
Abstract
Recently, there has been an increasing interest in personalized approach in cancer management. Two developments could be regarded important for realization of this concept: (1) new biomarkers and (2) in vivo molecular tracers for both positron emission tomography and single photon emission computed tomography. Both approaches are successful in exploring tumor biology individually and can serve as tools to better stratify tumors for potential personalized medicine. The fundamental concept comes from the observation that one treatment does not work for all patients, even those with similar histopathology, essentially because of varying tumor genotype and phenotypic behavior pattern in each individual. Clinically validated biomarkers and tracers allow physicians to determine which patient may benefit from a particular therapy. Despite progress in the past decade, the concept is still in the early stages of clinical translation. In this review, the authors hypothesize the feasibility of integration of these two powerful techniques, which could lead to a faster translation and provide a more reliable basis toward the personalized approach in oncology. The authors believe that clinically validated biomarkers and tracers would allow physicians to determine which patients may benefit from personalized therapy. The logistics and implications of this combined approach for the day-to-day clinical oncology practice are discussed with special emphasis on neuroendocrine tumors, which demonstrates widely variable tumor biology. A logical way is also illustrated to explain how biomarkers and in vivo tracers could be complemented in a clinical workflow.
Personalized Medicine in Oncology: The Concept
“Personalized Medicine” has been conceptualized in recent years with its potential implications in the field of oncology. 1,2 The concept originated from the observation that, in a subset of patients, similar tumor types display differential clinical behavior. Treatment with a single agent or modality would thus be inefficient in all subsets of patients and the concept of “one size fits all” therapy does not necessarily work for all patients. Identification of an inefficient therapy at the earliest opportunity is of paramount importance for this group of patients, because of the fact that many of these therapies have a spectrum of associated adverse effects. Balancing efficacy with toxicity is an important consideration for any treatment approach. Hence, clinical decision making tailored to the individual patient would be beneficial rather than employing the same protocol to a broad group.
Recent advances in genomics and proteomics have opened up immense possibilities for correlating patient's genetic makeup or tumor protein profile ( = genotype) with a predictable tumor type or behavior ( = phenotype). 3 –5 Definitive examples of association between patient's genetic makeup (germline mutations), spontaneous mutations detected in cancer cells (somatic mutations), and altered protein expression profile in tumor cells, with characterization of tumor behavior, formed the basis of personalization. For example, B-Raf proto-oncogene serine/threonine kinase (BRAF)-mutated patients do not respond to panitumumab or cetuximab treatment in metastatic colorectal cancer. 6 Similarly, therapeutic grouping based on expression of estrogen receptor (ER), progesterone receptor (PR), or human epidermal growth factor receptor 2 (HER2) has been effective in breast cancer treatment. 7 Similarly, a plethora of new radiopharmaceuticals have been employed in research and clinical domains (such as receptor and metabolic pathway-specific positron emission tomography [PET] tracers) that have aided in developing targeted therapies in various malignancies and assessing their response on an individual basis. 8 Thus, accurate characterization of an individual tumor by in vitro clinical genetics and proteomics of the tumor specimen 9 –13 and in vivo molecular imaging (particularly PET-based imaging) 14 –16 would substantially impact selection of tailored therapeutic regimens.
To make the case, here we chose examples of neuroendocrine tumors (NETs) from our own routine clinical practice and discuss with specific examples how the management of a group of outliers could be benefited from a combined approach. Based on available literature and clinical experience, we present a schematic for correlation of NET differentiation with genetic background, molecular imaging outcome, and biomarker-based personalized treatment options (Fig. 1) discussed in detail as hereunder.

Schematic diagram illustrating intercorrelation between tumor classification and grade, histological parameters (Ki-67 or Mib1 index), genetic background, tumor proteomic characteristics, molecular imaging features, and the potential of the various therapeutic approaches in NET. NET, neuroendocrine tumor. Color image available online at
Classical Approach Toward Management of Neuroendocrine Tumors
NETs originate from the neuroendocrine cells in many different organs of the body (most common locations being the intestine and pancreas termed as gastroenteropancreatic NET [GEP-NET] or the lungs belonging to the thoracic NET). Clinically, they demonstrate widely variable tumor biology. Over the years, the learning of the tumor genotype, their clinical behavior, and their relation with histological grading has led to multiple systems and terminologies and subsequent various pathological classifications of NETs (two prominent systems are World Health Organization [WHO] and European Neuroendocrine Tumor Society [ENETS] classification). Interestingly, even the same standardized classifications such as WHO grading system for NET has undergone three modifications over the past three decades (in 1980, 2000, and 2010) as the understanding grew on this complex group of malignancies. Tumor grading is heavily dependent on the Ki-67 or Mib1 index of the tumor specimen, which forms a strong basis for grading and biological classification of this group of tumors: grade 1 (<2 mitoses/10 hpf and Ki-67 < 3%) and intermediate grade/grade 2 (2–20 mitoses/10 