
Abstract
99mTc-HYNIC-TOC is a cost-effective and logistically viable agent for scintigraphy of neuroendocrine tumors overexpressing somatostatin receptors as compared with [111In-DTPA-D-Phe1] Octreotide (Octreoscan®). Several studies have been reported, wherein the efficacy of this agent is demonstrated. In the present article, the authors report the preparation of a single-vial HYNIC-TOC kit suitable for the preparation of 4–5 patient doses (15 mCi/patient) of 99mTc-HYNIC-TOC. The kits were tested for sterility and bacterial endotoxins to assure safety of the product. A significant modification in this kit is the inclusion of buffer in the kit itself, unlike in commercially available kits where the buffer solution has to be added during preparation. 99mTc-HYNIC-TOC was prepared by adding 20–80 mCi (740–2960 MBq) of freshly eluted Na99mTcO4 in 1–3 mL of sterile saline directly into the kit vial and heating the vial in a water bath at 100°C for 20 minutes. The labeling yield and radiochemical purity of 99mTc-HYNIC-TOC, prepared using the lyophilized cold kit, were consistently >90%. The kits were evaluated over a period of 9 months and found to be stable when stored at −20°C. Limited clinical studies performed with the 99mTc-HYNIC-TOC, formulated using the kit, showed adequate sensitivity and specificity for the detection of gasteroenteropancreatic neuroendocrine tumors.
Introduction
Somatostatin (SST) is a cyclic peptide neurotransmitter or hormone that exhibits inhibitory action on the production of other hormones and plays a pivotal role in regulatory processes, such as cell division, proliferation, and apoptosis.
1
Cellular action of SST is mediated by binding to cell membrane proteins, termed as somatostatin receptors (SSTRs). Five different subtypes of SSTRs have been identified in the central nervous system, neuroendocrine system, and in the gastrointestinal tract. They have been found to influence specific actions in different tissue types.
2
Although SSTRs are overexpressed in different types of tumors, those of neuroendocrine origin, such as gasteroenteropancreatic (GEP) tumors, carcinoid tumors, insulinoma, pheochromocytoma, and lung cancers, are most common ones where a predominant expression of SSTRs is observed.
3
The therapeutic potential of SST is limited due to its short half-life. Hence, enzymatically stable synthetic SST analogs such as octreotide, lanreotide, and vapreotide, are used for the treatment of tumors expressing SSTRs and these analogs exhibit varying affinity toward different subtypes of SSTRs.
4,5
The use of somatostatin peptide analogs (SSTA), labeled with suitable diagnostic and therapeutic isotopes, has gained clinical significance since the 1990s, for management of various neuroendocrine tumors (NETs). Among several SSTA [
However, considering the easy availability, lower cost, and optimal decay characteristics of 99mTc, an SSTA radiolabeled with this radionuclide would naturally find wider applications. Additionally, as peptide receptor radionuclide therapy (PRRT) using 177Lu-DOTA-TATE is being routinely carried out in India, an indigenously developed single-vial kit for the formulation of 99mTc-HYNIC-TOC [HYNIC-2-Hydrazinonicotinic acid] proves particularly useful for preclinical screening-in of patients to carryout out PRRT. 68Ga-DOTA-TOC 15 –20 can be used for the same purpose, but its use constitutes a costly option for patients in most cases since 68Ga is sourced from the 68Ge/68Ga generator. In comparison, 99mTc-HYNIC-TOC would be a more affordable radiopharmaceutical, particularly in centers that do not have access to a 68Ge/68Ga generator.
Direct labeling of Octreotide with 99mTc is known to affect binding affinity, and the complex being lipophilic, limits its application for the detection of tumors in the gastrointestinal region. 21 HYNIC is a bifunctional chelating agent used for radiolabeling of biomolecules with 99mTc, which results in high specific activity radiotracers. The HYNIC group is conjugated to the pendant amine group of lysine in the biomolecule. HYNIC imparts advantage of site-specific conjugation, especially for small peptides, where modifications can adversely affect the binding affinity.
