
Abstract
Purpose:
To evaluate any potential value of 2-deoxy-2-[18F] fluoro-
Materials and Methods:
The authors retrospectively reviewed data of the 47 patients with Pancoast tumors who underwent initial staging by conventional imaging methods and FDG PET/CT. FDG-PET images were visually and quantitatively evaluated, and metabolic tumor volume (MTV), total lesion glycolysis, and maximum standardized uptake values of primary tumors were calculated. The correlations between quantitative PET parameters and tumor stages, as well as overall survival, were analyzed.
Results:
By detecting unknown distant metastasis, PET/CT upstaged 21% of patients. The sensitivity and specificity for detection of lymphatic involvement were 100% and 83.75%, respectively. Having surgery (p = 0.01) and being at an early stage (p = 0.004) were the most predictive factors for overall survival. Although there was no significant correlation between quantitative PET parameters and overall survival, MTV was the most powerful discriminator for operability and preoperative staging (p < 0.05).
Conclusions:
FDG-PET imaging was found to be a valuable method for an accurate staging in the management of patients with Pancoast tumor. Having surgery and being at an early stage at presentation were found to be significant predictors for survival. Quantitative metabolic parameters may contribute to clarification of operable patient subgroups having an early disease stage with low MTV.
Introduction
Pancoast carcinoma (superior sulcus carcinoma) is a rarely seen tumor that locates in the apex of lungs. These tumors directly invade the adjacent tissues (chest wall and structures of thoracic inlet) and can cause specific symptoms such as pain, weakness, atrophy of shoulder and arm, upper arm edema, and Claude Bernard-Horner syndrome. 1 Most of the superior sulcus tumors are nonsmall cell lung cancers. Small cell lung cancers are responsible for less than 5% of the cases. 2,3 Lymphatic involvement plays an important role in therapy planning. Generally, one third of patients have distant metastasis at the time of diagnosis and the brain is the most frequent metastatic area. 4,5 Multimodality treatment regimens are the current concept for Pancoast tumors. 6
Accurate staging is mandatory for the optimal therapy decision and to avoid unnecessary treatment side-effects. The 2-Deoxy-2-[18F] fluoro-
Materials and Methods
The records of patients diagnosed with Pancoast carcinoma at this institution between 2008 and 2013 were reviewed retrospectively. Clinical and laboratory data and radiological findings of patients were documented. Clinical symptoms (arm pain, back pain, others), physical examination findings (Horner syndrome, hand edema, ulnar hand, others), and performance status of patients according to the ECOG performance scale were analyzed. 12 Patients were staged according to the new seventh edition of the TNM lung cancer staging system. 13 All available surgical and pathological results and clinical notes were taken into consideration. CT, magnetic resonance (MR) imaging, and PET/CT examinations were reassessed by two radiologists and two nuclear medicine specialists. Informed consent was deemed as this is a retrospective study using existing hospital records, documents, and data, which belong to patients referred by this institution's chest surgery or chest diseases departments to FDG PET/CT for primary staging due to lung masses. The study was approved by the Ethics Committee of Keciören Training and Research Hospital and the Institutional Review Board Committee.
The authors identified 47 newly diagnosed patients and categorized them according to stage, operation status, and histological subtypes. Fourteen (14) patients were treated surgically with or without neoadjuvant therapy. Thirty-three inoperable patients were treated by radiotherapy, chemotheraphy, chemoradiotherapy, or palliative therapy. Survival after PET/CT was determined as the time between the scan and death or last consultation. The PET/CT images were visually and quantitatively evaluated, and MTV, TLG, and SUVmax of primary tumors were calculated. The correlations between quantitative PET parameters and tumor stages, as well as overall survival, were analyzed.
FDG PET/CT imaging
PET/CT evaluation was carried out with an integrated PET/CT scanner, Siemens, Biograph 6 HI-REZ (Siemens Medical Solutions, Knoxville, TN). All patients were instructed to fast for at least 6 hours before the examination. After confirmation of an acceptable peripheral blood glucose level (<180 mg/dL), patients were given an intravenous injection of 370–555 MBq (10–15 mCi) FDG and rested for 60 minutes before the scanning. Oral contrast material was used in all patients for better visualization of the gastrointestinal lumens. PET data were acquired from the top of skull to proximal femur with the arms up position at six to eight fields of view (3 minutes/field). The CARE Dose (Siemens Medical Solutions) CT scan was performed with automatic, real-time dose modulation amperage. The CT scan was used for attenuation correction of PET data, and images were reconstructed using a standard iterative algorithm.
Quantitative PET/CT parameters
SUVmax corrected for body weight were computed by standard methods from the activity at the most intense voxel in the three-dimensional tumor region from the transaxial whole body images on attenuation-corrected PET/CT images. MTV (cm3) was measured with semiautomatic PET analysis software using an automatic isocontour threshold method, which is based on a theory of being greater than SUVmax of 2.5 within the tumor. 14 The TLG values were calculated by multiplying the MTV and SUVmean values.
Statistical analyses
Descriptive statistics was introduced as frequency, percentage, mean, standard deviation, median, minimum, and maximum values. The Shapiro–Wilk test was used for the normalcy test as sampling numbers in the groups were lower than 50. The Mann–Whitney U test or Student's t-test was applied for the analysis of difference between the measured values of two groups according to their distribution type in each case. Sensitivity (Sn), specificity (Spc), positive predictive value (PPV), and negative predictive value (NPV) for nodal staging on a per node basis were calculated. Receiver operating characteristic (ROC) analysis was performed to distinguish patient subgroups in three different groups of characteristics (histological subtypes, stage, and operation status), according to particular measurements and to specify a useful cutoff point. The cutoff value was defined as the point of the highest combination of sensitivity and specificity in the ROC analysis. The log-rank test was used to reveal differences in survival of each patient group. For all indicators, area under curve (AUC), cutoff points, Sn, Spc, PPV, and NPV are presented. p-Values lesser than 0.05 are accepted as statistically meaningful. All analyses were done by SPSS 20.0 software package.
