
Abstract
The aim of this work was to evaluate the sensitivity of time-integrated activity coefficients (TIACs) on the erroneously chosen prior knowledge in a physiologically based pharmacokinetic (PBPK) model used for treatment planning in peptide receptor radionuclide therapy (PRRT). Parameters of the PBPK model were fitted to the biokinetic data of 15 patients after the injection of 111In-DTPAOC. The fittings were performed using fixed parameter values taken from literature as prior knowledge (reference case, Ref). The fixed parameters were gender, physical information (e.g., body weight), dissociation rate koff , dissociation constant KD , fraction of blood flow, and spleen and liver volumes. The fittings were repeated with changed fixed parameters (Changed). The relative deviations (RDs) of TIACs calculated from Changed and Ref were analyzed for kidneys, tumor, liver, spleen, remainder, whole body, and serum. A changed koff has the largest effect on RD, the largest RD values were found for changed koff = 0.001 L/min: RDkidneys = (3 ± 3)%, RDtumor = (0.5 ± 4)%, RDliver = (6 ± 9)%, RDspleen = (5 ± 5)%, RDremainder = (2 ± 31)%, RDserum = (−4 ± 25)%, and RDwholebody = (3 ± 16)%. For other changed parameters, the maximum RDs were <1%. The calculation of organ TIACs in PRRT using the PBPK model was little affected by assigning wrong prior knowledge to the evaluated patients. The calculation of bone marrow-absorbed doses could be affected by the inaccurate TIACs of serum and remainder in the case of an inadequate koff .
Introduction
The aim of treatment planning in peptide receptor radionuclide therapy (PRRT) is to determine the administered activity that is high enough to kill cancer cells and low enough to ensure the safety of organs at risk. 1,2 Patient-based treatment planning in PRRT has been shown to have better accuracy than cohort-based treatment planning. 2,3 In patient-based treatment planning, the individual biokinetics (determined from quantitative imaging, e.g., planar scintigraphy) of the patient is used to calculate the activity to administer. 4,5
Physiologically based pharmacokinetic (PBPK) modeling is a powerful tool to fit and simulate biokinetics in the human or animal during PRRT and radioimmunotherapy. 6 –8 Knowledge about the values of physiological parameters of the patient and also the characteristics of the labeled substance are included in the PBPK model as prior knowledge.
This prior knowledge about the model parameter determination could be important to ensure the accuracy of treatment planning when using a PBPK model. Currently, a set of individual prior knowledge parameters, which were taken from the literature or determined individually for the patients, are used as fixed PBPK model parameters in each patient. 3,9 The erroneously chosen prior knowledge could affect the calculation of the time-integrated activity coefficients (TIACs), which in turn is used to calculate the predicted absorbed dose for treatment planning in PRRT. 2,4 Therefore, an investigation of the sensitivity of the TIAC values on the possibly erroneously fixed prior knowledge (i.e., used values of fixed parameters of a PBPK model) is needed.
The aim of this study was therefore to investigate the sensitivity of the TIAC values to erroneously chosen fixed parameters of the PBPK model representing the used prior knowledge. This investigation is conducted for treatment planning with the example of 111In-DTPAOC (Octreoscan) based on planar scintigraphy data.
Methods
Patients and measurements
In this study, biokinetic data of 15 patients with proven metastasized neuroendocrine tumors (NETs) scheduled for four cycles of PRRT using 90Y-DOTATOC were involved (Fig. 1A). Note that the same patients were used as in the previous study. 3 In the pretherapeutic stage, 111In-DTPAOC with the mean activity of (152 ± 15) MBq (total peptide amount [5.78 ± 0.25] nmol) was injected intravenously as a bolus to all patients. Five planar whole-body scintigraphy data (ECAM-Siemens) were obtained at 45 minutes, 4 hours, 1, 2, and 3 or 5 days postinjection. The scatter, background, and attenuation corrections were performed as described elsewhere 9 according to MIRD pamphlet 16 in Ref. 10 for conjugate view counting. Whole-body activity data and the organ activity data of kidneys, tumor, liver, and spleen were determined using the ULMDOS software 11 by drawing the regions of interest in the planar scintigraphy data manually by the physicians. The ROIs were placed in an area without overlap with other organs and scaled to the calculated organ size.
