
Abstract
Aim:
The prostate-specific membrane antigen (PSMA) is a cell surface protein, which is overexpressed in nearly all cases of prostate cancer (PCa). PET imaging with 68Ga-PSMA-HBED-CC has recently found widespread application in the diagnosis of recurrent PCa. In this study, the diagnostic potential of 64Cu-labeled PSMA ligand (PSMA-617) PET in patients with PCa has been investigated.
Materials and Methods:
The study was conducted simultaneously at two nuclear medicine centers, Austria (Vienna, Center 1) and Germany (Bad Berka, Center 2). The patients (n = 29) included in this study were referred for PET (Center 1, 21 patients) or PET/CT (Center 2, 8 patients) imaging with either a high suspicion of recurrent disease or for possible surgical or PSMA radioligand therapy planning. PET images of the whole body were performed at 1 hour p.i. and additional images of the pelvis at 2 hours p.i.
Results:
In 23 of 29 patients, at least one focus of pathological tracer uptake suspicious for primary disease in the prostate lobe or recurrent disease was detected. Among healthy organs, the salivary glands, kidneys, and liver showed the highest radiotracer uptake. Lesions suspicious for PCa were detected with excellent contrast as early as 1 hour p.i. with high detection rates even at low prostate-specific antigen (PSA) levels.
Conclusion:
The preliminary results of this study demonstrate the high potential of 64Cu-PSMA ligand PET/CT imaging in patients with recurrent disease and in the primary staging of selected patients with progressive local disease. The acquired PET images showed an excellent resolution of the detected lesions with very high lesion-to- background contrast. Furthermore, the long half-life of 64Cu allows distribution of the tracer to clinical PET centers that lack radiochemistry facilities for the preparation of 68Ga-PSMA ligand (satellite concept).
Introduction
Prostate cancer (PCa) is considered the most frequent tumor in men worldwide, resulting in significant morbidity and mortality. 1 The treatment of prostate carcinoma is impeded by the late clinical manifestation of the tumor and its early metastatic spread, which is revealed by metastases of the skeleton and lymphatic glands. 2 Particularly in younger men with benign prostatic hyperplasia (BPH), PCa is often diagnosed late and associated with symptomatic skeletal metastases, which can lead to sacroiliac pain, implying that sacroiliac or sciatic pain in men above 45 years of age should be considered for clinical assessment of the prostate gland in the absence of other etiological factors. 2,3 The determination of serum PSA is a standard procedure for screening and early detection of prostate carcinoma, but previous studies have demonstrated its suboptimal diagnostic value. 3 –5 Despite local therapy, such as radical prostatectomy (RP) and radiotherapy, up to 30% of patients eventually experience disease recurrence based on PSA measurements. 6 In these patients, localization of the site of cancer recurrence and of the extent of metastatic disease may allow individualized therapy associated with less side-effects and potentially higher survival rates.
Therefore, improvements in the early detection of prostate adenocarcinoma by methods that complement PSA determination are a subject of research. 2 Although choline-based PET/CT has been widely used for this purpose, numerous clinical studies have reported the low sensitivity and specificity of this technique, especially at low PSA levels and high Gleason score. In addition, 11C- or 18F-Choline is flow limited and higher uptake may be present in BPH. 6 11C- or 18F-Choline PET/CT has good specificity for detecting lymph node metastases, but has low sensitivity, ranging from 10% to 73%. 7 In a prospective study, Poulsen et al. demonstrated in 210 patients that 18F-Choline PET/CT is not sensitive enough when compared with lymph node dissection (LND), and therefore cannot replace this invasive procedure. 8 Further studies demonstrated that disease detection rate using 18F-Choline PET/CT was related to serum PSA levels, showing values of 20%, 44%, and 81.8% for PSA levels of ≤1.1, PSA ≤5, and PSA >5 ng/mL, respectively. 8,9 However, Chondrogiannis et al. underlined the high detection rate of 18F-Choline PET/CT (80%, 37/46 patients) proportional to serum PSA and not influenced by androgen deprivation therapy. 10
