumor cells (n=10), they also displayed CEA positivity. In 2 of the 10 cases, isolated tumor cells were identified after multilevel sectioning of paraffin-embedded blocks.
Conclusions:
The presence of acellular mucin pools in surgical specimens of rectal cancers cannot be interpreted as an indicator of complete response to radiotherapy if at least 10 multilevel sections are performed in at least three tumor blocks per case, and CEA negativity is not proved.
Introduction
In patients with locally advanced rectal cancer, neoadjuvant preoperative chemoradiotherapy is used as the standard of care. Postchemoradiotherapy, in the surgical specimens, the identification of fibrotic areas without embedded remnant tumor cells and the absence of lymph node metastases are considered as indicators of the complete pathological response. 1 Recently, in patients with rectal cancer who underwent preoperative chemoradiotherapy, acellular mucin lakes (Alcian blue-positive mucin pools lacking neoplastic epithelium) were identified in the postoperatively examined resection specimens; their prognostic significance being controversial. 2 –6 The College of American Pathologists suggested that they are an indicator of treatment response and not of residual tumor. 2 –6 Based on this suggestion, further analyzed in few reported studies, 1 –6 the identification of mucin lakes in the muscularis propria of the rectum is not even reported by pathologists as a postchemoradiotherapy remnant tumor 1 or is not included in the postradiotherapy staging system (yTNM), 6 although the real significance of these pools has yet to be elucidated. No data about the immunoprofile of these pools have been published thus far.
The main aim of this article was to perform an attentive evaluation of the histological aspect of the resected rectal carcinomas in which the chemoradiotherapy was preoperatively performed. A special consideration was assigned to the significance of the acellular mucin pools and their immunohistochemical features based on the expression of AE1/AE3 keratin and carcinoembryonic antigen (CEA).
Materials and Methods
The histopathologic features of rectal carcinomas were analyzed in 30 consecutive cases of biopsy-proven locally advanced rectal cancer diagnosed in clinical stage II or III, in which surgical resection was performed after preoperative chemoradiotherapy. All patients were treated with preoperative concomitant capecitabine and pelvic radiotherapy, with doses ranging from 45 to 62 Gy, according to the previously reported protocols. 7 Surgical removal of the tumor was performed at 4–8 weeks after completion of chemoradiotherapy. The radiologic response and the histological postradiotherapy staging were evaluated based on histological examination of the surgical specimens. The presence or absence of acellular mucin pools after multilevel sectioning of paraffin blocks (10 successive sections for each block, three blocks per case) was the main characteristic taken into account. PAS–Alcian blue staining was also performed in each case. The Head of the Department of Pathology in the University of Medicine and Pharmacy of Tirgu-Mures, Romania, approved the processing of the cases.
Immunohistochemical staining was performed on paraffin-embedded tissues with the use of the Novolink Polymer detection system (Novocastra, Newcastle Upon Tyne, United Kingdom). The antibodies AE1/AE3 keratin and monoclonal CEA (clone II-7) from Dako (Glostrup, Denmark), diluted at 1:200 and 1:50, respectively, were used. Sections of 5 μm thick were deparaffinized, rehydrated, and incubated at 100°C with pepsin (keratin) and citrate (CEA). Slides were developed by using the diaminobenzidine (DAB) solution (Novocastra). Counterstaining was performed with Mayer's hematoxylin (Novocastra). The normal mucosa of the rectum was used as internal positive control. For negative controls, incubation was performed with the omission of specific antibodies.
Results
From the 30 patients, 16 were males and 14 were females, with the median age of 65.41±11.23 years (range, 50–78 years). All the patients were still alive without reported recurrences 3 years after surgical intervention. Based on the preoperative biopsies, three histological types were included in this study: well-differentiated adenocarcinomas (n=7), moderately differentiated adenocarcinomas (n=15), and mucinous adenocarcinomas (n=8).