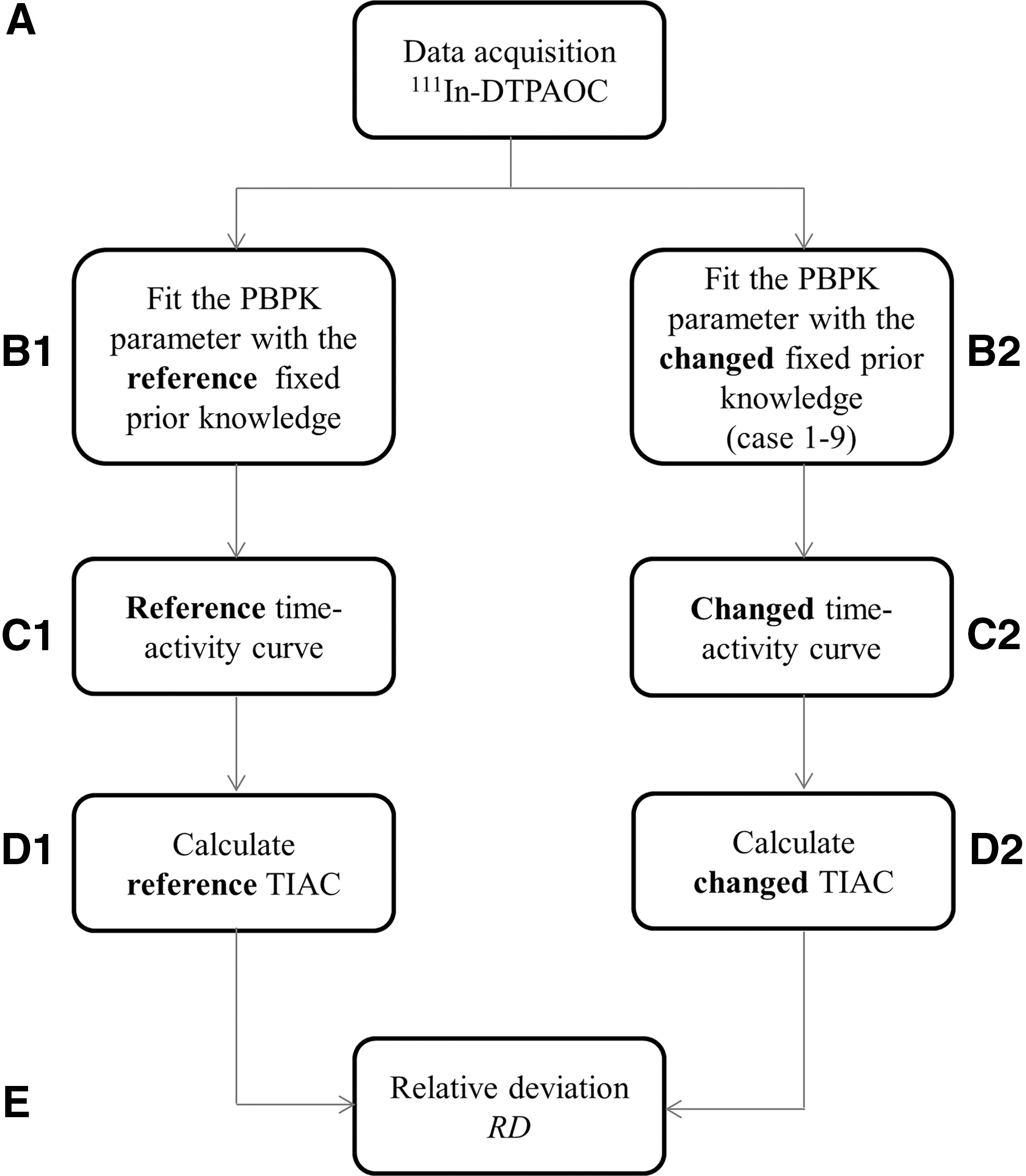
Flowchart of the investigation for the fitting using reference and changed prior knowledge. For more detailed description, please see Patients and measurements; PBPK model; Definition of reference TIAC values; Measurement of TIAC sensitivity; and Relative deviation of the TIAC sections and Tables 1 and 2. PBPK, physiologically based pharmacokinetic.