Since the HYNIC group does not have a sufficient number of donor atoms to complex with 99mTc, the use of suitable coligands is necessary. The use of different coligands, such as glucoheptonate, tricine, ethylenediamine diacetic acid (EDDA), and their combinations has been reported for the radiolabeling of HYNIC derivatives of biomolecule with 99mTc. 22 Monodentate coligands, such as water soluble triphenylphosphine sulfonates, have also been successfully used for radiolabeling HYNIC-peptide. 23 Among the different coligands, EDDA was found to be the most suitable for in vivo applications. 24 However, the use of EDDA alone usually results in poor radiolabeling yields. This problem was circumvented by using both tricine and EDDA as coligands. 25 Guggenberg et al. had reported formulation of a lyophilized HYNIC-TOC kit suitable for preparation of 2 patient doses of 99mTc-HYNIC-TOC. 26 The same formulation was used in the commercially available HYNIC-TOC kit vial (99mTc-Tektrotyd) manufactured and supplied by NCBJ.
Considering a higher density of cancer patients in Indian hospitals, the formulation of a lyophilized kit for the preparation of 4–5 patient doses, or more, of 99mTc-HYNIC-TOC was envisaged. Herein, the authors report the preparation of such a kit and its use in a clinical setup.
Materials and Methods
Hydrazinonicotinamide-Tyr3-octreotide (HYNIC-TOC) was purchased from M/s. Pi Chem. The chemicals tricine, EDDA, sodium phosphate dibasic heptahydrate, and sodium phosphate monobasic were purchased from M/s. Sigma Aldrich. Stannous chloride dihydrate was purchased from M/s. Riedel de Haan. Sodium pertechnetate was eluted from 99Mo/99mTc column generator using normal saline. Silica gel-based instant thin layer chromatography (ITLC) paper was purchased from M/s. Varian. The commercially available HYNIC-TOC kit, 99mTc-Tektrotyd (manufactured by NCBJ), used for comparing with the in-house developed HYNIC-TOC kit, was obtained as a gift from Tata Memorial Hospital. High performance liquid chromatography (HPLC) analyses were performed on a JASCO PU 2080 Plus dual pump HPLC system (HPLC software: JASCO-Borwin, Version 1.5), with a JASCO 2075 Plus tunable absorption detector and a Gina Star radiometric detector system, using a C18 reversed-phase HiQ Sil (5 μm, 4×250 mm) column. Lyophilization was carried out in a bench-top freeze drier (Martin Christ, GmBH, Model:Alpha 1–2 LD plus). The sterility test kit containing sterile fluid thioglycolate media and soybean casein media was obtained from Himedia Laboratories. The bacterial endotoxin test was carried out using FDA-approved Endosafe PTS instrument and cartridges for endotoxin detection (sensitivity: 0.5–0.05 EU/mL) procured from Charles River Laboratories Pvt. Ltd. The pH of the final preparation was determined by a narrow range nonbleeding pH paper procured from Merck.
Preparation of lyophilized HYNIC-TOC kits
The protocol for the preparation of a 30 vial batch of lyophilized HYNIC-TOC kits was optimized. A phosphate buffer (0.2 M, pH=6) was prepared by dissolving sodium phosphate dibasic heptahydrate (720 mg) and sodium phosphate monobasic (180 mg) in 30 mL of nitrogen purged autoclaved water for injection. EDDA (300 mg) and tricine (600 mg) were dissolved in 28 mL of 0.2 M buffer solution, and to this solution 1 mL of freshly prepared stannous chloride dihydrate (1.2 mg/mL) and 1 mg of HYNIC-TOC, dissolved in 1 mL of 10% aqueous ethanol, were added. The pH of this solution was 6. The solution was filtered through a 0.22-μm millipore filter, and 1 mL each was dispensed into 10 mL sterile vials. The vials were quickly frozen in a liquid nitrogen bath and lyophilized at −54°C for 7 hours. Lyophilized kits were sealed under a vacuum and then stored at −20°C. The whole process was carried out in a clean area.