The gold standard for N staging of PCa is LND. In patients with biochemical recurrence (BR) after RP, salvage LND can be considered as a treatment option. Contemporary imaging techniques, such as 11C-/18F-Choline PET and diffusion weighted magnet resonance imaging (DW-MRI), appear to enhance the accuracy in identifying lymph node (LN) relapse in patients with BR after RP. However, for staging of patients with primary PCa, lymph node size should not solely be used as a surrogate for the presence of lymph node metastases. Unfortunately, CT or MRI cannot detect microscopic lymph node invasion, because detection rates are typically <1% in patients with a Gleason score <8, PSA <20 ng/mL, or clinically localized disease. 11
The prostate-specific membrane antigen (PSMA) has recently gained increasing attention because of its significant overexpression in PCa cells and restricted expression in normal tissue. 12,13 Thus, PSMA is a highly attractive target for the diagnosis of metastatic disease 14 and subsequent therapeutic application following the concept of theranostics. 15 –17
The introduction of PET imaging with 68Ga-labeled urea-based PSMA ligands was a significant step forward in the diagnosis of recurrent PCa, as the outstanding feature is the detection of lesions even at very low PSA values (<0.2 ng/mL), which can significantly influence further clinical management. 18,19 However, because of the short half-life, the application of 68Ga-PSMA is limited to PET centers with radiochemistry facility. In this regard, it would be of interest to use a PET radionuclide with a longer half-life. 64Cu is an excellent candidate as it decays with a half-life of 12.7 hours and emits positrons of favorably low energy (Eβ+ av = 278 keV) similar to 18F (Eβ−av = 250 keV). Therefore, the image resolution is expected to be increased as compared with 68Ga that emits positrons of a higher energy (Eβ+ av = 830 keV). 20
This study reports the first clinical use of the 64Cu-labeled ligand PSMA-617 for PET imaging 21 performed at two different centers in Austria and Germany.
Materials and Methods
Patient preparation
The present retrospective clinical study was conducted at two nuclear medicine centers, Wilhelminenspital, Vienna (Center 1) and Theranostics Center for Molecular Radiotherapy and Molecular Imaging (PET/CT), Zentralklinik Bad Berka (Center 2), respectively, between October 2014 and March 2015. The patients were referred for PET (Center 1, n = 21) or PET/CT (Center 2, n = 8) imaging before surgery or before PSMA radioligand therapy (PRLT) using 177Lu-labeled PSMA small molecules or with high suspicion of recurrent disease.
All PET and PET/CT examinations were performed in compliance with the German Medicinal Products Act (section 13, subsection 2b), the 1964 Declaration of Helsinki, and the responsible regulatory bodies in Austria and Germany. All patients received 64Cu-PSMA under the “compassionate use” clause of the German Medicinal Products Act. 18 The study was performed in accordance with the regulations of the Austrian and German Federal Agency for Radiation Protection.
Twenty-nine patients with a mean age of 71 years (age range 51–91 years) were included in this study. Inclusion criterion for PET or PET/CT imaging with 64Cu-PSMA-617 was either a progressive tumor at primary staging (4 patients at each center, n = 8) or a suspected tumor relapse with previously histologically proven PCa with BR after therapy with curative intent (17 in Center 1 and 4 in Center 2, n = 21). The average PSA value in patients with suspected recurrent disease was 7.3 in Center 1 and 57.9 ng/mL in Center 2 (range 0.3–44 ng/mL in Center 1 and 0.02–222.6 ng/mL in Center 2). Table 1 represents the characteristics of the patients included in this study.
PSA, prostate-specific antigen.
Synthesis of 64Cu-PSMA-617 (ACOM, Italy)
For each patient dose, 25 μg PSMA-617 (DOTA [1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid] as chelating agent, ABX) dissolved in 50 μL acetate buffer was adjusted to pH 5.5 (sterile filtration Millipore, Millex-GV, Art.: SLGV 013SL). Metal ions were removed with Chelex (Suprapur®, Merck Art. 1062640050). This precursor solution was then radiolabeled with 370 MBq Cuprymina® (64CuCl2, 925 MBq/mL radiopharmaceutical precursor solution, EU/1/12/784/001 Sparkle s.r.l.), which had been added to 400 μL acetate buffer. Incubation time was 15 minutes at room temperature and final pH was adjusted to 4–5.5. Radiolabeled product was obtained in high yield (>95%) and radiochemical purity (99.15%) determined by radio thin-layer chromatography (radio-TLC).