The postoperative examination of the surgical specimens proved the presence of remnant tumor cells in 20 of the 30 cases. In all these cases, independently by the preoperative aspect, mucin pools were identified in the deep tumor layers, some of the pools being lined by remnant neoplastic epithelium. In the invasion front, most of the pools became acellular (Fig. 1). In the other 10 cases, no remnant tumor cells were identified after the first three multilevel sectioning. Despite the absence of the tumor cells, the Alcian blue-positive acellular mucin pools were observed in all the cases, in the submucosa and muscularis propria; they expressed positivity for CEA and were negative for keratin. In two of these cases, at the periphery of one of these pools, thin keratin-positive residual fragments of tumor epithelium were identified after the 8th and 10th deeper section (multilevel sectioning), respectively (Fig. 2). In both the cases, the tumor cells occurred in only one of the three blocks that have been sectioned; at first level section, CEA positivity and keratin negativity were also seen. Based on these findings, all the other cases with acellular mucin pools, without tumor cells, were included in yT2 stage and benefited by postoperative radiotherapy, similar to the other cases. No recurrences occurred in each of the cases after 3 years of follow-up.
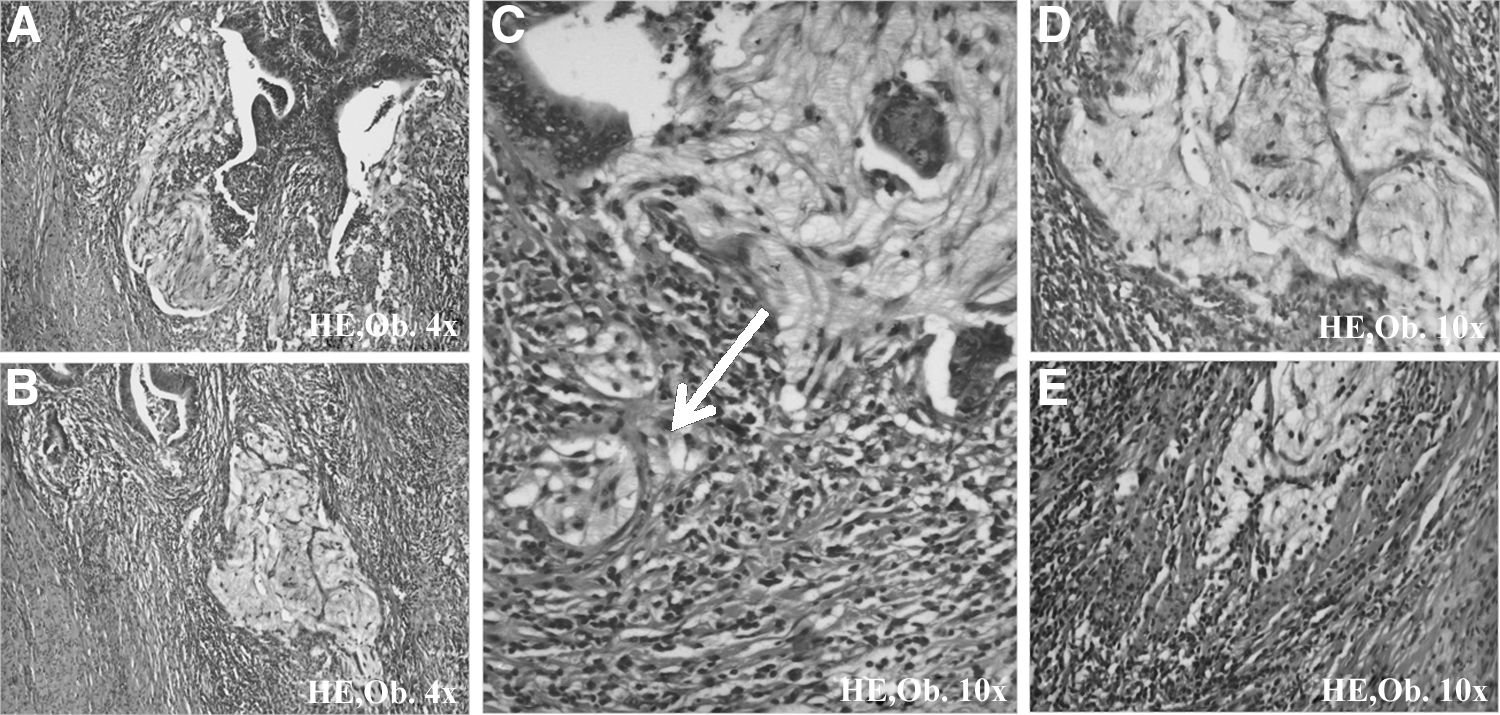
In rectal adenocarcinomas examined after preoperative chemoradiation, the mucin pools are lined by remnant tumor epithelium
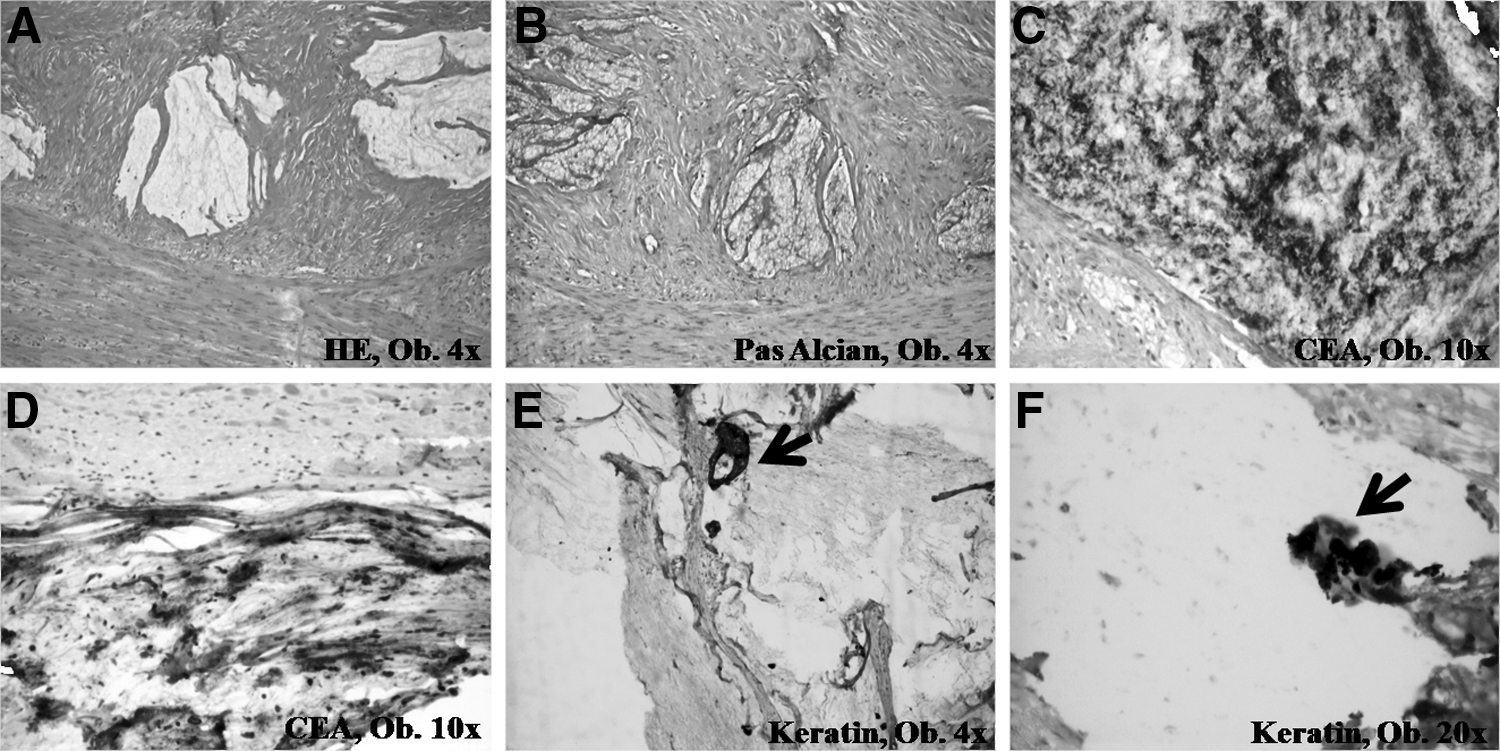
In rectal adenocarcinomas examined after preoperative chemoradiation, in cases without remnant cells, acellular mucin pools can be seen in the muscularis propria
Discussion