Sterility and bacterial endotoxin test of lyophilized kit vial
A sterility test was carried out following the reported procedure. 27 The kit components were dissolved in 1 mL of sterile saline. About 0.5 mL of this solution was separately inoculated in a soybean casein digest medium and a fluid thioglycollate medium and incubated for 14 days. The former solution was incubated at 25°C and the latter was incubated at 35°C. Positive and negative controls were set up, along with each run of sterility test. Both the test solutions were inspected visually every week for 2 weeks and compared with the controls for any contamination. Bacterial endotoxins were determined quantitatively, using an Endosafe PTS unit from Charles River Laboratories. FDA-licensed disposable cartridges with a sensitivity range of 0.5–0.05 EU/mL were used with a 1:250 and 1:1000 dilution of kit components after reconstitution in 1 mL saline. PTS cartridge used for BET contains a precise amount of licensed Limulus Amebocyte Lysate (LAL) reagent, chromogenic substrate, and control standard endotoxin. The test sample added in the sample reservoir of the cartridge is drawn and mixed with LAL reagents, incubated, and combined with a chromogenic substrate. Optical density was measured and analyzed against an internally achieved batch-specific standard curve. Spike recovery values for all bacterial tests were obtained in the range of 50–200%, indicating no interference from the test sample either by inhibition or enhancement on LAL activity, ensuring the validity of endotoxin test results.
Preparation of 99mTc-HYNIC-TOC using lyophilized HYNIC-TOC kit
99mTc-HYNIC-TOC was prepared by adding 20–80 mCi (740–2960 MBq) of freshly eluted 99mTc-sodium pertechnetate activity in 1–3 mL volume of sterile saline to the lyophilized kit vial and heating the vial in a water bath at 100°C for 20 min.
High-performance liquid chromatography
About 15 μL of the 99mTc-HYNIC-TOC preparation (∼0.37 MBq) was injected into the HPLC column, and elution was monitored by observing the radioactivity profile. Acetonitrile and water, both containing 0.1% trifluoroacetic acid, were used as elution solvents with the following gradient elution program: 0–3 minutes 100% water, 5 minutes 70% water, 5–18 minutes 70% water, 22 minutes 50% water, 22–24 minutes 50% water, and at 25 minutes, again, 100% water. The flow rate was maintained at 1 mL/min. The radiochemical purity (RCP) of the complex was calculated from the peak area measurements from the chromatogram.
Instant thin layer chromatography
About 2 μL (1–2 μCi) of the 99mTc-HYNIC-TOC preparation was spotted on two separate Varian ITLC strips (11 cm long) at a distance of 1 cm from the bottom of the strip. One strip (Strip A) was developed in methyl ethyl ketone (MEK) and the other strip was developed in acetonitrile:water (1:1, v/v) (Strip B) unitl the solvent reached 1 cm from the top of the strip. To determine the RCP of 99mTc-HYNIC-TOC, the strips were dried, cut into two equal segments, and the activity associated with each segment was measured in a NaI(Tl) counter with the energy window set for 99mTc. Thereafter, RCP was determined using the following equation, where A
top=Activity of strip A top segment, A
total=Total activity of strip A, B
bot=Activity of strip B bottom segment, and B
total=Total activity of strip B.
To obtain the distribution pattern of 99mTc-HYNIC-TOC on ITLC in MEK and acetonitrile:water (1:1, v/v), the strips developed in respective solvents, as discussed above, instead of cutting into two segments were cut into 1-cm segments and the activity (counts/min) associated with each segment was determined using a well-type Na(I)Tl counter with the energy window set for 99mTc. A plot was made with the count rate as the Y-axis and the length of the strip as the X-axis.
Determination of pH of the reconstituted solution
The pH of 99mTc-HYNIC-TOC prepared using the lyophilized kit vial was determined using a narrow range nonbleeding pH paper. About 2 μL of the radioactive solution was applied to the pH paper, and the color pattern obtained was matched with the standard color pattern supplied by the manufacturer to determine the pH.
Stability studies of lyophilized HYNIC-TOC kit
Performance of the lyophilized HYNIC-TOC kits was evaluated over a period of 9 months. 99mTc-HYNIC-TOC was prepared using these vials every month for nine consecutive months. RCP, determined by HPLC as well as ITLC, was considered to be an indicator of the stability of the lyophilized kit.
