
Abstract
Purpose:
Although some algorithms are defined for the treatment of advanced hepatocellular carcinoma (HCC), the expected survival cannot be prolonged as it is intended. Treatment options for this group of patients are limited. Radioembolization with yttrium-90 (Y-90) microspheres is a new treatment modality, which has also been used in advanced HCC patients. In this study, the authors aimed to assess the efficiency of radioembolization with Y-90 microspheres and evaluate prognostic factors that influence the survival in HCC patients.
Patients and Methods:
The authors retrospectively evaluated data of 29 HCC patients who had radioembolization with Y-90 resin or glass microspheres between May 2009 and January 2014. Patient survival was evaluated by using the Kaplan–Meier method. Subgroup comparisons in terms of age, sex, prior treatment status before radioembolization, tumor burden, time between HCC diagnosis and radioembolization, alpha fetoprotein (AFP) level before radioembolization, presence of portal vein thrombosis (PVT), hepatopulmonary shunt ratio, extrahepatic disease burden, multifocality, bilaterality, Eastern Cooperative Oncology Group (ECOG), Child-Pugh, and Barcelona Clinic Liver Cancer (BCLC) status were performed to evaluate prognostic factors that affected survival.
Results:
There were 29 HCC patients (mean age: 59.9±12 years) in the patient group. Grade ≤1 and 2 ECOG performance status was present in 19 and 10 patients, respectively. Twenty-six patients were classified as Child A and 3 patients as Child B. According to the BCLC staging system, 18 patients were in stage B and 11 patients were in stage C. PVT was diagnosed in 12 patients. The median follow-up was 15 months. The median overall survival was 17±2.5 months. BCLC disease stage was a significant prognostic variable associated with survival, but other parameters, even the presence of PVT, were found to be not significantly affecting survival.
Conclusion:
Radioembolization provides favorable survival time in advanced HCC patients. Even patients who are not eligible for transarterial chemoembolization due to PVT can have radioembolization without a decrease in the median survival time.
Introduction
Hepatocellular carcinoma (HCC) accounts for 90% of all liver cancers, resulting in at least 500,000 deaths per year. 1 Algorithms, which are used for the treatment of advanced HCC, fail to prolong expected survival.
The curative treatment options include resection, transplantation, and percutaneous ablation for early-stage disease. Local palliative treatments, such as transarterial chemoembolization (TACE) or multikinase inhibitors, mainly sorafenib, are the choice of treatment for more advanced HCC. Radioembolization with yttrium-90 (Y-90) microspheres is another possible treatment option for this group of patients, which produces disease control rates of about 80%. 2
Radioembolization is usually indicated for intermediate- or advanced-stage patients who are poor candidates for TACE because of bulky/bilobar disease or portal vein thrombosis (PVT). 2 For this group of patients, which has limited options for treatment, radioembolization seems to be a promising choice of treatment when survival outcomes of studies with large patient populations are regarded. 3,4 Radioembolization can also be a treatment choice in patients who are slightly above the criteria of curative treatments and need downstaging of the tumor. 2
In this study, the authors aimed to evaluate the efficiency of radioembolization with Y-90 microspheres in advanced HCC patients and to determine prognostic factors, which influence the survival in this patient group.
Patients and Methods
The authors retrospectively evaluated data of 153 patients who had radioembolization with Y-90 microspheres between May 2009 and January 2014 in their department. From these patients, 29 HCC patients who had minimum follow-up of 6 months after radioembolization were included to this study. The institutional ethics board approved the study and all the patients provided informed consent.
The indication for Y-90 microsphere treatment was driven by an institutional board of specialists that included oncologists, hepatologists, surgeons, interventional radiologists, and nuclear medicine physicians. Hepatic disease was evaluated by a three-phase computed tomography (CT) or magnetic resonance imaging (MRI) of the liver. Radioembolization was considered if radical treatments such as resection, liver transplantation, radiofrequency ablation, or TACE were not convenient for the patients, mostly with large, infiltrating, and/or multifocal tumors, or who have PVT.
