
Abstract
Aims:
In this study, the authors aimed to identify prognostic factors after selective internal radiation therapy (SIRT) for colorectal cancer (CRC) liver metastasis.
Methods:
Forty-nine (28 male, 21 female; mean age: 64.6 ± 10.8) patients who received SIRT for CRC liver metastasis were studied. Effects of number (<5 vs. ≥5), maximum dimension, and standardized uptake value (SUV) of liver metastases, liver tumor load (<25% vs. 26%–50% vs. 51%–75%), presence of extrahepatic disease, and metabolic early response on overall survival were analyzed.
Results:
Mean follow-up time was 44.1 ± 27.5 months. Overall survival time was calculated as 10.03 ± 1.61 (95% CI; 6.86–13.20) months. SUV (0.004) of liver metastases, early metabolic response (p = 0.015), and presence of extrahepatic metastasis (p = 0.001) were identified as significant factors influencing overall survival. The hazard ratio was 1:2.3 for the presence of extrahepatic metastasis and 1:2.7 for the absence of early metabolic response.
Conclusion:
These findings suggest that patients with CRC liver metastasis who have lower SUV at presentation and early metabolic response have better outcomes after SIRT.
Introduction
Presence of liver metastasis is a negative prognostic factor for colorectal cancer (CRC) patients. Although surgery remains the only curative treatment, only 20% of patients are suitable for surgical resection. Moreover, the 5-year survival rate is 20% even in the cases who underwent surgical resection. 1 Selective internal radiation therapy (SIRT) is an effective transarterial treatment method for unresectable CRC liver metastasis. 2 Selective/superselective administration of 90Y microspheres through the hepatic artery delivers high radiation doses to the tumor without damaging the normal liver parenchyma. 3,4
Although all the patients fit the appropriateness criteria for SIRT, response rates and survival times after SIRT vary in the current literature. 5 –7 In the context of personalized medicine, descriptions of novel prognostic factors are needed for the selection of patients for whom SIRT is likely to improve survival. Thus, the number and dimension of liver metastases are important because they are directly correlated with tumor load in the selection for surgical resectability and are expected to effect survival. 8 Although the presence of extrahepatic disease is not a contraindication, and liver dominant disease is an application option for CRC liver metastasis, its effect on survival and treatment response is controversial. 9
After administration, the method of choice for evaluation of response to SIRT is also subject to debate. 10 Radiological response evaluation could be performed by contrast enhanced computed tomography (ceCT) or magnetic resonance imaging (MRI). Radiological size criteria (Response Evaluation Criteria in Solid Tumors [RECIST]) have limitations for the evaluation of response to radioembolization. 11 Indeed, tumors that responded to radioembolization may show an initial transient increase in size. 12 Although the first dimensional changes may already be observed after 1 month, it is widely accepted that at least 3–4 months are necessary to reliably estimate the actual response and, therefore, evaluate whether retreatment may be considered. Metabolic response evaluation can be performed with either 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) or computed tomography PET (CT-PET) and is especially beneficial in CRC liver metastases. Metabolic imaging is advantageous because of the possibility for response prediction within 6–8 weeks, when radiological changes do not yet occur. 13
Here the authors aimed to analyze the effects of all of the factors mentioned above to predict survival times after SIRT for CRC liver metastasis.
Methods
Patients
Between June 2008 and April 2015, 72 patients received SIRT for CRC liver metastasis. Twelve patients were directly excluded from the analysis because their follow-up data were unavailable. All cases were reviewed by an experienced hepatobiliary surgeon with expertise in advanced liver surgery. Considering recent developments in liver surgery, a further 11 cases were identified as potentially resectable. 14 Finally, 49 (28 male, 21 female; mean age: 64.6 ± 10.8) patients who received SIRT for inoperable CRC liver metastasis were included in the analysis. Follow-up data were gathered through the electronic medical records. Seven patients had received radiofrequency ablation treatment and 1 patient had undergone chemoembolization for liver metastasis before SIRT. During evaluation of appropriateness for SIRT, routine biochemistry tests, including liver and kidney functions, ceCT of liver, 18F-FDG-PET/CT, and hepatic artery perfusion scintigraphy with 99mTechnesium (99mTc) macro aggregated albumin, were performed. Number and maximum dimension of liver lesions and tumor load in the liver were calculated from ceCT images that are obtained 1–4 weeks before SIRT.
