
Abstract
The gastrointestinal stromal tumor (GIST) is a rare disease with limited therapeutic options when resistance to tyrosine kinase inhibitor (TKI) treatment occurs. The authors investigated binding of various 68Ga-labeled peptides, targeting receptors reported to be overexpressed in GIST, in different cell lines. For this purpose, three GIST cell lines were tested: GIST-T1, GIST882 (Imatinib sensitive), and GIST430 (Imatinib resistant). DOTA-NT 8–13 (targeting NTR1), DOTA-TATE (targeting SSTR2), CP04 (a minigastrin derivative targeting CCK2-R), VIP-DOTA (targeting VPAC2-R), and 2 DOTA-bombesin derivatives [targeting gastrin releasing peptide receptors (GRPR)] were radiolabeled with 68Ga and incubated with the respective tumor cell and control cell lines. Membrane-bound and internalized activity was measured. Very low or no specific binding to GIST cells was found for all 68Ga-labeled DOTA peptides except for bombesin derivatives indicating no or very low expression of respective receptors. Related to GRPR a pronounced specific binding to all GIST cell lines with no preference related to TKI resistance status was found, both for an agonist (AMBA) with high internalization and for an antagonist (NeoBOMB1) with mainly membrane-bound activity (with up to >80% bound/mg protein). GRPR expression was confirmed by immunohistochemistry. The results show that radiolabeled bombesin analogues, especially antagonists are very promising candidates for targeting GIST.
Introduction
The gastrointestinal stromal tumor (GIST) is the most common mesenchymal tumor of the gastrointestinal tract. With an incidence of 11–14.5 per million inhabitants annually, 1 it is a rare disease that frequently affects young patients and often results in a short life expectancy of less than 3 years. Besides surgical resection, the development of the tyrosine kinase inhibitor (TKI) imatinib (Glivec®), which specifically targets oncogenic KIT (CD117) and platelet-derived growth factor receptors (PDGF-Rα) and benefits 80% of patients with advanced GIST, provided an effective treatment. 2 However, initially sensitive tumors acquire resistance at a median of only 18 months, most often caused by secondary KIT mutation. Sunitinib (Sutent®) and regorafenib (Stivarga®) are two additional multikinase inhibitors for patients who do not respond to imatinib. These drugs are providing a temporary benefit to some patients, but the overall median time to tumor development is only 5–6 months. Targeted molecular therapies have revolutionized the treatment of patients with GIST, but for patients with resistance to TKIs, no treatment alternatives exist and new targeted treatment strategies are needed. 3,4
Targeted radiopharmaceuticals could provide effective means for molecular imaging, 5 radionuclide therapy, or characterization of GIST for minimal invasive therapies. In particular, radiolabeled peptides can target a number of G-protein-coupled receptors overexpressed in a variety of cancers 6 and they have shown excellent results in the diagnosis and treatment especially of neuroendocrine tumors. 7 A variety of receptors have been reported to be overexpressed in GIST. Sternini et al. 8 found a high density of somatostatin 2A (SST2A) receptors on Cajal cells, and Gromova et al. 9 found a high upregulation of neurotensin 1 (NT1) receptors on GISTs independent of their mutational status. Reubi et al. reported that gastrin releasing peptide (GRP) and vasoactive intestinal peptide (VPAC2) receptors were found in 16/19 of GIST tissues, whereas cholecystokinin 2 (CCK2) receptors were found in 12/19 cases. 10 For all these receptors, peptides have been developed that can be radiolabeled with trivalent radiometals for nuclear medicine applications, including diagnosis [positron emission tomography (PET) and single-photon emission computed tomography (SPECT)], as well as radionuclide therapy. 11,12
The MITIGATE consortium, cofunded by the 7th Framework Programme of the European Community, currently pursues the goal to develop new strategies to effectively diagnose and treat patients with metastatic GIST resistant to current treatment. Within this framework, the aim of this study was to investigate a series of 68Ga-labeled peptides targeting SST2A, VPAC2, NT1, GRP, and CCK2 receptors with respect to their binding behavior on three different GIST cell lines, representing different mutational status resulting in variable sensitivity to TKI treatment. So far, no data have been reported on binding of receptor-targeted peptides on GIST cells or on targeting properties in dependence on TKI resistance status. These data could provide a basis for not only selection of optimal candidates toward improved diagnosis but also for therapy of TKI-resistant GISTs.
Materials and Methods
Peptides
All peptides were either purchased commercially or provided within a European collaboration and used as supplied with no further purifications. DOTA (1,4,7,10-tetraazacyclododecane-N,N′,N″,N′″-tetraacetic acid)-conjugated peptides for radiolabeling were selected based on previous reports on high affinity to the target receptor. 13 –18 Their main properties are summarized in Table 1. For blocking studies in case of GRP, CCK2, and SST receptors, human GRP-27, pentagastrin, and octreotide (Sigma Aldrich, Vienna) were used, respectively, for other receptors, the DOTA-conjugated peptides were used.
GRP, gastrin releasing peptide.