Stability studies of 99mTc-HYNIC-TOC prepared using the lyophilized HYNIC-TOC kit
Room temperature stability of 99mTc-HYNIC-TOC, prepared using the lyophilized kit vial, was assessed by determining its RCP 6 hours postpreparation by the HPLC as well as the ITLC method, as described above.
Biodistribution studies
All procedures performed herein were in strict compliance with the national laws governing the conduct of animal experiments. Biodistribution studies were performed on normal Swiss mice at four different time points. About 100 μCi (∼3.7 MBq) of the radioactive preparation in 100 μL was administered intravenously through the lateral tail vein. Individual sets of animals (n=4) were utilized for studying the biodistribution at different time points (30 minutes, 1, 2, and 4 hours). At the end of the respective time periods, the animals were sacrificed and the relevant organs excised. The organs were weighed and the activity associated with them was measured in a flat-bed type NaI(Tl) counter with an energy window suitable for 99mTc. The activity retained in each organ/tissue was expressed as a percent of the injected dose per gram (% ID/g).
Clinical imaging
For imaging, a dose of 370–555 MBq (10–15 mCi) of 99mTc-HYNIC-TOC was injected intravenously in patients suspected to have GEP-NETs. After 1 hour postinjection (p.i.), patients underwent whole body scanning followed by a regional SPECT/CT of the primary and metastatic sites. No contrast agent was used. The whole body images were acquired at a table speed of 8 cm/min in a dual head gamma camera (Siemens Symbia T equipped with an LEHR collimator, with an energy window of 140 KeV±15%).
In the SPECT/CT system, the CT acquisition was performed with a slice thickness of 4 mm and a pitch of 1 on a helical dual-slice CT unit. Images were acquired using a matrix of 512×512 pixels and a pixel size of 1 mm. Additional spot views were obtained when necessary. SPECT data were acquired using a matrix of 128×128 pixels and a slice thickness of 1.5 mm. CT-based attenuation correction of the emission images was used. SPECT images were reconstructed by an iterative method ordered subset expectation maximization (two iterations and nine subsets).
Results and Discussion
Higher population density of cancer patients per hospital in India provided the necessary impetus to explore the possibility of formulating a single-vial kit capable of preparing 4–5 patient doses (60–80 mCi). Guggenberg et al. had earlier reported preparation of a lyophilized HYNIC-TOC kit suitable for preparing up to 2 patient doses. 26 The present kit was developed in similar lines using HYNIC-TOC, EDDA, and tricine as coligands and stannous chloride as the reducing agent. The kit preparation reported by Guggenberg et al. contained 20 μg of HYNIC-TOC, 10 mg of EDDA, 20 mg of tricine, and 20 μg of SnCl2·2H2O. The procedure for the reconstitution of the kit involved the addition of a stipulated volume of a 0.2 M phosphate buffer followed by 99mTc-sodium pertechnetate. The maximum total volume that can be added to the kit vial was capped at 2 mL, and the maximum recommended activity that can be used with the kit was 2 GBq (54 mCi). 26 The intention was to prepare a single vial kit that can be used with activity as high as 2.9 GBq (∼80 mCi) and to include the required buffer in the kit itself so that no pH adjustment is required at the time of reconstitution. Guggenberg et al. had shown that good quality images could be obtained with a peptide amount of 5–15 μg/patient. The authors, therefore, decided to use ∼30 μg of HYNIC-TOC to prepare 4–5 patient doses. Also, since the aim was to prepare a kit that can take activity as high as 80 mCi in volume up to 3 mL, the authors decided to increase the amount of stannous chloride dihydrate to 40 μg per kit instead of 20 μg per kit reported by Guggenberg et al. 26
Kit preparation and quality control
Protocol for the preparation of a 30 vial batch of lyophilized HYNIC-TOC kits is described in the experimental section. Each lyophilized kit vial contained 33 μg of HYNIC-TOC, 10 mg of EDDA, 20 mg of tricine, 40 μg SnCl2·2H2O, 22.4 mg of sodium phosphate dibasic, and 5.6 mg of sodium phosphate monobasic as ingredients. Inclusion of an appropriate buffer took care of the final pH (6–7) of the formulation and this avoided the need of addition of buffer solution to the kit vial at the user end.
