
Abstract
The authors aimed to assess the risk of recurrence in patients with nonsmall-cell lung cancer after surgery with no evidence of disease (NED) demonstrated on 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT). A total of 140 subjects with adenocarcinoma or squamous cell carcinoma of the lung were included in this study. Patients had FDG PET/CT scans within a year after surgery between January 2007 and December 2014. Patients with PET/CT scans with NED were included. Following an NED PET/CT scan, recurrence or metastasis was found in 14 patients (10.0%), and deaths in 4 (2.9%) during a median follow-up of 636 days. Although the rates of recurrence or metastasis were very low, the risk for recurrence continuously increased after 600 days up to 0.03%. The risk was higher in patients with positive margin at surgery, lymphovascular invasion, N2 stage, and TNM stage III/IV. In conclusion, according to the smoothed hazard functions, there was a very low risk of recurrence until 600 days after normal 18F-FDG PET scans. The risk was higher in patients with positive margin at surgery, lymphovascular invasion, N2 stage, and TNM stage III/IV.
Introduction
Lung cancer is the leading cause of cancer-related mortality, expected to account for 22.6% of all cancer-related deaths. 1 The 5-year survival rates were improved dramatically from 11.3% to 21.9% for the last two decades. 1 Approximately, 15% of patients are diagnosed with localized disease confined to the primary site, 22% with involvement of regional lymph nodes (LN), and 57% with distant metastatic disease. 2 Disease confined to the primary site or with regional LNs can be treated with surgery. However, 25% of patients with nonsmall-cell lung cancer (NSCLC) will have locoregional recurrence 5 years after surgery. 3 Computed tomography (CT) of the chest is recommended every 6 or 12 months after surgery. 4 Routine use of 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET)/CT in patients after surgery is not recommended, 4,5 in part, because benign conditions such as atelectasis, infection, and radiation fibrosis are difficult to differentiate from malignancy on PET/CT scans. 4
PET/CT has a major role in the initial workup of lung cancer. 4 Only a few studies have evaluated the role of PET/CT for surveillance or follow-up after surgery. During surveillance, 18F-FDG PET/CT identified recurrence in more than 40% of patients without pretest clinical suspicion for recurrent diseases. 6 Twenty-eight percent of patients experienced a change in treatment management after the fourth or subsequent follow-up PET/CT scan. 7 Although the current guidelines do not recommend the routine use of PET/CT after surgery, there might be a value of surveillance PET/CT in certain specific clinical settings. Therefore, it is not clear whether PET/CT should be used in the routine surveillance after surgery for NSCLC.
In this study, the authors assess the risk of recurrence in patients with NSCLC after surgery with no evidence of disease (NED) on their initial follow-up FDG PET/CT. To our knowledge, this is the first study evaluating the value of FDG PET/CT scans, which demonstrates NED after surgery.
Materials and Methods
Patient characteristics
A total of 1711 patients with adenocarcinoma (ADC) or squamous cell carcinoma (SCC) of the lung treated with surgery were initially evaluated and 140 were included in this study. All of the included patients had NED 18F-FDG PET/CT scans within 1 year after surgery between January 2007 and December 2014. Patients were excluded on the following criteria: (1) time interval between surgery and PET/CT scan of more than 1 year, (2) lung cancer other than ADC or SCC, (3) history of other malignancies, or (4) PET/CT scans showing evidence of disease within 1 year after surgery. The current study was approved by the institutional ethics committee.
18F-FDG PET/CT
According to the standard protocol at this institution, patients were administered 5.18 MBq/kg of 18F-FDG intravenously after fasting for at least 6 hours. All patients had a blood glucose level <140 mg/dL. PET/CT scans were started ∼60 min after injection using a Biograph 40 (Siemens, Knoxville, TN). The CT scan was obtained first for attenuation correction, and then, the emission scan was obtained from the skull base to the proximal thighs. PET images were reconstructed using an iterative algorithm (ordered-subset expectation maximization, iteration 3, subset 21) with image matrix size of 256 × 256.
