
Abstract
Objective:
To establish the optimal safe dose of everolimus in combination with 177Lu-octreotate peptide receptor radionuclide therapy (PRRT) of advanced progressive gastro-entero pancreatic neuroendocrine tumors (GEP-NETs) and to define dose-limiting toxicity.
Patients and Methods:
Patients with advanced unresectable progressive well-differentiated GEP-NETS avid for 68Ga-octreotate on positron emission tomography–computed tomography imaging underwent PRRT with four cycles of 7.8 GBq 177Lu-octreotate at 8 week intervals. Successive cohorts of 3 patients received escalating doses of everolimus comprising 5, 7.5, and 10 mg daily for 24 weeks.
Results:
Sixteen patients comprised 4 at 5 mg, 9 at 7.5 mg, and 3 at 10 mg everolimus. Patient cohorts at 5 and 7.5 mg received 83% and 80% of the total planned dose of everolimus over 24 weeks. All patients required dose reduction or complete cessation of everolimus at the 10 mg level, which induced neutropenia and thrombocytopenia, and reduced creatinine clearance. The overall response rate was 44% (7 of 16 patients), and no patient progressed over the 6 month period of treatment. Four of 5 pancreatic NET patients achieved PR 80%. No patient progressed on study.
Conclusion:
In combination, PRRT with 177Lu-octreotate, the maximum tolerated dose of everolimus is 7.5 mg daily.
Introduction
Radionuclide therapy with Lutetium-177 was introduced more than a decade ago for targeted treatment of advanced gastro-entero-pancreatic neuroendocrine tumors (GEP-NETs) in the form of 177Lu-octreotate, which locks onto the somatostatin receptor overexpressed and upregulated on these well-differentiated tumors. 1 Peptide receptor radionuclide therapy (PRRT) has ever since been shown to be effective and safe in many small clinical trials, although the absence of randomized controlled trials of 177Lu-octreotate has precluded acceptance of PRRT in mainstream oncology practice. 2
Randomized controlled trials of 177Lu-octreotate PRRT are underway, but phase II studies over the past decade have demonstrated objective response rate (ORR) in 25% of GEP-NET patients 3 with encouraging stabilization of progressive disease and progression-free survival (PFS) of around 3 years. 3 –5
We have previously shown in phase II clinical studies that combining radiosensitizing drugs, such as capecitabine and temozolomide, can improve both the ORR and PFS of PRRT with little increase in toxicity. 6,7 Our phase I study reported here explored proof-of-concept by combining the mTOR inhibitor everolimus with a standard four-cycle course of 7.8 GBq 177Lu-octreotate PRRT to define maximum tolerated dose (MTD) and dose-limiting toxicity (DLT) and to evaluate objective response.
Everolimus inhibits mammalian target of rapamycin (mTOR), which is a serine-threonine kinase regulator of cell growth, proliferation, and apoptosis in the cell cycle of NETs. Everolimus is an FDA-approved therapeutic agent for NETs. Pavel et al. have demonstrated encouraging tumor control in a randomized phase III study of everolimus plus octreotide, compared with placebo (RADIANT-2), in patients with advanced carcinoid tumors. 8 The RADIANT-3 study compared everolimus with placebo in a large group of patients with advanced pancreatic NETs. 9 A median PFS of 11.0 months was achieved compared with 4.6 months in the placebo arm, but ORR was not reported. It should, however, be noted that true tumor responses objectively measured by RECIST criteria are low in number with most targeted therapies, usually occurring in less than 10% of patients. 8 –10
Improving the treatment of patients with cancer will require the field to embrace the revolution in tumor biology to develop companion therapeutics that will enhance the efficacy of radiotherapy in nontraditional ways. 11 By screening new drugs on the basis of monotherapy efficacy, we may fail to identify agents that ultimately provide their strongest clinical impact by exploiting basic principles of radiobiology. 12
We have extrapolated this potential to explore the complementary properties of radionuclide therapy and molecular targeted therapy in a prospective proof-of-concept clinical phase IB study to define DLT and preview tumor response.
Patients and Methods
The patient eligibility criteria were as previously described for the 177Lu-octreotate/capecitabine/temozolomide studies. 7 Briefly, all eligible patients had histologically proved NETs that were inoperable and progressive on serial computed tomography (CT)/magnetic resonance imaging (MRI) scans. Exclusion criteria were standard for PRRT. 7 Patients were required to show tumor somatostatin receptor avidity on baseline 68Ga-octreotate positron emission tomography (PET) scans. All patients provided written informed consent to participate in the clinical trial. The protocol was approved by the institutional ethics committee governed by the Australian National Health and Medical Research Council guidelines for human experimentation in accordance with the Declaration of Helsinski. The study was registered ACTRN 12611000207910 and conducted under Clinical Trial Notification (CTN) provisions of the Therapeutic Goods Administration (TGA) of the Commonwealth Government of Australia 10/243.