As per regulatory requirements, the quality of the lyophilized HYNIC-TOC kit was assured by determining pharmaceutical purity of randomly drawn kits from each batch. All the kit vials tested were found to be sterile and the endotoxin level in the kit vial was within permissible limits (<25 EU/mL).
Preparation and quality control of 99mTc-HYNIC-TOC
99mTc-HYNIC-TOC was prepared using the lyophilized kit following the protocol described in the experimental section. Formation of the complex and its RCP was determined by HPLC as well as ITLC. Typical HPLC and ITLC patterns obtained for 99mTc-HYNIC-TOC are shown in Figure 1a–c. In HPLC, 99mTc-HYNIC-TOC complex appeared as a single peak at 17.8±0.5 min, whereas the peak representing 99mTc-sodium pertechnetate was observed at 3.9±0.5 min. The RCP of 99mTc-HYNIC-TOC determined from HPLC peak area measurements was consistently >90%.
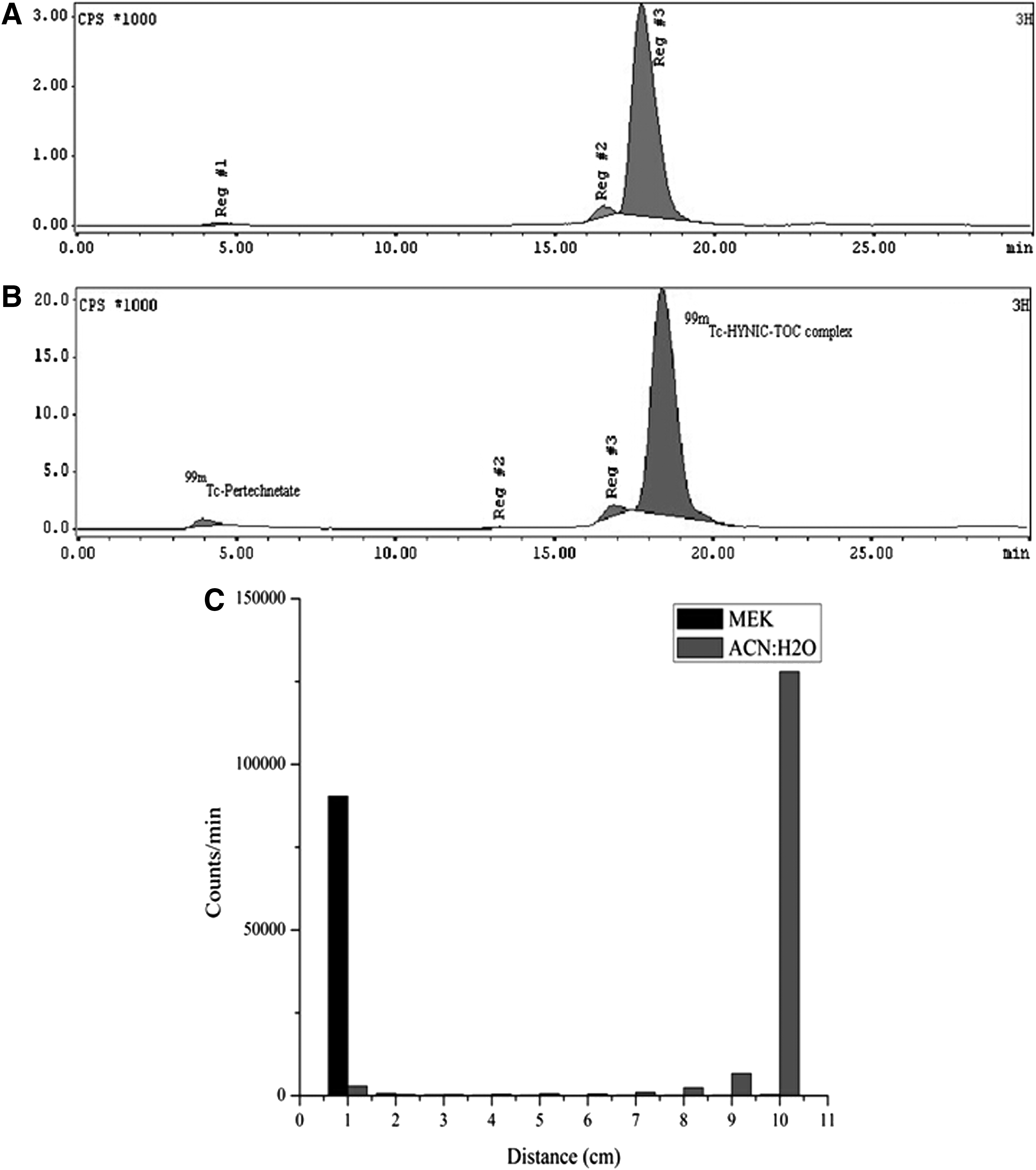
RCP of the preparation was also determined by ITLC in two different solvent systems (MEK and acetonitrile:water (1:1, v/v). Figure 1c shows a typical ITLC pattern obtained in MEK as well as acetonitrile:water. In MEK, pertechnetate moves with the solvent front, while 99mTc-HYNIC-TOC and reduced technetium (99mTcO2), if present, remains at the point of spotting. In the acetonitrile/water solvent system, pertechnetate as well as 99mTc-HYNIC-TOC move with the solvent front, while reduced technetium remains at the point of spotting. Using the equation given in section “Instant thin layer chromatography” and in section “Materials and Methods,” it is possible to calculate the % RCP of 99mTc-HYNIC-TOC (A top in the equation represents the activity of 99mTcO4 −, while B bot represents the activity due to reduced technetium. Similarly, A total and B total represent the total activity associated with respective strips).
The 99mTc-HYNIC-TOC solution was visually inspected for clarity, and its pH was also determined. The quality control checklist for 99mTc-HYNIC-TOC preparation is shown in Table 1.