Image analysis
18F-FDG PET/CT data sets were reviewed by two experienced nuclear physicians without prior knowledge of the clinical data. PET/CT scans without evidence of disease were defined as those with no abnormal FDG uptake or FDG uptake consistent with inflammatory changes related to surgery. Focal hypermetabolism in PET scans or the presence of a new pulmonary nodule, pleural mass in CT scans was interpreted as positive for recurrence during the follow-up. The disagreements were resolved by the consensus of the two readers.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation. The primary endpoint was the presence of recurrent or metastatic disease. Disease-free survival (DFS) was defined as the length of time between PET/CT scan and recurrent disease. Patients without an event were censored at last follow-up. Kaplan–Meier curves with log-rank test were generated to display survival probabilities. Multivariate analyses were performed by Cox proportional hazards regression model with variables of p-value less than 0.1 with stepwise method in univariate analysis. Smoothed hazard functions were used to estimate event rates depending on time. A p-value less than 0.05 was considered as statistically significant. Data were analyzed by Stata version 13.1 (StataCorp LP, College Station, TX) and MedCalc Statistical Software version 14.12.0 (MedCalc Software bvba, Ostend, Belgium).
Results
Patients’ characteristics
Flowchart is presented in Figure 1. In total, 1711 patients with lung cancer were treated with surgery. Of those, 140 (102 ADC and 38 SCC) were included in this study after excluding patients with non-NED PET scans, pathologies other than ADC or SCC, history of other malignancies, and an interval of more than a year after surgery. Demographics are summarized in Table 1. A positive surgical margin was seen in six patients and lymphovascular invasion in 13 patients. One hundred thirteen patients showed no evidence of nodal metastasis, 15 with N1, and 12 with N2 diseases.
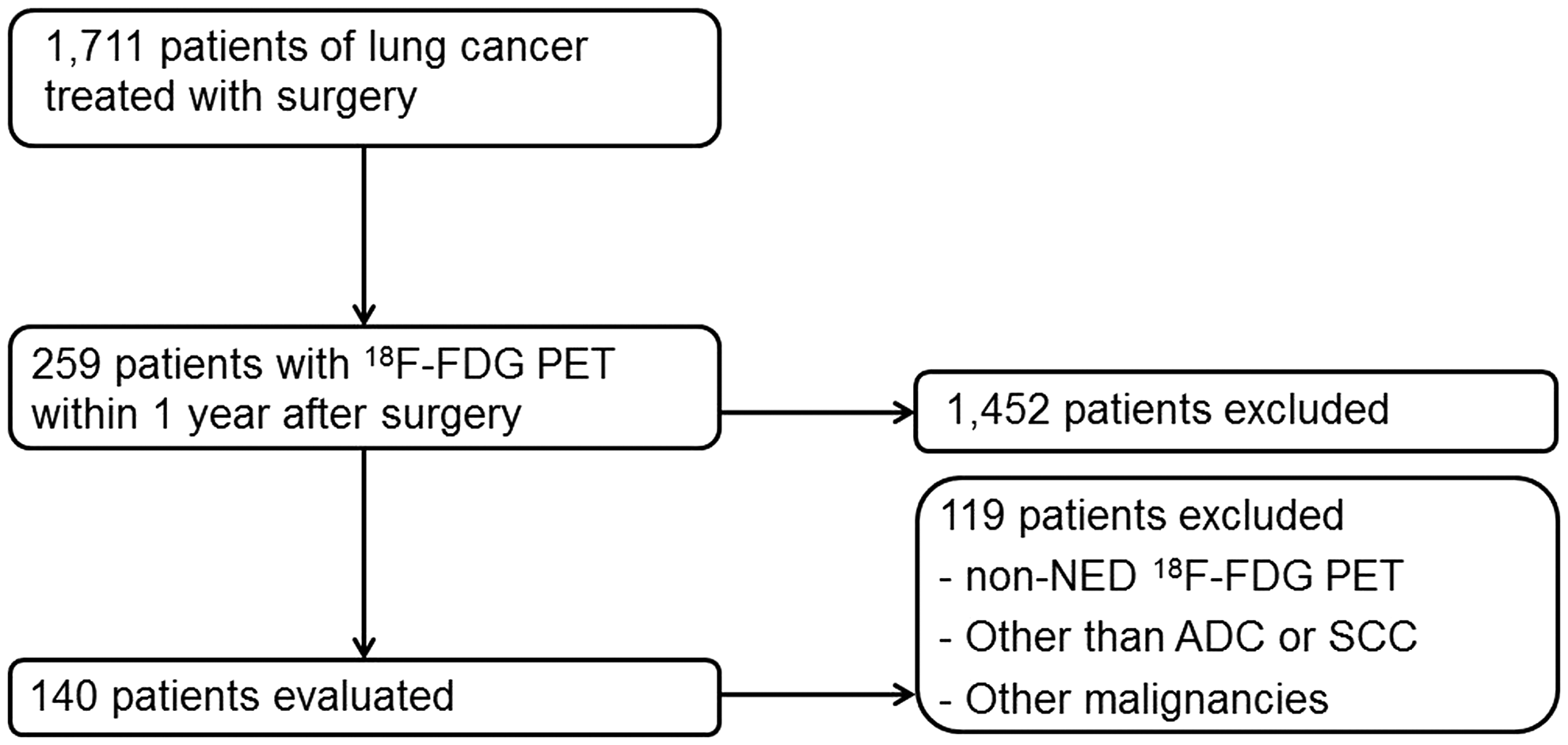
Flowchart of the study.
