
Abstract
Objective:
To explore the role of CDC25B, PED/PEA-15 in the development of esophageal carcinoma and its influence on the prognosis.
Methods:
Fluorescence quantitative real-time PCR and immunohistochemistry methods were used to analyze the expression of CDC25B, PED/PEA-15 in esophageal carcinoma. Moreover, survival analysis was done using the Kaplan–Meier method.
Results:
In 66 cases of esophageal cancer tissues, the relative content of CDC25B mRNA was 16.22 (13.93–18.90). The positive expression rate of CDC25B protein was 48.5%, significantly higher than normal mucosa tissues (0%) (p<0.01). The relative content of PED/PEA-15 mRNA was 12.47 (10.41–14.93). The positive expression rate of PED/PEA-15 protein was 68.2%, significantly higher than normal mucosa tissues (17.6%) (p<0.01). The CDC25B protein expression was correlated with differentiation grade and depth of invasion (p<0.05). The PED/PEA-15 protein expression was related to differentiation grade, lymph node metastasis, and depth of invasion (p<0.05). Survival analysis showed that the mean survival time of PED/PEA-15-positive expression group was lower compared with the negative expression group (χ 2=5.549, p=0.018). Analysis of the relationship between CDC25B and PED/PEA-15 suggested that there was a positive correlation between them (r=4.061, p=0.044).
Conclusion:
Both CDC25B and PED/PEA-15 play a certain role in the carcinogenesis of esophageal cancer, and PED/PEA-15 has a greater influence on postoperative survival time. They will be the new diagnostic/therapeutic targets in esophageal carcinoma.
Introduction
Esophageal carcinoma is a common malignant tumor of upper gastrointestinal tract. Currently, it is the eighth most common incident cancer in the world because of its extremely aggressive nature and poor survival rate. More than 90% of esophageal cancers worldwide are esophageal squamous cell carcinomas (ESCCs). 1 The major reason for high mortality is that most patients have entered the advanced stage when they receive treatment.
The occurrence of esophageal carcinoma is a progressive evolution process with multifactor, multistage, and multiple genes involved. The CDC25 family includes three homologous isomers (CDC25A, CDC25B, and CDC25C), which is a group of Thr/Tyr bifunctional enzymes. 2,3 Also, CDC25B is a potential cancer gene whose protein itself is tumor derived and highly expressed in many tumors. 4 –6 PED/PEA-15 is a kind of small-molecule protein with the function of broad-spectrum resistance to apoptosis. Meanwhile, it arouses people's concern because of the special molecular structure. 7 Therefore, CDC25B and PED/PEA-15 may open up a new approach and idea for the diagnosis and therapy of tumor as target proteins.
At present, the molecular mechanism of esophageal carcinoma is still unknown. This study explores the role of CDC25B and PED/PEA-15 in the process of occurrence and development of esophageal cancer, to provide theoretical foundation for uncovering the mechanism of esophageal cancer and finding the potential molecular markers as therapeutic targets.
Materials and Methods
Patients and samples
A total of 66 cases of advanced esophageal carcinoma (ESCC) were involved in this study. They were selected randomly and had the characteristics of universality and representativeness. The patients with esophageal cancer had undergone curative tumor resection at Cangzhou Central Hospital from January to December 2008. The resected surgical specimens were fixed in 10% formaldehyde, processed through graded ethanol, and embedded in paraffin. Also, the corresponding paraffin blocks of cancer tissues were saved for standby application. Among these cases, there were 43 males and 23 females. The mean age of all the patients was 54.9 years. Pathological diagnosis was done by two clinical pathologists of high quality. The 66 cases of ESCC were divided into different types according to the WHO 1990 esophageal cancer diagnosis standard. Among them, 10 cases were well differentiated and 56 cases were moderately/poorly differentiated; 45 cases were with lymph node metastasis and 21 cases were with no lymph node metastasis; 38 cases infiltrated through the fiber membrane, 16 cases invaded the muscular layer, and 12 cases invaded the mucous layer or submucosa. All the cases had no preoperative radiation and chemotherapy. Moreover, the postoperative follow-up data were integral. At the same time, 40 cases of normal esophageal tissue paraffin blocks, taken from the part with more than 5 cm distance from tumor margin, were used as the control group. Cases were followed up from the first day of surgical treatment to December 31, 2013. All subjects were informed and consented to participate in this study, which was also approved by the Affiliated Hospital of Hebei University Ethics Committee.