Radiolabeling and analysis
68Ga was obtained from a 68Ge/68Ga generator (IGG 100 Gallium 68-Generator; Eckert & Ziegler Berlin), which was eluted with 0.1 N HCl solution (Rotem Industries, Israel). For radiolabeling with 68Ga to the DOTA-conjugated derivatives (10–35 μg), 100–600 μL 68GaCl3 solution (∼30–95 MBq) and 15–90 μL 1.15 M sodium acetate trihydrate—adjusting the pH to 4.0, were added and incubated for 10 minutes at 95°C. For CP04 and VIP-DOTA, temperatures were 90°C and 85°C, respectively. Radiochemical purity (RCP%) determination and the assessment of peptide degradation (e.g., oxidation) were carried out by reversed-phase high-performance liquid chromatography (HPLC) on a Thermo Fisher Ultimate 3000 gradient HPLC pump with a Thermo Fisher UV/VIS detector set at 220 nm using radiometric detection (Raytest Isotopenmessgeraete GmbH, Straubenhardt, Germany). As stationary phase, an ACE 3 μm C18 reversed-phase HPLC column (150 × 3 mm; ACE, Aberdeen, United Kingdom) with a flow rate of 0.6 mL/minute was used with the following gradient: A = 0.1% trifluoroacetic acid (TFA) in H2O, B = 0.1% TFA in acetonitrile ACN): 0–1 minute 0% B; 1–10 minutes 0–50% B; 10–14 minutes: 50% B.
Cell lines
GIST430 and GIST882 cell lines 19 were provided by Prof. Dr. J.A. Fletcher's workgroup (Boston). GIST882 was derived from a patient with a metastasizing tumor (exon 11 K642E). This cell line is moderately sensitive to imatinib and can be used as a model for primary untreated GIST. GIST430 stems from a patient who developed an imatinib resistance during treatment. This cell line has one of the most common mutations in exon 11 (51 nucleotide deletion) and in exon 13V654A. The GIST-T1 cell line is also from a metastasizing GIST with in-frame KIT exon 11 deletion (57 nucleotide) 20 and was provided by Takahiro Taguchi, Kochi University, Japan. As control cells, AR42J rat pancreatic carcinoma cells (expressing rat-SSTR2, -GRP, and -CCK2 receptors), PC-3 cells (human prostate cancer cell line expressing GRP receptors), and HT-29 cells (human colorectal adenocarcinoma cell line expressing NT1 receptors) were used, all from ATCC (Manassas, VA). For VIP-DOTA, no receptor-positive control cells were available.
GIST-T1 cells were cultured in Dulbecco's modified Eagle's medium (DMEM) (Gibco, Invitrogen GmbH, Darmstadt, Germany) supplemented with 10% (v/v) of Gemini fetal bovine serum (FBS) (Thermo Fisher Scientific, Vienna), 0.5% of penicillin/streptomycin/glutamine (PSG) solution (Thermo Fisher Scientific), and 0.5% of Fungizone/amphotericin B (Gibco). GIST430 cells were cultured in RPMI 1640 (Gibco), GIST882 in Iscove's modified Dulbecco's medium (IMDM, Gibco), both supplemented with 15% (v/v) of FBS, 1% of PSG, 0.5% of Fungizone/amphotericin B, and 10 μg/mL (final concentration) of gentamycin. AR42J and PC-3 cells were cultured in RPMI 1640 supplemented with 10% (v/v) of FBS and 1% of PSG. HT29 cells were cultured in McCoy's 5A medium with glutamine (Gibco) and 10% (v/v) of FBS.
All cells were grown to confluence in tissue culture flasks (Cellstars; Greiner Bio-One, Kremsmünster, Austria) at 37°C in a humidified atmosphere containing 5% CO2. The cells were passaged two times per week using 1 mL of a solution containing 2.5% of trypsin (Thermo Fisher Scientific) mixed with sodium chloride (1:10). GIST-T1 cells were split 1:3 or 1:5, whereas GIST430 and GIST882, which have a slower growth rate, were split only 1:3.
Binding and internalization assays
Cells were seeded at a density of 1 × 106 cells per well in six-well plates (Greiner Bio-One) and grown to confluency for 48 hours. On the day of the experiment, the medium was removed and cells were washed twice with 1 mL of ice-cold internalization medium (DMEM containing 1% FBS). After addition of 1.2 mL of medium, 150 μL of phosphate-buffered saline (PBS) containing 0.5% bovine serum albumin (BSA) (total binding) or 150 μL of 1 μM peptide blocking solution containing 0.5% BSA (nonspecific binding) was added, followed by addition of the corresponding 68Ga-labeled peptide (∼120,000 cpm; 1.13 nM) in 150 μL water. Plates were incubated for 10, 30, 60, or 90 minutes at 37°C. Incubation was interrupted by removing the incubation medium and washing the cells twice with 1 mL of ice-cold medium. Thereafter, 1 mL of ice-cold glycine buffer (pH 2.8, 0.05 M glycine/0.1 M sodium chloride) was added to release membrane-bound radioligand. After 5 minutes, the supernatant was collected in plastic vials. The procedure was repeated once and cells were then lysed two times with 1 mL of 1 N sodium hydroxide solution to release them from the plate and again the fractions were collected (internalized radioligand fraction). The radioactivity of membrane-bound radioligand fraction (glycine buffer) and the internalized fraction (sodium hydroxide) was measured in a 2480 Wizard 2 3″ automatic gamma counter (Perkin Elmer, Vienna, Austria). The sodium hydroxide fraction was used for the Bradford assay to determine the protein content. The membrane-bound, internalized activity or total cell-associated activity (membrane bound + internalized fraction) was expressed in relation to the total activity added and normalized to protein content (%bound/mg protein). Specific membrane-bound or internalized fractions were calculated as total membrane-associated or internalized activity minus the respective nonspecific activity expressed as % of total added activity normalized to protein content (% specific/mg of protein). Each peptide was tested at least in two independent experiments on each cell line.