Patient characteristics
Sixteen patients with progressive low-grade biopsy-proved NETs Ki-67 index <5%, positive on 68Ga-octreotate PET scan were studied between May 2011 and November 2014 (Table 1). There were 9 men and 7 women with a median age of 63 years (range 43–72). Primary sites included 11 small-bowel (GI-NETs) and 5 pancreas NET (PNETs). The principal metastatic sites were liver 16 (100%), nodes 10 (64%), bone 4 (27%), and peritoneum 6 (38%). Previous treatment surgery (including bowel resection, Whipple procedure, partial hepatectomy) cases were 8 (50%), somatostatin analogs were 11 (69%), chemotherapy were 6 (38%), PRRT were 5 (31%), and sunitinib 1, 90Y-microspheres were 2.
GI-NET, gastro-intestinal NET; LAR, long-acting depot injection; NET, neuroendocrine tumor; PRRT, peptide receptor radionuclide therapy; SIRT, selective internal radiation therapy.
Treatment
Radiopeptide
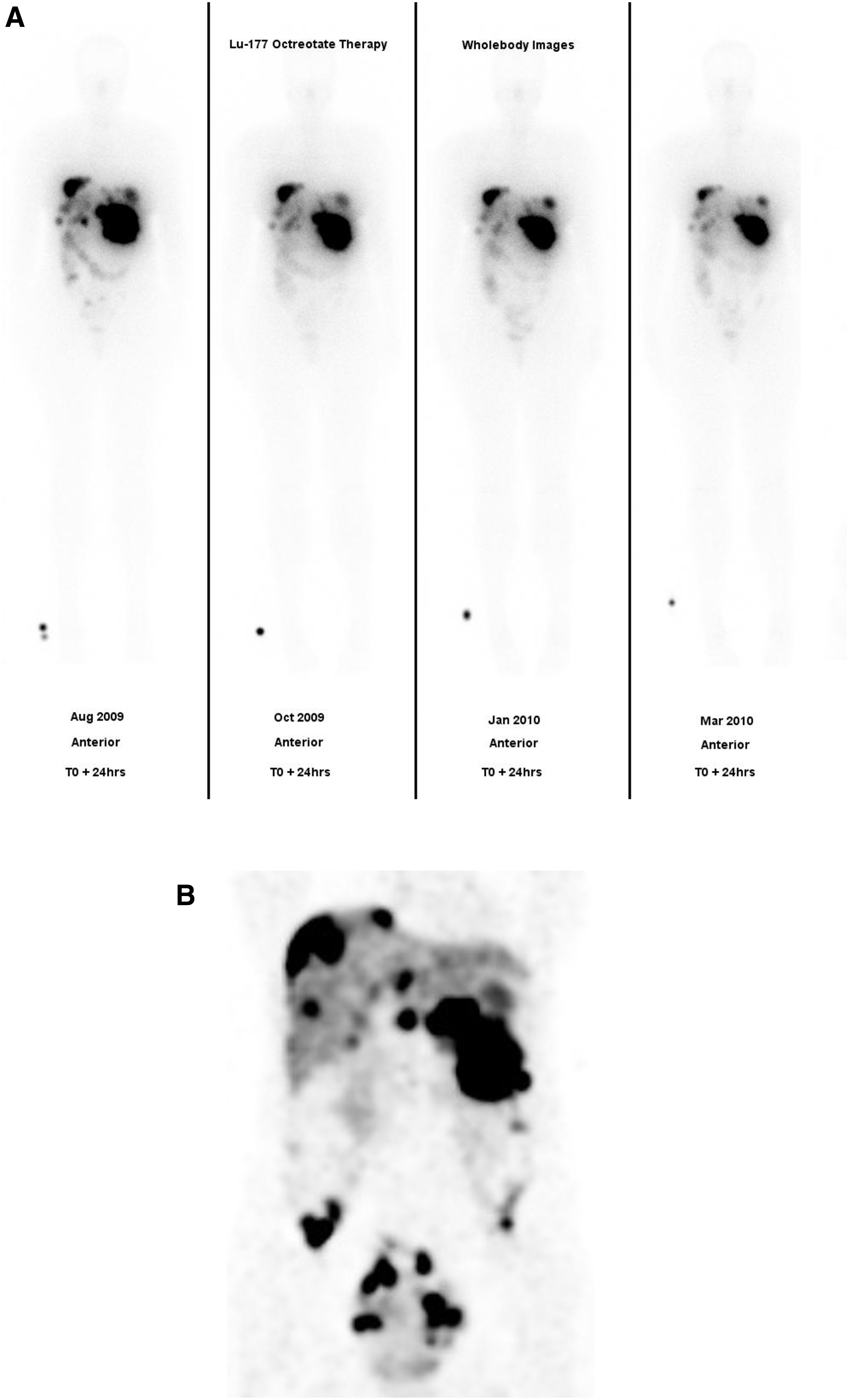
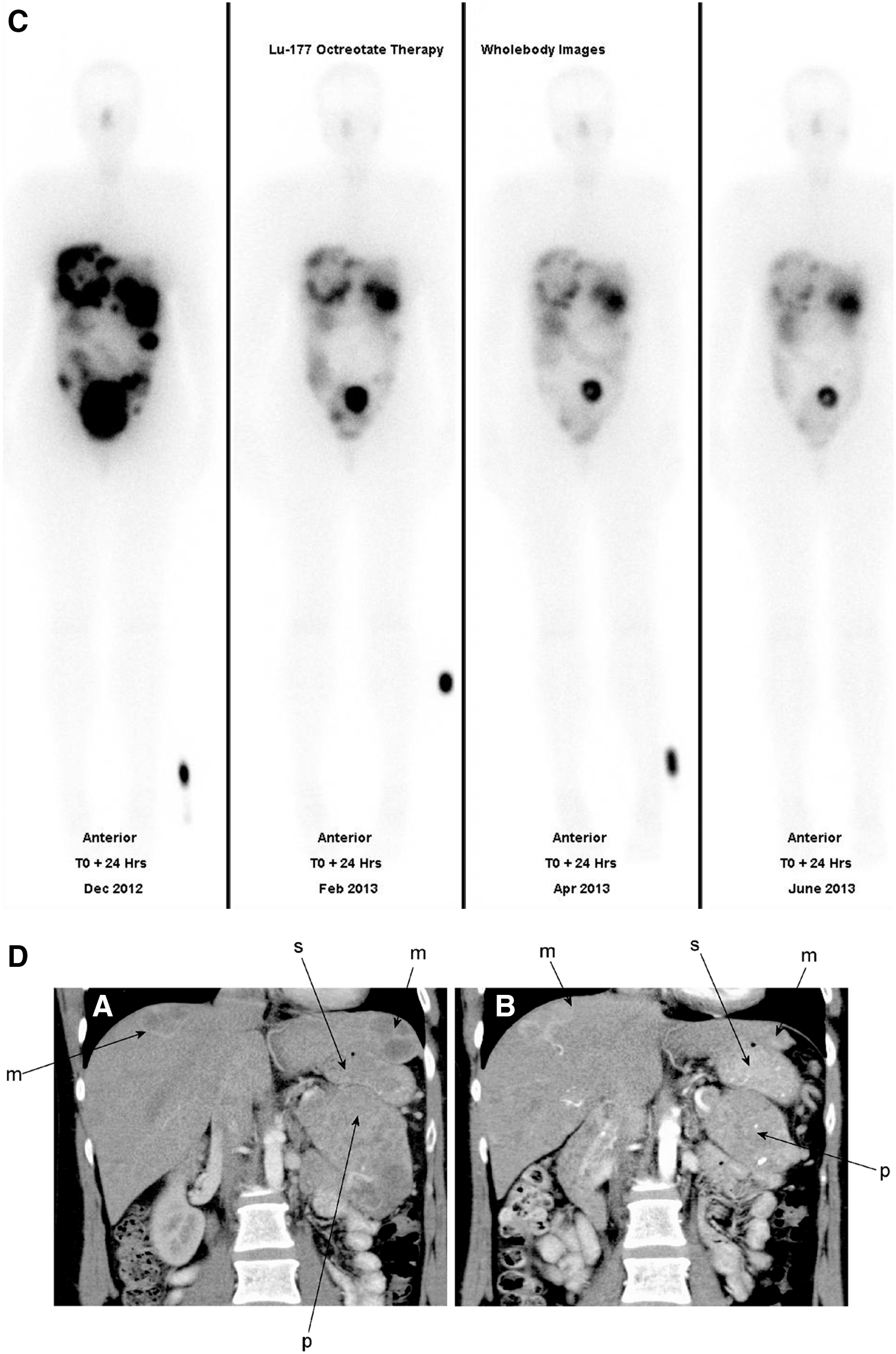
All patients were prescribed a fixed administered activity of 7.8 GBq 177Lu-octreotate to be given at intervals of 8 weeks for an intended course of four cycles, combined with everolimus. Lutetium-177 octreotate was prepared in-house from [DOTA, Tyr3] octreotate: 240 mcg of peptide was labeled with 9.3 GBq 177Lu Cl3 using an automated module. 13 Each patient received an infusion of amino acids (Synthamin; Baxter Healthcare), comprising 11.6 g/L lysine and 23 g/L arginine, at 240 mL/hour for 4 hours. At 30 minutes, 7.8 GBq 177Lu [DOTA 0, Tyr3] octreotate was co-infused with the amino acids over 10 minutes. Routine antiemetics were given in the form of IV tropisetron and dexamethasone and oral aprepitant. All patients were treated on an outpatient basis. 14 Monitoring of the tumor metabolic response to PRRT was performed by a direct comparison of semi-quantitative referenced whole body gamma imaging 24 hours after each cycle of administration of 7.8 GBq 177Lu-octreotate (Fig. 5). A definitive evaluation of objective response on RECIST version 1.1 criteria was performed on contrast CT imaging 3–6 months after the last cycle of 177Lu-octreotate PRRT.