Blood serum samples were drawn at eight different times after injection: 5 minutes, 0.5, 1, 2, 4 hours, and 1, 2, 3 or 5 days.
PBPK model
A PBPK model for PRRT 9 was used and implemented in the software simulation analysis and modeling software II (SAAMII v. 2.2; The Epsilon Group). 12 The main organs, which highly express somatostatin receptor type 2 (sst2) sites, were modeled, that is, tumor, kidney, liver, spleen, and the remainder as suggested in literature. 9 Blood was modeled as the central vascular compartment; the injection of the peptides is performed in the central vascular compartment, then distributed through blood flow and transported to the interstitial spaces of the organs. Model A in Ref. 9 for the kidneys was used, which was found to be the best model as it implements specific and unspecific uptake. The model consists of two equal systems of labeled and unlabeled peptides, which are connected by the competition of same receptors and by physical decay.
The blood flow to the organs was individually fixed as demonstrated in the literature 9 (Table 1). As the tumor perfusion fTU could differ significantly between patients, this parameter was fitted to the patient biokinetic data. The affinity parameters, that is, the dissociation rate koff and the dissociation constant KD , were fixed to the reported values (Table 1).
Hematocrit (dimensionless).
Body surface area (m2).
The estimation of parameter was constrained with the lower (10% of the starting value) and upper boundaries (1000% of the starting value).
The estimation of parameter was constrained with lower and upper boundaries plus additional constraint as Bayesian values (mean and the SD of the population).
BSA, body surface area; PBPK, physiologically based pharmacokinetic; SD, standard deviation.
The volume of the organs, that is, liver and spleen, and serum was calculated individually (Table 1). Volume of the kidneys was fixed at 0.31 L for males and 0.275 L for females. 13
Definition of reference TIAC values
The parameters of the PBPK model were fitted to the biokinetic data of the patients in the Patients and measurements section (Fig. 1, B1); these were blood samples, whole-body activity data, and the organ activity data of kidneys, tumor, liver, and spleen. The following computational settings were used: Rosenbrock algorithm, convergence criterion value of 10−4, central derivative, data-based variance model, and relative data weighting scheme. 3 Prior knowledge was used as fixed parameters, which were set according to literature. 9 The following types of fixed model parameters were implemented: global fixed parameters, for example, affinity parameters, and individual fixed parameters, for example, organ volumes and blood flow. Table 1 shows the setting of the fitting of some individual unknown parameters of the PBPK model.
Goodness of fit was tested by visual inspection of the fitted curves, 14 coefficients of variation, CVs, of the individual fitted parameters (CV <25% considered as plausible fit, CV <50% considered as acceptable fit as described in Ref., 15 chapter 15), the individual area under the curves (AUCs) of the organ time–activity curves, that is, kidneys, tumor, liver, spleen, whole body, and blood, and the elements of the correlation matrix ([−0.8;0.8] considered as an acceptable range for a good fit 14 ). The calculated TIAC (ratio of the AUC and the injected activity) from the time–activity curves were called reference TIAC (Fig. 1C1, D1).
Measurement of TIAC sensitivity
The parameters of the PBPK model were fitted to the biokinetic data of the patients in the Patients and measurements section with changed prior knowledge, that is, assumption of opposite gender, the changed affinity parameters, fraction of blood flow, and kidney, liver, and spleen volumes (Cases 1–9 in Table 2; Fig. 1B2) The computational setting, the fitted parameters, and the goodness of fit criteria were the same as written in the Definition of reference TIAC values section. The calculated TIACs called changed TIACs were used to estimate the sensitivity of the TIACs on the prior knowledge in the PBPK model (Fig. 1C2, D2). Note that only the values of the fixed parameters were changed for each case; the setting of other parameters remained the same. The same settings of fitted and Bayesian parameters were always used.