18F-FDG-PET/CT
All patients underwent 18F-FDG-PET/CT before SIRT for evaluation of disease stage. PET/CT images were acquired with a GE Discovery ST PET/CT scanner. Patients fasted at least 6 hours before imaging, and blood glucose levels were checked. Those with a blood glucose level above 150 mg/dL did not undergo scanning. Oral contrast was given to all patients. Images from the vertex to the proximal femur were obtained while the patients were in the supine position. Whole body 18F-FDG-PET/CT imaging was performed ∼1 hour after an intravenous injection of 8–10 mCi 18F-FDG. During the waiting period, patients rested in a quiet room without taking muscle relaxants. PET images were acquired for 4 minutes per bed position. Emission PET images were reconstructed with noncontrast CT images. CT images were also obtained from the patient's integrated 18F-FDG-PET/CT with the use of a standardized protocol of 140 kV, 70 mA, tube rotation time of 0.5 seconds per rotation, a pitch of 6, and a slice thickness of 5 mm. Patients were allowed to breathe normally during the procedure. Attenuation-corrected PET/CT fusion images were reviewed in three planes (transaxial, coronal, and sagittal) on a Xeleris Workstation 4.2 (GE Medical Systems). PET/CT images were evaluated and confirmed visually and semiquantitatively with standardized uptake value (SUV) by consensus of two experienced nuclear medicine specialists.
SIRT treatment
In all patients, widely accepted parameters for liver reserve, bone marrow reserve (granulocytes >1500/μL, platelets >60,000/μL), and hepatic vascularity were used as inclusion and exclusion criteria. Liver reserve was evaluated using bilirubin, aspartate transaminase (AST), alanine transaminase (ALT), and alkaline phosphatase (ALP) levels in blood. A bilirubin level <2 mg/dL and AST/ALT/ALP levels less than five times the normal upper limit were required for radioembolization. In patients who were suitable for therapy, informed consent was obtained. The 90Y dose was adjusted according to the following body surface area (BSA) method: activity (GBq) = (BSA −0.2) + tumor volume/total liver volume. Tumor and liver volumes were calculated from CT images. Lung shunt fraction was calculated from hepatic artery perfusion scintigraphic images. Mean absorbed dose thresholds were accepted as 120 Gy for tumor, 50 Gy for nontumorous liver tissue, and 20 Gy to the lung. 15 The 90Y resin microspheres (Sirtex Medical) were injected through selective catheterization of the hepatic artery catheter under intermittent fluoroscopic visualization. Within 1–24 hours after microsphere infusion, Bremsstrahlung images were obtained to confirm that the 90Y was deposited only in the liver. All patients were hospitalized overnight and medications (e.g., analgesics, antiemetic, and H2 antagonists) were administered, if necessary. All patients were closely monitored until acute or late toxicities were resolved.
Evaluation of treatment response
Early metabolic response evaluation was done at the 6th week after SIRT by 18F-FDG-PET/CT with PERCIST criteria. In addition, radiological evaluation was performed at the 3rd month of treatment by RECIST criteria.
Data and statistical analysis
Effects of number (<5 vs. ≥5), maximum dimension, and SUV of liver metastases, liver tumor load (<25% vs. 26%–50% vs. 51%–75%), presence of extrahepatic disease, and metabolic early response on overall survival were analyzed. Statistical analysis was carried out with SPSS 16.0 (SPSS) for Windows. Data are expressed as the mean ± standard deviation. Kaplan–Meier analysis and life tables were used for survival analysis. Cox regression analysis was performed to analyze the effect of different parameters to overall survival. A p-value less than 0.05 was considered as significant.
Results
Patients
Primary tumor locations were colon and rectum in 41 and 8 patients, respectively. Pretreatment mean serum AST, ALT, and bilirubin levels were calculated as 45.2 ± 26.1 IU/mL, 35.6 ± 25.9 IU/mL, and 0.8 ± 0.4 mg/dL, respectively. The number of liver lesions was <5 and ≥5 in 39 (80%) and 10 (20%) patients, respectively. Mean dimension of the largest liver lesion was calculated as 50.86 ± 37.6 mm (min–max: 10–160 mm). Tumor load of the liver was <25%, 26%–50%, and 51%–75% in 18 (37%), 19 (39%), and 12 (24%) patients, respectively. Twenty-nine (59%) patients had extrahepatic diseases that are located on the lung (17, 34%), lymph nodes (18, 37%), bone (5, 10%), and adrenal gland (1, 2%). Mean SUVmax of liver metastases was calculated as 14.2 ± 7.3.
