
Abstract
To assess the prognostic role of total lesion glycolysis (TLG) in patients with breast cancer liver metastases (BCLM) after sequential lobar 90Y-radioembolization (90Y-RE). Seventeen patients with bilobar BCLM underwent FDG PET/CT and TLG calculation before 90Y-RE. The hepatic lobe with the highest TLG was treated in the first session. PET was performed 6 weeks postprocedure and decrease in TLG (ΔTLG) in the treated lobe was calculated before the second 90Y administration. Subjects were divided in two groups (group 1: ΔTLG >50%, group 2: ΔTLG <50%). After the two consecutive 90Y-therapies, patients underwent follow-up until death. Statistical analysis was performed to identify prognostic factors on overall survival (OS). After the first 90Y administration, 10 cases showed a ΔTLG >50% and seven had a ΔTLG value <50%. After the two consecutive procedures, the mean OS for all patients was 13.5 ± 0.8 months. Subjects with a ΔTLG >50% and ΔTLG <50% had a mean OS of 16.4 ± 0.6 and 10.3 ± 0.4 months, respectively (p < 0.001). Cox regression analysis demonstrated hepatic tumor load (p = 0.048) and ΔTLG as the only significant (p = 0.005) predictors of survival. ΔTLG after the first 90Y administration agrees with final outcome in BCLM patients after separate sequential lobar 90Y-RE.
Introduction
Breast cancer metastases still represent a serious challenge for clinicians. 1,2 Liver is a site of colonization in 12%–15% of patients with metastatic disease. In these cases, surgery represents the most effective approach, unfortunately it is practicable only in few patients with small metastases. Therefore locoregional treatments, such as chemoembolization and radio frequency, can be considered. 3
Radioembolization (RE) with 90Y-resin or glass microspheres is a relatively new technique for treatment of malignant hepatic lesions using 90Y embedded in microspheres, which are infused directly into the hepatic arterial circulation. 4 90Y spheres, once implanted in liver, can release a significant radiation burden to neoplastic cells with a relative low dose to normal parenchyma due to the different vascularization pattern. Recent reports suggest that 90Y-RE can be an effective approach for breast cancer liver metastases (BCLM). 5,6
When bilobar liver lesions are present, 90Y spheres can be administrated as either whole liver or sequential lobar treatment. Previous published reports suggested that the whole-liver embolization has more hepatic toxicity compared to sequential lobar RE. 7 In case of sequential lobar treatment, the response of the hepatic lobe treated after the first session should be assessed before the second 90Y administration.
90Y-RE results as a combination of embolization and radiation therapy, thus the standard radiologic follow-up modalities may be not sufficiently accurate to assess tumor response to treatment. 2-deoxy-2[ 18 F]fluoro-D-glucose (FDG) PET is a well-established diagnostic tool in oncology and can provide information in terms also of semiquantitative data, such as the SUV max, the functional tumor volume (FTV), and the total lesion glycolysis (TLG). 8 Gulec et al. have recently demonstrated that these values can be useful quantitative criteria for patient selection and disease prognostication in patients affected by cancer colon liver metastases treated with 90Y spheres. 9 It is worthy of note that the authors demonstrated that metabolic response in liver tumors can be detected as early as 4 weeks after 90Y-RE.
The objective of this study was to assess whether the decrease of TLG (ΔTLG), after the first 90Y treatment, can be a prognostic indicator in patients with BCLM submitted to separate sequential lobar 90Y-selective internal radiation therapy.
Materials and Methods
Patients
Seventeen female patients (mean age 59.2 ± 9.6 years) with bilobar BCLM were evaluated. The enrolment criteria were as follows: histologic proof of breast cancer; liver-only or liver-predominant disease; age ≥18 years; ability and willingness to provide written informed consent; life expectancy >3 months; Eastern Cooperative Oncology Group (ECOG) performance status ≤2; bilirubin <2.0 mg/dL, albumin >2.0 g/dL, international normalized ratio (INR) <1.5; creatinine <2.0 mg/dL; platelets ≥100.000/μL, Hb ≥9.0 g/dL, and WBC ≥1.500/μL. Patients with predominant extrahepatic disease, active CNS metastases, or diffuse peritoneal metastases were excluded.