Note that for each case, all other parameters were unchanged and the same as written in Table 1.
Parameters are defined in Table 1.
Hematocrit.
A factor of 1.23 was calculated from the total blood flow (F = 6500 mL/min) and blood volume (Vp male = 5300 mL) of the average normal adult (blood) as demonstrated. 9
Mean value was calculated from the population.
BW, body weight; TIAC, time-integrated activity coefficient.
Gender, body weight, body surface area, and hematocrit
The knowledge of gender is included in the recently developed PBPK model 9 affecting the model parameters of volume of total body serum Vp , total flow in the plasma F, and total volume of the kidneys VtotK (Table 2). False genders are implemented in which all patients were assumed to be male or female or all patients were assumed to have a wrong gender (Table 2, Case 1). The effect of erroneously chosen physical information, that is, body weight (BW), body surface area (BSA), and hematocrit, using mean value was investigated in Case 2 (Table 2).
Organ volume
In the literature, 9 the equation model to calculate the total volume of the liver and spleen in the PBPK model was based on the publication of Johnson et al. (model 2a in Ref. 16 ) and Harris et al. 17 The equation model 2a used in the PBPK model for the total liver volume was only recommended for the human age up to 18 years. Equation model 3 (which is recommended in the literature for the human age beyond 18 years 16 ) was implemented in this study (Case 3).
The calculation of the total volume of the spleen can be performed using two models, which depend on the BW and the BSA according to Harris et al. 17 The current PBPK model is using the BSA value; the other model, which is based on BW, is implemented in this study for comparison (Case 4).
Additional analyses using the mean organ volume of liver and spleen for individual fitting were performed (Table 2, Cases 3–4). The mean organ volume was calculated from the population.
The affinity parameters of the labeled peptide
Dissociation rate koff and dissociation constant KD were used to describe the affinity parameters of the labeled peptide in the PBPK model. The used dissociation rate koff in the literature 9 for the PBPK model is based on the study of Ferl et al. 6 Dissociation rate koff was estimated from the fitting of the compartment model, which describes the binding and internalization of the peptide, to the biokinetic data of 20 mice after injection of 18.5 kBq of 64Cu-DOTA-RGD peptide. The estimated value of dissociation rate koff was (0.013 ± 0.06) L/min.
The used dissociation constant KD in the literature 9 for the PBPK model is based on the study of Edwards et al. 18 Measured dissociation constant KD for 111In-DTPAOC was (5.57 ± 0.95) nmol/L. Standard deviation (SD) was calculated from the percentage error of the measurement error, that is, 17%.
The inaccuracy of determination of affinity parameters is calculated based on the SD. 6,18 Six different levels of inaccuracy were implemented: +1SD, −1SD, +2SD, −2SD, +3SD, and −3SD for both the dissociation rate koff (Case 5) and the dissociation constant KD (Case 6). Note that because the dissociation rate koff cannot be negative, the inaccuracy of −3SD was not implemented in Case 5.
The fraction of blood flow
Mean values reported in the literature 19 of the fraction of the blood flow to the kidneys FK , liver FL , and spleen FS are used in the current PBPK model. The uncertainty of these parameters is represented by the reported lower and upper limits of the fraction. 19 Four different levels of uncertainty were implemented: 0.5 times the lower limit, lower limit, upper limit, and two times the upper limit for the fraction of blood flow to the kidneys FK (Case 7), liver FL (Case 8), and spleen FS (Case 9).
Relative deviation of the TIAC
To investigate the sensitivity of prior knowledge on the calculation of the TIACs, the relative deviation (RD) of the changed TIACs from Case 1 to 9 to the reference TIACs was calculated according to Equation (1) for the following organs: tumor, kidneys, liver, spleen, remainder, whole body, and serum (Fig. 1E). The maximum RD ≤10% is assumed as an acceptable accuracy to be used in further calculations of dosimetry.