Everolimus
Successive cohorts of patients received escalating doses of everolimus, in groupings of 5, 7.5 and 10 mg, given as a daily oral dose for the 24 weeks of radiopeptide therapy. Everolimus was commenced at the start of the first cycle of 177Lu-octeotate and continued until the administration of the fourth and final cycle of PRRT. Patients were assessed at baseline with clinical assessment, electrocardiogram, gated cardiac scan, chest radiograph, serum lipid profile, and quality of life index, in addition to measurement of tumor parameters such as Chromogranin-A assay and urinary 5-HIAA level. Interim 68Ga-octreotate PET/CT scanning was performed at the conclusion of all four cycles and compared with baseline images. During treatment, patients were monitored each 2 weeks with clinical assessment and blood testing and dose-limiting toxicities were established by standard NCI common terminology criteria (CTCAE v 4.03). Dose reductions were prescribed for any grade 3–4 toxicities, after a recovery rest period.
Results
Toxicity
Sixteen patients were treated: 4 patients at 5 mg, 9 patients at 7.5 mg everolimus, and 3 patients at the 10 mg level. Full-dose 177Lu-octreotate for four cycles was possible in 10 of 13 patients in cohorts 1 and 2, while only 1 of 3 patients completed all cycles at the 10 mg dose level. Patients at 5 and 7.5 mg doses of everolimus received 83% and 80%, respectively, of the total planned dosage over 24 weeks (Table 2). All patients required dose reduction or complete cessation of everolimus at the 10 mg level because of unacceptable toxicities. The most common reasons for dose reductions in cohorts 1 and 2 were grade 2 or 3 neutropenia and thrombocytopenia (Figs. 1 –3). Reversible grade 2 nephrotoxicity caused significant reductions of 40%–50% in creatinine clearance levels in 2 of 3 patients in the 10 mg cohort, which were not seen in the lower dose levels (Fig. 4).
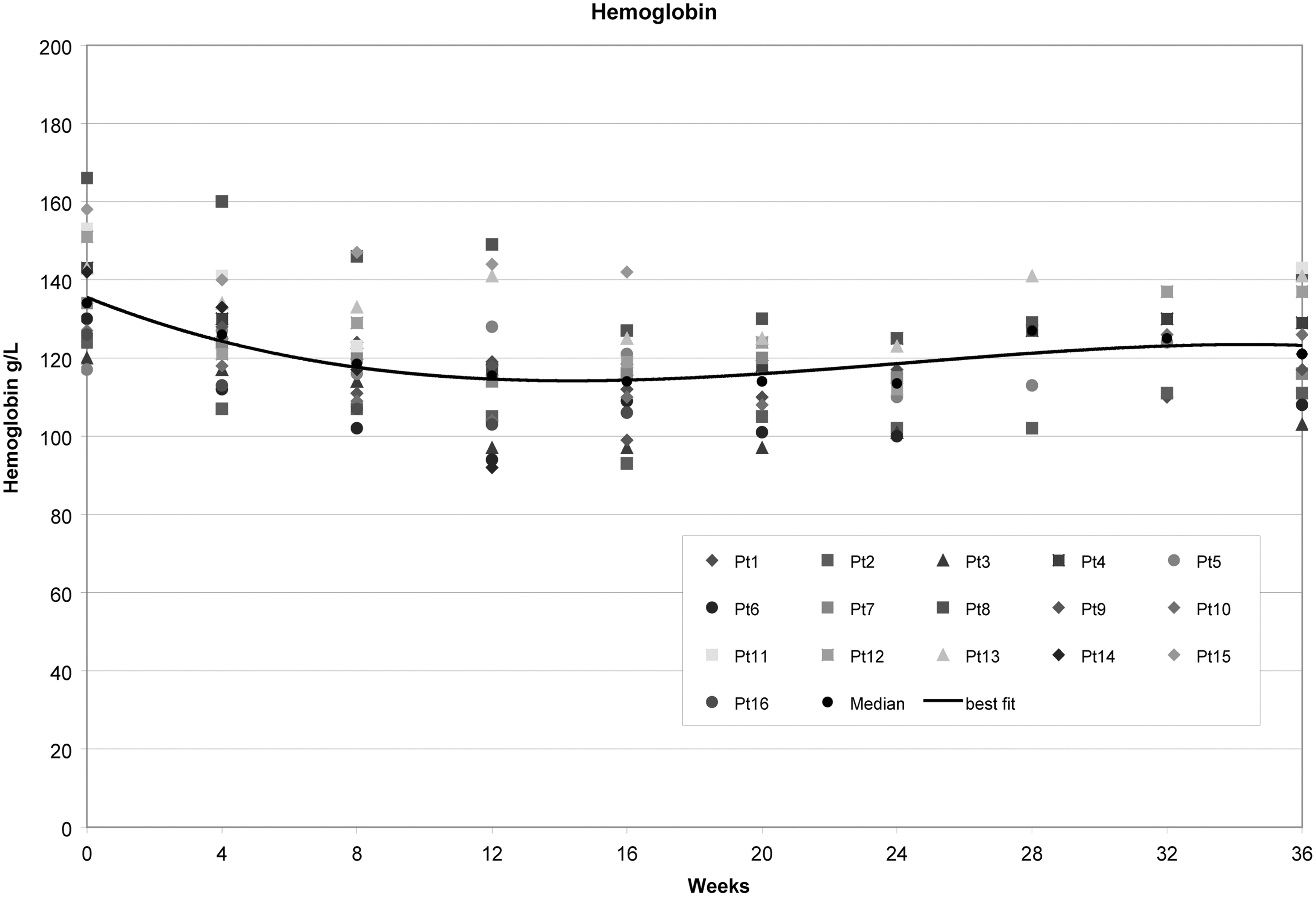
Hemoglobin levels followed for 36 weeks after commencing NET PRRT with 7.8 GBq 177Lu-octreotate at 8 week intervals for four cycles combined with daily everolimus for 24 weeks at a dose of 5 mg (patient 1, 2, 3, 6), 7.5 mg (patient 4, 5, 8, 9, 12, 13, 14, 15, 16), or 10 mg (patient 7, 10, 11). No significant anemia was observed at any dose level of everolimus till 10 mg daily in combination with PRRT. NET, neuroendocrine tumor; PRRT, peptide receptor radionuclide therapy.
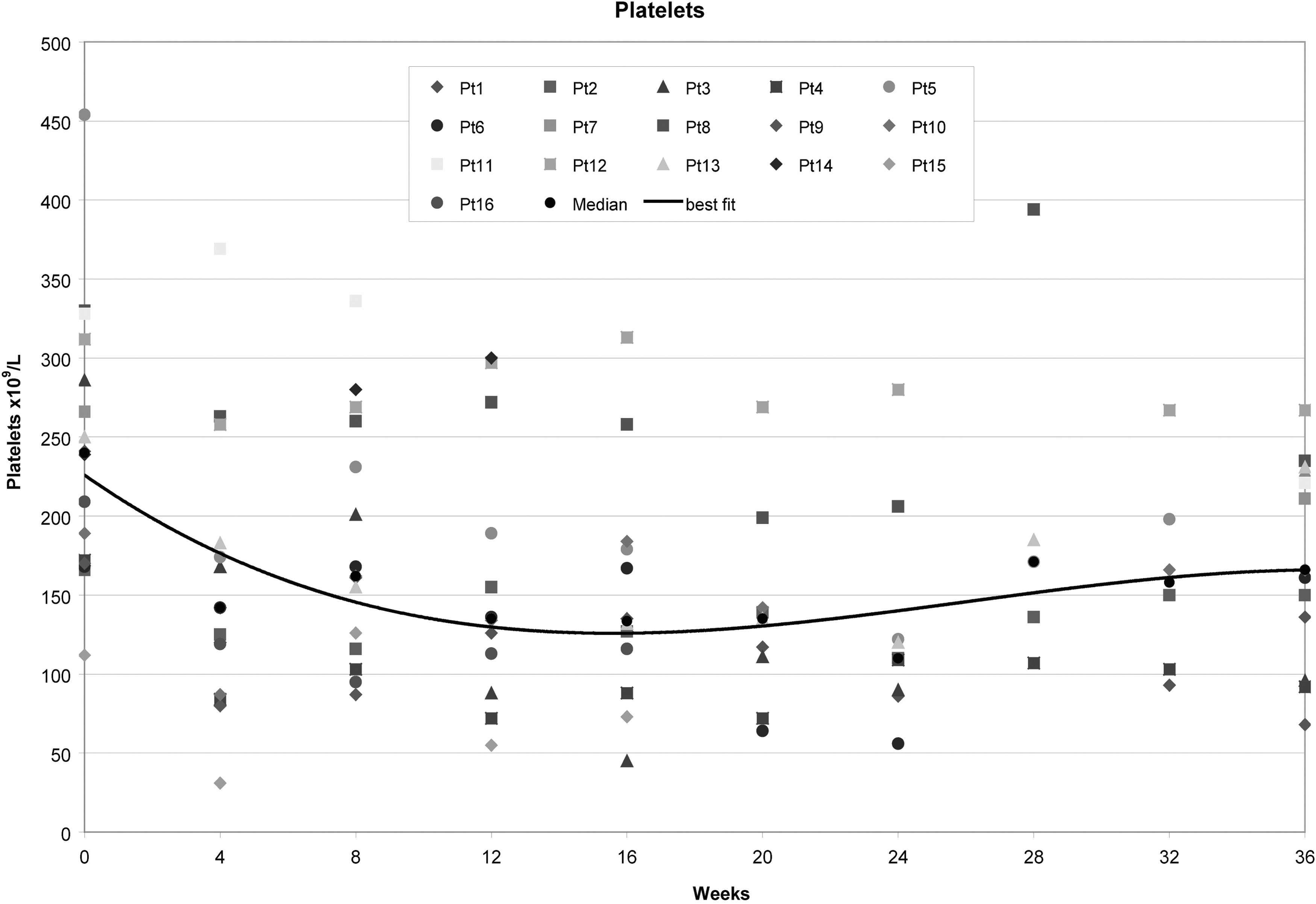