Study design
All patients provided written informed consent before procedure and associated risk. Preprocedural evaluation included baseline imaging studies (contrast enhanced CT, FDG PET-CT, liver sonography, and clinical and laboratory examination were performed).
Angiography with selective visceral catheterization was performed to evaluate the vascular and tumor anatomy and blood-flow dynamics, enabling a determination of the optimal placement of the catheter for selective treatment. 99mTc-MAA was injected in the right or left hepatic artery. The mean applied activity for all patients was 156.2 ± 28.6 MBq of 99mTc-MAA.
After 7–10 days, patients returned to the department for the treatment session performed by selective catheterization of the main hepatic artery by transfemoral approach, embolization of gastroduodenal and gastric artery. After selective catheterization of the right/left hepatic artery, the patient, without sedation, was administered by a slow manually controlled injection lasting about 30 minutes, under intermittent fluoroscopic guidance, alternating the 90Y spheres suspended in sterile water with a contrast medium for assessing persevered anterograde arterial flow. In all cases, resin spheres (SIR-Spheres; Sirtex Medical, Sydney, Australia) were administered.
The prescribed 90Y activity was calculated as the patient-specific activity according to the manufacturer's vial applying the body surface area (BSA) formula
10
:
All the patients were treated with separate sequential lobar 90Y administration with a 6-week interval between the two procedures. TLG was determined on pretreatment PET scan using PET VCAR (GE Healthcare, Milwaukee, WI). Every lesion was segmented with a threshold of 42% of the maximum SUV value within the bounding box of the lesion. All the metastases in liver were considered. The hepatic lobe with the highest TLG value was considered the target lobe and treated at the first 90Y-RE session.
ΔTLG of target lobe was calculated on the PET scan performed 6 weeks after the first 90Y administration.
Six weeks after the two consecutive REs, patients underwent FDG PET. To assess metabolic response to 90Y-RE, the follow-up PET-CT was compared to the pretreatment scan according to the PET Response Criteria in Solid Tumors (PERCIST). 11
Afterward, patients resumed a routine schedule of laboratory tests and imaging at quarterly intervals until reaching the endpoint (death). Survival was calculated from the time of first 90Y-treatment to the time of death.
FDG PET imaging
All patients were submitted to PET-CT scan 60 minutes after the intravenous administration of 3.7 KBq/kg of FDG. The PET-CT device was a Discovery ST (GE Healthcare) with bismuth germanate crystal units arranged to form 24 rings combined with a 16-slice Light Speed Plus CT scanner. The average FWHM axial resolution of PET (full width at half maximum) is 5.2 mm and system sensitivity 9.3 cps/KBq for 3D acquisition mode. Scanning was performed from the neck to the proximal thigh in 3D modality, with an acquisition time of 3 minutes per table position. Images were reconstructed by using an ordered subset expectation maximization iterative algorithm (OSEM-SV, VUEPoint HD, GE, 2 iterations, 15 subsets). The CT was performed immediately before PET in the identical axial field of view using a standardized protocol consisting of automatic tube current modulation with auto mA, tube rotation time of 0.5 sec/rotation, and slice thickness of 3.75 mm. The CT data were resized from 512 × 512 to a 256 × 256 matrix to match the PET data.
The data were transmitted to a nuclear medicine database, fused, and displayed using a dedicated software (Advantage; GE Healthcare).
90Y-PET imaging
All patients were submitted to PET scan to evaluate the pattern of spheres distribution. 12
Statistics
Overall survival (OS) was calculated by the Kaplan–Meier method (MedCalc 11.3.8.0; MedCalc Software, Mariakerke, Belgium), measured from the date of the procedure to the death of the patients. With the same method, the time to progression (TTP) in liver was calculated for the whole population. The Kaplan–Meier method was used to analyze differences in TTP and OS between patients with a 6-week ΔTLG >50% and those with ΔTLG <50%; significance was established at p < 0.05 level. To determine parameters significantly influencing survival Cox analysis, variables included in the analysis were as follows: age, bilirubin levels, tumor load, metabolic response, and presence of extrahepatic disease. Data are expressed as mean ± standard deviation.