Displacement assay
Binding affinity of NeoBOMB1 was determined by using GIST-T1, GIST430, GIST882, and PC-3 cells and 125I-Tyr4-bombesin (Perkin Elmer, Waltham, MA) as radioligand incubated with increasing concentrations of NeoBOMB1 as competitor.
Ninety-six-well MultiScreenHTS-FB plates (Merck Millipore, Darmstadt, Germany) were washed with 250 μL 10 mM TRIS-buffered saline (pH 7.3). Cells were diluted in 50 mM HEPES buffer containing 5 M MgCl2, 14 mM bacitracin, and 0.3% BSA. Then, 150 μL of the cell solution (1–8 × 105 cells/mL) was added into each well and incubated with 50 μL 125I-Tyr4-bombesin (81.4 TBq/mmol, ∼20,000 cpm/well, diluted in 20 mM HEPES buffer pH 7.3 with 0.4 g BSA, 10 M MgCl2, and 14 mM bacitracin). Hereafter, 50 μL of NeoBOMB1 was added at increasing concentrations (0.001–1000 nM) and the plate was incubated for 1 hour at room temperature (RT). Unbound radioligand was removed by two washes with 250 μL TRIS-buffered saline. Filters were collected in plastic tubes and the remaining radioactivity on the filter was measured in the gamma counter. IC50 values were determined by fitting the percent inhibition data using nonlinear curve fitting (Origin 6.1, Northampton, MA).
Immunohistochemistry
The different GIST cell lines (GIST-T1, GIST430, GIST882) and the control cells PC-3 (expressing the GRP receptor), at a concentration of 0.6 × 106 cells, were seeded onto poly-
Results
Radiolabeling
Samples of RP-HPLC radiochromatograms of the 68Ga-labeled peptides (DOTA-TATE, CP04, NT 8–13, VIP-DOTA, NeoBOMB1, and AMBA) are shown in Figure 1. For all peptides, a radiochemical purity of >90% was achieved. Therefore, all radiolabeled peptides were used in binding assays without further purification.
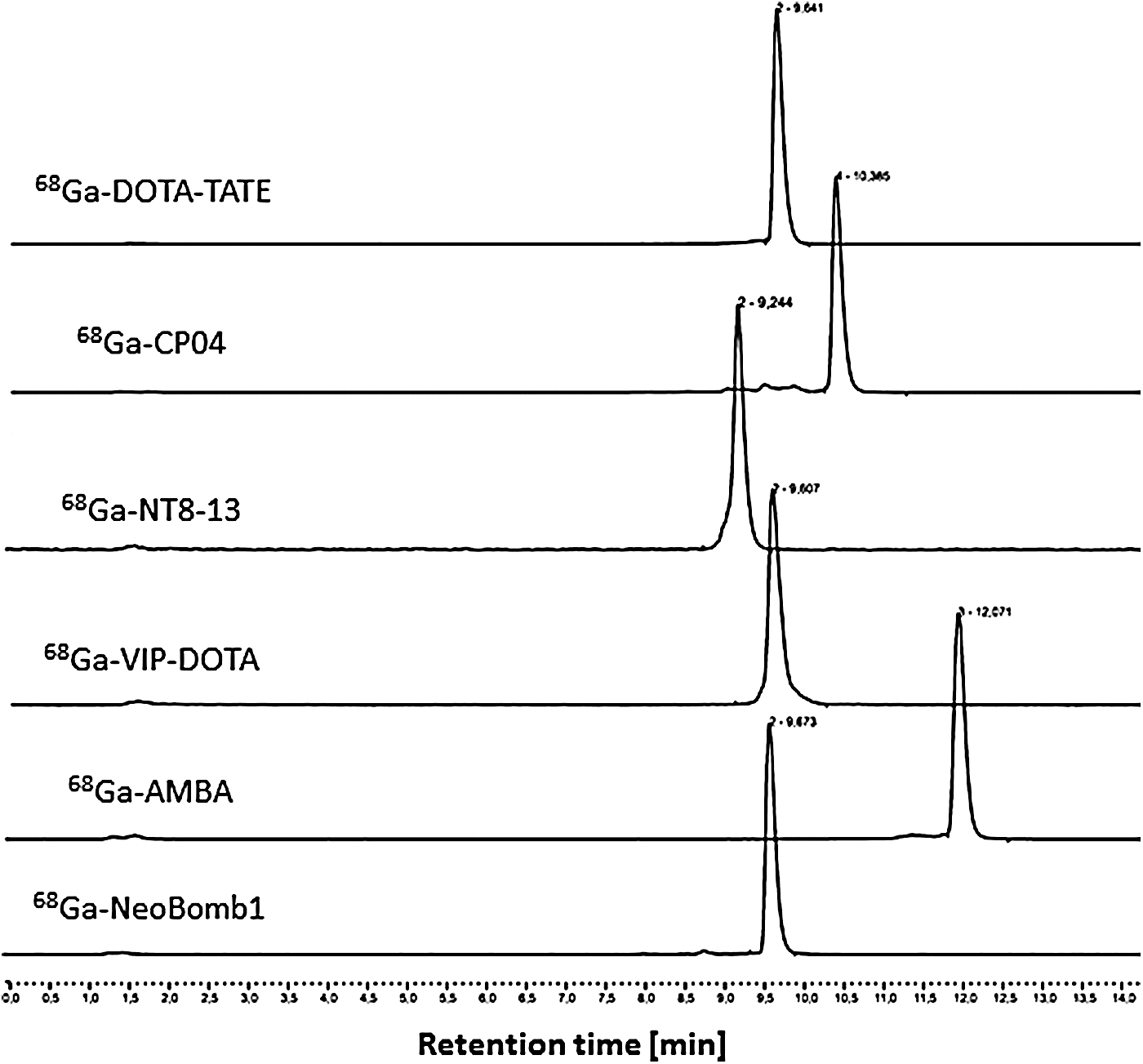
RP-HPLC radiochromatograms of the 68Ga-DOTA peptides under study. RP-HPLC, reversed-phase high-performance liquid chromatography.