Hematological, liver function, blood biochemical tests, and physical examinations were performed in every patient. Patients with sufficient hematological parameters (granulocyte >1.5×109/L, thrombocyte >50×109/L), renal function (creatinine ≤2 mg/dL), and adequate liver function (total bilirubin ≤2 mg/dL, albumin ≥3 g/dL, and transaminase levels <5 times of institutional upper limit of normal range) were selected. Patients with signs of liver failure such as ascite and insufficient pulmonary reserve were not included among the candidates. Child-Pugh, Eastern Cooperative Oncology Group (ECOG), and Barcelona Clinic Liver Cancer (BCLC) status of the patients were evaluated. Patients with a Child-Pugh ≤7 score, ECOG 0–2, and BCLC B–C status were evaluated as the candidates for radioembolization. Patients with limited extrahepatic tumor burden, such as lymph nodes <2 cm, lung nodules <1 cm, and bone metastates, which would not affect survival, were not excluded from the candidates for radioembolization.
After being chosen as the candidate, a comprehensive angiographic evaluation was performed to every patient to detect possible parasitic arteries feeding the tumors and collateral vessels feeding extrahepatic organs and to evaluate portal blood flow. Aberrant hepatic vessels and extrahepatic collaterals were then embolized to avoid risk of extrahepatic leakage of Y-90 microspheres to the abdomen, especially to the gastrointestinal tract. Then, 5 mCi technetium-99m macroaggregated albumin (MAA) was injected to either the right or left hepatic artery according to the extent of the tumor. A whole body and a single-photon emission computed tomography (SPECT)-CT fusion imaging were performed after MAA-angiography for detection of radiation distribution in tumor, healthy liver parenchyma, lungs, and/or visceral organs. SPECT images of the upper abdomen were gathered with Siemens ECAM gamma camera. CT acquisitions of the same region were performed on spiral 4-slice CT (CT component of Biograph™ TruePoint™ PET-CT). The CT images and reconstructed SPECT images were evaluated after fusion images were rendered using Siemens SYNGO™ software. An elevated hepatopulmonary shunt or the failure to prevent deposition of microspheres in extrahepatic visceral organs such as the stomach and intestines was exclusion criteria for radioembolization. Within 1–2 weeks from MAA angiography, Y-90 resin (SIR-Spheres®) or Y-90 glass (TheraSphere®) microspheres were administered from the same route with MAA. For resin microsphere treatments, the doses were calculated according to the body surface area method and for glass microsphere treatments, the doses were calculated as per the manufacturer's instructions.
The follow-up data, including adverse events, hematological and liver function alterations, and changes in alpha fetoprotein (AFP) levels, were evaluated. Treatment response was evaluated with CT/MRI and/or F-18 fluorodeoxyglucose positron emission tomography–computed tomography (F-18 FDG PET-CT). Survival was calculated from the day of treatment by using the Kaplan–Meier method and subgroup comparisons were performed by the log-rank test. Univariate Cox regression modeling was performed for covariate adjustment. The authors applied a significant level p of 0.05 for each statistical test. They reported 95% confidence intervals (95% CIs) for estimated parameters.
Results
Twenty-nine HCC patients (22 males, 7 females) were included to the study. The median follow-up was 15 months (range: 1–49 months). A total of 22 (76%) death events were recorded.
The mean age at diagnosis of HCC was 59.9±12 years (range: 26–77 years). Seventeen patients were <65 years old and 12 patients were ≥65 years old. Grade ≤1 and 2 ECOG performance status was present in 19 and 10 patients, respectively. Liver function, which was classified by the Child-Pugh score, was Child A in 26 and Child B in 3 patients. According to the BCLC staging system, 18 patients were classified as stage B and 11 patients as stage C. Hepatitis B was recorded as the etiology in 13 patients and Hepatitis C in 3 patients. In the remaining patients, the etiologies were alcoholic, Budd–Chiari, autoimmune, hematochromatosis, and idiopathic liver diseases. Nineteen patients were therapy naive, whereas 10 patients had prior treatments (TACE in 4 patients, resection in 1 patient, TACE and resection in 1 patient, systemic therapy with sorafenib in 2 patients, systemic therapy with conventional chemotherapeuticals in 1 patient, and resection and chemotherapy in 1 patient).