hpf or Ki-67 3%–20%) together form the well-differentiated group, whereas high grade or grade 3 (>20 mitoses/10 hpf or Ki-67 index >20%) forms the poorly differentiated subtype of NETs. This theoretical tumor grading and classification defines the inherent biological aggressiveness of the NETs. In a real-life clinical scenario, exceptions are frequently encountered. Cases where the well-differentiated tumors behave in a biologically aggressive manner have been reported, 17 or at certain specific clinical case scenarios, between 20% and 30% of patients with Ki-67 or Mib1 respond and behave akin to the well-differentiated group. Furthermore, the intermediate grade tumors, a subgroup whose biology cannot be clearly demarcated purely by the Ki-67 indices, can behave in either manner clinically and biologically. Although these observations may be controversial, such variation has been recently explored and explained by the in vivo molecular imaging studies. 18,19 The biological classification of NETs has important implications for therapeutic decision making in advanced/inoperable NETs and determine the success of a particular therapeutic approach. Among the advanced/metastatic NETs, a common observation is that chemotherapy with cisplatin and etoposide is marginally effective in well-differentiated NETs, whereas more efficacious in poorly differentiated neuroendocrine carcinoma (PD-NEC). 20 In an ideal case, the PD-NECs usually demonstrate somatostatin receptor (SSTR)-negative tumors on somatostatin receptor scintigraphy (SRS), whereas the former (i.e., the well-differentiated group) demonstrate strongly SRS-positive tumors (response rate is >70% in receptor-negative tumors compared with 10% in the former group). 21 Thus, the present consensus is to employ somatostatin analogues (subcutaneous or intramuscular) or more desirably peptide receptor radionuclide therapy (PRRT) with somatostatin analogues radiolabeled with 177lutetium or 90yttrium in tumors demonstrating adequate uptake of the tracer examined by SSTR imaging (by 68Ga-DOTATATE/TOC/NOC PET/CT or 99mTc-HYNIC-TOC scintigraphy). 22,23 Usually the well-differentiated NETs form these subsets that are candidates for this therapy. Everolimus and sunitinib are other targeted therapy agents that are approved in several countries for locally advanced or metastatic pancreatic NETs. 18,19 With multiple therapeutic options now available, it is important to select the right therapy for the right patient at the earliest, thus underscoring the importance of determining biological characteristics in the tumor that would aid in this right identification. 18,19 To that end, there have been attempts in recent years toward correlating genetic predisposition and aberrant expression of proteins that regulate cell proliferation or angiogenesis with tumor behavior. A host of high-throughput advanced techniques such as exome sequencing, transcriptomics, or proteomics have been employed to understand molecular events leading to tumor progression and to design therapeutic regimen to block specific pathways in individual tumors.
Recent Advances in Understanding Genetic Landscape of Neuroendocrine Tumors
A biomarker refers to an easily measurable biomolecule whose presence or absence from concerned tissue or body fluids acts as a specific indicator of underlying pathogenesis and facilitates diagnosis or treatment by accurately predicting cause, progression, treatment response, or relapse. 24 Conventionally, diagnosis of NETs is based on location of the tumor, routine histological examination, and increased levels of plasma chromogranin A (CgA), whereas pathological evaluation relies on CgA and synaptophysin immunostaining, Ki-67 proliferation index, and mitotic count. 25 Prognosis is often multivariate and depends on stage of the tumor at the time of diagnosis, aggressiveness, and response to therapy. However, a group of outliers that fail from therapy would benefit from cellular-based personalized management. Recent advances in high-throughput methodologies have opened up a plethora of prospective markers that may evolve a comprehensive landscape of molecular events driving aberrant cellular pathways that play a crucial part in determining susceptibility, precise diagnosis, and predicting disease progression, therapy options, and prognosis.
Biomarkers in gastroenteropancreatic neuroendocrine neoplasms
Gastroenteropancreatic neuroendocrine neoplasms arise in esophagus, stomach, small intestine, pancreas, colon, appendix, cecum, and rectum. 26 They are classified into low (G1), intermediate (G2) grade well-differentiated neuroendocrine tumors (GEP-NETs), and high (G3 grade) poorly differentiated neuroendocrine carcinoma (gastroenteropancreatic NEC [GEP-NEC]). 26 The individual variation of the various genetic mutations and their importance for biomarker determination for personalized oncology have been discussed in a site-specific and tumor characteristic-specific manner.
Pancreatic neuroendocrine neoplams
Pancreatic neuroendocrine neoplasms are classified into low (G1), intermediate (G2) grade well-differentiated pancreatic neuroendocrine tumors (Pan-NETs), and high (G3 grade) poorly differentiated pancreatic neuroendocrine carcinoma (Pan-NEC). About 3% of the primary pancreatic neoplasms are neuroendocrine in origin. 27 Majority of the well-differentiated Pan-NETs harbor somatic mutations in genes MEN1 (44%), DAXX (25%), or ATRX (18%), although these genes were unaffected in poorly differentiated Pan-NECs. 28,29 To the contrary, majority of the poorly differentiated Pan-NECs harbor somatic mutations in genes TP53 (95%), Bcl-2 (75%), or RB1 (75%), although these genes remain largely unaffected in well-differentiated Pan-NETs. 29 Mutations in MEN1, DAXX, or ATRX are associated with better survival, 28 although complete loss of DAXX or ATRX expression leads to chromosome instability and reduced survival. 30 Multiple endocrine neoplasia type 1 (MEN1) encodes menin, a tumor suppressor gene for endocrine tissues, that regulates gene transcription and is an integral component of histone methyltransferase complex, 31 whereas death-domain-associated protein (DAXX) and a thalassemia/mental retardation syndrome X-linked (ATRX) are subunits of chromatin remodeling complex that control replication-independent chromatin assembly at telomeres. 32 TP53 (tumor protein 53) and RB1 (retinoblastoma 1) are tumor suppressors that regulate cell growth and mutations in these genes are associated with a variety of cancers in humans. 33 Bcl-2 is an oncogene that regulates cell death by apoptosis and its overexpression has been associated with higher proliferation rate in higher grade NECs because of inhibition of apoptosis, 29 neuroendocrine differentiation, 34 aggressive malignant phenotype, 35 and resistance to chemotherapeutic agents that induce apoptosis. 36