This study presents data in line with those previously published in the literature, except CEA expression of acellular mucin pools. Similar to the findings of this study, acellular mucin pools have been reported to occur in surgical specimens of 15%–27% of patients with rectal cancer treated with neoadjuvant preoperative chemoradiation followed by proctectomy, predominantly in male patients. 2 –4 These findings also seem to be associated with the mucinous phenotype of the primary tumor 2 and to have been noted in the lymph nodes, 6 although these observations have not been emphasized by all authors, even in the cases of this study.
Although most of the authors agreed that acellular mucin pools are a marker of treatment effect, 2 –4,6 they also reported that acellular mucin pools neither have an impact on oncologic outcomes nor an influence on the survival rate 2,4,6 ; this is despite the better survival rate emphasized by some researchers. 6 Moreover, among patients who achieved complete pathological response after chemoradiation (yT0N0M0), those with acellular mucin pools had increased distant recurrence, decreased disease-free survival, and decreased overall survival rate, respectively. 3 Based on these findings, the authors concluded that the presence of acellular mucin pools does not affect local recurrence but could be an indicator of aggressive tumor biology. 3 The expression of monoclonal CEA in these pools confirms their hypothesis, and the multilevel sectioning of specimens could identify some residual tumor cells, as in one of the cases of this study.