Imaging
At Center 1, a mean of 250 MBq (4 MBq per kg bodyweight, range 230–290 MBq) of 64Cu-PSMA-617 was administered intravenously. Whole body PET images (Siemens Medical Solutions AG, Erlangen, Germany) were performed 1 hour p.i. and additional images of the pelvis were obtained 2 hours p.i.
Additional images were acquired for dosimetric calculations in Center 1 in 3 patients at 24 hours p.i. For this purpose, volumes of interest (VOIs) were drawn over the organs with high physiological uptake using an HERMES workstation (HERMES Medical Solutions, Stockholm). These organs included liver, spleen, kidneys, and the salivary glands. The total body absorbed dose was calculated for all 3 patients, and the tumor dose was calculated for 1 of these patients.
At Center 2, a mean of 259.8 MBq (range 89–353 MBq; 1 MBq/kg in 2/8, and 4 MBq/kg in 6/8 patients per body weight) of 64Cu-PSMA-617 (ACOM, Italy) was administered intravenously. Low radioactivity was administered in the first 2 patients to monitor the safety of 64Cu-PSMA-617, followed by higher radioactivity in the other patients to obtain optimal image quality, particularly at later time points of image acquisition. Radionuclide purity was >99.5%, and radiochemical purity (TLC) was >95%. PET/CT imaging (Biograph mCT Flow 64; Siemens Medical Solutions AG, Erlangen, Germany) was performed from 90 minutes up to 17.5 hours p.i. of 64Cu-PSMA. All patients received 20 mg of furosemide i.v. to accelerate renal tracer excretion. Spiral contrast-enhanced CT was acquired after intravenous administration of 60–100 mL nonionic iodinated contrast. Imaging/reconstruction parameters were 120 kV, 160 mA, gantry rotation time 0.3 seconds, slice thickness 0.4 mm with increment of 0.1–10 mm, 40 images/second, and 512 × 512 matrix. PET imaging was acquired from the skull vault through to the feet in three-dimensional (3D) flow motion. Reconstruction matrix was 400 × 400 (Hi-REZ processing), achieving an axial resolution of 4.4 mm. Maximum standardized uptake values (SUVmax) were obtained by drawing circular regions of interest, which were automatically adapted (40% isocontour) to a 3D VOI using commercial software provided by the vendor. The subsequent images were reconstructed using the ordered subset expectation–maximization reconstruction algorithm. The PET and PET/CT studies were analyzed independently by two nuclear medicine physicians with more than 10 years of experience. There were no adverse effects or clinically detectable pharmacological effects in any of the patients after injection of the 64Cu-PSMA-617.
Results
Image analysis and quantification of the activity
Center 1
In 5 of 21 patients (n = 5, 24%), tracer accumulation was observed in the prostate bed, which was confirmed as local recurrence by histology; the fifth case was a suspected local recurrence with bone metastases. Twelve of the remaining 16 patients demonstrated focal tracer uptake in lymph node (n = 9) metastases (Fig. 1) or in the skeleton (n = 5) (Fig. 2 and Table 2A). As shown in Figure 1, there was high uptake in the metastatic lesions (SUVmax of the positive left iliac lymph node was 7.6 at 1 hour p.i., increasing to 13.4 at 2 hours p.i.), with low background activity (e.g., SUVmax in the left gluteal region was 1.07 and 1.17 at 1 and 2 hours p.i., respectively). In 1 patient, very faint focal uptake was noted in the lung, which was considered to be a nonspecific inflammatory process, and in another case mild uptake in a rib was attributed to an old rib fracture. Both lesions were not appreciable on late images and were not interpreted as metastases. No further parenchymal organ manifestations were observed.