Results
Goodness of fit using reference prior knowledge was acceptable based on visual inspection (e.g., Fig. 2A), the coefficients of variation of the fitted parameters and AUCs (<30%), and the elements of the correlation matrix (within −0.8 and 0.8 except for seven elements of 825 elements [55 elements in each patient]).

Goodness of fit using changed prior knowledge was acceptable based on visual inspection (e.g., Fig. 2B), the coefficients of variation of the fitted parameters and AUCs (<30%), and the elements of the correlation matrix (mostly within −0.8 and 0.8, the maximum total number of elements of the correlation matrix, which is outside of the acceptable range, were nine in eight patients for Case 2).
A change of the dissociation rate koff (Case 5) has the largest effect on the RD of the organ TIACs (Fig. 3) compared with the other investigated cases; the largest RD values were found for changed koff to mean − 2SD, that is, RDkidneys = (3 ± 3)%, RDtumor = (0.5 ± 4)%, RDliver = (6 ± 9)%, RDspleen = (5 ± 5)%, RDremainder = (2 ± 31)%, RDserum = (−4 ± 25)%, and RDwholebody = (3 ± 16)%. In all other cases, the maximum RDs of the changed TIACs were <1% except in Case 1 for plasma volume Vp RDserum = (−4 ± 8)%.
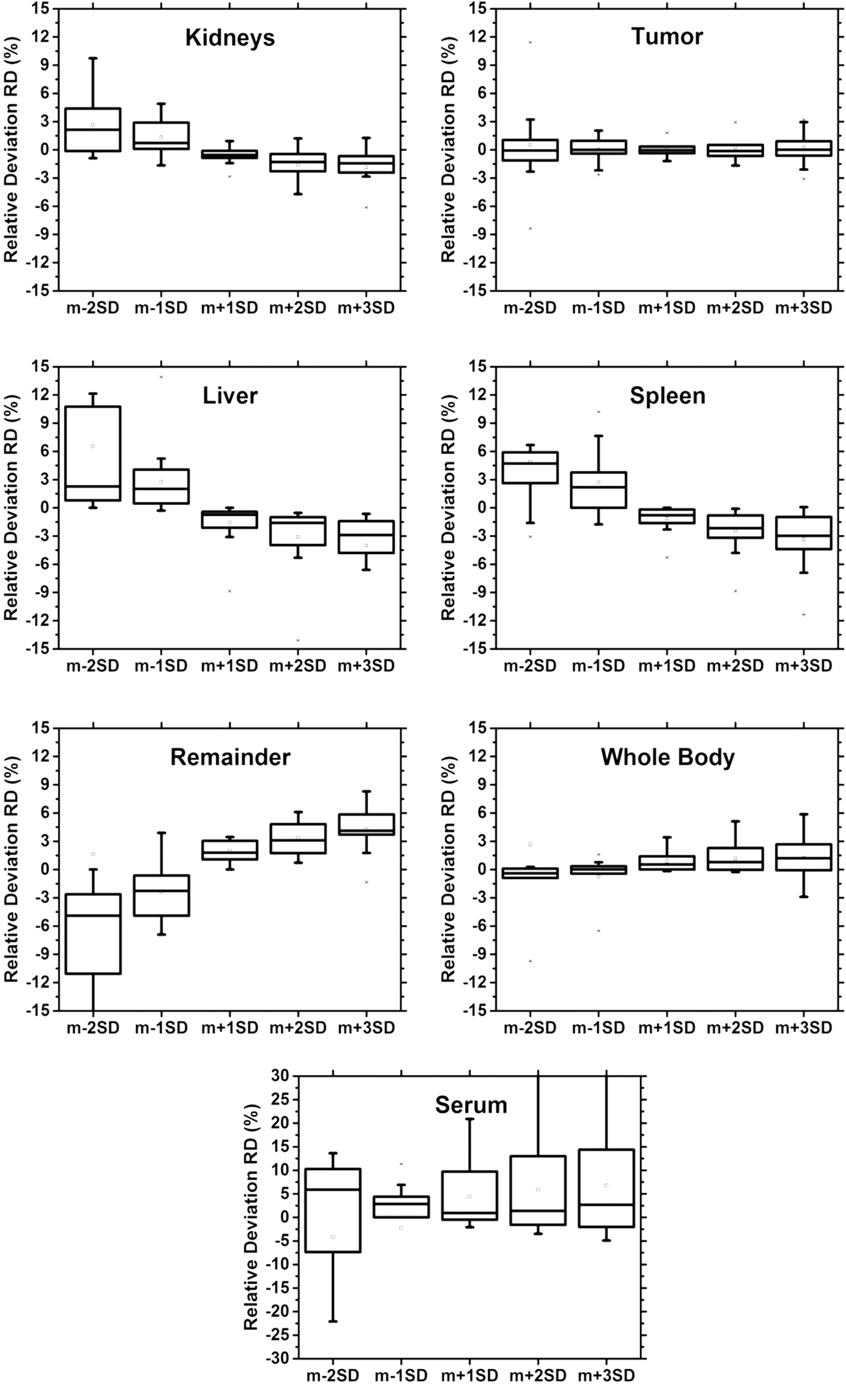
RD for different assigned values of the dissociation rate (Case 5, Table 2) for kidneys, tumor, liver, spleen, remainder, whole body, and serum. The value for mean − 3SD is not shown as it would correspond to a negative value of koff . The values outside of −15%–15% in serum and remainder are not shown. Note that a different scale is used for the serum. RD, relative deviation.
Discussion