Results
All 17 patients showed intense tracer uptake in bilobar multiple liver metastases at pretreatment FDG-PET/CT. Seven out of 17 cases presented exclusive hepatic disease. Ten patients had liver-predominant disease with extrahepatic localizations: seven presented bone lesions, two had small pulmonary lesions, and 1 had positive abdominal lymph nodes. No patients were found to have significant hepatopulmonary shunts.
Characteristics of patients' population are summarized in Table 1. Patients' clinical features and their final outcome after 90Y-RE are summarized in Table 2.
ΔTLG, decrease in total lesion glycolysis; TTP, time to progression; BCLM, breast cancer liver metastases; BM, bone metastases; R, right; L, left; PR, partial response; CR, complete response.
Pretreatment TLG ranged from 3521.7 g to 170.9 g. Among the 17 patients, the right hepatic lobe presented the predominant tumoral involvement and was treated at the first session in 15 cases. In 2 patients, the left hepatic lobe presented the highest TLG and was delivered with 90Y spheres at the first session.
Six weeks after the first 90Y-RE session, FDG-PET/CT was performed and images were visually evaluated. In three cases, almost no tracer uptake was detected in the lobe that had undergone the 90Y administration (Fig. 1). In 14 subjects, the lesions of the lobe treated with microsphere presented a reduction in number and grade of tracer uptake.
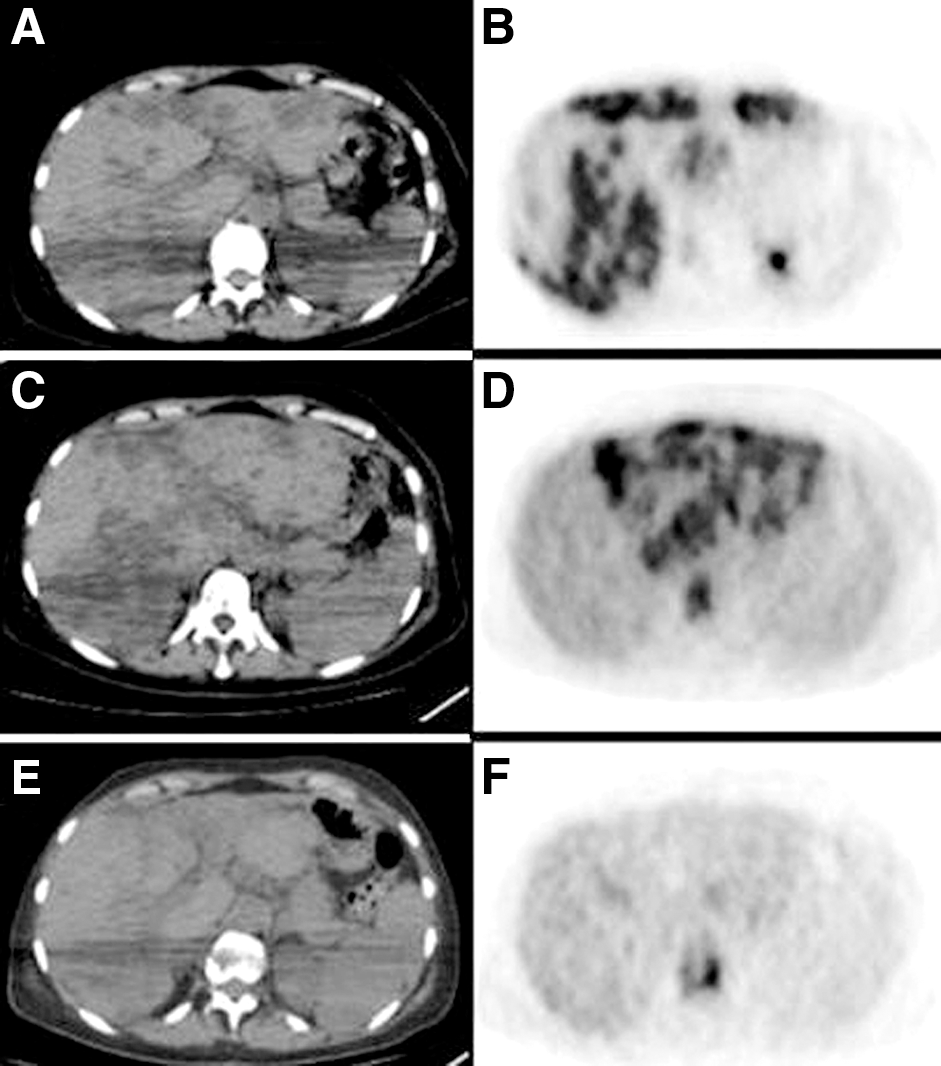
Corresponding unenhanced CT
In all patients, the lobe that had not received radioembolization presented a progression of disease (i.e., increased uptake and/or number of metastases).