Based on the histological findings, the authors tend to believe that the postchemoradiotherapy steps of tumor destruction consist of breakage of the tumor glandular epithelium that keeps the secretion property until the total disappearance. However, a thin tumor fragment is enough to conserve the integrity of the tumor mucus, this being proved by its CEA positivity. The presence of mucinous pools in both mucinous and nonmucinous adenocarcinomas (preoperatively diagnosed) could show that the mucinous component is not identified at biopsy in all the cases.
CEA is well known to protect tumor cells from apoptosis and anoikis; thus, improper downstaging of these cases could favor tumor recurrence. 8 Because one recent study emphasized the increased resistance to 5-fluorouracil of CEA-positive cancer cell lines, 8 which remains the only tumor marker of efficacy in monitoring patients with colorectal cancer, 9 the authors decided to recommend postoperative radiotherapy without associated chemotherapy in the cases of this study.
This study primarily aimed to show that the presence of acellular mucin pools cannot be considered to indicate complete response to adjuvant chemoradiotherapy. Although the recommendation is to consider acellular mucin pools as an indicator of therapeutic response, their diffuse CEA positivity show that tumor cells can be identified after multilevel sectioning of paraffin-embedded tissues. To not consider them as an indicator of tumor activity, at least three tumor blocks should be multilevel sectioned, at least 10 sections per blocks being mandatory to be performed. This hypothesis could influence the postradiotherapy staging and the therapeutic management of rectal cancer.
Footnotes
Acknowledgments
This work was partially supported by the Threepharm S.A. and University of Medicine and Pharmacy of Tirgu-Mures, Romania, team research projects frame. The English-language manuscript was polished by SPI Global Professional Editing Service.
Disclosure Statement
No conflicts of interest are declared.