Binding assays
The binding and internalization studies showed highly variable results for the different DOTA peptides in terms of membrane binding and cell internalization. Even though internalized activity values increased up to 90 minutes, the 60-minute time point was chosen as comparison for all radiolabeled peptides, being the optimal compromise between high cell binding and internalization and decay of the radionuclide 68Ga with a half-life of 68 minutes.
Figure 2 shows examples of binding assays on GIST882 cells for all peptides studied. Low binding and no pronounced difference in binding between nonblocked and blocked cells for 68Ga-DOTATATE, VIP-DOTA, DOTA-NT(8–13), and CP04 both in the membrane-bound fraction and in the cells (internalized fraction) were found. Nonspecific binding varied between different peptides from <1% and >5% of activity/mg protein. For both bombesin analogues (AMBA and NeoBOMB1), a high binding of >10% was observed in at least one fraction that could be blocked with excess of cold peptide.
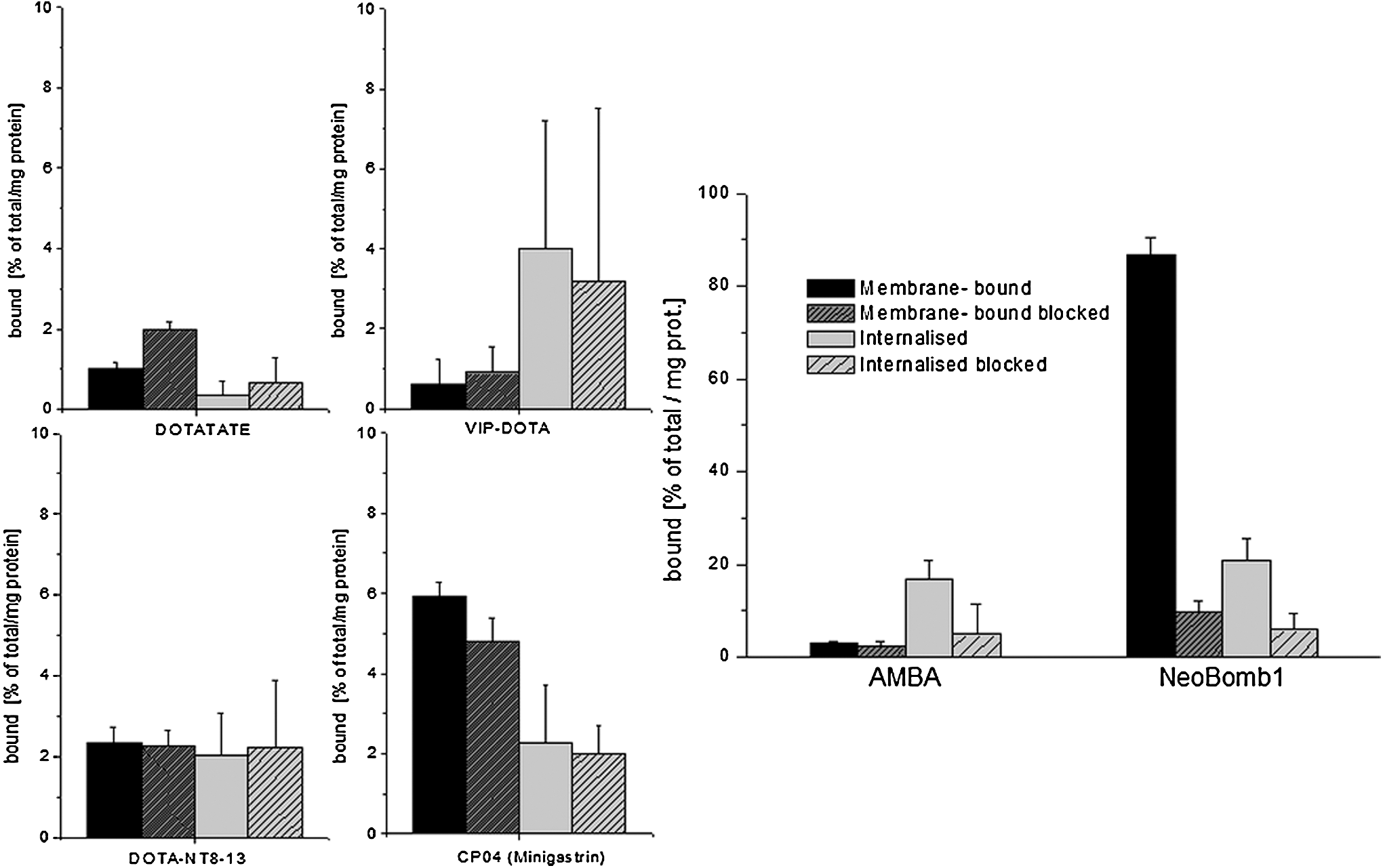
Examples of binding assays: Blocked and nonblocked membrane-bound and internalized activity (% of total/mg protein) comparing all 68Ga-labeled peptides under study after 60 minutes of incubation on GIST882 cells. The binding is expressed as mean ± SD of three independent experiments (n = 3; % of total/mg protein). Receptor blocking was performed (assay concentration 1 μM) with octreotide (SSTR2), pentagastrin (CCK2), GRP human (GRP), or the corresponding DOTA peptide (VIP-DOTA, DOTA-NT8-13) itself. GRP, gastrin releasing peptide; SD, standard deviation.