Results
The authors retrospectively evaluated data from 47 patients (1 female and 46 male; mean age: 59.5 years; age range: 39–81 years) with Pancoast tumors. Of the 47 patients, 6 had tuberculosis and 38 had a smoking history (mean 50 package/year). The most common complaint was back pain (70.2%) followed by arm pain (61.7%). Besides that, 6 of 47 patients had the Horner syndrome initially. Histopathological diagnosis was made by a transthoracic fine needle aspiration biopsy (FNB) in 41 patients. Surgery and mediastinoscopy were used on the remaining 6 patients for a definitive diagnosis. The ECOG score was between 0 and 1 in 85% of the patients. The histological subtypes noted were small cell lung cancer in 2, adenocarcinoma in 17, nonsmall cell lung cancer (NSCLC) in 12, squamous cell cancer in 14, and large cell cancer in 2 patients, respectively. The primary tumor location was the right apex in 28 (59.6%) patients, while the remaining 19 (40.4%) patients had Pancoast tumor in the left apex (Table 1).
Edema, weakness, atrophy of shoulder and arm; eye asymmetry.
FNB, fine needle aspiration biopsy.
TNM staging
Of the 47 patients, 31 had T3 tumor and 16 had T4 tumor. All the 14 patients treated with surgery had T3 tumor. When the pathological T stages of the operated patients were compared with PET/CT results, PET/CT ensured the correct T staging in 11 cases (78.6%) by accurate assessment of rib and chest wall invasion (Fig. 1). PET/CT results were not discriminative for T3 tumors in 3 patients. In contrast, 9 of 16 patients (56.2%) were staged as T4 tumor because of adjacent vertebral invasion, concordant with PET/CT findings, and the remaining 7 patients were staged only with MR because of the determination of brachial plexus involvement (Fig. 2). A total of 82 lymph nodes were histopathologically evaluated by either cytology following mediastinoscopy or surgery. The sensitivity and specificity of PET/CT for the detection of lymph node metastasis were 100% and 83.75%, respectively. The PPV and NPV were calculated as 13.3% and 100%, respectively (Table 2). Thirteen (13) (27.6%) patients had distant metastasis. The PET/CT revealed 13 distant metastatic sites in 10 patients. The adrenal glands (four), followed by the lungs (three) and bone (two), were the most prominent metastatic sites, whereas the brain, liver, spleen, and parotid gland had solitary metastasis on pretreatment FDG PET/CT. The FDG PET/CT scan upstaged 10 patients (21.3%) by detecting distant metastasis. Brain metastases could not be detected in 3 patients because of high physiologic background FDG activity in normal brain parenchyma.
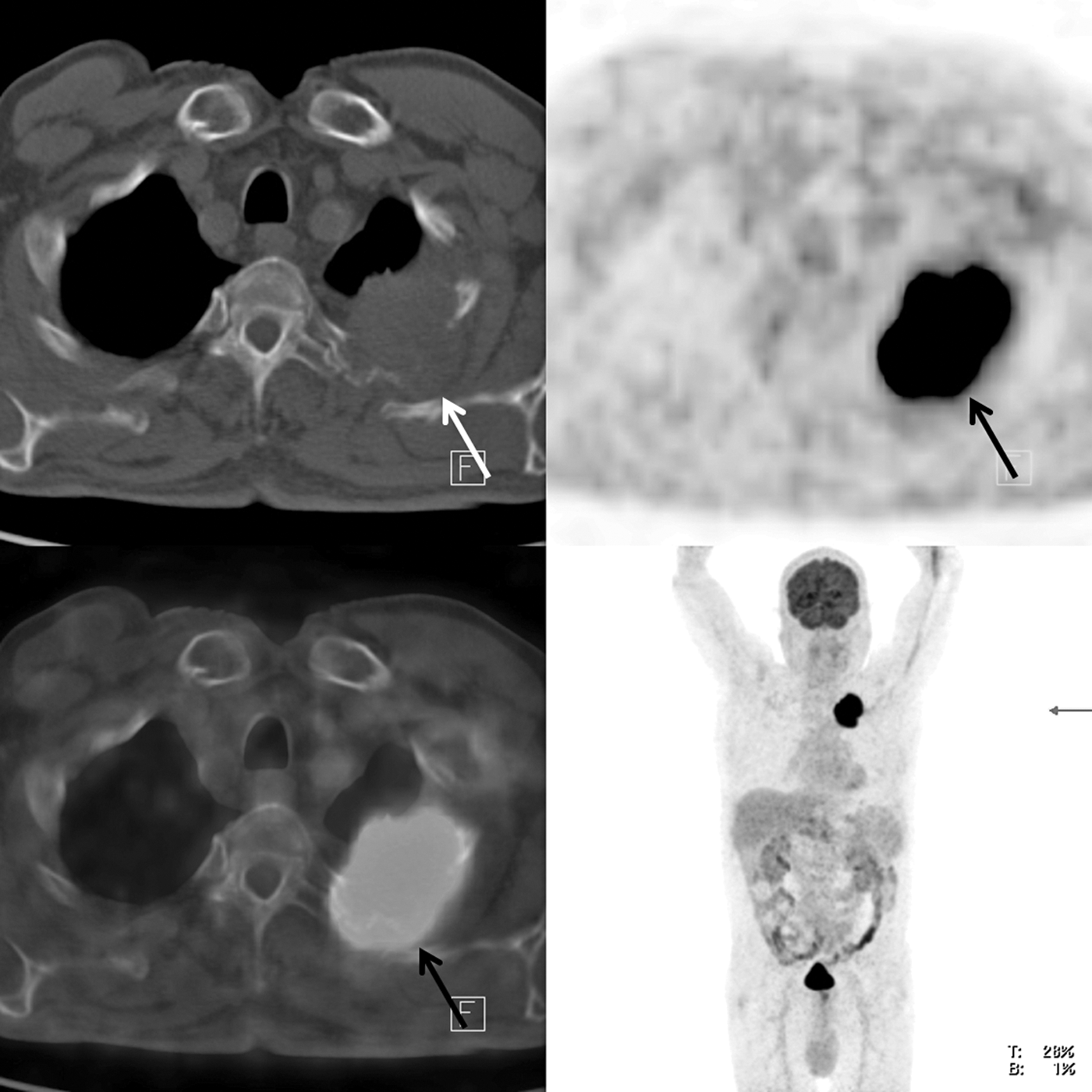
The tumor, which is located on the apex of the left lung with a high fluoro-deoxyglucose (FDG) accumulation (maximum standardized uptake value: 30.8), is extending to the chest wall and invading the second rib. Tumor boundaries and its extension to the adjacent chest wall can be distinguished easily with positron emission tomography (dark arrow) unlike the clearly indistinguishable one on computed tomography images (white arrow).