Both Pan-NETs and Pan-NECs display aberrant expression of proteins that could act as the indicators of altered pathways and would be potentially useful predictors of prognosis. Tuberous sclerosis 2 (TSC2) and phosphatase and tensin homologue (PTEN) are the key inhibitors of the Akt/mammalian target of rapamycin (mTOR) pathway and their loss-of-function mutations in Pan-NETs are indicative of tumor proliferation, shorter disease-free, and overall survival due to activation of mTOR pathway. 28,37 Mutations in tumor suppressor NF-1 gene, which regulates mTOR pathway through regulation of TSC2, may also be involved in tumor development. 38 In contrast, enhanced expression of catalytic subunit of phosphatidylinositol 3-kinase (PIK3CA) was found to be associated with higher MIB-1 index in Pan-NETs, 39 but such correlation was not observed in Pan-NECs. 40 Elevated expression of tyrosine kinase receptors such as stem cell factor receptor (c-KIT), platelet-derived growth factor receptors (PDGFRs), vascular endothelial growth factor receptor (VEGFR), and epidermal growth factor receptor (EGFR) leads to metastasis and angiogenesis. 41,42 Expression of KIT in Pan-NETs has been associated with larger tumors, higher WHO grading, distant metastasis, lymphovascular invasion, and lower survival rate. 43 Pan-NETs with CK19 expression had similar physiological features as those with KIT expression, but had better survival rate. 43 However, expression of both the markers, KIT and CK19, has been associated with significantly poor prognosis and lower survival. 43,44 High expression of DNA repair enzyme O 6 -methylguanine DNA methyltransferase (MGMT) is associated with temozolomide resistance in Pan-NETS, whereas Pan-NETs with low expression of MGMT are suitable for temozolomide therapy. 45,46
Small intestinal neuroendocrine neoplams
Small intestinal neuroendocrine tumors (SI-NETs) are the most common but least understood with respect to their protein expression. 47 Cytosolic expression of oncogene mTOR or loss of nuclear ATRX expression was evident in 76.2% or 13% of the ileal-NET samples, respectively. 48 Exome sequencing of SI-NETs identified (1) genetic alterations in the PI3K/Akt/mTOR pathway in 29% of the tumors, (2) amplification of oncogene SRC or HSP90 in 23% or 10.5% of the tumors, respectively, (3) and deletions in signal transducers SMAD2 and SMAD4 in 45.8% of the tumors. 49 About 8.5% SI-NETs harbor somatic mutations in CDKN1B (cyclin-dependent kinase inhibitor 1B) gene. 50
Biomarkers in pulmonary neuroendocrine neoplasms
As per WHO classification, the pulmonary-neuroendocrine neoplasms (NENs) comprise typical carcinoid (TC, low grade), atypical carcinoid (AC, intermediate grade), large cell neuroendocrine carcinoma (LCNEC, high grade), and small cell lung cancer (SCLC, high grade). 51 TC and AC of lung are well-differentiated pulmonary neuroendocrine tumors (pNETs), whereas LCNEC and SCLC are poorly differentiated pulmonary neuroendocrine carsinoma (pNECs). 52 About 25% of primary lung neoplasms are of neuroendocrine origin. 52
About 13% of pNETs had genetic background of MEN1 gene mutation, however, low expression of MEN1 was associated with adverse disease outcome. 53 In addition to MEN1, other chromatin remodeling genes ARID1A and PSIP1 genes were mutated in pNETs but TP53 and RB1 genes were not significantly affected. 54 In contrast, TP53 and RB1 mutations were highly prevalent in SCLC. 55 Histone modifiers of the SWI/SNF complex were mutated in pNETs, whereas CREBBP, EP300, and MLL genes were mutated in SCLC. 54,55
Coexpression of c-KIT and Bcl-2 in pNECs was associated with higher grade, 56 whereas overexpression of TP53 and Bcl-2 or loss of CD44v6 correlated with more aggressive pNENs. 57 Lung NECs also displayed loss of PTEN from both cytosol and nucleus and had concomitantly low levels of TP53 and USP7 but global increase in the levels of SUMO2/3. 58 One study described elevated serum levels of complexin-2 (CPLX2) and its correlation with lymph vessel invasion, pathological stage, and poor disease-specific survival in the patients of pNECs. 59
Molecular Imaging: How Can It Aid in Personalized Medicine
Molecular imaging with PET and single photon emission computed tomography (SPECT) has several advantages compared with the conventional anatomical imaging. The detailed technical specifics are beyond the scope of this review and the readers are suggested to peruse other communications that deal with the concept in a detailed manner. 14,60 Functional molecular imaging encompasses both radionuclide-based methods (such as PET and SPECT) and nonradionuclide-based methods (such as functional magnetic resonance imaging, magnetic particle imaging [MPI], and optical imaging). In vivo molecular imaging affords the ability to image tumor biology and subsequent phenotypic heterogeneity. This idea, nowadays popularly described by the term “radiomics,” includes all quantitative in vivo imaging for tumor phenotype mapping. 61,62 Both tumor biology and tumor phenotype in an individual are critical determinants of treatment outcome in cancer, where Molecular Functional Imaging (MFI) has a major role to play. 63,64 The major strength of in vivo molecular imaging compared with the in vitro diagnostics is that it provides tumor phenotype assessment on a global and real-time scale by addressing the complex interactions in an individual patient.