Prognosis
After an NED PET/CT scan, recurrence was found in 14 patients (10.0%) and deaths in four (2.9%) during a median follow-up of 636 days. CT chest scan detected recurrence in nine patients and PET/CT scan in five. Pleural seeding metastases were found in five patients, metastatic mediastinal LNs in two, and metastatic pulmonary nodules in seven. Three of eight patients with recurrence died during the follow-up. The cumulative probability of DFS within the whole population is shown in Figure 2. In univariate analysis, positive lymphovascular invasion and N2 stage predicted DFS in patients with NSCLC (hazard ratio 7.34, 95% confidence interval 2.55–21.12, p = 0.0002) and N2 stage (4.17, 1.40–12.41, p = 0.0105). Both positive lymphovascular invasion (12.32, 3.32–45.75, p = 0.0002) and TNM stage III/IV (8.54, 2.15–34.0, p = 0.0025) were independent predictors of DFS in multivariate analysis (Table 2). Kaplan–Meier survival curves are shown in Figure 3.
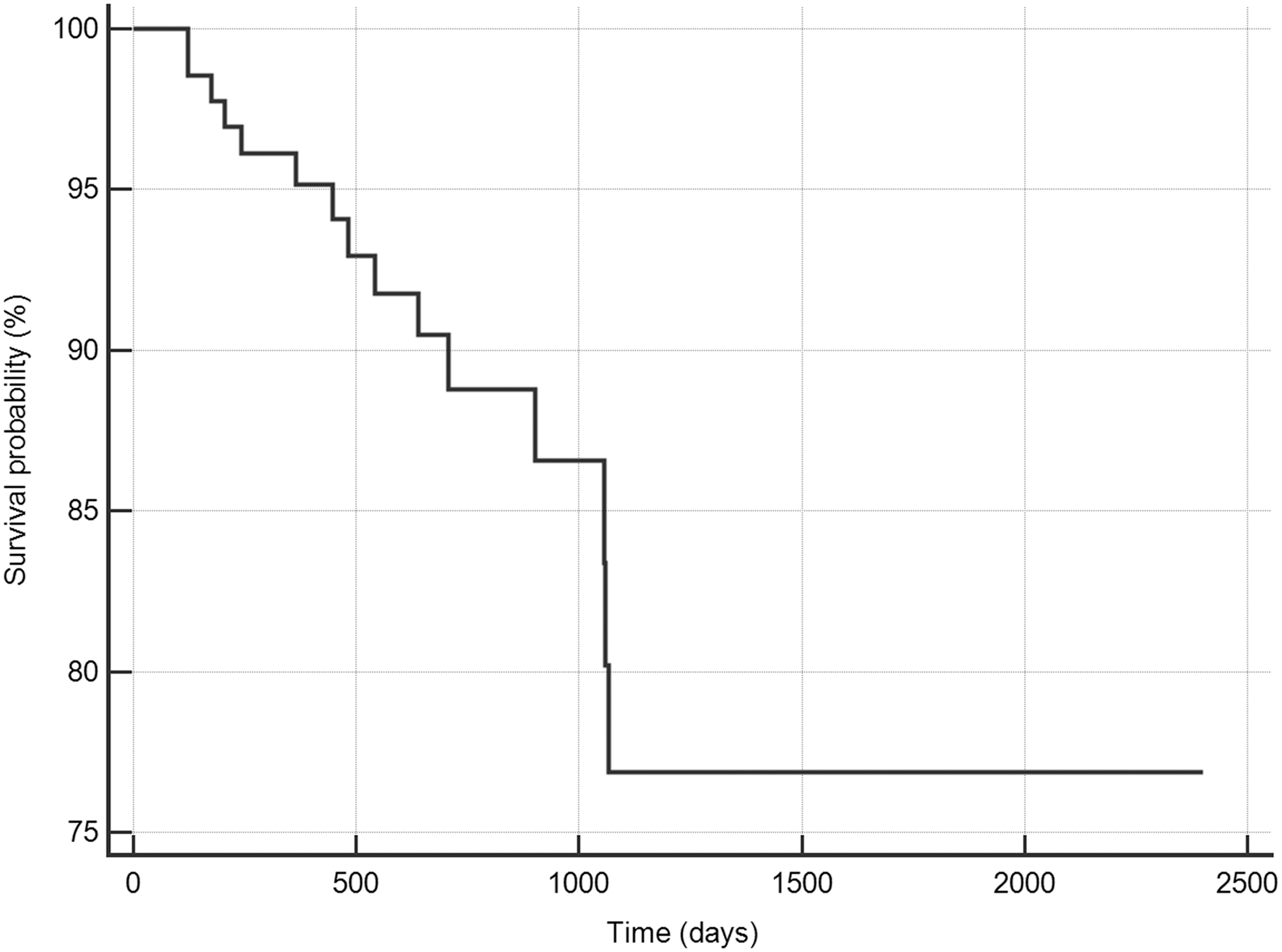
The cumulative probability of disease-free survival in whole population.