90Y-PET imaging
No extrahepatic sites of 90Y spheres' uptake were registered.
Semiquantitative analysis and second 90Y-RE session
The ΔTLG was calculated in the target lobe. A decrease in the TLG was found in all patients; in particular, ten cases showed a ΔTLG >50% (mean 72.2% ± 13.8) and 7 patients had a ΔTLG value <50% (mean 30.1% ± 5.4).
The average activity of 90Y-microspheres administered was 1.8 ± 0.7 GBq.
Two among the 17 patients who underwent the 2 consecutive 90Y-RE lobar treatments showed complete metabolic response in liver at a 6-week FDG-PET/CT. The remaining 15 patients had a partial response and underwent further oncological treatments.
Clinical outcome
The mean OS for all patients was 13.5 ± 0.8 months (95% CI 11.9–15.2). Subjects with a ΔTLG >50% and ΔTLG <50% had a mean OS of 16.4 ± 0.6 and 10.3 ± 0.4 months, respectively (p < 0.001) as shown in Table 3. The Kaplan–Meier survival curve as function of ΔTLG is shown in Figure 2.
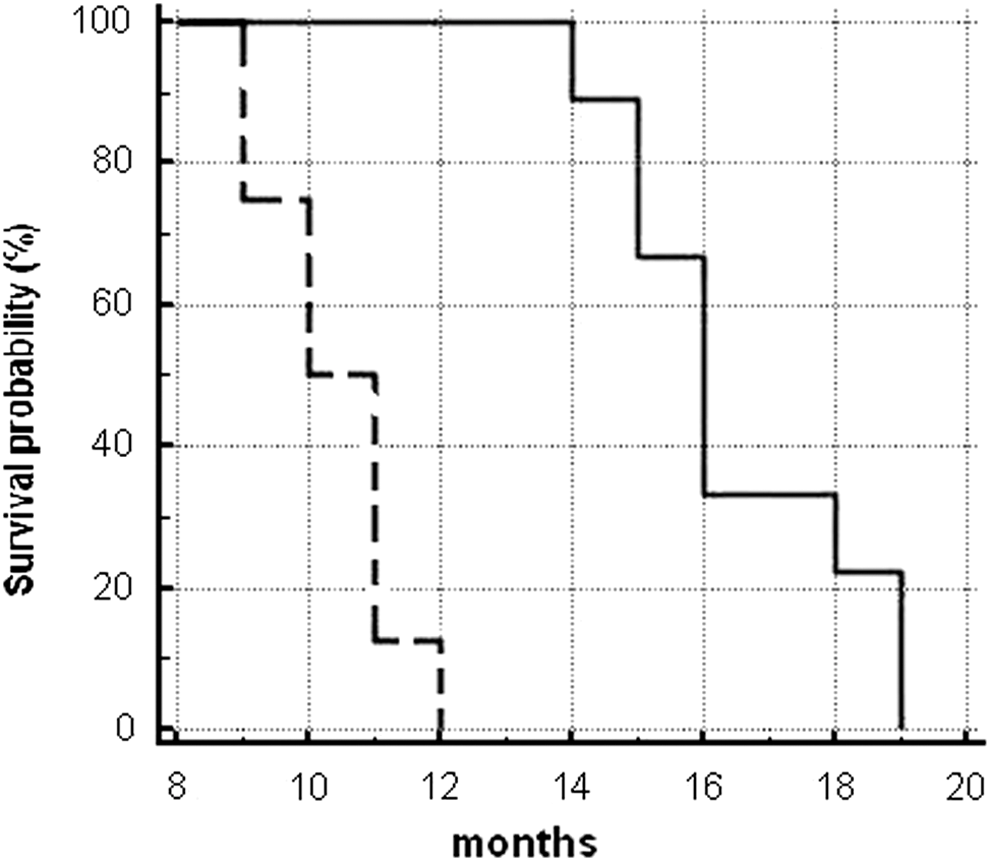
Kaplan–Meier survival analysis as function of ΔTLG. Patients with ΔTLG <50% (dashed line) had significantly lower (p < 0.001) survival than those having ΔTLG >50% (solid line).