Drawing examples from the NETs, we have earlier explored the significance of the dual tracer imaging approach (with SSTR imaging with 68Ga-DOTATATE/TOC/NOC PET/CT or 99mTc-HYNIC-TOC scintigraphy and glucose metabolism with FDG) in exploring tumor biology of the NETs in both GEP-NETs and thoracic NETs. 63,64 As the Ki-67 indices increase, the tumors tend to illustrate more FDG uptake and reduction in SSTR positivity. Typically, the well-differentiated low-grade NETs are SSTR positive and FDG negative (Fig. 2). In contrast, the poorly differentiated group with high Ki-67 index would ideally be SSTR negative and FDG avid (Fig. 3). Although this is usually the rule, as mentioned in the section, “Personalized Medicine in Oncology: The Concept,” exceptions can be encountered where molecular imaging can improve the disease characterization compared with only Ki-67-based grading approach (Figs. 4 –6). Also, as highlighted before, the patients with intermediate grade Ki-67 indices can demonstrate a varying biology, a place where the dual tracer imaging approach can be of substantial help (Figs. 5 and 7) in disease characterization and thereby tailoring treatment. It is now an evolving concept that the tumors that are highly FDG positive might be targeted with combined chemo-PRRT to obtain the best results. This needs to be examined further. Another area is when the tumor Ki-67 index is between 20% and 30%, where if the metastatic lesions continue to show high SSTR avidity on pretreatment imaging, PRRT continues to be a potential therapeutic option. 18,65
Well-differentiated (G1) SSTR-positive and FDG-negative NET. A 35-year-old male was diagnosed for a well-differentiated NET of ileocaecal region (Mib 1 index <2%) for which he had undergone right hemicolectomy. Subsequently he had undergone three cycles of chemotherapy with cisplatin and etoposide, but had progressive hepatic metastases and abdominal pain and was referred for consideration of PRRT. 68Ga-DOTATATE PET-CT scan shows multiple SSTR-positive lesions in the liver. 18F-FDG PET-CT scan was normal. He was treated with multiple cycles of 177-Lu-based PRRT with a cumulative dose of 670 mCi. There was a dramatic response with total resolution of all the constitutional symptoms. Follow-up 68Ga-DOTATATE PET-CT scan at 32 months shows similar lesions as those of pretherapy scan. Serum CgA level was almost same as baseline. Patient was labeled to have stable disease. SSTR, somatostatin receptor; PRRT, peptide receptor radionuclide therapy; PET, positron emission tomography; 18F-FDG, fluorine-18 fluorodeoxyglucose; CgA, chromogranin A; NET, neuroendocrine tumor.