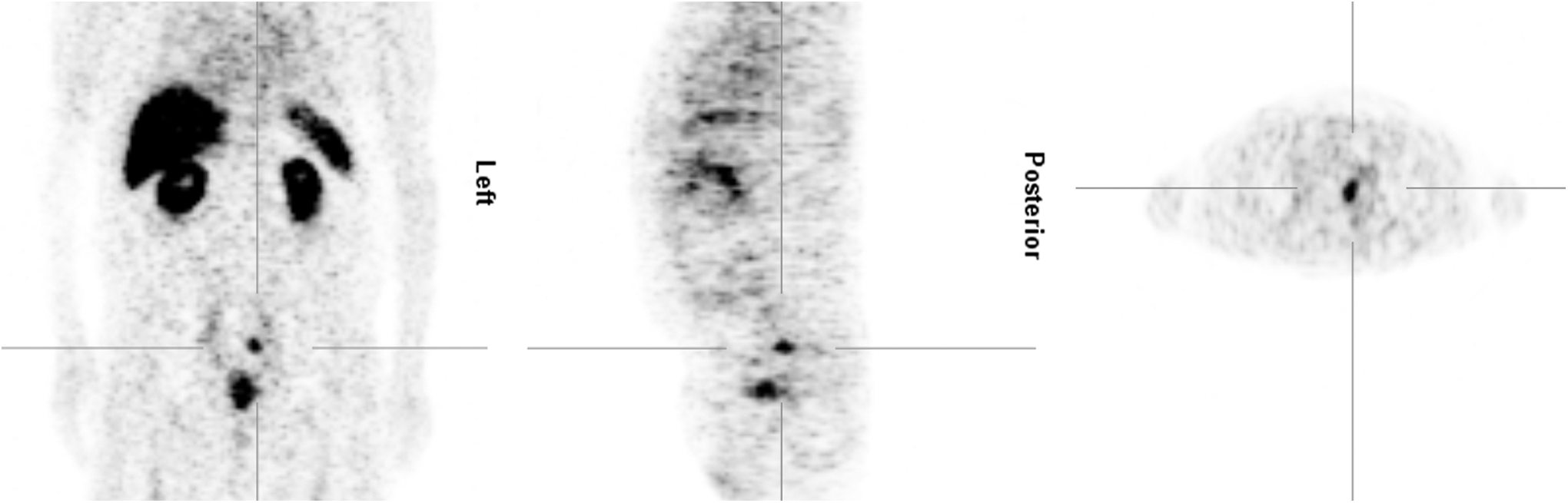
Center 1: male, 75 years, left iliacal lymph node metastasis.

Center 1: male, 70 years, bone metastasis in the right femur.
NA, not applicable.
Center 2
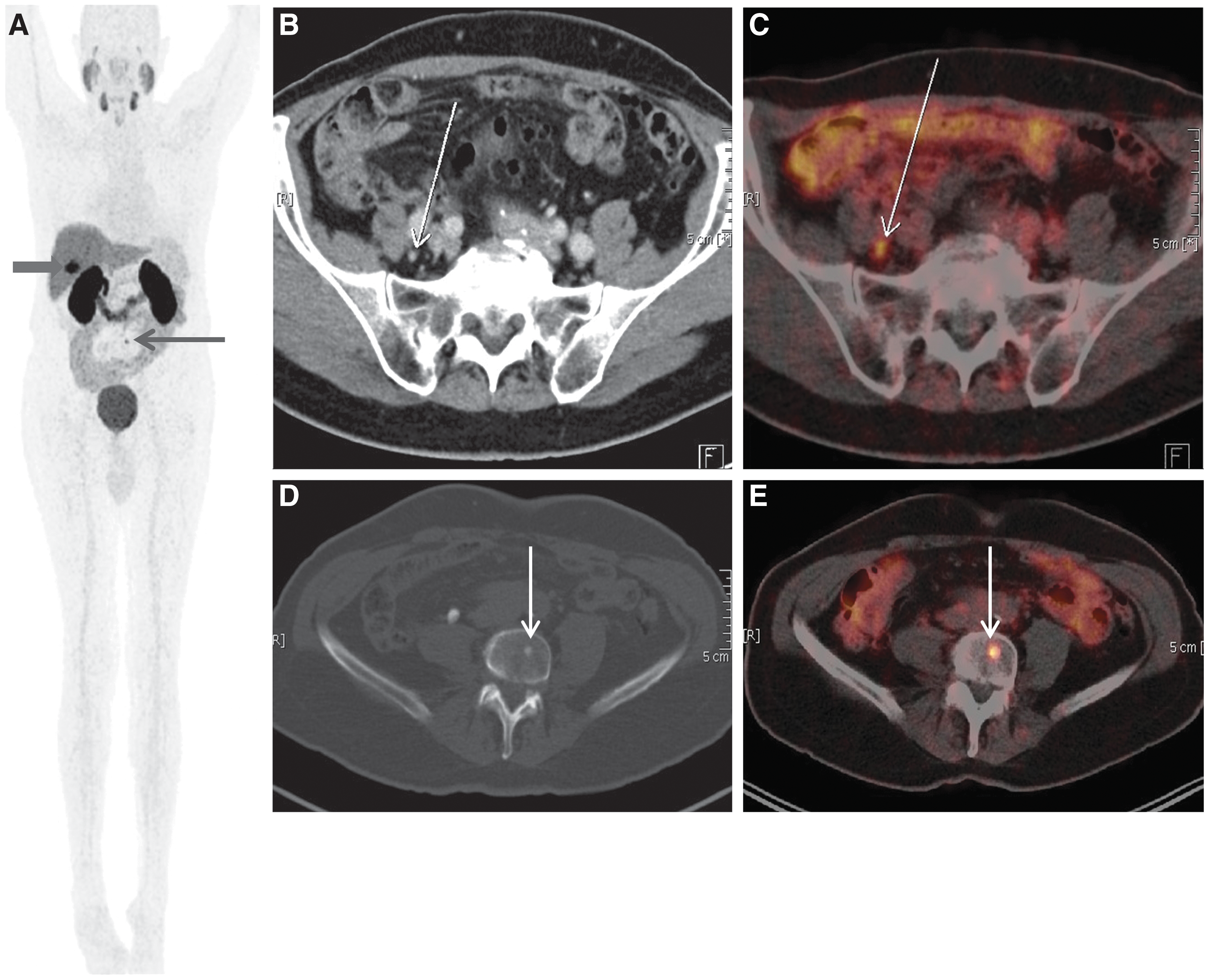
Overall, 6 out of 8 (75%) patients demonstrated high focal uptake of 64Cu-PSMA on PET/CT images. Two (25%) out of 8 patients showed uptake in the prostate bed, suggestive of local recurrent disease, in 1 patient after RP more than 8 years ago, whereas the other patient had residual tumor after brachytherapy about 9 months ago. Four (50%) patients exhibited tracer uptake in lymph nodes metastases, of which 2 patients had a significant increase in the extent of the disease when compared with previous 18F-Choline PET/CT studies (Fig. 3); a complete match was found with a previous 68Ga-PSMA PET/CT study in 1 patient and corresponding well to CT (Fig. 4) in another patient (Table 2B).
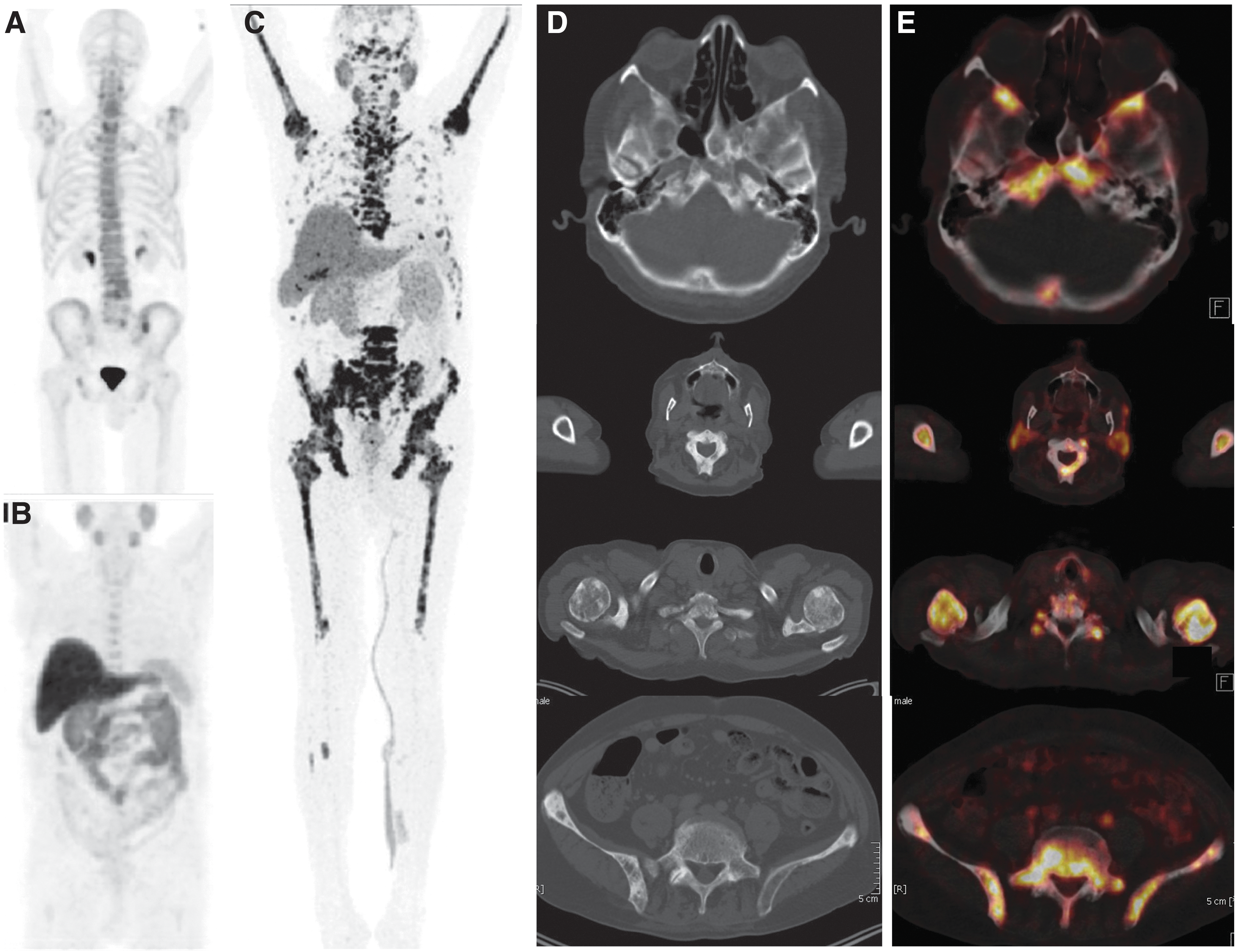