ΔTLG, decrease in total lesion glycolysis; mo, months.
TTP resulted of 4.9 ± 0.4 months for the whole cohort. Patients with a ΔTLG >50% had a significantly longer TTP (mean 6.3 ± 0.3 months) than those with ΔTLG <50% (mean 3.4 ± 0.4 months, p = 0.001). The Kaplan–Meier TTP curve as function of ΔTLG is shown in Figure 3. Among the examined variables, Cox regression analysis demonstrated a significant impact on survival for both hepatic tumor load (p = 0.048, HR = 3.9, 95% CI 1.0–15.1) and ΔTLG (p = 0.005, HR = 0.9, 95% CI 0.85–0.97).
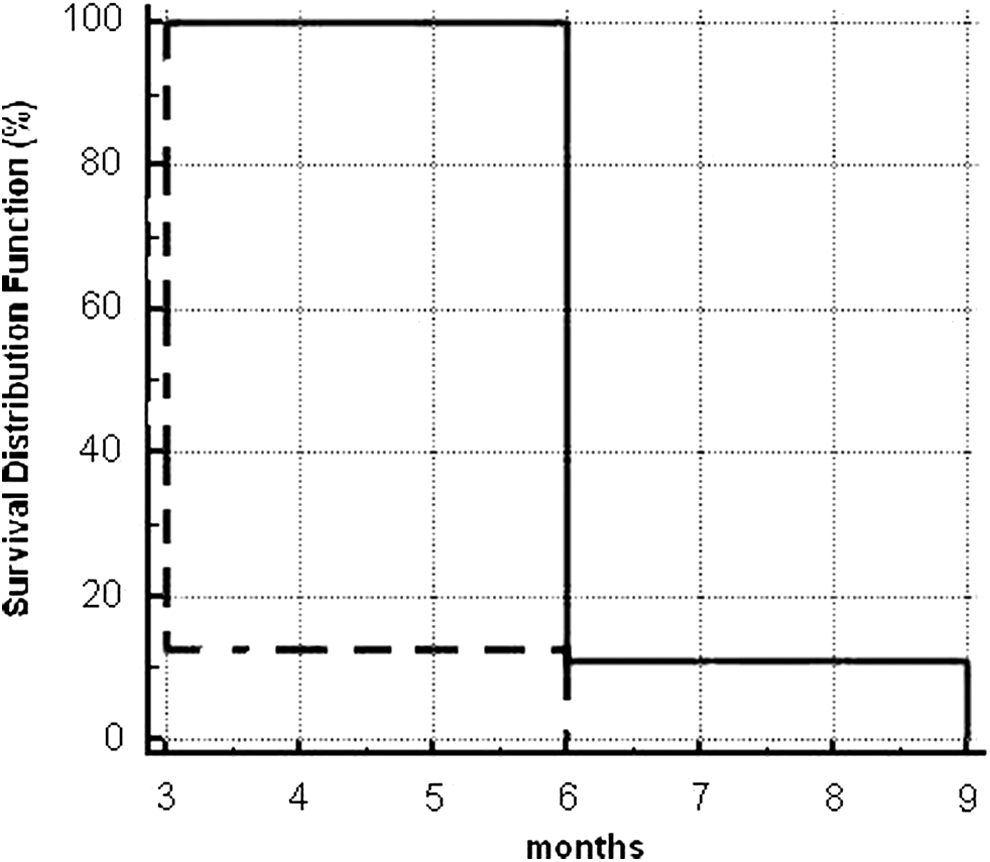
Kaplan–Meier time to progression analysis as function of ΔTLG. Patients with ΔTLG <50% (dashed line) had significantly faster (p = 0.001) time to progression than those having ΔTLG >50% (solid line).