To correct for differences in nonspecific binding, which varied between peptides and different cell lines, nonspecific binding was subtracted from total binding to allow comparison between different tracers and cell lines. Results were expressed as specific membrane-bound or internalized activity. A summary of specific binding data on all cell lines is shown in Table 2 and Figure 3. Based on differences in cell numbers and nonspecific binding, the authors defined a receptor-specific signal as >3%/mg protein, that is, >25% of the specific value found on control cell lines AR42J and HT-29.
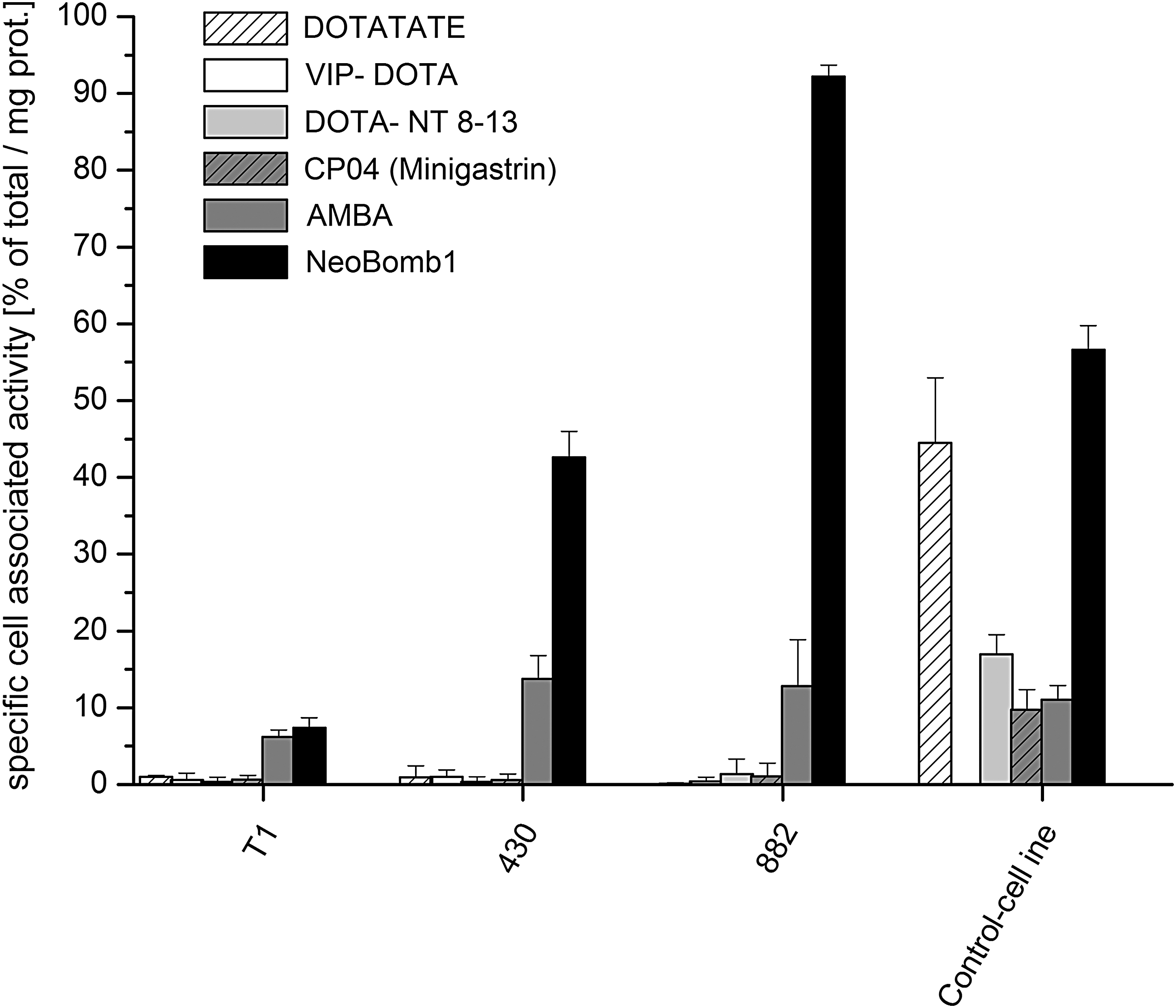
Comparison of receptor-specific cell-associated activity (membrane bound + internalized minus the nonspecific activity) calculated as % of total activity added/mg protein of the different 68Ga-labeled DOTA peptides on GIST cell lines after 60 minutes of incubation at 37°C. AR42J was used as the control cell line for SST, GRP, and CCK2 receptors, HT29 for NT1 receptors; no control cell line was available for VPAC2 receptors.
Data are shown as range from the values obtained in the three cell lines.
Receptor-specific signal (>3%/mg protein).
All peptides except those targeting the GRP receptor displayed no or only very low-specific binding signals. AR42J cells demonstrated receptor-specific binding for 68Ga-labeled CP04, DOTA-TATE, as well as AMBA and NeoBOMB1 and HT29 cells for 68Ga-DOTA-NT 8–13, proving the applicability of the method for evaluation of receptor targeting properties.
Concerning GIST, only the 68Ga-labeled bombesin analogues, AMBA and NeoBOMB1, displayed a clear receptor-specific signal in the internalized fraction and in the membrane-bound fraction, respectively. 68Ga-AMBA showed a specific internalization (3.2%–12.0%/mg protein) and also specific membrane binding up to 3.4%/mg protein. 68Ga-NeoBOMB1 showed a specific membrane-bound fraction (6.2%–77.1%/mg protein) with a lower fraction being internalized (1.29%–15.06%/mg protein).