In 22 patients, there was not any extrahepatic disease, whereas in 7 patients, there was limited extrahepatic tumor burden. PVT was diagnosed in 12 (41%) patients (main branch in 7 patients, lobar branch in 3 patients, and segmental branch in 2 patients). The AFP level was >400 ng/mL in 13 patients and <400 ng/mL in 15 patients (unknown in 1 patient). Tumor burden was ≤25% in 7 patients, 26%–50% in 14 patients, and 51%–75% in 8 patients. Sixteen patients had multifocal and 13 patients had solitary disease. In 22 patients, the disease was limited in one lobe, whereas in 7 patients, there was bilobar disease.
On the whole body and SPECT-CT fusion images taken after MAA angiography, there was no extrahepatic distribution of microspheres in the visceral organs. Although in 21 patients the hepatopulmonary shunt ratio was ≤10%, in 8 patients the ratio was between 11% and 20%. In these 8 patients, the dose adjustment of Y-90 microspheres was done to prevent excessive lung radiation exposure (>30 Gy).
Twenty-one patients were given radioembolization in the year following the diagnosis of HCC. In 4 patients radioembolization was given in the first year, in 2 patients in the second year, in 1 patient in the third year, and in 1 patient in the tenth year of HCC diagnosis.
Twenty-three patients received Y-90 resin (SIR-Spheres) and 6 patients received Y-90 glass (TheraSphere) microspheres. For resin microsphere treatments, the mean dose was 1.5 GBq (range: 1–2.2 GBq). For glass microsphere treatments, the mean dose was 2.6 GBq (range: 1.6–3 GBq). The treatment route was right hepatic artery in 26 patients and left hepatic artery in 3 patients.
Most of the patients had nausea and abdominal pain after the treatment and some reported fatigue in the initial weeks after the treatment. Transient rise in bilirubin levels occurred in 19 patients. In 12 patients, AFP levels decreased after the treatment.
Treatment response was evaluated with CT/MRI and/or F-18 FDG PET-CT in a range between 6 weeks and 6 months after the treatment. Sixteen patients were evaluated as responders to the treatment. In these patients, reduction in size, increase in amount of necrosis, and reduction in metabolic activity were regarded as treatment response. In 5 patients, there was no remarkable change (stable disease) in the tumors. In 2 patients, there was anatomic and metabolic progression. In 6 patients, the evaluation of treatment response could not be managed. When treatment response was evaluated according to the type of treatment, there were 14 responders, 2 stable disease, 2 progressions, and 5 not evaluated patients in the resin microsphere treatment group (total of 23 patients), whereas there were 2 responders, 3 stable disease, and 1 not evaluated patient in the glass microsphere treatment group (total of 6 patients).
Twenty-two patients died during the follow-up period. Nine of 22 deceased patients had PVT. Time of death was <6 months in 2 patients. In 1 of these patients, the cause of death was hepatic failure. The other patient was lost due to infection.
Seven patients were alive at the end of the follow-up period. Four of these patients had stable disease with 17, 23, 24, and 49 months of survival.
The median overall survival was 17±2.52 months (95% CI: 12.07–21.94) (Fig. 1). Survival varied significantly with the BCLC disease stage. Median survival was significantly better in patients with BCLC stage B than stage C (21±3.47 months; 95% CI, 13.55–28.46 vs. 12±2.21 months; 95% CI, 7.68–16.33; p=0.006) (Fig. 2). Survival was not significantly different in subgroups of patients according to sex, age, prior treatment status, tumor burden, time between HCC diagnosis and radioembolization, PVT (Fig. 3), hepatopulmonary shunt ratio, multifocality, bilaterality, ECOG, and Child-Pugh status. Although a low level of the AFP level before treatment and no extrahepatic tumor burden seemed to affect survival in a positive way, the differences did not reach statistical significance (p=0.055) (Table 1).

Kaplan–Meier survival curve for the whole group of patients. Median overall survival is 17±2.52 months.