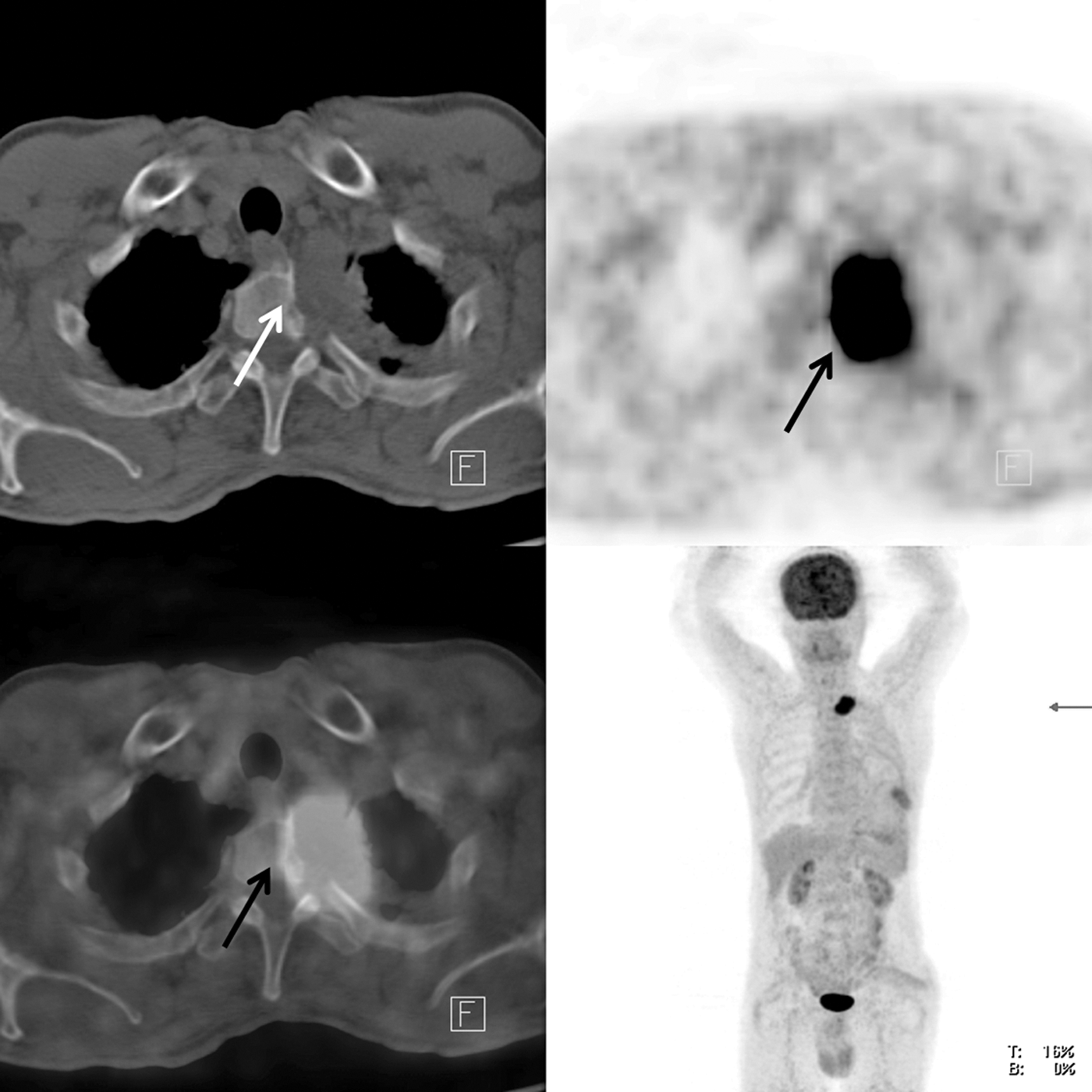
There is a tumor with a high FDG accumulation (dark arrow) on the left pulmonary apex causing vertebral destruction (white arrow) and extending into the left neural foramen. This lesion determined as adenocarcinoma with fine needle aspiration biopsy was staged as a T4 tumor.
TP, true positive; FP, false positive; TN, true negative; FN, false negative; Sn, sensitivity; Spc, specificity; PPV, positive predictive value; NPV, negative predictive value; PET/CT, positron emission tomography/computerized tomography.
Quantitative PET/CT parameters
The mean tumor diameter was 6.2 ± 1.7 cm. Mean quantitative values for SUVmax, MTV, and TLG were 17 ± 8.4, 131.7 ± 98, and 964.7 ± 952.9, respectively. Volumetric parameters were not statistically different between adenocarcinomas and other histological subtypes (squamous cell, large cell, and NSCLC) (Table 3). A prominent difference was found between tumor MTV (p = 0.018) and TLG (p = 0.031) values of primary tumor in patients with stage IIB+IIIA and stage IIIB+IV (Table 4). No difference was observed between SUVmax, TLG values, and tumor size of operated and nonoperated groups. However, MTV values (p = 0.048) of nonoperated patients are found significantly higher (Table 5). An ROC analysis is performed for prediction of stage by meaningful variables after a univariate analysis. The best cutoff value for MTV was found as 140 cm3 (AUC: 0.704 [p = 0.0097], Sn: 60%, Spc: 81.5%) (Fig. 3). Conversely, the cutoff value for TLG was found to be 733.6 (AUC: 0.685 [p = 0.021], Sn: 65%, Spc: 70.4%) (Fig. 4). An ROC analysis is also performed to predict operability by meaningful variables after univariate analysis. The best cutoff value to predict operability for patients with Pancoast tumor was found to be MTV of 86 cm3 (AUC: 0.684 [p = 0.0228], Sn: 71.4%, Spc: 69.7%) (Fig. 5).