At final survival analysis (November 2014), all patients had died of their disease.
Toxicities
Immediate complications such as nausea and mild abdominal pain were registered in 8 patients in the 10 hours following radioembolization. Routine medications allow obtaining a complete remission of these symptoms. Moderate cholecystitis (grade 2) was observed from 7 to 10 days after the procedure in 2 patients, which were successfully treated with anti-inflammatory drugs.
Late complications consisted of moderate gastritis (grade 2) in 3 cases and severe gastritis in 1 case (grade 3).
Discussion
Liver represents a site of frequent metastatic colonization both in breast cancers. In the presence of multiple or bilobar localizations, surgery is often not practicable. In such cases, patients are submitted to chemotherapy and/or locoregional treatments (i.e., embolization and/or radiofrequency). 90Y administration has emerged as a new and effective treatment for unresectable and chemorefractory liver lesions, although there are relatively few data addressing the usefulness of this therapy for BCLM. To the best of the authors' knowledge, this report is the first correlating change in TLG and overall survival in patients affected by BCLM treated with separate sequential lobar 90Y-RE.
FDG-PET has been introduced as an indispensable staging modality in many types of tumors. 13 In particular, PET/CT proved useful in breast cancer for an early detection of lymph node involvement and relapse of disease. 14 Furthermore, this imaging modality resulted useful for assessing patients' response to 90Y-RE. 15,16
In 2007, Colwell and Kennedy reported good results of 90Y-RE in 44 patients with hepatic lesions from breast cancer. 5 They found the following response rate according to RECIST: 41% partial response (PR), 47% stable disease (SD), and 5% disease progression (PD). When the response to 90Y-RE was analyzed by FDG PET, 95% of patients resulted in PR and only 5% was in SD. In a recent report, Cianni et al. evaluated the response to 90Y-RE in 52 patients with liver metastases from breast cancer both according to RECIST and FDG PET. 6 At the first follow-up performed at 8 weeks postprocedure, the majority of subjects (81%) showed a reduction of hepatic lesions' metabolism consistent with PR, among them 2 subjects showed complete disappearance of FDG uptake and were considered in CR.