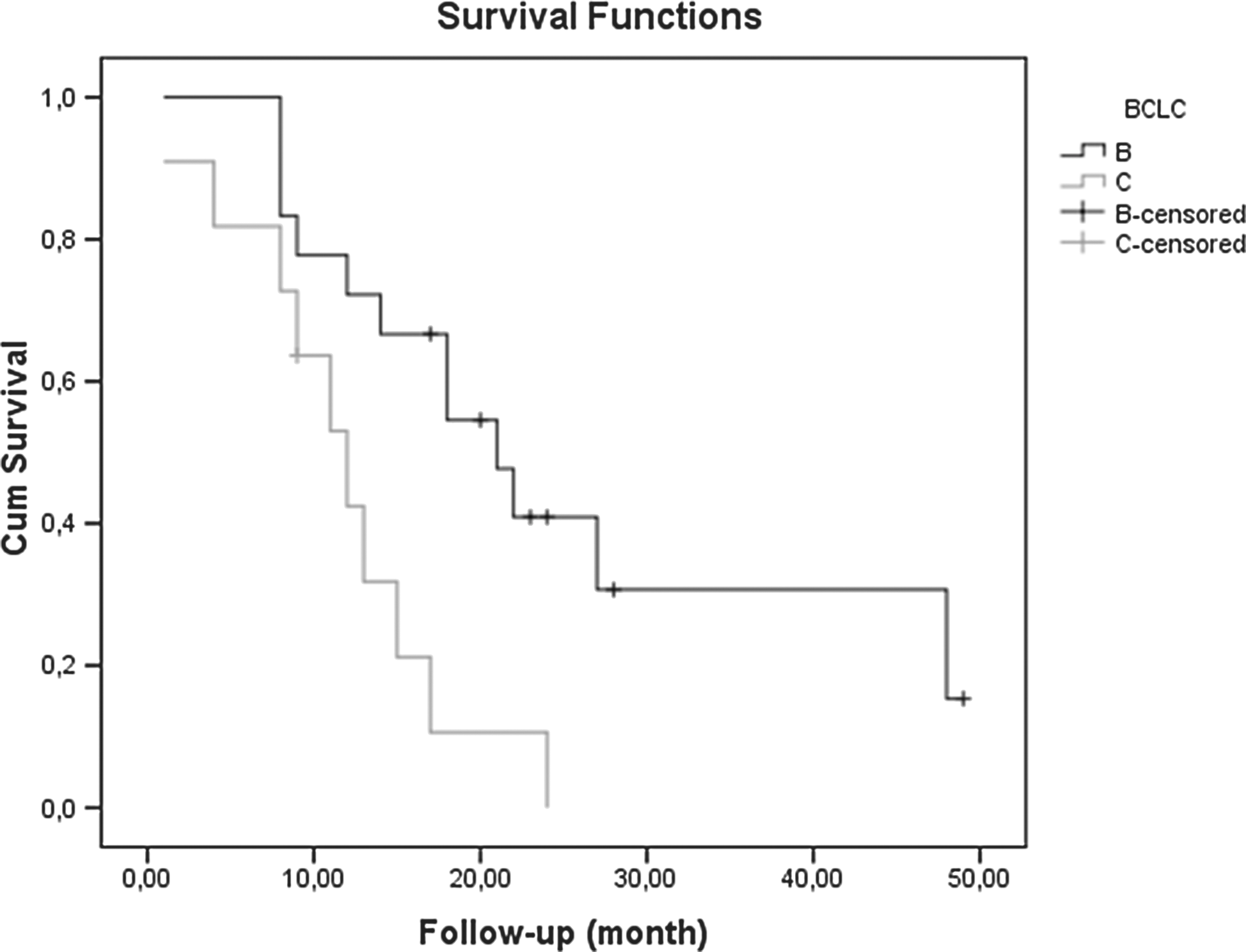
Survival curves for patients with BCLC B (median survival time: 21±3.47 months) versus BCLC C (median survival time: 12±2.21 months), p=0.006. BCLC, Barcelona Clinic Liver Cancer.

Survival curves for patients with and without portal vein thrombosis (PVT), (p=0.506).