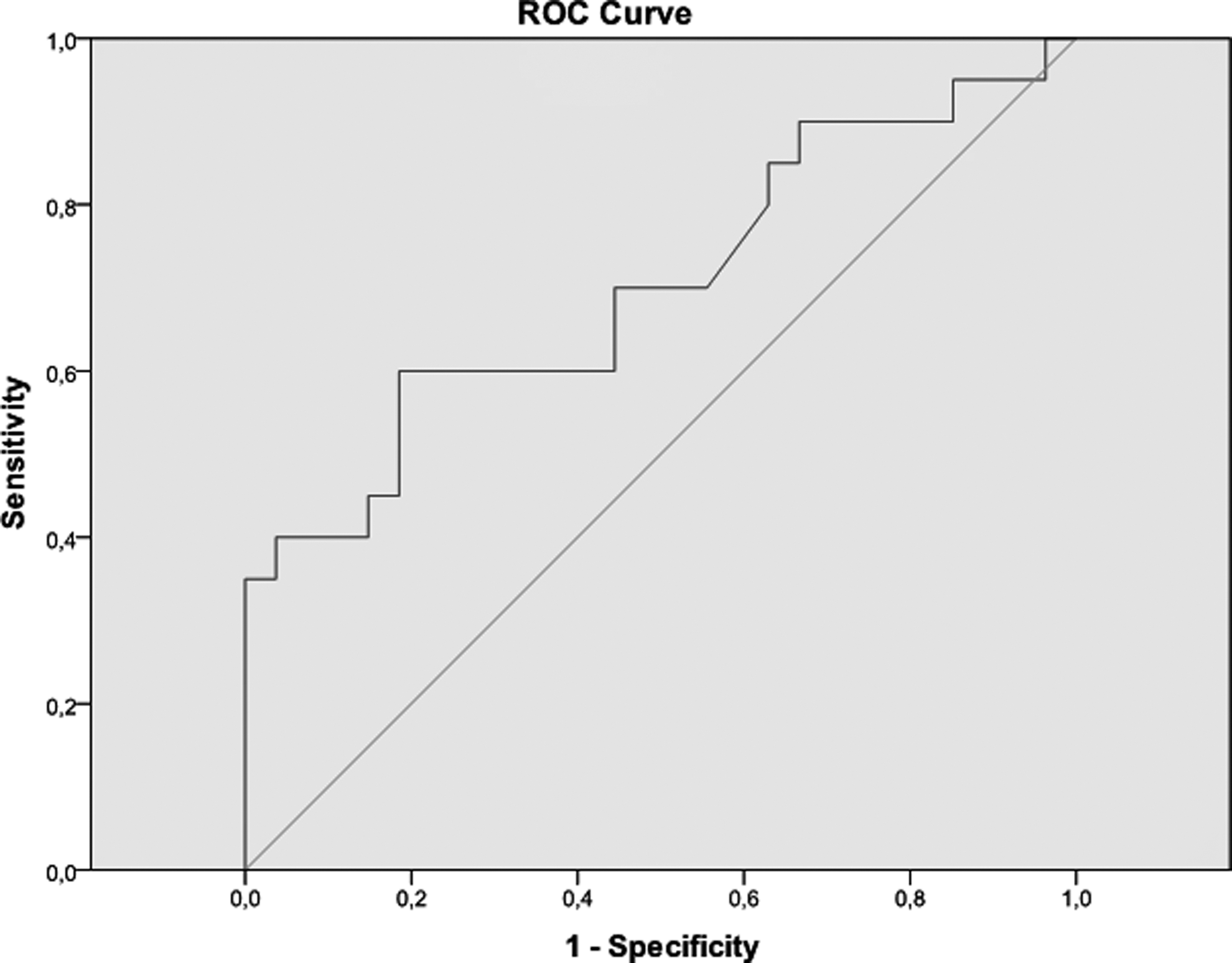
The receiver operating characteristic (ROC) of metabolic tumor volume (MTV) in relation to stage (area under curve [AUC]: 0.704, [p = 0.0097], sensitivity [Sn] 60%, specificity [Spc] 81.5%).
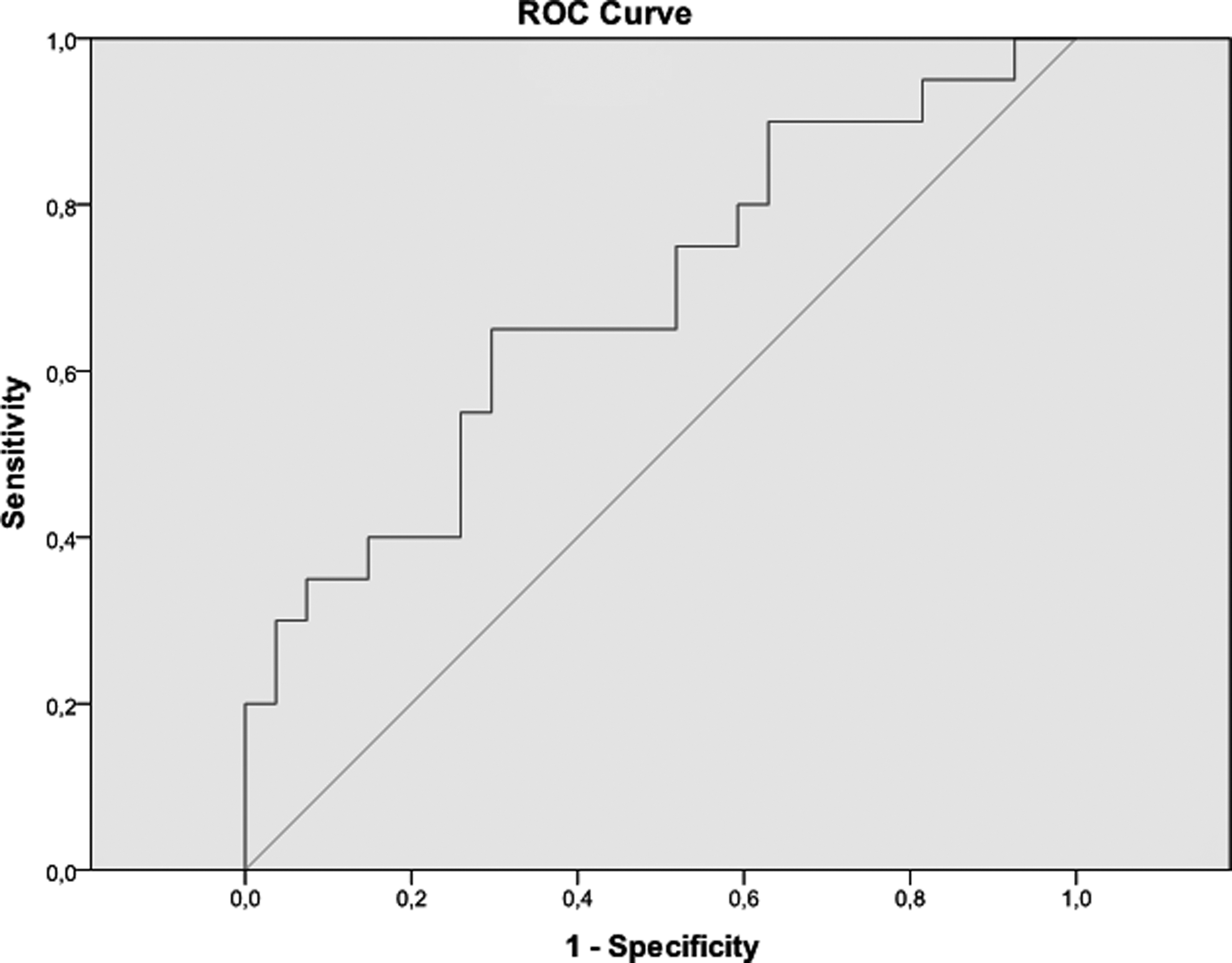
The ROC of total lesion glycolysis in relation to stage (AUC: 0.685, [p = 0.021], Sn 65%, Spc 70.4%).