Main reagents
The paraffin tissue DNA extraction kit (DEXPAT™) and Taq DNA polymerase were purchased from Takara Bio Company. Real-time quantitative PCR (RT-qPCR) detection kit (SYBR Green® Real time PCR Master Mix) was purchased from Toyobo Company. The rabbit anti-human CDC25B polyclonal antibody (50×), rabbit anti-human PED/PEA-15 polyclonal antibody (100×), and horseradish peroxidase (HRP) goat anti-rabbit IgG were all purchased from Santa Cruz company. The Streptavidin-Peroxidase (SP) Immunohistochemistry Kit and 3,3N-Diaminobenzidine Tetrahydrochloride (DAB) Chromogenic Reagent Kit were purchased from Beijing Zhongshan Jinqiao Biotech Co., Ltd. All the primers were synthesized by the Sangon Biotech Co., Ltd. The sequences of primers were as follows: CDC25B forward primer: 5′-CTCATTAGTGCCCCACTGGT-3′, CDC25B reverse primer: 5′-ATCAGCTCTCGGTGGTCACT-3′; PED/PEA-15 forward primer: 5′-TACCACTGAGCC TGAGATG-3′, PED/PEA-15 reverse primer: 5′-GGTTTCCTAA GTAAGTCCCT-3′; and GAPDH forward primer: 5′-AGAAGGCT GGGGCTCATTTG-3′, GAPDH reverse primer: 5′-AGGGGCCATCCACAGTCT TC-3′.
Extraction of genomic DNA
Paraffin tissue DNA extraction was operated according to the instructions of the DEX-PAT kit. Three to five slices of 10 μm paraffin sections were put into a 1.5-mL tube and 10 drops of DNA extraction liquid (0.5 mL DEXPAT) were added then. The mixture was fully blended, heated at 100°C for 10 minutes, and centrifuged at 12000 rpm for 10 minutes. Then, the supernatant (extracted DNA) was drawn and directly used for RT-qPCR. The DNA content was measured by an ultraviolet spectrophotometer and its quality was determined by 1% agarose gel electrophoresis.
Real-time quantitative PCR
The RT-qPCR test was done according to the instructions of SYBR Green Real Time PCR Master Mix kit. Extracted DNA was divided into three groups, respectively, with CDC25B, PED/PEA −15, and GAPDH gene (as a reference gene) primers for fluorescence quantitative real-time PCR amplification. The RT-qPCR solution contained the components of 16 μL PCR grade water, 25 μL SYBR Green Real Time PCR Master Mix, 0.4 μM forward primer, 0.4 μM reverse primer, and 10 ng template DNA (extracted DNA). A three-step cycle operation was conducted and the cycling condition was set as follows: predenaturation at 95°C for 1 minute initially, followed by 40 cycles of denaturation at 95°C for 15 seconds, annealing at 55°C–65°C for 15 seconds, and extension at 72°C for 45 seconds; finally, data were collected. Every experiment was repeated for thrice and the average Ct value was calculated. The experimental data were analyzed by Multiplex Quantitative PCR System software using the housekeeping gene GAPDH as a reference, and the difference between target gene expression and GAPDH gene expression in each sample was indicated as ΔCt=Cttarget−CtGAPDH. 2−ΔCt was the relative expression quantity of target gene expression to reference gene expression. The expression difference between two genes in different tissues was judged by comparing the 2−ΔCt value of tumor group with that of normal group.
Immunohistochemical analysis
Specimens were fixed in 10% neutral formaldehyde immediately after resection and dehydrated by gradient alcohol following the steps of 70% ethanol for 1 hour, 80% ethanol for 2–4 hours, 95% ethanol for 2–4 hours, 95% ethanol for 2–4 hours, 100% ethanol for 2–4 hours and 100% ethanol for 2–4 hours. Then, the tissues were embedded in paraffin with melting point as 52°C–54°C. Paraffin specimens of ESCC tissues and normal tissues were sectioned into 3–5 μm slices and dewaxed conventionally. After treatment for 30 minutes with 1% H2O2-methanol liquid, the samples were put into 92°C–98°C citric acid/sodium citrate buffer solution (0.01M,PH6.0), microwaved for 10 minutes, and then washed thrice with a PBS buffer, 5 minutes every time. Sheep serum (1%) was used to block the antigen for 20 minutes and CDC25B/PED/PEA-15 antibodies were dropwise added. The reaction proceeded in the refrigerator overnight at 4°C. IgG-HRP was added and incubated at 37°C for 40 minutes in a humidified box, followed by the avidin–biotin–peroxidase complex (1:100) added; the sample was incubated at 37°C for another 40 minutes in the humidified box. Then, it went through DAB chromogenic reaction, dehydration, transparency, and sealing. The PBS buffer was used as the blank control instead of first antibody. Normal sheep serum was used as the negative control instead of first antibody. Known hepatocellular carcinoma tissues with CDC25B- or PED/PEA-15-positive expression were used as the positive control.