Comparing the binding behavior of the bombesin analogues, 68Ga-AMBA and 68Ga-NeoBOMB1 on the three different GIST cell lines, higher signals were found for GIST430 and GIST882 cells compared to the GIST-T1 cell line. However, this difference may be overestimated, as GIST-T1 cells revealed much better cell growth that was possibly overcorrected when normalizing to the protein content of the cells. A clear difference in binding behavior was found for the 68Ga-bombesin analogues reflecting the difference of an agonist versus an antagonist, as shown in Figure 2. In the case of 68Ga-AMBA, activity was mainly internalized, whereas for 68Ga-NeoBOMB1, membrane-bound activity was predominant, even though a small specifically internalized fraction was also detected. Blocking reduced the receptor signal significantly in all cases.
Binding affinity of NeoBOMB1 on GIST cells
Displacing of 125I-Tyr4-bombesin from GIST cell lines with NeoBOMB1 revealed the high binding affinity of bombesin antagonist to all cell lines comparable with PC-3 control cell lines. The mean IC50 values of the different independent experiments (n = 3–4) were 0.73 ± 0.31 nM, 0.38 ± 0.01 nM, and 0.51 ± 0.04 nM for GIST-T1, GIST430, and GIST882, respectively, compared to a value of 0.98 ± 0.45 nM for PC-3 control cell lines. Representative displacement curves are shown in Figure 4.

Representative displacement curves of 125I-Tyr4-bombesin by NeoBOMB1 from GIST-T1, GIST430, GIST883, and PC-3 as control cell line.
Immunohistochemistry
To better characterize the GRP receptor expression on GIST cells with different mutational status, IHC was performed. Results are shown in Figure 5. The brown staining displays the presence of the GRP receptor in the cells and confirms the results from binding assays. GIST-T1, GIST882, and PC-3 control cells showed >95% of cells stained, whereas for GIST430, a slightly lower percentage of 80% stained cells was found.