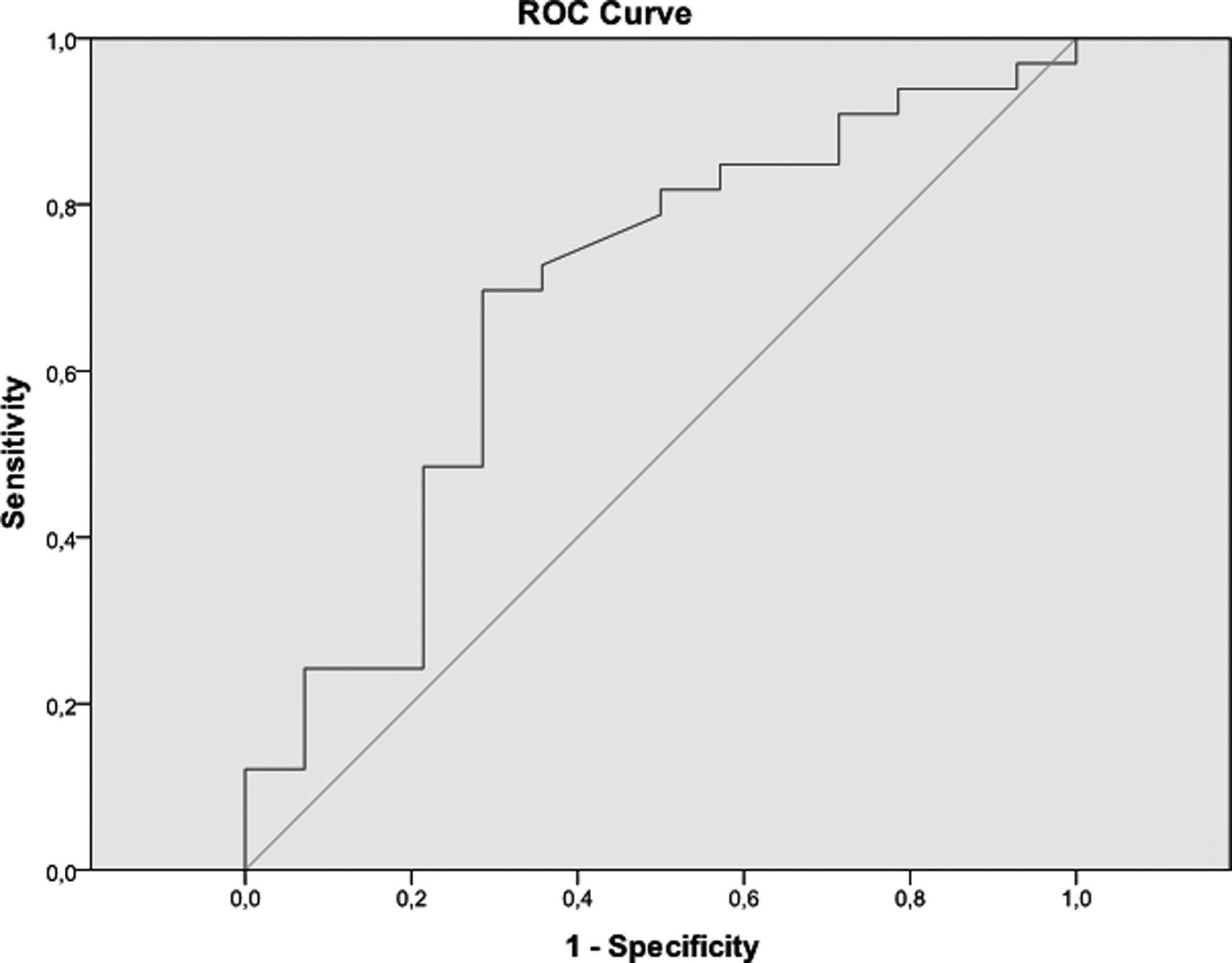
The ROC of MTV in relation to operation (AUC: 0.684, [p = 0.0228], Sn 71.4%, Spc 69.7%).
Student's t-test.
Mann–Whitney U test.
Log-rank test.
CI, confidence interval; MTV, metabolic tumor volume; SUV, standardized uptake value; TLG, total lesion glycolysis.
Mann–Whitney U test.
Student's t–test.
Statistically significant.
Log-rank test.
Student's t-test.
Mann–Whitney U test.
Statistically significant.
Log-rank test.
Survival
At the end of the study, 26 of 47 patients were dead. The average survival time was 13.9 ± 12.6 months. The mean follow-up time was 31.9 ± 16.8 months for the remaining 21 patients. The relationship between overall survival and TNM staging in patients with Pancoast tumor was evaluated. While patients with T3 tumors are expected to have a better survival than those with T4 tumors (p = 0.053, p-value is at the edge of a point, statistically insignificant but clinically significant), existence of distant metastasis dramatically shortens the overall survival (p = 0.025) (Figs. 6 and 7). Alternatively, no relationship between the lymph node involvement and overall survival (p = 0.139) could be found.