Immunohistochemical results were assessed referring to the criteria reported, 8 and the expression of protein was evaluated according to the frequency of positive staining in the cytoplasm or nucleus of cancer cells. Ten different horizons were selected randomly to double-blind count at high magnification. One hundred cells were assessed for each high-power field. The expression was classified as positive (+) in cases with more than 50% positively stained cells, with other samples being classified as negative (−).
Statistical analysis
All the statistical results were handled by SPSS17.0 and Matlab7.0 software. The chi-square test was used to compare the positive rate. Measurement data were in terms of (mean±standard error). The t test or Mann–Whitney U test was used for the comparison between two groups. Significant difference was defined as p<0.05. The Kaplan–Meier method was adopted to carry on survival analysis.
Results
Detection of CDC25B and PED/PEA-15 genes mRNA expression
The Ct value data of target gene and reference gene were processed using formula. 2−ΔΔCt was the multiple relationship of the amount of gene expression between groups. The calculation formula of Ct value (mean±standard error) difference between two groups was
ΔCt=CDC25B Ct value (or PED/PEA-15 Ct value)-GAPDH Ct value; ΔΔCt=ESCC group ΔCt value - Normal group ΔCt value; 2−ΔΔCt=ESCC relative to Normal group.
Detection of CDC25B and PED/PEA-15 protein expression
CDC25B-positive products of ESCC were located in the nucleus in the form of tan particles, while CDC25B expressed weakly only in basal layer cells in the normal mucosa (Fig. 1). The positive expression rate of CDC25B protein in ESCC was 48.5%, which was significantly higher than normal mucosa tissues (0%) (p<0.01).
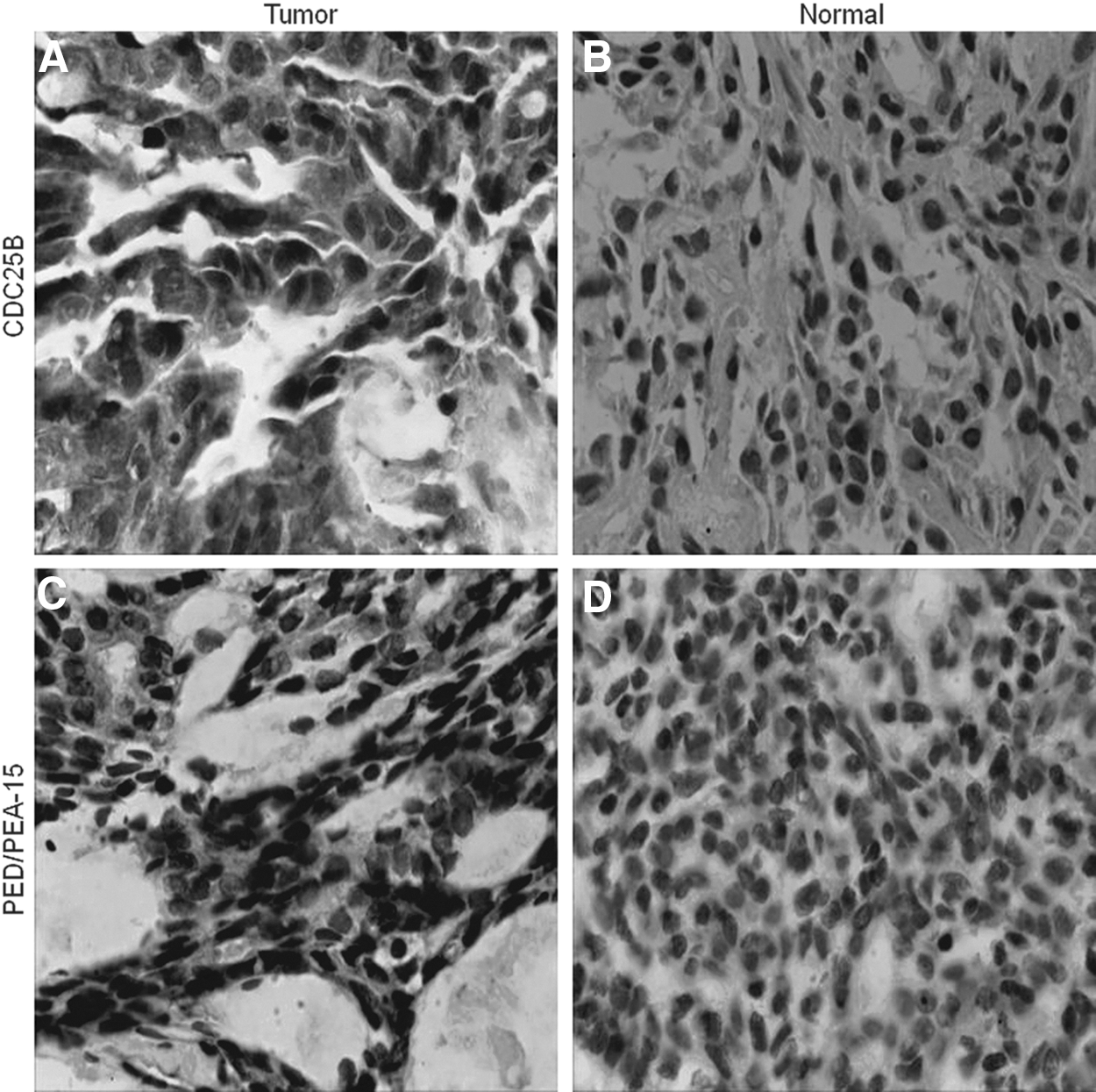
Immunohistochemical detection of CDC25B and PED/PEA-15 (×200).
PED/PEA-15-positive staining was located in the cytoplasm. The cell nucleus and cell membrane were not colored visibly (Fig. 1). The positive expression rate of PED/PEA-15 protein in ESCC was 68.2%, while that in normal esophageal tissue was 17.6%. Difference between them was significant (p<0.01).