SIRT treatment
SIRT was given in the right, left, or both liver lobes in 30, 7, and 12 patients, respectively. Mean administered dose was calculated as 1.54 ± 0.2 GBq. Mean absorbed dose to the tumors ranged between 565 and 870 (mean: 675 ± 123) Gy. The authors observed no severe treatment-related side-effect that could not be controlled with symptomatic treatment. 90Y deposit was confirmed in all patients' liver lesions in Bremsstrahlung images.
Treatment response, follow-up, and survival
Early metabolic treatment response was evaluated by 18F-FDG-PET/CT in the 6th week of treatment. Radiological response was interpreted in the 3rd month of treatment. Twenty-nine (59%) patients had early metabolic response to treatment. Forty-two patients died during the 44.1 ± 27.5 months mean follow-up period. Overall survival time was calculated as 10.03 ± 1.61 (95% CI; 6.86–13.20) months. SUV (0.004) of liver metastases, early metabolic response (p = 0.015), and presence of extrahepatic metastasis (p = 0.001) were the significant factors to influence overall survival (Table 1). The hazard ratio for the presence of extrahepatic metastasis was 1:2.3 (Fig. 1) and absence of early metabolic response was 1:2.7 (Fig. 2).
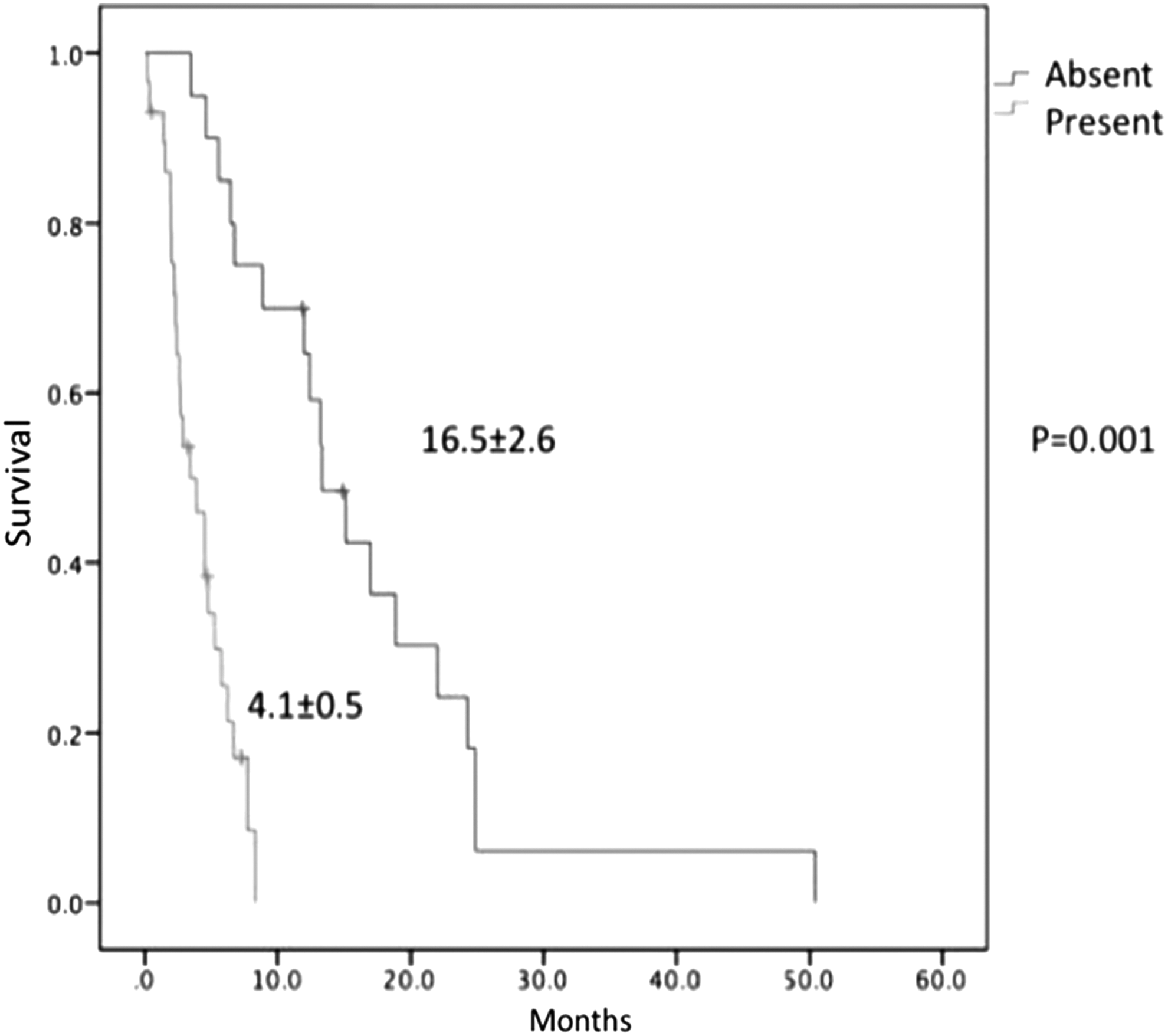
Survival curves of patients either with or without extrahepatic metastasis.