Results obtained for Batch 1.
The 99mTc-HYNIC-TOC prepared in-house was also compared with 99mTc-HYNIC-TOC prepared using a commercially available kit vial following the protocol recommended by the manufacturer. The RCP of 99mTc-HYNIC-TOC prepared using the commercial kit was 95.3% by HPLC. Figure 1b shows the HPLC elution profile of 99mTc-HYNIC-TOC prepared using the commercial kit vial. It could be observed that Figure 1a and b show identical retention time in the radioactivity elution profile indicating their equivalence.
The kit vial prepared in-house was gradually challenged with the increasing level of 99mTc-sodium pertechnetate activity (20–80 mCi, 740–2960 MBq) in 1–3 mL volume. In all cases >90% RCP could be achieved (Table 2). It is pertinent to note that kinetics of complex formation was not affected even with 3 mL (volume tested so far) of 99mTc-sodium pertechnetate. Although the recommended maximum activity that can be used in the present kit is 2960 MBq, the authors have observed that even by using activity as high as 4810 MBq (130 mCi) in 3 mL volume, 99mTc-HYNIC-TOC can be prepared in more than 90% RCP (data not presented).
HPLC, high performance liquid chromatography; ITLC, instant thin layer chromatography.
The commercial kit requires the addition of a stipulated volume of 0.2 M phosphate buffer, which restricts the volume of 99mTc-sodium pertechnetate that can be added to the kit vial. This in turn limits the patient doses that can be prepared using a single kit vial. For example, if the volume of pertechnetate that could be added to the commercial kit vial is 1 mL and the specific concentration of the generator eluate is 15 mCi/mL (which may be the case at the end of the 99Mo/99mTc generator life), then only a single patient dose can be prepared using a single commercial HYNIC-TOC kit vial. However, using the kit reported here, up to 3 patient doses (3 mL×15 mCi/mL=45 mCi) of 99mTc-HYNIC-TOC could be prepared under the same condition.