Relationship between expression of CDC25B and PED/PEA-15 and clinical pathological features
The positive expression rate of CDC25B protein in the well-differentiation group was 30%, lower compared with the moderately/poorly differentiation group (51.8%) (p<0.01).
Among patients with tumor invasion to mucous membrane layer, the positive expression rate of CDC25B was 25.0%. As for patients with tumor invasion to fibrous membrane, the positive expression rate of CDC25B was 65.8%. The positive expression rate of CDC25B was 25.0% among those with tumor invasion to muscular layer. The CDC25B protein expression was not correlated with gender, age, and lymph node metastasis (p>0.05), although related with the differentiation grade and depth of invasion (Table 2).
The positive expression rate of PED/PEA-15 protein in the well-differentiation group was 20%, lower compared with the moderately/poorly differentiation group (76.8%) (p<0.01). The positive expression rate of PED/PEA-15 protein in the lymph node metastasis group was 88.9%, significantly higher than that without lymph node metastasis (23.8%) (p<0.01). Among patients with tumor invasion to mucous membrane layer, the positive expression rate of PED/PEA-15 was 41.7%. Among patients with tumor invasion to fibrous membrane, the positive expression rate of PED/PEA-15 was 84.2%. Among patients with tumor invasion to muscular layer, the positive expression rate of PED/PEA-15 was 50.0%. The PED/PEA-15 protein expression was not correlated with gender and age (p>0.05), while affected by differentiation grade, lymph node metastasis, and depth of invasion (Table 2).
Survival analysis
Long-term follow-up was conducted to 66 patients with esophageal cancer. Results of survival analysis for patients showed that the mean survival time of CDC25B-positive expression group was (27.19±3.18) months and that of negative expression group was (32.77±3.31) months, with no statistically significant difference (χ 2=1.945, p=0.163) (Fig. 2). The mean survival time of PED/PEA-15-positive expression group was (23.57±2.87) months and that of negative expression group was (37.67±3.88), with significant difference (χ 2=5.549, p=0.018) (Fig. 2).