When small changes in tumors after treatment should be assessed, semiquantitative methods are mandatory. In 1993 Wahl et al. evaluated the response to chemotherapy in breast cancer by using quantitative FDG-PET. 17 Haug et al. recently published a research on the role of FDG-PET in predicting survival after 90Y-RE in a cohort of 58 patients with hepatic metastases from breast cancer. 18 FDG PET was performed at baseline and 3 months after the procedure. To evaluate the response to treatment, the authors used modified PET Response Criteria in Solid Tumors (PERCIST). According to the unmodified PERCIT, in fact, the change of SUVmax in the 2 hottest lesions per organ is considered. On the contrary, Haug et al. based their definition of the response on the summed percentage change in the SUVmax in up to five of the most prominent hepatic lesions. Response as assessed with SUVmax correlated significantly with survival after 90Y RE. In the authors' experience, they found the unmodified PERCIST accurate and not time-consuming, to define response of BCLM patients to 90Y-RE. It is worth of note that in the cited article, 18 all patients received treatment of the whole liver within a single session, thus the prognostic value of PET-derived parameters in predicting survival after 90Y lobar sequential administration was not determined. In addition, the authors found the metabolic response as the only predictor of survival after RE. In this series, both hepatic tumor loads before 90Y-RE and ΔTLG were found to be significant predictors of patients' outcome, substantially in line with the results recently published by Sabet et al. 19
When bilobar metastases are present, the sequential 90Y administration is often preferred to the whole-liver treatment. It has been reported that the sequential approach, delivering partitioned doses to the left and right liver lobe at an interval of 4–6 weeks, can be useful to mitigate symptomatic RE-induced disease. 7 All patients affected by BCLM are heavily treated with chemotherapy before undergoing 90Y-RE, thus toxicity may be an important issue in these women. To this regard, the safety of 90Y spheres' administration is an argument widely discussed. In a recently published article, Kennedy et al. evaluated data from 606 patients submitted to 90Y-RE: all activity calculations for 90Y were planned using the BSA methodology as per consensus guidelines. 90Y-RE resulted to have a favorable risk/benefit profile, even among patients who had received ≥3 prior lines of chemotherapy. 20 The authors' results are substantially in agreement with Kennedy's group; the authors did not register, in fact, any radiation-induced liver disease, confirming the favorable toxicity profile of BSA method for activity calculation. Furthermore, the sequential lobar approach was found safe and efficient in BCLM subjects.
The authors did not include different histotypes in the same quantitative study. Their purpose, in fact, was to describe an innovative approach to the sequential RE by assessing the early quantitative response after the first 90Y injection. It is well known that every tumor presents specific treatment history and biology, which might result in different susceptibility to RE. In the cohort, the response of the hepatic lobe treated after the first session has been assessed by FDG-PET before the second 90Y administration. It is well known that PET is able to disclose early metabolic response to treatments, before the morphological changes are detectable by CT or MRI. It is becoming more and more important in oncology to identify, as early as possible, patients with poor clinical outcome to timely start adjuvant or palliative treatments. Visual examination of the PET scan acquired 6 weeks after the first 90Y-RE session resulted useful for assessing whether or not the treated lobe had responded to the procedure. Further information has been achieved by calculation of TLG and its modification. TLG and FTV have been recently introduced as powerful prognostic indicators in patients undergoing antitumoral therapies. 21,22 Fendler et al. have validated these PET-derived parameters for predicting survival in 80 patients with colorectal liver metastases submitted to 90Y-RE. 23 The authors performed FDG PET at baseline and after 3 months and demonstrated that decrease in FTV and TLG had a strict correlation with survival. Similar results were recently achieved by this group: the relationship between change in TLG and final outcome after 90Y-RE has been investigated in 17 patients affected by unresectable and chemoresistant intrahepatic cholangiocarcinoma. 24
The authors focused their attention on this parameter since TLG is strictly related to the viable tumoral mass. It is reasonable to speculate, in fact, that the greater residual mass after the first 90Y administration might have lead to a worse prognosis in group 2 patients (i.e., ΔTLG <50%) compared to group 1 subjects (i.e., ΔTLG >50%). The authors' results suggest that TLG and its modification represent a very effective and not so much time-consuming method to categorize patients after the first 90Y-treatment.
This study has several limitations. First of all, the cohort of patients is relatively small. Comparative studies collecting data from different centers are needed to better define the efficacy of this treatment for this population. Furthermore, breast cancer often metastasizes beyond the liver. In such patients, 90Y-RE may present limited survival benefit, although providing an adequate control of the hepatic disease. Further studies, also combining 90Y spheres' treatment with systemic therapy, should be strongly encouraged to fully define the role of 90Y-RE in the management of metastatic breast cancer.
Conclusions
The decrease of TLG after the first treatment might be useful for predicting the final outcome in patients affected by BCLM treated with sequential lobar 90Y RE. Further studies with larger series are needed to better assess whether the reduction of the tumoral mass in the lobe treated with 90Y spheres might be applied to discriminate between responder and nonresponder patients before the second lobar administration.
Footnotes
Disclosure Statement
No competing financial interests exist.