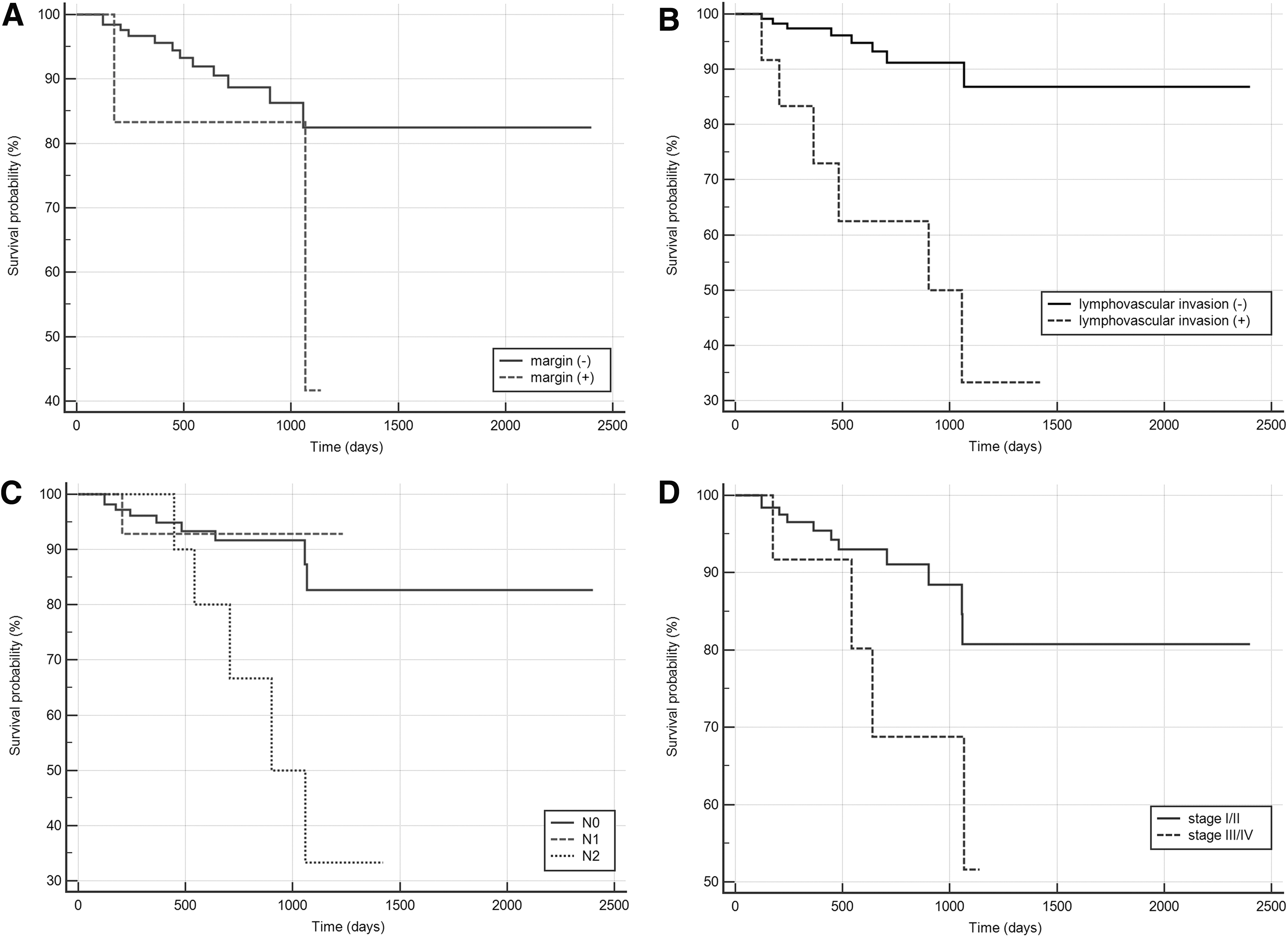
Kaplan–Meier curves;
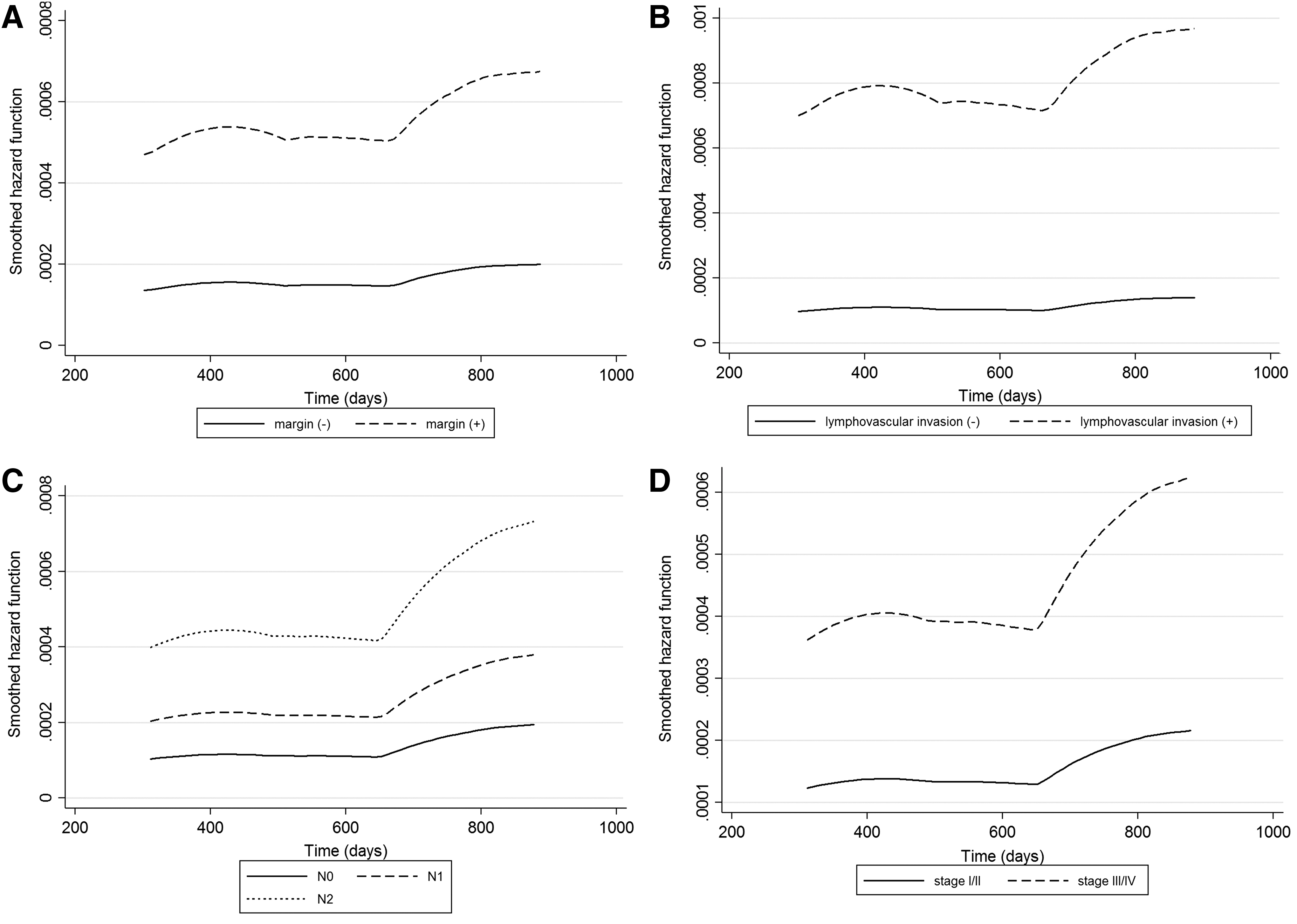
Smoothed hazard functions
Smoothed hazard functions are shown in Figure 4. For the whole population, there was a very low risk until 600 days after normal 18F-FDG PET/CT scans. However, the risk for recurrent disease is continuously increasing after 600 days up to 0.03%. The risk was higher in patients with positive margin at surgery, positive lymphovascular invasion, N2 stage, and TNM stage III/IV (Fig. 5).