PBPK modeling has shown to be a powerful method to analyze, fit, and simulate patient biodistribution in PRRT. 3,9 To ensure efficacy and safety of the treatment planning using a PBPK model, the used prior knowledge in the model could be important to be accurately determined. The calculation of the TIACs for subsequent dosimetric calculations could be affected by inadequate values of fixed parameters representing the used prior knowledge. The estimated TIAC in pretherapeutic measurements is important for accurate treatment planning. In this study, the effect of the chosen fixed parameters on the accuracy of TIACs when using a specific PBPK model 3,9 was investigated, for example, of 111In-DTPAOC.
The goodness of fit showed accurate fits 3 (as defined in the Patients and measurements section). Note that the fitting and the goodness of fit analysis using reference prior knowledge have already been performed previously, 3 therefore the fitting results, that is, the fitted parameters, are not shown.
The genders of the patients (Case 1) affect the calculation of the total volume of kidneys VtotK , 13 the total flow of the peptide in plasma F, 19 and the total volume of plasma Vp 20 (Table 2). Assumed wrong assignment of patient gender affecting VtotK and F led to a small RD (maximum RD <1%) for tumor, kidneys, liver, spleen, remainder, serum, and whole body. A similar result was obtained for a false calculation of total volume of plasma Vp except for RD in the serum (RDserum = (−4 ± 8)%). Assumptions of fully wrong assignment of the gender, that is, male considered being female and female considered being male, has marginally increased the RD value, that is, maximum RD <1% in all organs for the calculation of VtotK , F, and Vp (Table 2, Case 1) except for the serum (RDserum = [−8 ± 4]%) in Vp case. The large deviation of TIACs in the serum may be due to the fact that the affected parameters are basically related directly to the plasma kinetics. Another result showed that erroneously chosen hematocrit, BW, and BSA (Case 2), that is, using mean values for the individual fitting, lead to RD <1%.