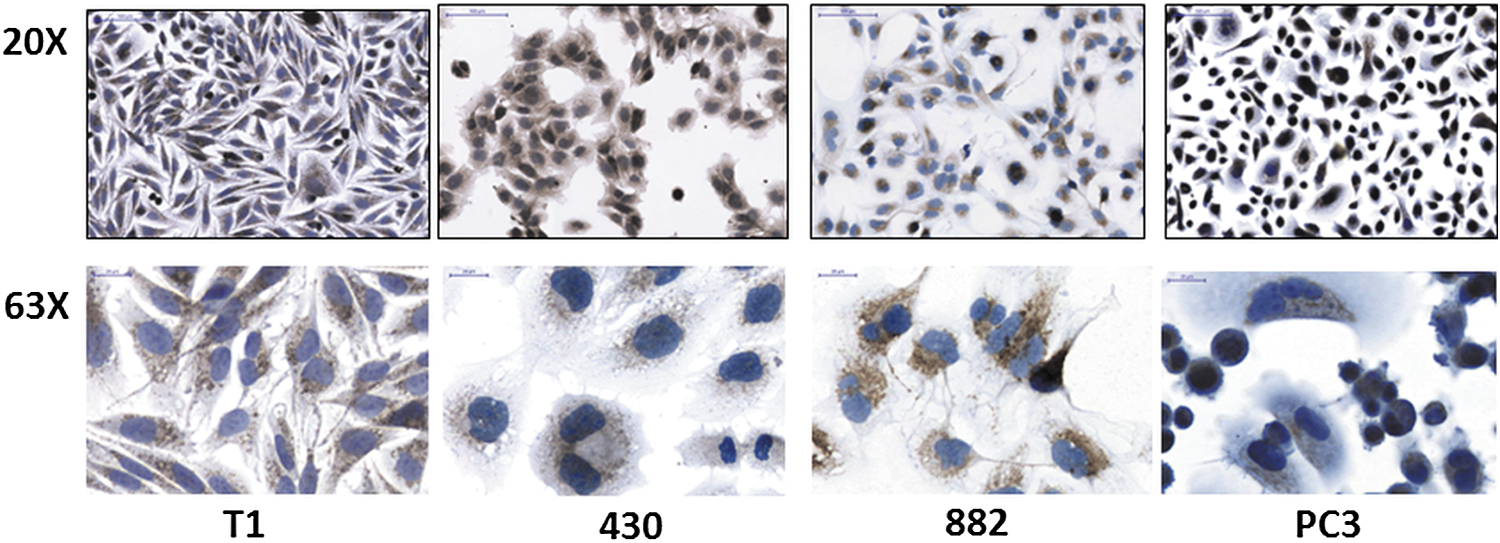
Staining of GRP receptors on GIST-T1, GIST430, GIST882, and PC-3 (control) cells. Positive staining is indicated by the brownish color, blue staining represents the nucleus counterstaining (Mayer's Hämalaun). Color images available online at
Discussion
GIST is a rare disease that metastasizes in up to 85% of patients with subsequent median progression-free survival (PFS) of only around 30 months. Tumors are characterized by activating mutations in the KIT or the PDGF-Rα gene, and therefore, treatment is mainly based on TKI designed to block these mutated receptors. However, drug resistance is often based on mutations changing the conformity of the receptor, leaving a few effective therapeutic options to these patients. To date, second-line chemotherapy offers a median PFS of 6–9 months and external beam radiotherapy is limited by organs at risk close to the tumor. Alternative approaches are inconsistently used and are not tailored to the individual patient's type of disease. Radiolabeled peptides, mostly originating from regulatory peptides, are a potential alternative in GIST aiming at receptors overexpressed on tumor cells. 21 This can be utilized for improved diagnosis by not only providing an imaging biomarker but also by switching from a diagnostic radionuclide to a particle emitter, for targeted radionuclide therapy. With the advances of PET for molecular imaging, in particular Ga-68 as a generator radionuclide, with short half-life of 68 minutes, has found a tremendous interest with a variety of clinical applications in combination with peptides. 22
The authors therefore selected different 68Ga-labeled peptides to evaluate their binding behavior on GIST cell lines, originating from patients with different status of resistance in relation to TKI treatment. They chose an assay that allows direct assessment of the binding behavior of the 68Ga-labeled peptide itself. As regulatory peptide receptors, belonging to the G-protein-coupled receptor type, typically internalize after binding of an agonistic peptide, a protocol allowing distinguishing between membrane-bound and internalized activity was selected.
Literature reports the expression of different regulatory peptide receptors on GISTs, 8 –10 and the initial aim was to see whether the authors could find a target suitable to distinguish between TKI-resistant and TKI-sensitive tumors. To their surprise, most peptides studied did not reveal any specific receptor-related binding, neither binding to cell membranes nor showing internalization into the cell. This could be based on the fact that tumor cell lines were used, which do not reflect the natural tumor itself, where these receptors were usually found, for example, for CCK2 and VPAC2 receptors. 10 Also, receptor overexpression was not found in 100%, but only in 63% and 84% for these receptor subtypes, respectively. For other receptors, this finding could be based on the fact that overexpression was proven by qPCR 6 and not on the protein level for NT1 or was only found on tumor precursor cells for the SST2A receptors. 8 Even though some DOTA peptides chosen for this evaluation have shown suboptimal in vivo properties, 15,16 they all were reported to have high receptor affinities in the low nanomolar range and to be stable under in vitro testing conditions. In addition, for most peptides, assays using control cells with known overexpression of the respective receptor revealed a clear receptor-specific binding of the 68Ga-labeled peptides. Therefore, the lack of receptor binding has to reflect the lack of receptor expression on the cell surface and not the lack of binding ability of the DOTA peptide conjugates. In any case, it gives a strong indication that these peptides will be unsuitable to be used to target GISTs in patients.