Not known in 1 patient.
AFP, alpha fetoprotein; BCLC, Barcelona Clinic Liver Cancer staging classification; ECOG, Eastern Cooperative Oncology Group performance status; NA, not applicable; NE, not estimated; PVT, portal vein thrombosis.
Discussion
Median overall survival was 17 months in this study, in which the endpoint was reached in 76% of the patients. This survival rate is similar with an observational cohort study of 108 patients that of which was 16.4 months. 3 In this study, although there were more patients with PVT (41% vs. 31%), the survival time was comparable with this multicenter study. The overall survival rates of HCC patients who received radioembolization are reported between 7 and 13 months in various other studies. 4 –8 One of these studies is a multicenter analysis of eight European centers of 325 patients in which the overall survival was 12.8 months. 4 In this study, advanced HCC patients consisted ∼57% of the patients, whereas this rate was about 38% in this patient group. This may explain the lower survival time in this multicenter analysis.
In this study, median overall survival was significantly better in patients with BCLC stage B than stage C (27 vs. 9 months; p=0.01). Sangro et al. and Salem et al. also emphasized the significant relationship between BCLC disease stage and survival. 4,9 In advanced HCC patients, diminution of therapy doses due to low hepatic reserves may also affect survival. Survival was not significantly different in terms of age, sex, tumor burden, time between HCC diagnosis and radioembolization, level of AFP level before treatment, extrahepatic tumor burden, ECOG, and Child-Pugh status in this study. In contrast to these findings, there are some investigations which demonstrated that these factors also influenced survival. 4,9 This discrepancy of these data with literature in terms of statistical analysis is probably caused by a small patient number and different patient characteristics. Although the difference between low (<400 ng/mL) and high (>400 ng/mL) levels of AFP before treatment did not reach statistical significance in this study (p=0.055), it is worth mentioning that the longest survivals (48 and 49 months) were determined in patients with low levels of AFP (38 and 2 ng/mL, respectively). As pointed out by Toro et al., the serum AFP level may be used as a tool to predict prognosis in HCC patients. 10
One of the patients with longest survival time (49 months) was a young woman with the Budd–Chiari syndrome as the etiology of HCC who had stable disease since radioembolization. Her initial AFP level was 2 ng/mL and there was no elevation throughout her follow-up. CT follow-up at 4 and 12 months after the treatment showed stable disease and on F-18 FDG PET-CT, taken at 6 weeks after the treatment, there was faint F-18 FDG uptake in the tumor, showing a low level of metabolic activity. The other patient was an older man who had limited treatment options due to large tumor size and PVT. Although he had hepatic progression after 11 months from radioembolization, his overall survival was 48 months (Fig. 4). Transplantation, local therapies, and sorafenib could not be additional treatment options for this patient due to PVT and liver malfunction. In the practice guideline of American Association for the Study of Liver Diseases (AASLD), sorafenib is the choice of treatment in advanced patients like this patient, 11 but the survival rates are limited in clinical studies. In a phase II study of 137 patients, which assessed efficacy of sorafenib in advanced HCC patients, overall survival was 9.2 months. 12 In the large phase III study (SHARP), which was conducted on the basis of these data, overall median survival was found to be significantly longer in the group that received sorafenib than the group that received placebo (10.7 vs. 7.9 months). 13 This study and other studies, which deal with radioembolization, demonstrate a comparable or even more favorable survival time than sorafenib. 3 –8 Although drawing definite conclusions is not possible at the present time, several prospective randomized on-going trials, which compare effectiveness of these two modalities, may determine a conclusion in the near future.