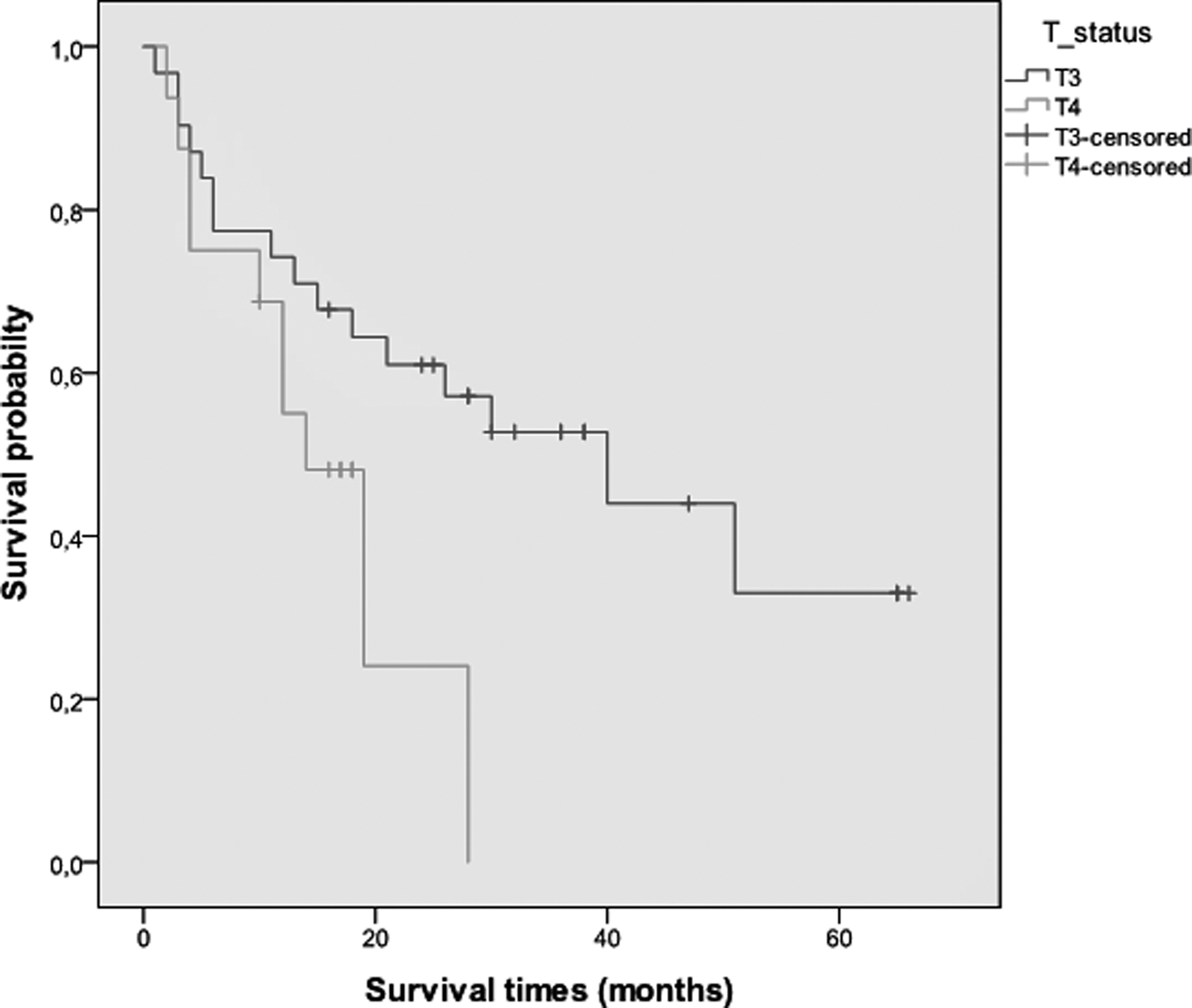
Kaplan–Meier survival curves according to T status (p = 0.053, log-rank test).
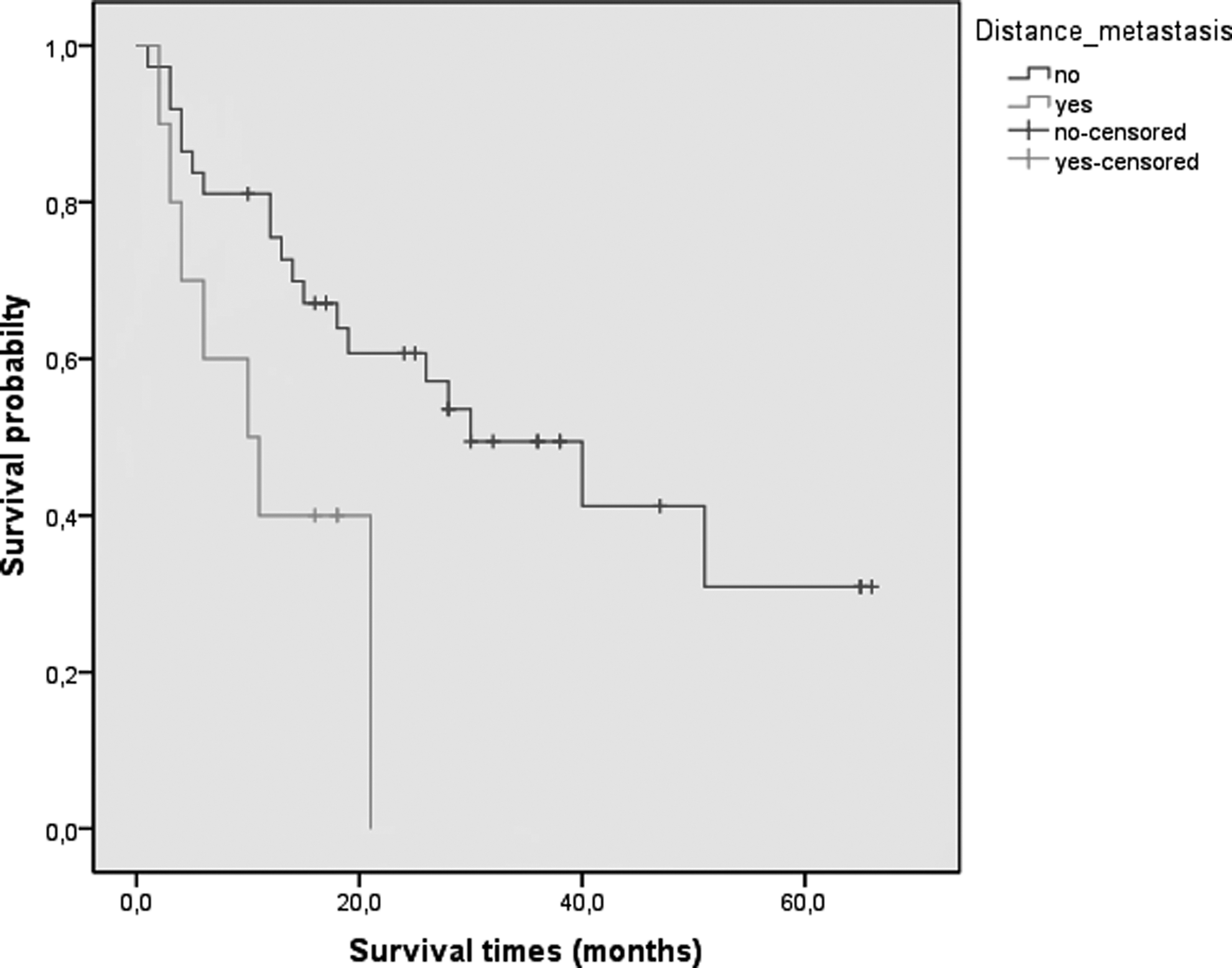
Kaplan–Meier survival curves according to distant metastasis (p = 0.025, log-rank test).
The relationship between overall survival and quantitative PET/CT parameters was also investigated. There is no difference between tumor size (p = 0.202), SUVmax (p = 0.923), MTV (p = 0.872), and TLG (p = 0.999) values in terms of survival status. Unfortunately, cutoff values used for the predicting stage (p = 0.237 for cutoff 140 cm3, p = 0.488 for cutoff 733.6) and operability (p = 0.521 for cut off 86 cm3) do not also help for prediction of survival. Stage (p = 0.004) and operation status (p = 0.01) were noticed as significant variables for survival, but not histological subtype (p = 0.753). Survival was not statistically different between patients with adenocarcinoma and those with other histological subtypes (squamous cell, large cell, and NSCLC) (median survival: 28 months vs. 40 months). The patients who underwent surgery had a significantly longer survival period than the nonoperated group (median survival: 60 months vs. 18 months). Similarly, survival was longer in the early-stage group (IIB+IIIA, median survival: 40 months) than the advanced-stage group (IIIB+IV, median survival: 10 months). Tumor size, SUVmax, MTV and TLG values, median survival, histological subtypes, stage, operation status, and pairwise comparisons are summarized in Tables 3 –5.
Discussion
PET/CT is accepted as the most effective imaging modality for management of oncological patients, especially those having lung cancer. However, there is no specific study on the evaluation of Pancoast tumors with PET/CT; whereas, due to its nonspecific symptoms and localization, the diagnosis and treatment of these tumors are more challenging and time consuming. The majority of patients who applied to the hospital came with arm and back pain complaints that are not specific to lung cancer. Due to the unique localization of the primary tumors, it is almost impossible to establish the diagnosis by bronchoscopy. Hence, most of the patients in the patient population were diagnosed with FNB. When the possible biopsy complications are taken into account, biopsy decision gains importance. In contrast, sequelae changes in pulmonary apex on X-ray and CT make it difficult to differentiate benign lesions from probable malign pathologies in a country like Turkey, where tuberculosis continues to be a prevalent health problem. Previous studies have shown low SUVmax (ranging from 1.8 to 4.3) in chronic active infection or the healing process of tuberculosis. 15 Contrary to this finding, SUVmax of Pancoast tumor in this study patient group were quite high (mean: 17 ± 8.4), which is a favorable finding for PET/CT in distinguishing apical lung lesions from sequelae changes leading to biopsy decision for the clinician.