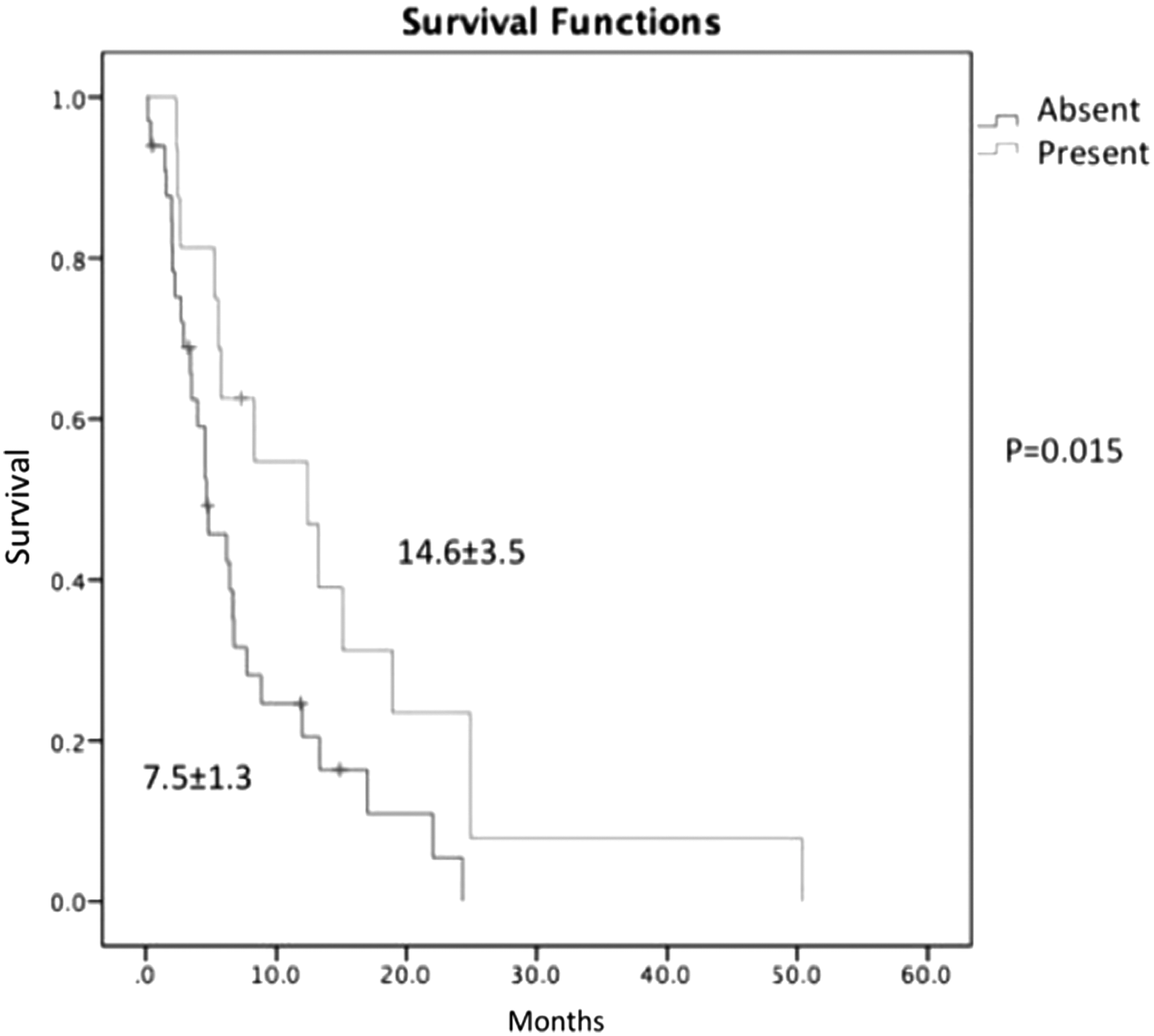
Survival curves of patients either with or without early metabolic response.