Platelet monitoring over 36 weeks after commencement of NET PRRT with 7.8 GBq 177Lu-octreotate at 8 week intervals for four cycles combined with daily everolimus for 24 weeks at a dose of 5 mg (patient 1, 2, 3, 6), 7.5 mg (patient 4, 5, 8, 9, 12, 13, 14, 15, 16), or 10 mg (patient 7, 10, 11). All patients required dose reduction, or complete cessation, of everolimus at the 10 mg level because of unacceptable toxicity, which included thrombocytopenia. Some patients in the 5 and 7.5 mg cohorts also required dose reduction.

Neutrophil monitoring over 36 weeks after commencement of NET PRRT with 7.8 GBq 177Lu-octreotate at 8 week intervals for four cycles combined with daily everolimus for 24 weeks at a dose of 5 mg (patient 1, 2, 3, 6), 7.5 mg (patient 4, 5, 8, 9, 12, 13, 14, 15, 16), or 10 mg (patient 7, 10, 11). All patients required dose reduction, or complete cessation, of everolimus at the 10 mg level because of unacceptable toxicity, which included neutropenia. Some patients in the 5 and 7.5 mg cohorts also required dose reduction.
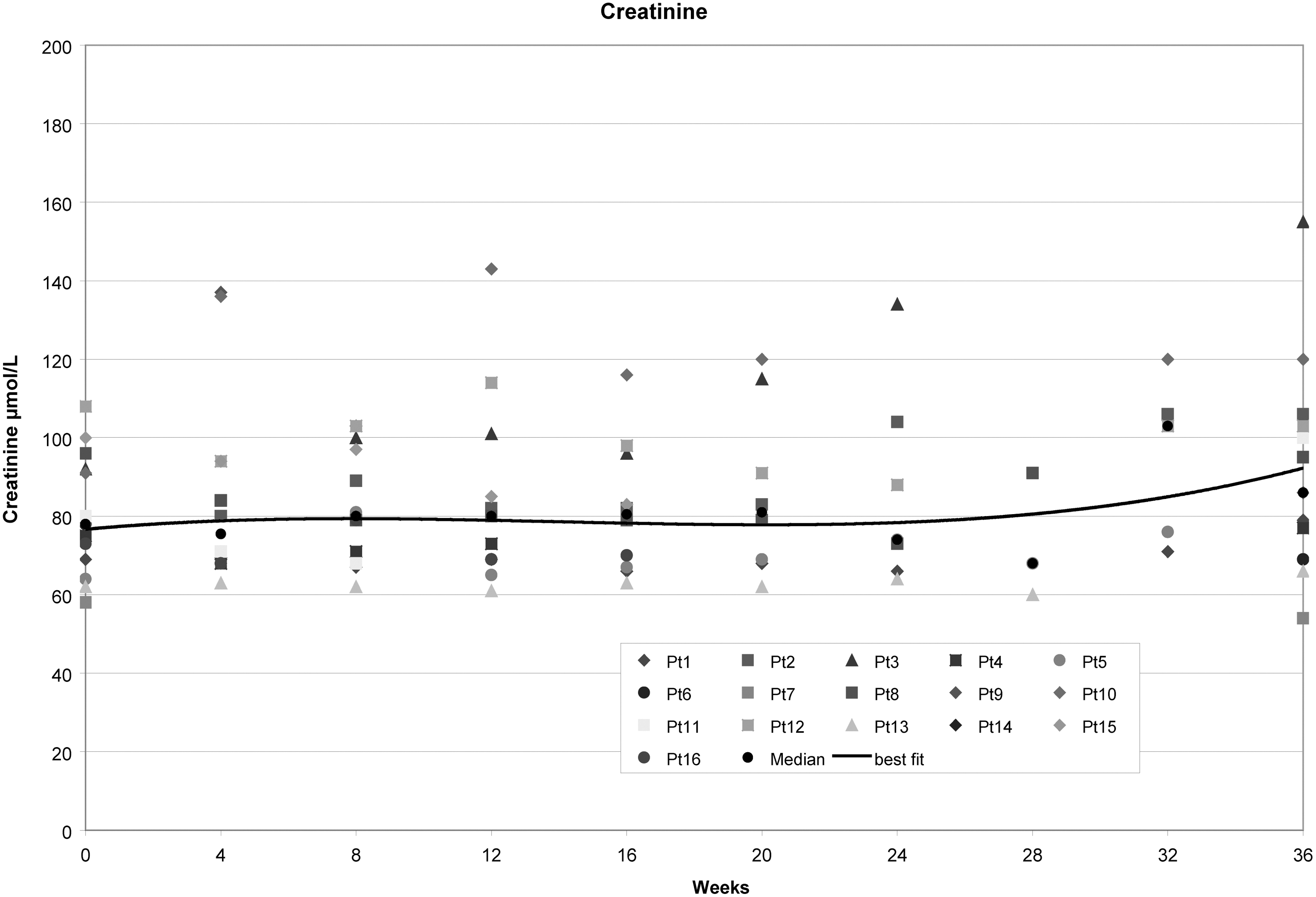
Nephrotoxicity monitoring by serial measurement of serum creatinine for 36 weeks after commencement of NET PRRT with 7.8 GBq 177Lu-octreotate at 8 week intervals for four cycles, combined with daily everolimus for 24 weeks at a dose of 5 mg (patient 1, 2, 3, 6), 7.5 mg (patient 4, 5, 8, 9, 12, 13, 14, 15, 16), or 10 mg (patient 7, 10, 11). While no obvious correlation of everolimus dose and serum creatinine levels is apparent in this plot, 2 of the 3 patients receiving 10 mg everolimus in combination with PRRT developed significant 40%–50% reduction in creatinine clearance, indicative of nephrotoxicity, which was reversible on cessation of the drug.
Responses
Tumor responses measured by RECIST criteria were seen at each everolimus dose level: at the 5 mg level, two PR and two stable disease (SD); at the 7.5 mg level, four PR and four SD; and at the 10 mg level, one PR and two SD (Table 3). Overall 7 of 16 patients achieved PR (44%) and no patient showed progression during the 6 month treatment period. An example of metabolic and objective response in a patient receiving 7.5 mg everolimus daily in combination with four cycles of 7.8 GBq 177Lu-octreotate is shown in Figure 5. Median follow-up was 34 months (range 18–42 months), and median overall survival was not reached. Patient survival at 12 months was 14 of 16 (88%), whereas that at 24 months was 10 of 16 (63%). No patient was lost to follow-up. Patient numbers were insufficient for valid statistical analysis.
NA, not assessable; ORR, objective tumor response; pNET, pancreatic neuroendocrine tumor; PD, progressive disease; PR, partial response; SD, stable disease.