Pancoast tumors are locally advanced cancers and confront us as T3 or T4 tumors. While T3 tumors invade the chest wall and/or sympathetic chain, T4 tumors infiltrate brachial plexus, vertebral bodies, trachea, esophagus, and vascular structures. In studies comparing the methods for T staging, similar results have been acquired in CT and PET/CT. 16 The most important contributions of FDG PET/CT in T staging are the detection of malignant pleural effusion, depicting chest wall invasion and discrimination between tumor and atelectasis. 17 In this study, PET/CT was able to determine rib invasion and, hence, made accurate T3 staging in 78.6% of the patients treated with surgery. Although there are different reports about the achievement of MR for the evaluation of chest wall invasion, it seems that MR appears to be a superior technique for assessing local extension in pulmonary regions of lesser moves where Pancoast tumors originate. 18 Of the 47 patients in this study group, PET/CT was eligible for T4 tumor distinction by showing only vertebral involvement in 56.2% of patients, whereas MR outshone it by revealing not only vertebral involvement but also invasion of brachial plexus, subclavian artery, and the vein. When the correlation between T stages and overall survival is observed, a meaningful difference is observed between T3 and T4 tumors. In the study of Rusch et al., there is also a difference between T3 and T4 superior sulcus tumors with regard to pathologic complete resection (R0) achievement (64% of T3N0 and 39% of T4N0 tumors) and survival. It is obvious that a greater tumor size means greater possibility of residual tumor after surgery, ending with diminished overall survival. 19,20
CT and MR cannot precisely describe the presence or absence of nodal metastasis. FDG PET/CT seems to be a better method in nodal involvement. In previous studies, the pooled sensitivity and specificity of PET/CT for nodal staging of nonsmall cell lung cancer in the mediastinal lymph node station based data analysis was 68% and 95%, respectively. 21 In this study, sensitivity and specificity of PET/CT for detecting lymphatic metastasis are 100% and 83.75%, respectively, in the invasive surgical staging subgroup (n = 14). Most probably, the location of primary lesion away from the mediastinal lymph nodes and also their high FDG affinity enhances the discrimination of lymphatic uptakes in this study. However, the authors could not find any correlation between survival and nodal involvement. In our series not all patients had surgery, and this is one of the main drawbacks decreasing the power of the statistical results of the study. One of the main reasons for a low PPV in this patient group may be accompanying inflammatory diseases, such as tuberculosis and anthracosis, caused by widespread use of coal for heating.