Two different models for calculating the total volumes of the liver VtotL and spleen VtotS were investigated (Cases 3 and 4). From the obtained results, it can be concluded that a different equation model for the calculation of the organ volumes does not strongly affect the resulting TIACs (maximum RD <1%). This is due to a small difference of the obtained organ volumes calculated using different models. For example, the calculation of the spleen volume in a patient with BW 97 kg, BSA 2.71 m2, and age 75 years using the equation model of VtotS = BSA × 278 × age−0.36 gave a volume of 0.159 L, and using the other model of VtotS = BW × 6.47 × age−0.31 (Table 2), gave a volume of 0.165 L, which differs only by 3%. However, the use of an actual organ volume, for example, determined from a CT image, clearly should be preferred.
To investigate the effect of using wrong organ values for liver and spleen, the corresponding fixed parameters for individual fitting were fixed to mean organ volumes (Table 2). The obtained RD was <1% in all organs except for the RD in the serum for the case of wrong liver volume (mean value): in this case, the authors obtained RD = (−0.8 ± 4)%.
The dissociation rate koff is prior knowledge that has an important role for the binding of the radiolabeled peptide. Change of the koff value (Case 5) led to a large RD in the serum (Fig. 3, RD = [−4 ± 25]%). Nevertheless, RD of the TIAC in the organ at risk, that is, kidneys, 21 –23 and also RD in the tumor are acceptable (maximum RD <1%).
The tendencies of RD depending on the dissociation rate koff in the remainder are different compared to kidneys, tumor, liver, and spleen (Fig. 3). For smaller dissociation rates, peptides bind stronger to the receptors at the organ cell surface. Thus, the number of unbound peptides in the remainder is reduced. For larger dissociation rates, the number of unbound peptides is increased. However, the total effect of a changed dissociation rate koff on the whole body TIACs is more or less constant (Fig. 3).
Apart from the kidneys, it has been shown that bone marrow is also an organ with high risk in PRRT. 24 –27 The calculation of absorbed dose in the bone marrow can be performed based on the absorbed dose in whole body and serum. 28 Thus, the inaccuracy of dissociation rate koff and total volume of plasma Vp must be considered if the calculation of the absorbed dose in the bone marrow is performed based on the whole body and serum data.
The inaccuracy of the determination of the dissociation constant KD in Case 6 only marginally affects the calculation of the TIACs (maximum RD <1%).
The uncertainty due to an assumed wrong fraction of the blood flow to the kidneys (FK ) Case 7, flow to the spleen (FS) Case 8, and flow to the liver (FL ) Case 9 did not significantly affect the TIAC values (maximum RD <1%). Small RD showed that the fitted parameters could compensate the wrong assignment of prior knowledge for the calculation of TIACs.
Conclusion
Based on the investigated cases in the patient population, the authors conclude the following:
1. The inaccuracy in the used dissociation rate koff showed a large effect (maximum RD >10%) on the calculation of TIACs in serum and remainder, for example, koff = 0.001 L/min, RDremainder = (2 ± 31)%, RDserum = (−4 ± 25)%. This could become relevant if the calculation of the absorbed dose to bone marrow is based on the serum and remainder.
2. Differently chosen organ volume calculation, false gender, incorrect physical information, incorrect dissociation constant, and inaccuracy of flow parameter marginally affect the calculation of the organ TIAC in the tumor, kidneys, liver, spleen, and whole body.
Clearly, this is true only for 111In-DTPAOC and the investigated patient group. Therefore, additional sensitivity analyses must be performed using larger patient populations and for other radiopharmaceuticals.
Footnotes
Acknowledgments
The authors gratefully acknowledge grants by Direktorat Jendral Pendidikan Tinggi (Directorate General of Higher Education DIKTI of Ministry for Research, Technology and Higher Education, Republic Indonesia, Grant Number: 2644/E4.4/K/2013) for DH, grants by LPDP-Lembaga Pengelola Dana Pendidikan (Indonesia Endowment Fund for Education, Ministry of Finance, The Republic of Indonesia, Ref: s-61/LPDP.3/2014) for N.J.B., and Perspektivförderung Translationale Radiochemie und Radiopharmazie (Land Baden-Württemberg) for G.G. The authors also gratefully acknowledge the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) for support (GL 236/11-1 and KL 2742/2-1).
Disclosure Statement
No competing financial interests exist.