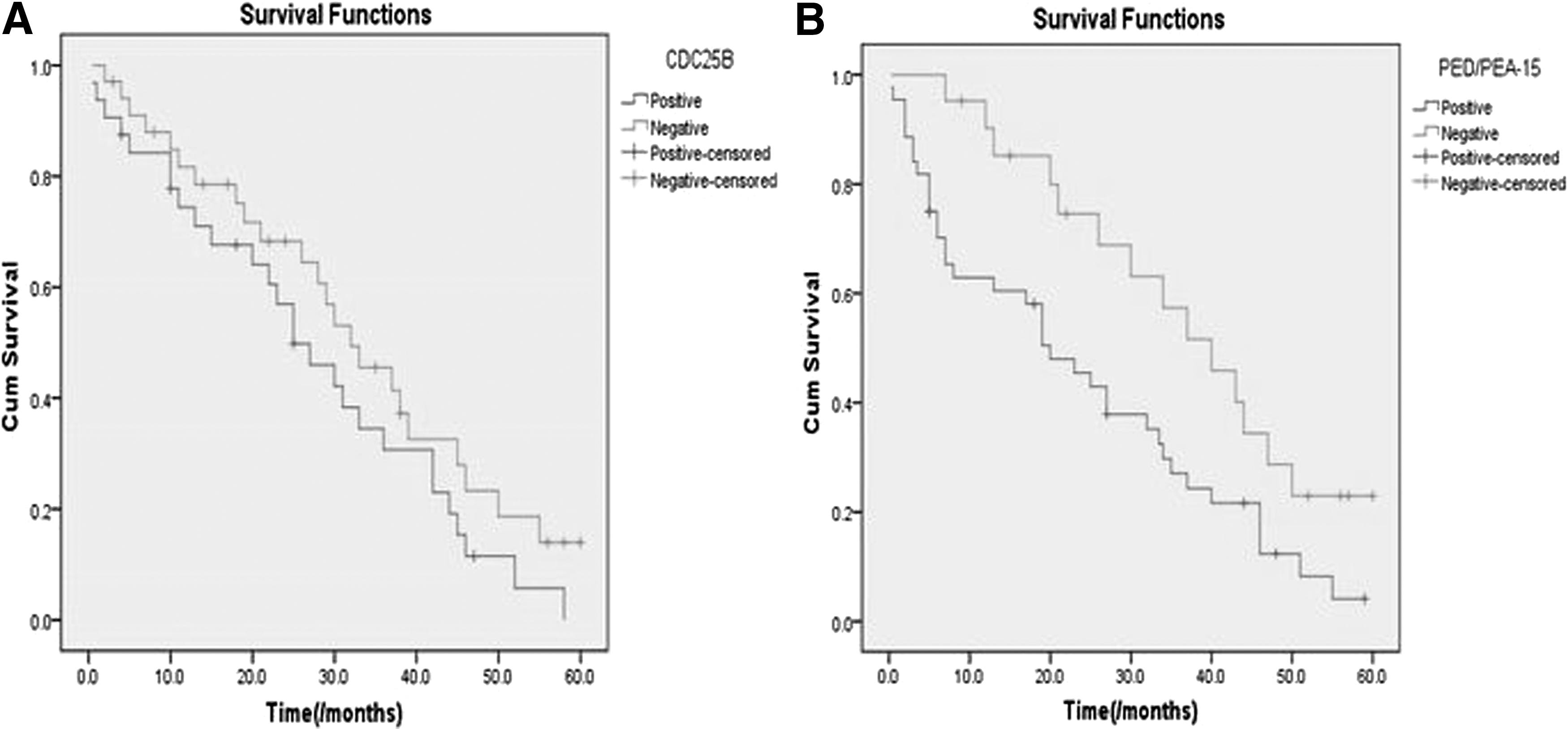
Kaplan–Meier curves for CDC25B and PED/PEA-15 expressions associated with postoperative survival time.
Correlation analysis of CDC25B and PED/PEA-15 in ESCC
Among 66 cases of esophageal cancer patients, 22 cases from the CDC25B-positive expression group (a total of 32 cases) also showed PED/PEA-15-positive expression. Meanwhile, 19 cases from the CDC25B-negative expression group (34 cases) also showed PED/PEA-15-negative expression. Analysis of the relationship between CDC25B and PED/PEA-15 suggested that there was a positive correlation between them (r=4.061, p=0.044) (Table 3).