Stability of lyophilized HYNIC-TOC kit and 99mTc-HYNIC-TOC prepared using lyophilized HYNIC-TOC kit
The stability of the lyophilized kits, stored at −20°C, over a period of 9 months from the date of preparation was also studied. This is done by preparing 99mTc-HYNIC-TOC using these kits and determining its RCP. Table 3 shows the RCP of 99mTc-HYNIC-TOC prepared using kits at different time intervals up to 9 months. No significant decrease in RCP of the 99mTc-HYNIC-TOC was observed during the period of study. Stability of the 99mTc-HYNIC-TOC complex 6 h postpreparation was assessed by HPLC. No significant degradation of the complex was observed during this interval (Table 4).
RCP, radiochemical purity.
Biodistribution studies
Biological studies of the 99mTc-HYNIC-TOC complex prepared using the lyophilized kit vial were carried out in normal Swiss mice. Distribution of 99mTc-HYNIC-TOC observed in various organs and tissue at different time points is shown in Table 5. More than 90% of injected activity was eliminated within 4 hours predominantly through the renal route, as expected with 99mTc-HYNIC-TOC complexes. 28 A fraction of activity was also cleared through the hepatobiliary route, as is evident from the presence of activity in the gastrointestinal tract. There is no significant uptake of activity in any other major organs, such as the heart, lungs, spleen, and bone. About 4.89 (3.0)% ID/g of activity was observed in muscles. However, the activity cleared with time with no detectable level of activity in the muscle at 4 hours p.i. Similar to the case of muscle, about 4.37 (0.3)% ID/g of activity was found in blood initially, which cleared with time.
% ID/g, percent of the injected dose per gram; p.i., postinjection; BG, background.
Clinical studies
Authorization for the manufacture and supply of cold kits in India was obtained from the Radiopharmaceutical committee and the institutional regulatory authority, after submitting the required data. To assess the performance of the HYNIC-TOC kit in the clinical setup, limited clinical trials were carried out in patients known to have NETs, subsequent to obtaining necessary ethical clearances from the competent authority at the hospital end. Scintigraphy images were obtained as described in the experimental section. Figure 2 shows the images obtained using 99mTc-HYNIC-TOC in 3 patients after 1 hour