Poorly differentiated (G3) SSTR-negative and FDG-positive NEC. A 25-year-old female patient initially presented with vomiting and generalized weakness. CT scan of the abdomen shows a mass in the body and tail of the pancreas, as well as multiple liver lesions. CT-guided liver biopsy revealed it to be NEC, with MiB1 index being 45%. 99mTc-HYNIC-TOC shows no SSTR-positive lesions. The right kidney was pushed to the front by the huge mass. 18F-FDG PET-CT scan shows intense 18F-FDG-avid lesions in both lobes of the liver and in the body and tail of the pancreas. The patient was considered for chemotherapy with carboplatin and etoposide (Reprinted with permission, Patel et al.
2
). NEC, neuroendocrine carcinoma. Color image available online at

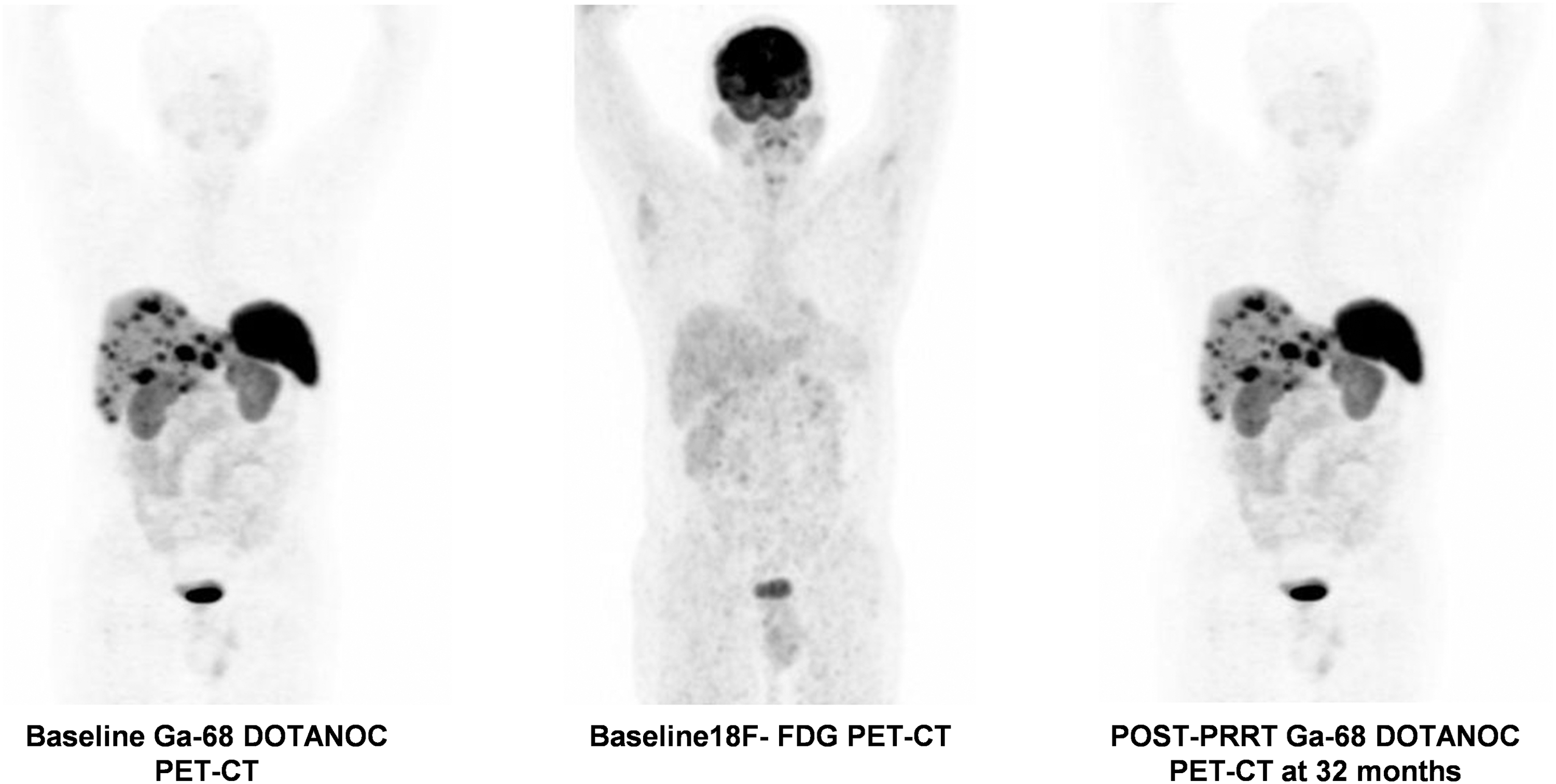
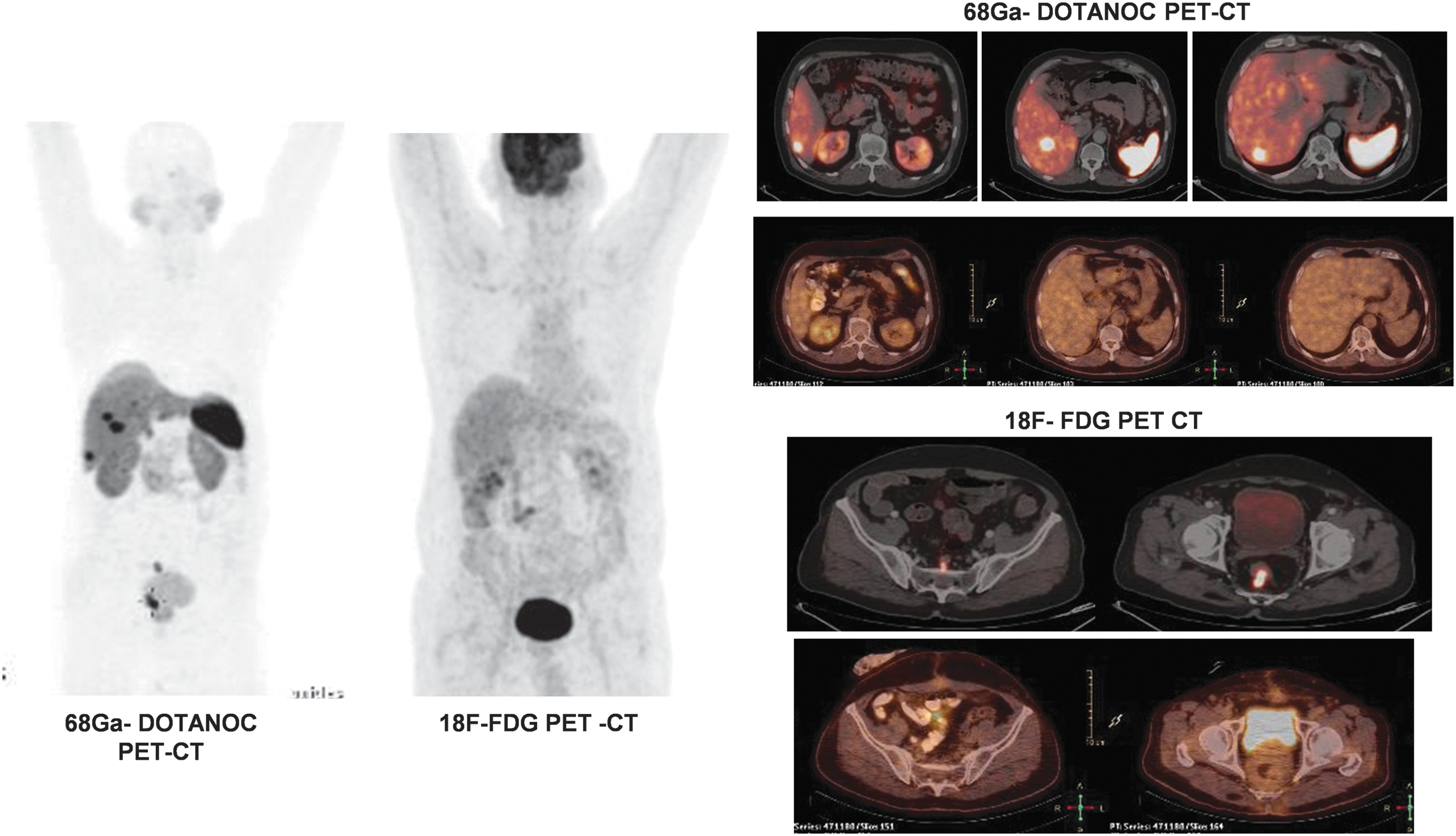
Poorly differentiated (G3) SSTR-positive and FDG-positive NEC. A 46-year-old female was a known case of NET of pancreatic tail; biopsy from pancreatic mass shows this to be a poorly differentiated NEC with Ki-67 index 22%. She was operated with resection of mass with splenectomy. Subsequently, she presented with recurrence of pain and CT scan of abdomen shows recurrence of mass in the tail region of the pancreas with infiltration of the left kidney as well as left adrenal gland. 68Ga-DOTANOC scan shows SSTR-positive pancreatic tail mass lesion with extension in left kidney and left adrenal gland. The pancreatic tail lesion was FDG avid on 18F-FDG PET-CT scan. The patient was treated subsequently with three cycles of PRRT with 177-Lu DOTATATE of cumulative dose of 458 mCi. Although there was initial symptomatic response in terms of resolution of abdominal pain and reduction in the frequency of vomiting after three cycles of PRRT as well as reduction in tumor marker (serum CgA level from 334 to 102 ng/mL), both 18F-FDG PET-CT scan and 68Ga-DOTATATE PET-CT scan show multiple new lesions after three cycles, clearly suggesting disease progression, although there was decrease in the size and the intensity of the pancreatic tail lesion in both scans. In view of scan features of disease progression at 16 months after first therapy, the patient was considered for chemotherapy.