The most important contribution of FDG PET/CT for staging is its ability to show unexpected distant metastases. In 13 (27.6%) patients, remote metastases were discerned at the time of diagnosis. Three patients had more than one metastatic focus and 10 had solitary metastatic focus. The brain is the most frequent metastatic area of Pancoast tumors in declared series, and the sensitivity of PET for detecting brain metastases was reported as low as around 60%. 4,5,22 Similar to the literature, brain metastases in 3 patients did not take up FDG in this group. Although anatomical changes (shift, edema, etc.) can be discriminated on the CT component of PET/CT scanner and diagnostic accuracy can be increased by meticulous examination of CT images and administration of IV contrast media, MR still emerges as the best method in the evaluation of brain metastases. Alternatively, superiority of FDG PET/CT over the other conventional methods in the evaluation of surrenal lesions was proven as in the case of this study. 23 To sum up, FDG PET/CT made a great contribution and staging changed in a substantial patient group in M staging.
When evaluations on quantitative parameters are considered, there was no marked difference between the tumor size, SUVmax, MTV, and TLG values of both the surviving and dead patients. In many studies regarding lung cancer, it has been reported that SUVmax may provide additional prognostic information in staging and a correlation between tumor aggressiveness and cutoff values, changing between 2 and 15, was clarified. 24,25 The mean SUVmax of the patients are calculated as 17 ± 8.4 and a great majority of them are over the cutoff levels declared in previous studies. It is thought that the reason for the high SUVmax of the patients is both cellular aggressiveness of tumors and delayed diagnosis in a more advanced stage according to other cancers. Patients in this study group had unfavorable prognosis, 55% of the patients died during a period of mean 22 months follow-up.
Although MTV was reported as a good prognostic indicator in many studies, the authors could find any correlation between survival and metabolic parameters such as MTV and TLG. Operability and R0 resection in Pancoast tumors are the main factors for long-term survival expectation. 26,27 Concordant with the literature, stage and operability were the main survival markers in this study group. The eligibility for surgery is much more related to invasion degree than the tumor size in patients with Pancoast tumors as opposed to the other lung cancers. Therefore, local invasion (more than 50% of vertebral body, trachea, esophagus, and brachial plexus) evaluated by anatomical imaging modalities such as CT and MR is the most important factor in determining operation decision. Despite development of imaging modalities, it may not always be possible to assess resectability exactly and it must be correlated with clinical symptoms. The evaluation of tumor extension accurately influences operation decision. By the quantitative PET indices, the authors found that tumor volume represents a significant difference between operable and inoperable patient groups in this study. Having a tumor volume more than 86 cm3 significantly diminishes operation chances. To identify the exact localization and extension of Pancoast tumors, because of it having complex surrounding anatomical components, requires critical consideration. The FDG PET/CT is an auxiliary method for showing extension and tumor border, and thus, it can affect the surgical procedure to be applied. As Bruzzi et al. previously introduced three-dimensional volumetric evaluations, which distinguish tumor borders more easily, a more correct T staging could help in deciding resectability and operation, 28 through which R0 resection rates would be increased.
The patients in this study group have statistically different MTVs with the correlation of disease stages. This difference is more prominent between the patients with disease stage IIB and stage IV. Having a higher pretreatment tumor volume increases the probability of distant metastasis. TNM staging system is currently the main method for estimating prognosis, and prognostic variation between stages is a well-known issue for all lung cancer types. Although sometimes prognosis and overall survival may differ in patients even if they are at the same stage, probably because of personal traits (ECOG) and the number of metastatic lesions. Therefore, determining tumor burden is crucial for the development of personalized treatment plans and avoidance of unnecessary treatment complications because of the aggressive multimodality therapies needed for Pancoast tumors. 29 Besides that, tumor volumes may help in deciding the best treatment option and aid the planning of radiotherapy, especially by outlining tumor boundaries. A strong correlation between prognosis and volume-based metabolic parameters has been shown in many previous studies. 30 –32 Conversely, while Hyun et al. did not find a significant correlation between MTV and prognosis in inoperable NSCLC patients with stage III disease, they showed a significant correlation in patients with the same disease stage, but eligible for surgery. Moreover, stage IV disease itself is seen as a poor prognostic factor. In this study, although MTV and TLG are not independent prognostic indicators for survey analysis, they are acting as cofactors in the determination of risk for advanced disease and decision of operability. The reason of not having a statistically significant correlation between MTV and prognosis in this patient group may be the failure in composing a homogeneous patient population and the number of patients having advanced disease stage with distant metastases. Because of the small number of patients in the study group, the stages could not be assessed separately by themselves. Although the redundancy of tumor burden reduces survival expectation, sometimes tumor location rather than volume could be more critical and should also need special consideration, as it happens in brain metastases.
This study has several limitations due to its retrospective design. Not having a standard treatment protocol for all patients, the limited number of study group, the absence of comparison of patients in the same stage are some of these limitations. A variety of histological subtypes in this study group and paucity of sampling for comparison in these subtypes were other restrictions. To achieve a more powerful conclusion about the prognostic value of the volume-based PET parameters, it might be reasonable to increase the sample number of the same TNM stage and subtypes with new studies. Besides that, although volume measurements were made to accept SUVmax 2.5 as a cutoff value in this study, it should be considered that standardization of the method preferred for volume calculations is still a controversial issue.
Conclusions
Although there was no correlation between overall survival and volume-based PET parameters, MTV might support the decision for surgery despite the fact that TNM staging seems to be the most significant method for the prediction of survival. Quantitative PET indices may help the management of patients with Pancoast tumors and guide patient-oriented therapies in the future.
Footnotes
Acknowledgment
The abstract of the manuscript was presented at the 27th Annual Congress of the TSNM (Turkish Society of Nuclear Medicine) in April 2015.
Disclosure Statement
No competing financial interests exist.