Smoothed hazard functions in whole population.
Smoothed hazard functions;
Discussion
PET/CT using 18F-FDG has become an essential tool in patients with lung cancer. According to NCCN guidelines for NSCLC, initial PET/CT at diagnosis should be considered for all patients with lung cancer regardless of stage. 4 Staging with FDG PET/CT was discordant with conventional imaging in ∼50% of patients, which led to a change in treatment management in 40% of patients. 8 FDG PET/CT also has a role in evaluating prognosis. 9 However, few studies have demonstrated the role of 18F-FDG PET/CT in surveillance. Currently, 18F-FDG PET is not warranted for routine surveillance and follow-up in lung cancer. 4,5 The National Comprehensive Network (NCCN) guidelines recommend CT chest scan every 6 or 12 months of surveillance. 4 Recently, studies using FDG PET/CT for surveillance of lung cancer were published. 6,7 Antoniou et al. reported that 18F-FDG PET/CT detected recurrence in 43.7% of scans without prior clinical suspicion and that FDG PET/CT had a role in predicting overall survival. 6 This is similar with the results from Cho et al., which demonstrate that FDG PET/CT could detect early disease recurrence in asymptomatic patients after surgery. 10
In this study, the authors used smoothed hazard functions instead of calculating averaged annual event rates or counting recurrence in a certain period, which was adopted from a study of myocardial perfusion single (MPS)-photon emission CT. 11,12 In patients with suspected or known ischemic heart disease, normal MPS showed a warranty period of 5 years in a study by Simonsen et al. 11 In this study, recurrence or metastasis was found in 15 of 140 patients and deaths in four after NED PET scans. Even in early-stage lung cancer, recurrence was found in 30% of patients in a study by Kelsey et al., 13 which is more common than these results. Using the smoothed hazard functions, the risk of recurrence or metastasis was relatively low (0.015%–0.02%) until 600 days after normal PET scans, increasing continuously after 600 days (0.025%–0.03%). The risk was higher in patients with positive margin at surgery, positive lymphovascular invasion, N2 stage, and TNM stage III/IV.
Lymphovascular invasion was an independent predictor of recurrence or metastasis in lung cancer with a hazard ratio of 12.32 in this study. Previously, the importance of lymphovascular invasion was reported by Shiono et al. 14 Over 90% of advanced NSCLC with lymphovascular invasion had a recurrence within 2 years after surgery. 14 In a meta-analysis, lymphovascular invasion was a strong prognostic indicator toward recurrence with a hazard ratio of 3.63 and deaths with that of 2.38. 15
The value of 18F-FDG PET/CT before and after therapy has been evaluated retrospectively after routine clinical use of FDG PET/CT. Recently, Marcus et al. assessed the value of four or more follow-up PET/CT scans. 16 Treatment was changed after PET/CT in 28% of patients. 16 However, there has been no study that evaluated the warranty period of PET/CT in oncology patients. Therefore, the authors adopted the smoothed hazard function to identify the risk at every time point. To evaluate the risk of patients of NSCLC, first PET scans after surgery with NED were included in this study. As the initial PET scans with evidence of disease after surgery led to subsequent treatment, warranty period could not be estimated and thus was excluded from this study.
There are several limitations in this study. First, this study was a retrospective study with a small sample size. Although the authors searched all databases in this institution between 2007 and 2014, there were only 140 patients who could be included in this study. Second, median follow-up was 636 days; however, studies of long-term follow-ups with a large cohort of patients are needed. In addition, further studies, including patients of subgroup stages, are needed in the future. However, this is the first study that evaluated the concept of warranty period in cancer patients.
Conclusion
Following an NED PET scan after surgery, rates of recurrence or metastasis were very low. However, the risk for recurrence of the disease continuously increased after 600 days up to 0.03%. The risk was higher in patients with positive margin at surgery, positive lymphovascular invasion, N2 stage, and TNM stage III/IV. In addition, lymphovascular invasion was a strong prognostic indicator toward recurrence.
Footnotes
Acknowledgment
This work was supported by the Financial Supporting Project of Long-Term Overseas Dispatch of PNU's Tenure-Track Faculty, 2014.
Disclosure Statement
No conflicting financial interests exist.