Well differentiated (G2) with intermediate Mib1 index, SSTR-positive and FDG-negative NET. A 68-year-old male, initially presented with constipation and weight loss. Colonoscopy shows a large polypoidal growth in lower rectum at about 7–8 cm from the anal verge. Biopsy from the same site proved it to be a rectal NET with MiB1 labeling index being 10%. CT scan shows two heterogeneously enhancing hypodense lesions in the liver one in seg IV and one in seg VI. He underwent three cycles of chemotherapy with cisplatin and etoposide followed by low anterior resection earlier. The patient was referred for consideration of PRRT. 68Ga-DOTATATE scan shows SSTR-positive liver lesions in right lobe. 18F-FDG PET-CT scan shows no FDG-avid lesion. The patient was treated with three cycles of 177-Lu DOTATATE-based PRRT (with cumulative dose of 476 mCi). At 34 months after first cycle of PRRT, the patient has overall reported resolution of symptoms, fall in the serum CgA level (serum CgA from 100.20 to 24 ng/mL), and stable disease status on follow-up scan, which shows similar lesions. Color image available online at
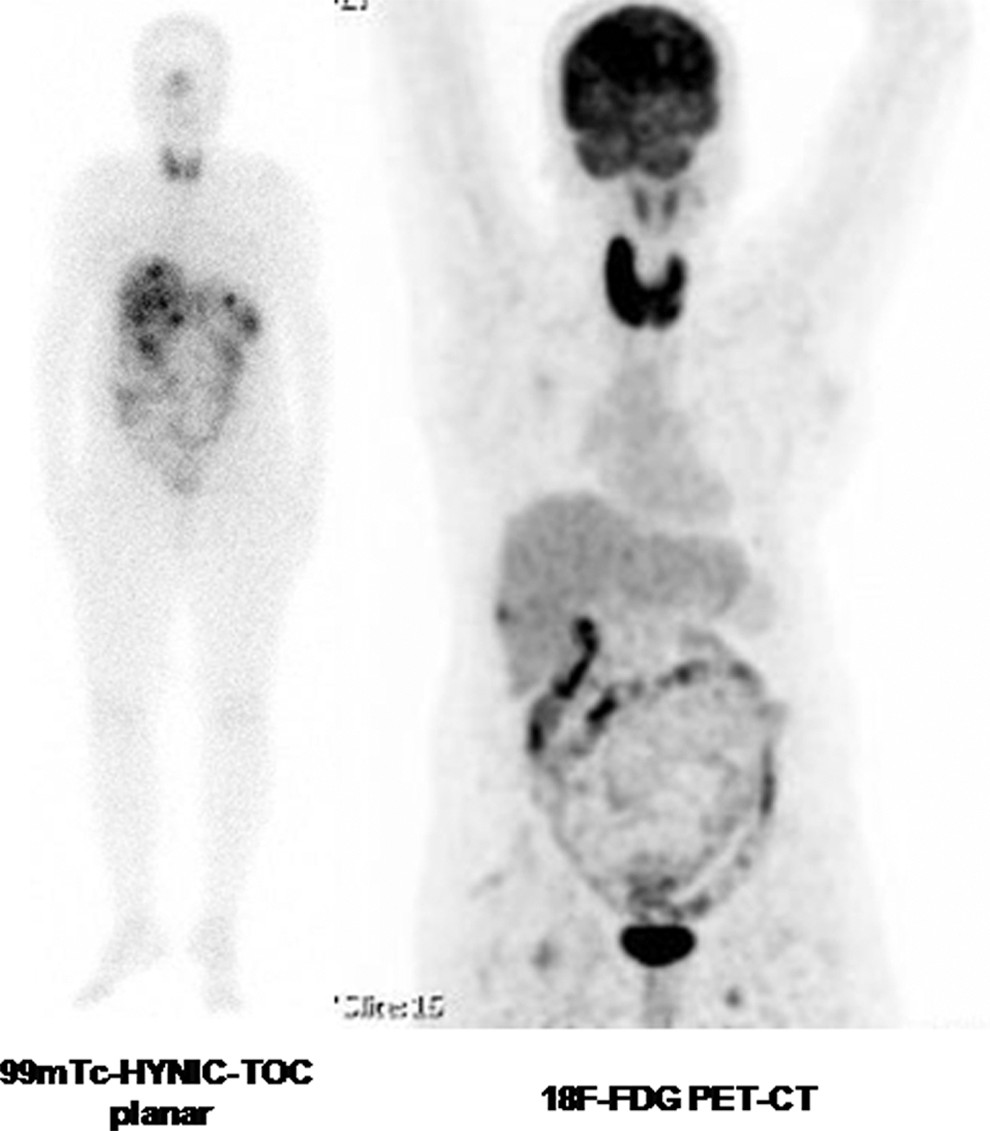
Poorly differentiated, high Mib1 index (20%), SSTR-positive, and FDG-negative NET. A 66-year-old female with initial presentation of abdominal pain and constipation. CT scan shows multiple liver lesions and periportal and perirectal lymph nodes. Biopsy from the liver lesions reported it as poorly differentiated NEC (with Ki-67 index 20%). Hence the patient was diagnosed as a case of NEC of unknown primary with liver metastasis. 99mTc-HYNIC-TOC scan shows SSTR-positive liver lesions. The 18F-FDG PET-CT scan was essentially normal with a single low-grade FDG-avid lesion. The patient was treated subsequently with four cycles of PRRT with 177-Lu DOTATATE with a cumulative dose of 725 mCi. At 28 months' follow-up, the patient had complete resolution of all the symptoms after four cycles of PRRT. The biochemical tumor marker response assessment showed reduction of patient's serum CgA from 3205 to 192.4 ng/mL. After four cycles, the 99mTc-HYNIC-TOC scan shows similar lesions and 18F-FDG PET-CT scan shows no additional lesions, with the single lesion in right lobe persisting (not shown in the figure).
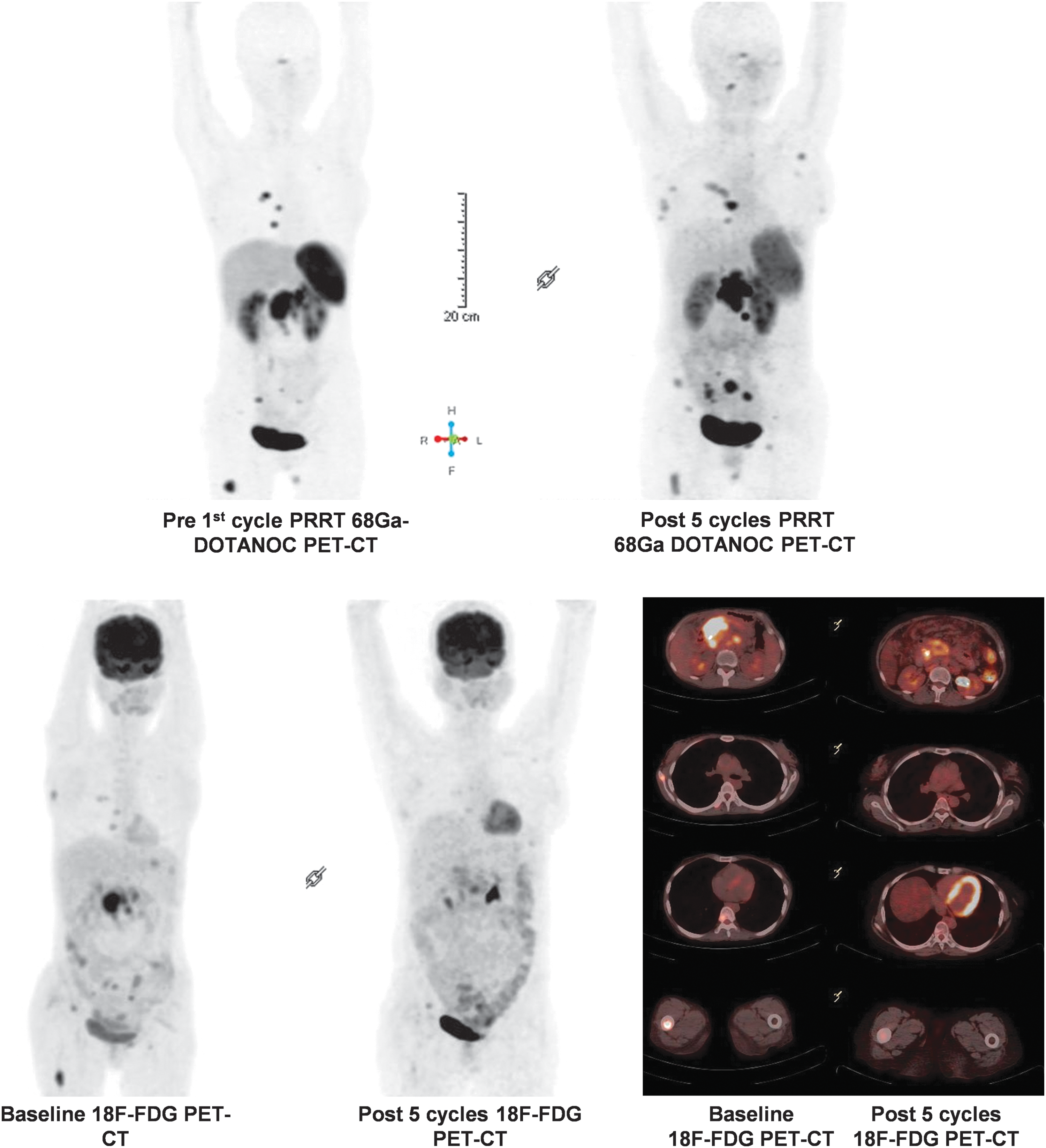
Well-differentiated (G2) with intermediate Mib1, SSTR-positive, and FDG-positive NET. A 38-year-old female with initial presentation of abdominal pain and diarrhoea. CT scan shows a lobulated heterogeneously enhancing mass in head of the pancreas with surrounding enlarged lymph nodes. Biopsy from pancreatic mass showed it as a well-differentiated NET with Ki-67 index 8%–10%. She had undergone pancreatico-jejunostomy and biliary stenting thrice and chemotherapy earlier and was put on long acting octreotide treatment. 