Magnetic resonance imaging (MRI) follow-up of the patient with 48 months of survival after yttrium-90 (Y-90) microsphere treatment. At the time of diagnosis, he was 47 years old. He had main branch PVT and Child-Pugh B disease. His BCLC grade was B and he had ECOG 2 disease. On his MRI before treatment, there was a tumor on the right hepatic lobe, 44×30 mm in diameter, consistent with a hepatocellular carcinoma lesion (images not shown). His AFP level was 37 ng/mL. MRI taken at 2 months
According to clinical experience, eventhough the patients with PVT do not have many treatment options, they have favorable survival with radioembolization. There were 12 (41%) patients who had different levels of PVT in this study and 9 of these patients deceased during follow-up. The median survival was 17±2.36 months (95% CI: 12.37–21.63) for the group of patients with PVT, which did not lead to a significant difference in survival analysis by the log-rank test (p=0.506). In the literature, there are some articles that reported diminished survival as the result of PVT. 4,9,14 Hilgard et al. reported a survival of 10 months in the PVT group, whereas this value was 16.4 months in the no PVT group (p=0.96) and stated that radioembolization with Y-90 microspheres had a role in locoregional therapy of advanced HCC patients with or without PVT. 3 Tsai et al. reported a median of 2.7 months of longer survival in patients with PVT treated with Y-90 microspheres. 7 Inarrairaegui et al. stated that Y-90 resin microspheres may provide some clinical benefit with decreased risk of complication in patients with PVT. 6 In this sense, radioembolization can be a therapeutical option in HCC patients with PVT. In this study, 12 patients out of 29 had PVT and 2 of these patients were Child B during referral to radioembolization. Both of these patients had favorable survival times of 21 and 48 months. Also from these 12 patients, 3 patients were still alive with survival times of 17, 24, and 49 months. All 3 patients received resin microspheres with doses 1.8, 1.2, and 1.7 GBq, respectively. Tumor loads were between 26% and 50% in the first and third patients and they had main branch PVT. The second patient had tumor load of 51%–75% and lobar branch PVT. AFP levels of all these patients were below 10 ng/mL at the initial diagnosis and showed no significant rise during follow-up. Favorable prognosis in these patients may be due to more indolent nature of their tumors, according to their low AFP levels. Another explanation may be the presence of benign PVT, instead of tumoral PVT, during diagnosis and throughout their follow-up.
The selection of patients for radioembolization must be achieved with great care, otherwise toxicities and complications, which would risk the life of a patient, can be seen more often. Radioembolization-induced liver disease (REILD), as first described by Sangro et al., is a syndrome that appears 4–8 weeks after radioembolization as jaundice, mild ascites, and moderate increase in GGT and ALP. 15 REILD is more likely seen in patients who have cirrhosis or who underwent prior or subsequent chemotherapy. 16 The reported incidence is 5.4%. 16 Similarly, in this patient group, 1 patient out of 29 (3.4%) had hepatic failure at 4 months after radioembolization. This patient who had infiltrative tumor in the left hepatic lobe had BCLC stage C disease. Due to left PVT, he could not be treated with TACE. At 6 weeks after radioembolization, the bilirubin levels started to increase and then the patient was lost due to hepatic failure. Because he had fairly low but normal limits of liver functions before radioembolization and had progressive hepatic failure after therapy, it was thought that the hepatic failure was caused by REILD. In another group of patients who were treated with radioembolization due to metastatic liver disease in this department, the rate of REILD was 3.3% (2 patients out of 61), which is very similar that of the HCC group. 17
This study has several limitations. First of all, the retrospective nature of this study was challenging during gathering of data. Treatment response assessments could not be made uniformly in terms of time and method. Therefore, the authors could not evaluate progression-free survival rates. Also, the small number of patients, which probably caused nonsignificant results at statistical evaluation, did not allow us to make comparisons between subgroups. Also, uneven distribution of patients, in terms of type of treatment used (resin vs. glass microspheres) made us also not to compare the outcomes of these subgroups. Despite these limitations, this study, in which endpoint was reached in 76% of the patients, demonstrates that radioembolization with Y-90 microspheres is an efficient treatment modality in advanced HCC patients, which provides a significant survival even in patients who have limited choices for treatment due to PVT.
Conclusions
Radioembolization provides a favorable survival time in advanced HCC patients. BCLC disease stage is a significant predictor of survival. Patients with PVT who are not eligible for TACE can have radioembolization with no decrease in survival time. Clinical studies with large patient numbers are necessary to be able to define the best treatment option in different patient groups.
Footnotes
Disclosure Statement
No competing financial interests exist.