Discussion
As a general principle, the clinical practice of oncology routinely employs a multimodality chemotherapeutic approach, which may also involve radiotherapy. In contrast, PRRT, since its inception more than a decade ago, has conventionally been used as monotherapy, although sometime varying the radionuclide component between 90Y and 177Lu-somatostatin analogs. 15 Our own practice is to combine 177Lu-octreotate PRRT with radio-sensitizing chemotherapy in our routine clinical management of advanced progressive GEP-NETs. 7
The combination of radiosensitizing chemotherapy with PRRT has led to enhanced objective responses with a minimal increase in toxicity. The addition of capecitabine and temozolomide to a standard four-cycle course of 177Lu-octreotate PRRT achieved ORR 57% in advanced GEP-NETs 7 with PFS upto 4 years. Toxicity was modest and mainly hematological. 16
Targeted biological molecular therapies may offer enhanced efficacy, improved selectivity, and concomitantly less toxicity, but their effects may not be durable when used alone. 17 Cellular pathways have multiple redundancies or alternative routes, which may be activated in response to the inhibition of a pathway. This tumor cell potential for overcoming metabolic blocks may promote the emergence of resistant cells under the selective pressure of a targeted agent, resulting in clinical relapse. Thus combination therapies are often needed to effectively treat many cancers. 17 Everolimus combined with the long-acting somatostatin analog pasireotide LAR was evaluated in a phase II randomized controlled trial in 160 patients with advanced progressive PNETs in the multinational COOPERATE-2 study, which reported a median PFS of 16.8 months versus 16.6 months for everolimus alone. 18 The objective response showed PR advantage for the combination (20.3% vs. 6.2%), but stabilization of disease was comparable in the two groups. Grade 3/4 toxicity in respect of fasting hyperglycemia was increased in the combination group (37% vs. 11%). 18
Contemporary clinical investigation of molecular targeted therapeutics may overlook agents that work most effectively in combination with radiation. 12 Co-development of innovative drug combinations with radionuclide therapy, such as that explored in our phase IB study of 177Lu-octreotate PRRT and everolimus, directed simultaneously at multiple therapeutic targets, has the potential to improve the response to treatment. We designed and commenced our clinical study before the publication of a report that concomitant everolimus actually impaired the therapeutic efficacy of 177Lu-octreotate in a rat model of neuroendocrine cancer and raised the possibility of enhancing the metastatic potential of the tumor. 19 The authors, in a later publication, acknowledged that no tumor-accentuating effects, or examples of accelerated metastasis, have been seen in NET patients treated with everolimus. 20 No such deleterious events were observed in our patient population treated with combination everolimus and 177Lu-octreotate PRRT. In a nude mouse NET xenograft model, the same authors found no evidence of distant metastasis related to everolimus therapy and speculated that the phenomenon observed in their immune-competent rat model may be immune mediated or species specific, peculiar to their preclinical CA 20948 tumor. 20 It may be conjectured that this tumor behaved similar to a more aggressive NET variant such as a small cell carcinoma, but Ki-67 values were not reported. It is always difficult to extrapolate animal preclinical data to humans, and this cautionary tale in the rat tumor model does not seem to translate to NET patients treated with everolimus in combination with 177Lu-octreotate PRRT in our, albeit limited, clinical trial experience.
The exact nature of the potential synergistic relationship in our clinical study is conjectural and may include enhancement of radiation-induced apoptosis of tumor cells by the targeted biological agent. We have examined the feasibility of this approach not only in a small pilot dose-escalation study designed primarily to document toxicity but also to initiate testing of the hypothesis that a biological modifier such as everolimus may enhance the efficacy of PRRT in patients with GEP-NETs. Everolimus monotherapy of advanced pancreatic NETs at a daily dose of 10 mg achieves objective response rates of 5% PR on RECIST criteria with a median PFS 11 months. 9
Lutetium-177 octreotate PRRT alone for GEP-NETs has a reported ORR of 30% with a standard administered activity of 7.2 GBq 177Lu-octreotate for four cycles at 8 week intervals. A median PFS of 40 months has been reported. 3,4
Combining everolimus with 177Lu-octreotate PRRT in our Phase IB NETTLE study was instituted with the intent to provide clinical benefit to each patient in accordance with the American Society of Clinical Oncology Policy Statement Update 2015 21 and to define toxicity. This pilot clinical proof-of-concept study was designed neither to measure pharmacokinetics nor to collect dosimetry data, and it was not powered for valid statistical analysis of variables pertaining to response and toxicity differences between patients. For instance, 4 of 5 pNET patients achieved PR, a finding, which although very encouraging, requires validation in a phase II appropriately powered study.
The majority of patients were treated at the MTD of 7.5 mg everolimus with manageable toxicity, although close monitoring was essential for patients receiving this combination therapy and dose reduction of everolimus was required in several patients during their course of 24 weeks of treatment on the study protocol. No patient experienced progression of their disease over the 6 month period of combination PRRT.
Conclusion
Everolimus can be combined safely with 177Lu-octreotate to treat low-grade NETs. Toxicities were observed at all dosage levels of everolimus, but they appear manageable and reversible. The principal toxicities were hematological with both neutropenia and thrombocytopenia. Renal impairment occurred with everolimus doses above 7.5 mg and was dose limiting. The MTD of everolimus was 7.5 mg daily in combination with 7.8 GBq 177Lu-octreotate in a four-cycle course over 24 weeks. Tumor responses were observed at each dose level of everolimus.
Footnotes
Acknowledgments
The authors wish to thank Ms. Jenny Lavin for preparation of this article, Ms. Anna Chiam for Clinical Data Management, and Mr. Phillip Calais for data collation. They also thank Novartis Pharmaceuticals for the supply of everolimus and research funding for clinical trial management of this investigator-initiated study.
Disclosure Statement
The authors have participated in meetings of the Advisory Board of Novartis Australia, but they have no other interest to declare.