Discussion
Liver is the most common site of metastasis in CRC patients, and mortality and morbidity are mostly related with the presence of liver metastasis. Approximately 60% of CRC patients will have liver metastasis, of which less than 20% are suitable for surgical resection. 16 A large proportion of these patients do not respond or become chemorefractory, despite the newer chemotherapeutic agents. 17 In these patient groups, locoregional treatments are effective treatment options for control of liver metastasis. SIRT with 90Y microspheres is a promising method in primary and metastatic liver tumors with prolonged survival and limited toxicity. 18 In CRC patients, SIRT has been associated with an improvement in survival in salvage conditions. 19
The findings of this study suggest that the initial SUV (0.004) of liver metastases and the early metabolic response (p = 0.015) after treatment have significant effects on overall survival. Similarly, Gulec et al. 20 found that patients with 18F-FDG-PET response had longer survival periods than those without response. Beyond metabolic response evaluation, the authors found that the baseline SUV of liver lesion also has a prognostic role. SUV in 18F-FDG-PET/CT is highly correlated with tumor differentiation and has been identified as a prognostic factor in most solid tumors. In this analysis, overall survival times after SIRT were 10.03 ± 1.61 months, similar with previous reports of 4.5–17 months overall for progression-free survival times after SIRT. 5 –7,21
In routine oncological practice, response evaluation with RECIST criteria is considered the gold standard. 22 However, because these criteria were based on the change in tumor size, they have limitations in the evaluation of therapies that lead to tumor necrosis, resulting in an increase in tumor size. 21 This is the case with SIRT, in which tumor shrinkage can take several months. For this reason, Tochetto et al. 23 suggested the use of a different radiological parameter in ceCT to evaluate the treatment response after SIRT. They have reported that early change in attenuation of liver metastases may predict the 18F-FDG-PET responses, which is currently accepted as gold standard in the early evaluation of response to anticancer therapies in a variety of solid tumors. Moreover, metabolic response in 18F-FDG has a prognostic role. 24 –28 Widely accepted standardized metabolic response criteria include the European Organization for Research and Treatment of Cancer (EORTC) and PET response criteria (PERCIST). In this study, the authors used the PERCIST criteria and found that the presence of early metabolic response has a prognostic role after SIRT in CRC liver metastasis. Zerizer et al. 13 compared early metabolic response with EORTC criteria, RECIST, and tumor density criteria as predictors of progression-free survival after SIRT and found that early response assessment is superior to RECIST criteria and tumor density.
Although SIRT could be administered to patients with limited extrahepatic disease in the case of liver dominant disease, as well as liver only disease, another significant parameter in this analysis was the presence of extrahepatic metastasis. Clearly, these patients represent a cohort with a higher tumor burden with systemically disseminated disease. Thus, these patients, with a higher number of extrahepatic metastases, were already representing a riskier group. The results suggest that this may be an important consideration in the patient selection for SIRT. SIRT could be applied in combination with systemic treatments to improve disease control in the presence of extrahepatic disease.
Unlike Damm et al., 8 the authors did not find prognostic importance for lesion number and tumor load. This maybe be the result of selective SIRT treatment, similar with anatomical liver surgery targeting multiple lesions in the same lobe, which may be effective in controlling the disease. However, this should be considered cautiously because of the limited number of patients in this analysis.
A major limitation of this study was its retrospective design, with potential bias in patient selection. However, the authors gathered a multidisciplinary team and a relatively higher number of patients representing evolution of the authors' clinical experience within the study period.
Conclusion
This study suggests that patients with CRC liver metastasis who have lower SUV at presentation and early metabolic response have better outcomes after SIRT.
Footnotes
Disclosure Statement
No competing financial interests exist.