68Ga-DOTANOC PET-CT scan shows SSTR-positive pancreatic mass lesion as well multiple abdominal lymph nodes and multiple skeletal sites. All the lesions were FDG concentrating on 18F-FDG PET-CT scan. The patient was treated subsequently with five cycles of PRRT with 177-Lu DOTATATE (with a cumulative dose of 781 mCi). After five cycles there was excellent symptomatic improvement and she was better than her prefirst cycle status (at 24 months after first cycle PRRT). On SSTR imaging, after five cycles, 68Ga-DOTATATE PET-CT scan shows reduction in the pancreatic mass but increase in the number of skeletal lesions as well as development of a breast metastasis. Although the aforementioned outcome was commensurate with the FDG-avid primary, interestingly, on 18F-FDG PET-CT scan there was metabolic response of the skeletal lesions and abdominal lymph nodes and decrease in the metabolic intensity of the pancreatic lesion scan. The patient's tumor marker has remained almost stable over the period (serum CgA from 387.5 to 362 ng/mL). The patient is being followed up for the outcome. Color image available online at
Combining Clinical Genetics and Biomarker Proteomics with Molecular Imaging or Targeted Chemotherapy
Currently there has been no definitive guidelines in correlating genetic background of the tumor or expression of clinically relevant proteins with molecular imaging and chemotherapy; however, it could be hypothesized that this approach will be useful in overcoming the individual shortcomings and thus would aid in a more scientific clinical approach. 64,65 To our knowledge, there is no convincing data that examined the use of the combination approach in clinical oncology in a systematic way.
A feasible clinical decision-making workflow pattern by integrating the in vitro biomarkers and the in vivo molecular imaging in management of advanced inoperable NETs has been illustrated in Figure 1. The knowledge of somatic mutations in the tumor tissue (e.g., somatic mutations associated with well-differentiated subtype as in genes MEN1, DAXX, or ATRX versus those occurring in the setting of poorly differentiated NECs such as TP53, Bcl-2, or RB1) and complementing the information with dual tracer-based PET imaging of SSTR and glucose metabolism would aid in better risk stratification of patients. When chemotherapy has been decided for a particular individual, the choice of the agent could be decided further by exploring the aberrant expression of proteins that could serve as indicators of altered pathways and would be potentially useful for selecting the appropriate chemotherapeutic agent. The relative amount of key inhibitors of the Akt/mTOR pathway (e.g., reduced TSC2, PTEN, PIK3CA, or enhanced SRC) would prompt for employing mTOR pathway inhibitors like everolimus, whereas elevated expression of