64Cu-PSMA PET/CT showed lymph node and skeletal metastases suggestive of progressive disease in comparison with previous 18F-Choline PET/CT from 2012 with solitary lymph node metastasis. 64Cu-PSMA PET/CT: MIP image
Skeletal metastases were detected in 4 out of 8 (50%) cases, which correlated with the findings on 68Ga-PSMA-11 PET/CT in 2 patients, and to CT findings in another patient, whereas in 1 patient, there was a significant increase in the extent of the disease when compared with previous PET/CT studies using 18F-Choline and 18F-Fluoride (Fig. 5). Two out of 8 patients, who presented for restaging with suspicion of recurrent disease, had no focal tracer uptake and no structural abnormalities on 64Cu-PSMA-617 PET/CT scans.
Implication on clinical management
Four (50%) patients were diagnosed with progressive disease (PD) according to Response Evaluation Criteria In Solid Tumors (RECIST) and PET Response Criteria in Solid Tumors (PERCIST) in Center 2 when compared with other imaging modalities or previous PET/CT imaging (68Ga-PSMA-11 PET/CT and/or 18F-Choline PET/CT). In 3 out of these 4 patients, a decision was made to commence PRLT because of disease progression after having exhausted all other therapy options, such as surgery, chemotherapy, radiation therapy, and hormone therapy; the fourth patient was restaged before the second PRLT cycle.
One patient demonstrated focal 64Cu-PSMA-617 uptake in the dorsal part of the left prostate lobe with PSA rising from 2.18 to 4.53 ng/mL, post high-dose rate (HDR) brachytherapy and laparoscopic lymphadenectomy; another patient with a PSA of 2.88 ng/mL exhibited 64Cu-PSMA-617 uptake in L4 vertebra and in a pelvic lymph node after previous prostatectomy and regional lymphadenectomy. These patients were recommended for follow-up with 68Ga-PSMA-11 PET/CT at the discretion of the referring urologist.