p.i. While 99mTc-HYNIC-TOC planar or SPECT/CT detected metastases in all three patients, conventional imaging (X-ray, CT-scan, or ultrasound scan) detected metastases only in 2 patients. In all 3 patients, one or two additional metastatic lesions were detected with 99mTc-HYNIC-TOC, which the conventional imaging has missed. Thus, on a lesion by lesion basis, 99mTc-HYNIC-TOC planar or SPECT/CT was found to be superior to conventional imaging.
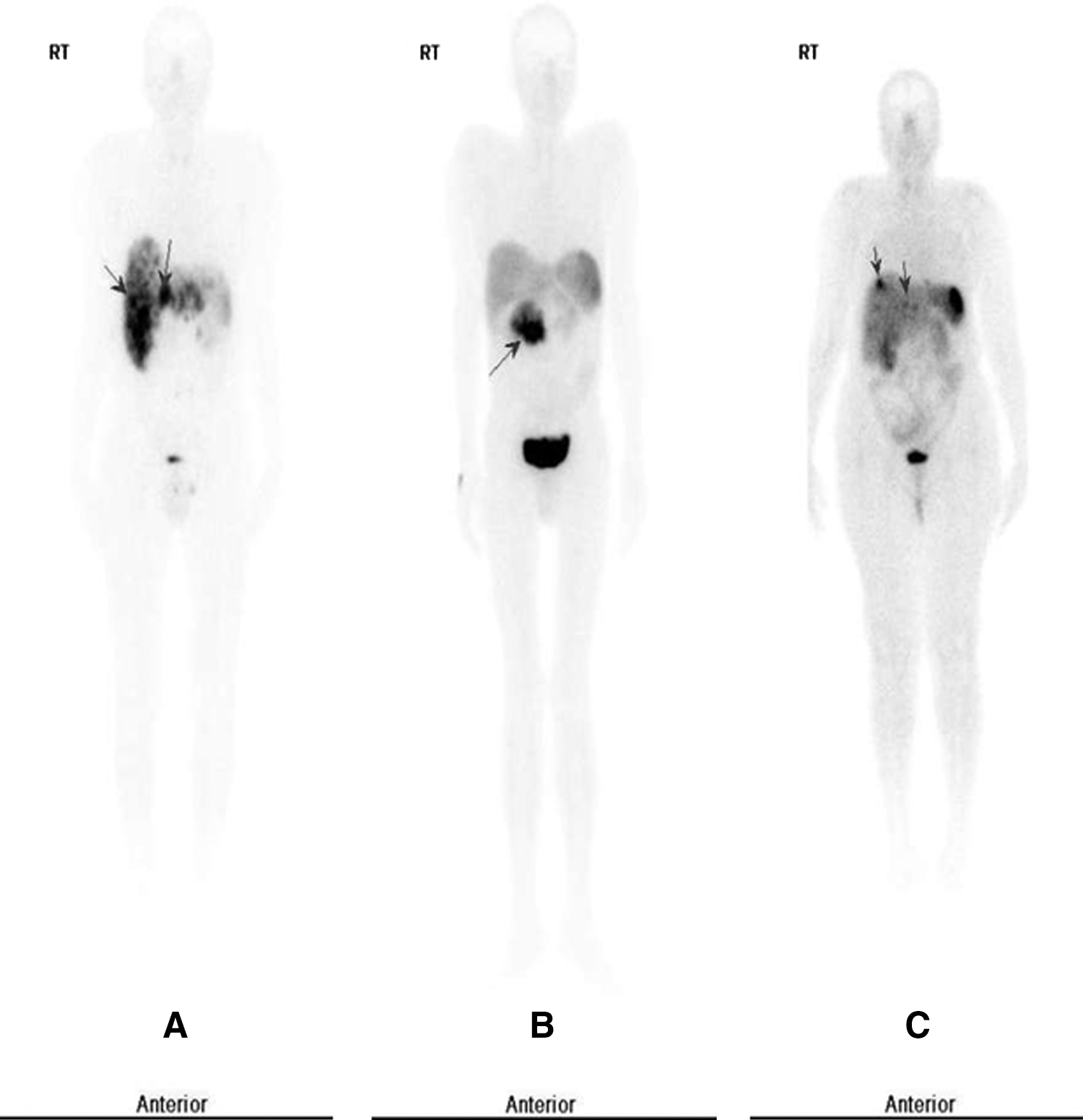
Planar images (at 1 hours p.i.) obtained in 3 patients having NET using 99mTc HYNIC-TOC. In
The high rate of positivity obtained with in vivo 99mTc-HYNIC-TOC planar or SPECT/CT is consistent with high-affinity STT-binding sites, which have been found in vitro on most well-differentiated gastroenteropancreatic endocrine tumors. The detection of a high degree of SSTR expression can be exploited to treat patients with cold octreotide therapy and PRRT.
Conclusions
A single vial lyophilized kit for the preparation of 99mTc-HYNIC-TOC with desired radiochemical and pharmaceutical purity was prepared, and its suitability for clinical application is demonstrated. The present kit, which can be used for the preparation of multipatient doses of 99mTc-HYNIC-TOC, avoids the addition of buffer solution during kit reconstitution at the user end, thus simplifying the procedure. An additional advantage of the present kit is that it permits addition of up to 3 mL of pertechnetate, which allows preparation of multipatient doses of 99mTc-HYNIC-TOC with high RCP even when specific concentration (activity/mL) of pertechnetate obtained from the generator is low. Limited clinical studies reported here also demonstrated the efficacy of the product for imaging neuroendocrine tumors that express SSTRs.
Footnotes
Acknowledgments
The authors are thankful to Dr. Meera Venkatesh, former Head of Radiopharmaceuticals Division, for initiating this work. The technical insights and support provided by Prof. M.R.A. Pillai, former Head of Radiopharmaceuticals Division, in the clinical translation of the radiopharmaceutical from laboratory to patients are being gratefully acknowledged. The authors also thank Dr. K.L. Ramakumar, Director, RC & I Group and Dr. Gursharan Singh, Associate Director (I) RC & I Group, BARC, for their support.
Disclosure Statement
The authors declare that they have no conflict of interest.