tyrosine kinase receptors (c-KIT, PDGFRs, and VEGFR) would justify for tyrosine kinase inhibitors (e.g., sunitinib). NETs with low expression of MGMT are suitable for temozolomide therapy, whereas those with high expression are associated with temozolomide resistance. Similarly, tumors with low expression of SMAD2/SMAD4 are associated with resistance to capecitabine and 5FU, whereas normal expression of the same predicts response to these agents, making them preferred in this group of patients.
As observed from the aforementioned discourse, both of these powerful approaches have aided in management personalization in a varying way: although molecular imaging has aided in furthering the global disease biology by the dual tracer characterization, the clinical genetics or proteomics would complement by selecting the appropriate treatment and deciding whether a particular treatment approach could be efficacious. For example, PRRT would be a treatment of choice for patients with SSTR2 expressing tumors and its success would depend on the extent of SSTR2 expression. In case of targeted chemotherapy, patients with tumors that harbor loss of expression mutation in mTOR pathway genes NF-1, TSC2, PTEN, or PIK3CA would benefit from mTOR pathway inhibitors such as everolimus. Patients with activating mutations in receptor tyrosine kinases (c-KIT, PDGFRs, and VEGFRs) would respond to tyrosine kinase inhibitors such as sunitinib. Patients with loss of expression mutation in MGMT would respond to temozolomide, whereas those who overexpress MGMT would be intrinsically resistant to it. SMAD4 deficiency induced MMP9-mediated migration of cancer cells, higher GLUT1 expression, and resistance to capecitabine or 5′-fluoruracil-mediated apoptosis. 66 In terms of prognosis, reduced expression of tumor suppressors or overexpression of SSTR2 leads to better prognosis, whereas loss of expression of tumor suppressors, overexpression of GLUT, and other receptor tyrosine kinases are predictive of poor prognosis and lower survival. We believe that through well-designed studies, the concept of integrated approach would be examined in the future in several malignancies for improving the overall management.
Conclusions: Achieving the Best Result Through a Combined Approach?
Thus, one can envision the amalgamation of these two apparently different but potentially powerful methodologies (in vivo molecular imaging or “Radiomics” and the genomic–proteomic map) for the achievement of best results in developing a personalized management model in NETs and potentially in multiple malignancies in the future. Employing them together would be complementary and thereby lead to a scientifically and practically sound personalized clinical approach in cancer management.
Footnotes
Disclosure Statement
No competing financial interests exist.