Dosimetry
The cumulated activity (
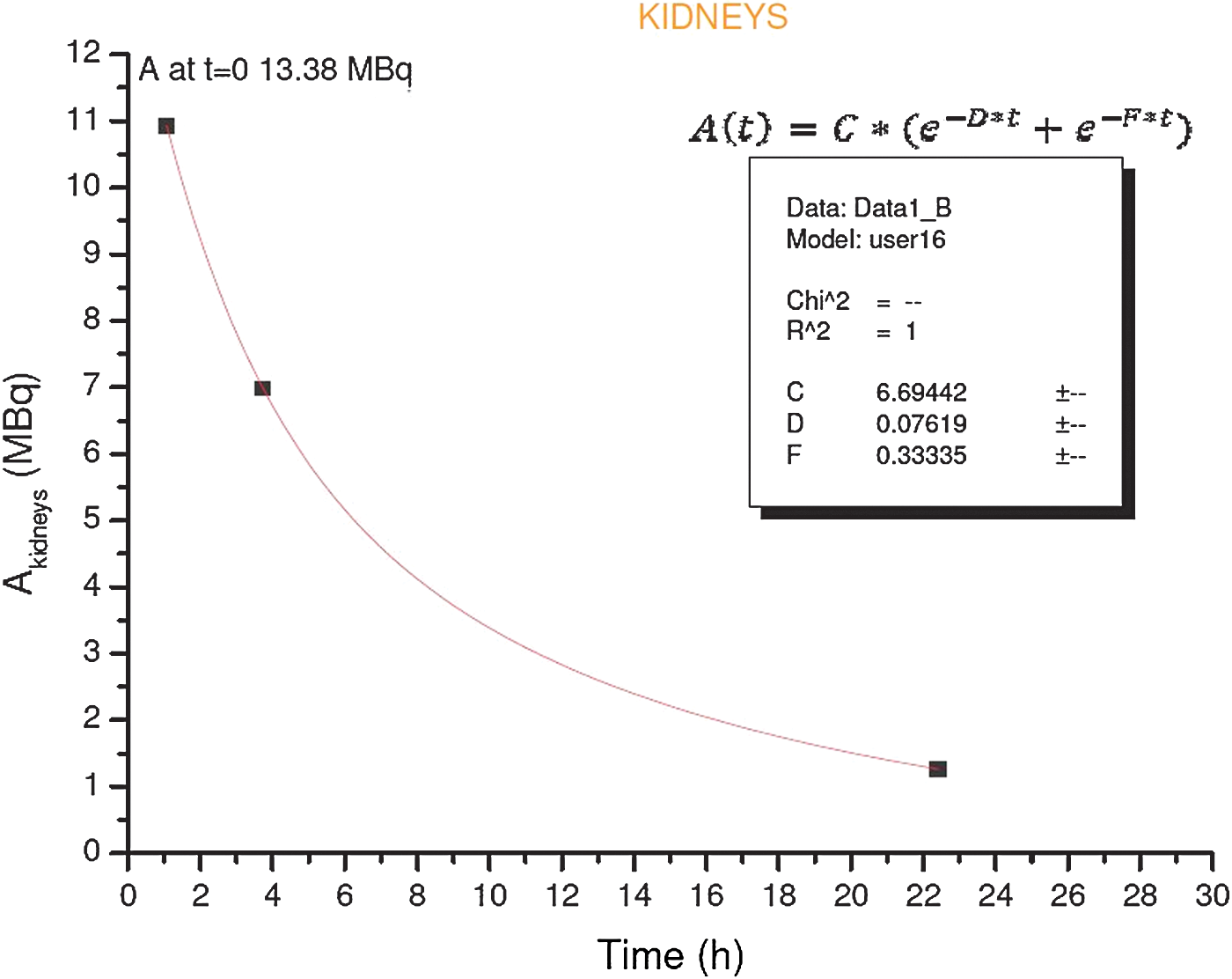
Relative time–activity curves for kidneys obtained from the activities measured by the three PET scans. The salivary glands (only for 2 patients) have only two measurement points because the first scan did not includethe neck. Color image available online at
where
For each organ, we also calculated the residence time (
where A o is the administered activity.
The organ dose was calculated according to the MIRD schema
22
by multiplying the cumulated activity by the
The cumulated activity of total body (
where
where
The dose to total body is then given by
The dose to total body per unit of activity administered average of the 3 patients was equal to 0.014 mGy/MBq, whereas T1/2 Eff was 7.8 hours (T1/2 Biol = 20.2 hours) (Table 3).