In contrast to that, GRP receptor (also called BB2 for bombesin receptor subtype 2) targeting was successful in all GIST cell lines. High receptor internalized fraction was found for 68Ga-AMBA, a GRP receptor agonist, whereas 68Ga-NeoBOMB1 was predominantly specifically bound to the cell membrane, reflecting its action as antagonist. GRP receptors are a well-known target for GIST. Reubi et al. 10 reported GRP receptor overexpression in primary GISTs, metastases, and even tumor samples from patients who did not respond to imatinib. 68Ga-BZH3, a GRP receptor agonist, has already been evaluated in GIST patients, 23 however, with a lower detection rate and tumor accumulation compared to 18F-FDG. This may, however, also reflect the suboptimal targeting properties of the agonist BZH3 used in this study. Besides, the Phe 13 analog of BZH3 has been shown to undergo rapid enzymatic degradation in vivo. 24 As an agonist, it also poses a safety concern due to potential side-effects. In recent years, numerous developments of GRP receptor targeting peptides have been made 25 mainly toward applications in prostate and breast cancer. In particular, the use of antagonists is seen favorable in terms of targeting, 26 and, more importantly, in terms of side-effects showing a much better safety profile. NeoBOMB1 is a recently developed receptor antagonist with excellent metabolic stability. 18 In this study, 68Ga-NeoBOMB1 showed a high accumulation on membranes of GIST cell lines with only a small fraction internalized in the tumor cells. This small amount of internalized activity is in accordance with findings of other GRP receptor antagonists, including 68Ga/111In/177Lu-NeoBOMB1, 18 indicating turnover of GRP receptors independent of ligand binding. Overall, a much higher receptor-mediated signal compared to the agonist 68Ga-AMBA could be detected. There seemed to be a somewhat better binding to both imatinib-resistant and imatinib-sensitive GIST430 and GIST882 cells compared to GIST-T1 cells and the authors wanted to confirm this by alternative methods. Unfortunately, flow cytometry (FACS), as well as western blot analysis, did not provide a receptor-specific signal with the antibody used (data not shown). IHC revealed a comparable high expression of the GRP receptor on all cell lines, including PC-3 control cells. Therefore, it can be expected that GRP targeting of 68Ga-NeoBOMB1 will be possible independent of the TKI resistance status of the tumor. Competition experiments were conducted to address potential differences in GRP receptor binding affinity on different GIST cell lines, not to differentiate receptor densities (data not corrected for cell numbers). Overall, the high affinity of NeoBOMB1 to the GRP receptor was confirmed by the low IC50 values on GIST cell lines below 1 nM, with no relevant difference in binding affinity between different GIST cell lines or compared to the PC-3 control cell lines. This is also in accordance with recently reported high affinity (IC50 values between 1.2 and 1.5 nM) of NeoBOMB1 and its metalated [natGa]- [natIn] and [natLu] species determined against [125I-Tyr4]BBN on PC-3 cell membranes. 18 This supports the suitability of NeoBOMB1 for specific targeting of GIST in vivo.
Conclusions
From a series of 68Ga-DOTA peptides binding to a variety of different regulatory peptide receptors, only bombesin analogues targeting the GRP receptor were found to specifically bind to GIST cells. The expression of the receptors was confirmed by IHC and was found to be comparable in three different GIST cell lines with variable status of resistance to TKI treatment. The GRP receptor antagonist 68Ga-NeoBOMB1 revealed a pronounced and specific binding to GIST cells with high affinity. Studies in GIST-bearing mice are currently in progress and will form the basis for clinical translation. The recently reported excellent targeting properties of 68Ga-NeoBOMB1 in prostate cancer both in animal tumor models and in patients 18 make it a highly promising candidate for GIST targeting with the aim to improve imaging and monitoring of TKI-resistant tumors, and also subsequently to open new options for targeted radionuclide treatment using, for example, 177Lu-labeled counterparts.
Footnotes
Acknowledgments
This work was performed within the MITIGATE project, cofunded by the European Community's 7th Framework Programme (FP7/2007-20013) under grant agreement no 602306. The authors thank Dr. J.A. Fletcher (Dana-Farber, Boston) for the kind gift of Cancer Center GIST cell lines (GIST430, GIST882). Dr. Anette Duensing and Dr. Sabrina Schubert are acknowledged for organizing all GIST cells. Dr. Patricia Moser is acknowledged for evaluation of IHC staining.
Disclosure Statement
No competing financial interests exist.