Discussion
So far, multiple molecular changes have been found to closely relate to the occurrence, development, and metastasis process of esophageal cancer. 9 –11 CDC25B as the key factor of cell cycle regulation plays an important role in promoting cell mitosis and cell cycle progression. By inhibiting the activity of CDC25B phosphatase, the authors can control cell mitosis and cell cycle progression to suppress the growth of malignant tumor. 3 Studies have found that CDC25B is closely related to gastric cancer and colon cancer. 12,13 Besides, CDC25B is highly expressed in head and neck squamous cell carcinomas, nonsmall cell lung cancer, and ovarian cancer. 4,14,15 According to this study, CDC25B expressed highly in esophageal carcinoma and hardly expressed in normal esophageal tissues, which confirmed the previous studies 8,9 About the location of CDC25B, this problem is still controversial. Most reports found that it located in the cytoplasm, 8,16 other studies showed the nuclear expression. 17 This study suggested that the CDC25B protein mainly appeared in the nucleus. The cause of presenting different positioning may be related to the fact that CDC25B can shuttle between the nucleus and cytoplasm with the help of nuclear localization signal and (or) N-terminal nuclear export sequence. 18 –20 Moreover, the authors found that CDC25B had a correlation with the tumor differentiation degree and infiltration depth, except with lymph node metastasis. This was a divergent result compared with that from Nishioka et al. 8
Meanwhile, they detected that CDC25B had no significant effect on the mean survival time of postoperative patients, which was consistent to the report by Nishioka et al. that they did not find the correlation between positive CDC25B expression and a lower survival time. That the differences came up between this study and that of Nishioka et al. may be caused by the same characteristic of the small sample size. However, Sunada et al. 21 demonstrated that ESCC with positive CDC25B expression responded well to chemoradiotherapy, which might explain that CDC25B expression has little effect on survival time. Okumura et al. 22 summarized and evaluated the biomarkers for predicting the response and/or prognosis of ESCC patients treated with neoadjuvant chemoradiation therapy (CRT) and found cell cycle marker CDC25B had the potential as a response biomarker. Studies from Dong et al. 23 showed that detection of serum CDC25B-Abs was superior to the tumor markers (EA, SCC-Ag, and CYFRA21-1) for diagnosis of ESCC, and CDC25B-Abs was a potential prognostic serological marker for advanced ESCC. Briefly, all these studies indicated that CDC25B involved in the occurrence and development of esophageal carcinoma, and sensitivity to CRT.
A number of studies indicated that the expression amount of PED/PEA-15 protein increased in a variety of tumors and the level was related to the nature of tumor, differentiation degree, prognosis, and chemoradiotherapy. 24 –26 However, there have been few reports about the role of PED/PEA-15 protein in esophageal carcinoma. This study showed that the PED/PEA-15 protein expressed highly in esophageal carcinoma and may weakly express in normal esophageal tissues. PED/PEA-15 had correlation with the tumor differentiation degree, lymph node metastasis, and infiltration depth. By survival analysis, the authors found that the positive expression of PED/PEA-15 could shorten the average survival time of patients. Therefore, PED/PEA-15 has more important impact on the occurrence, development, and prognosis. Moreover, it is expected to become a tumor marker of esophageal carcinoma, with a broad prospect for further research. According to the study results of Fiory et al., 27 it was believed that increased PED/PEA-15 levels may affect tumorigenesis and cancer progression, as well as sensitivity to anticancer agents, which supported these results. In addition, there was a positive correlation between CDC25B and PED/PEA-15, which may be associated with the involvement of both proteins in G-protein-coupled receptor signaling to MAPK/Erk pathways 28,29 (Fig. 3). CDC25B plays an important role in cell cycle, triggering G2-M or G1-S transition. 30,31 PED/PEA-15 represents a common target for multiple kinases transducing survival signals triggered by growth factors and cytokines, supporting an important role of PED/PEA-15 in the cellular regulation of apoptotic programs. 32 Therefore, it can be speculated that G-protein-coupled receptor signaling to MAPK/Erk pathways takes part in the pathogenesis of ESCC.

G-protein-coupled receptor signaling to MAPK/Erk (cited from the product of Cell Signaling Technology, Inc.).
Footnotes
Disclosure Statement
The authors declare no conflicts of interest.