There is also the effective dose per unit of activity administered, and in 1 patient the tumor dose per unit of activity administered. (Owing to head movement of patient 1, his salivary glands were excluded from dosimetry.)
In 1 patient, the dose to a tumor volume of 98 cc was calculated, and the cumulative activity was achieved with a biexponential fit on the three activities related to the corresponding PET scans (Fig. 7), whereas the S factor for the tumor was calculated using the spheres for 64Cu of the OLINDA/EXM software:

Relative time–activity curve for tumor obtained from the activities measured by the three PET scans only for a patient.
where
These factors were also used to calculate the dose absorbed by the salivary glands as OLINDA/EXM has not tabulated S factors for this organ.
The effective dose was calculated using the coefficients of radiosensitivity of the organs with distinctively higher uptake (liver, kidneys, spleen, and salivary glands). 24
Discussion
All cases with histologically proven local disease were clearly identified by 64Cu-PSMA-617 PET. In 2 patients, suspected lymph node metastases on PET were either confirmed on the corresponding MRI images or observed in three cases on previous PET imaging with different radiopharmaceuticals (Table 2A and B).
PSMA ligands have the potential to have a high impact on the management of patients with PCa. 25 PET imaging with 68Ga-PSMA-HBED-CC demonstrated great promise for detection of small PCa lesions. PSMA ligands also showed great promise for targeted radionuclide therapy because of high expression of PSMA in tumor tissue and low uptake in normal tissue. 12 A retrospective analysis of 319 patients, who underwent 68Ga-PSMA PET/CT from 2011 to 2014, demonstrated a high sensitivity (82.2%) for identifying patients with suspected cancer. 18 In another study in 248 patients with BR after RP, 68Ga-PSMA PET/CT revealed a high number of true positive findings in the clinically important range of low serum PSA values (<0.5 ng/mL), which in many cases leads to a change in clinical management. 14 A comparative study performed in 37 patients for the detection of recurrent PCa showed that 68Ga-PSMA PET/CT can detect metastatic lesions with improved contrast when compared with 18F-Choline PET/CT, especially at low PSA levels. SUVmax was clearly (>10%) higher in 62 of 78 lesions (79.1%) and the tumor-to-background ratio was clearly (>10%) higher in 74 of 78 lesions (94.9%) when compared with 18F-Choline PET/CT. 26
However, because of the short half-life of 68Ga, its application is limited to clinical PET centers with radiochemistry facility and a 68Ga generator available on site. Images obtained with 64Cu-PSMA-617 show a high lesion contrast with a reasonable effective dose as shown in this study. Radionuclides with a longer half-life such as 64Cu (T1/2 = 12.7 hours) allow distribution of the radiolabeled PSMA ligand to PET centers that lack radiochemistry facilities and 68Ga generators (satellite concept). To the best of our knowledge, this is the first in-human study of a urea-based PSMA ligand labeled with 64Cu, which showed great promise for the detection of primary PCa, relapse, and PD. Metastases were most frequently detected in pelvic lymph nodes and in the skeleton.
Conclusion
This study reports the first in-human application of a urea-based PSMA ligand labeled with 64Cu, combining the advantage of a small PSMA-targeting agent and of a longer lived positron emitter with good image quality, resulting in high image contrast. The results of this study ascribe high significance to PET imaging with 64Cu-PSMA-617 in the primary staging of selected patients and in patients with recurrent disease, especially in centers where 68Ga-PSMA ligands are not available. Following the concept of theranostics, 64Cu-PSMA can also be used to select patients for 177Lu PRLT, offering in future also the possibility to perform pretherapeutic dosimetry in the sense of a patient-specific and personalized targeted treatment approach.
Footnotes
Acknowledgments
We are grateful to Dr. Cristina Müller, Center for Radiopharmaceutical Sciences ETH-PSI-USZ, Paul Scherrer Institute, Villigen-PSI (Switzerland), for critically reading the article and useful comments.
The costs of the publication for the color figures were defrayed by DSD Pharma and ACOM SRL.
Disclosure Statement
No competing financial interests exist.