
Abstract
Objectives:
Biodistribution of antibodies is vital to successful immunoscintigraphy/immunotherapy, and it is assumed to be similar to antigen distribution. We measured and compared the binding pattern of radiolabeled antibody to tissue antigen distribution in a nude mouse xenograft model of human melanoma.
Methods:
We transplanted 107 FEM-XII human melanoma cells into the right flank of five nude mice. For the control, we transplanted 5 × 106 LS174T human colon cancer cells into the left flank. Two weeks later, 10 μCi of 131I-labeled melanoma-associated 96.5 monoclonal antibody (targeting p97 antigen) was intravenously injected. Three days later, we sacrificed the mice and evaluated 96.5 antibody binding and concentration in the tumors by ex vivo quantitative autoradiography (QAR). Two months later, we incubated adjacent tumor tissue slices in various concentrations of 125I-labeled 96.5 MoAb and evaluated the distribution/concentration of p97 antigen by in vitro QAR.
Results:
p97 antigen distribution was homogeneous in the tumors (total antigen concentration [Bmax] = 17.36–38.36 pmol/g). In contrast, radiolabeled 96.5 antibody binding was heterogenous between location within the tumor (estimated bound antigen concentration = 0.7–6.6 pmol/g). No quantifiable parameters were found to be related with radiolabeled antibody binding and tumor antigen distribution. Antibody-bound tumor antigen to total antigen ratios ranged between 2% and 38%.
Conclusions:
Heterogeneous features of target antibody binding were observed in contrast to relatively homogenous feature of tumor antigen. We did not identify any correlations between p97 antigen distribution and 96.5 antibody binding in melanoma tissue. Radiolabeled 96.5 antibody binding patterns within melanoma cannot be predicted based on p97 antigen distribution in the tumor, which needs to be further studied with several other methods and more subjects in the future.
Introduction
Targeted strategies for cancer management which is unique to a subgroup patient are referred as personalized therapy. 1,2 Monoclonal antibodies (MoAbs) have been used as representative target agents since the 1980s. Therapeutic studies using radiolabeled MoAbs have reported objective and often dramatic transient tumor responses. 3,4
However, many promising targeted therapeutic agents had disappointing results when clinically applied. 5 This may be due to several biological factors that can inhibit ligand binding to target cells, which affects therapeutic response and prognosis. 6 Especially, antibody binding is critical for successful immunoscintigraphy and immunotherapy. Several factors influence antibody binding, including immunoreactivity (most important in theory), radiolabeled antibody affinity, tumor blood flow, tumor vascular permeability, and so on. 7 Among them, the most critical factors are thought to be local concentration and target antigen distribution. 8
Antigen distribution can be easily identified by immunohistochemical (IHC) analysis. However, molar concentration of antigen cannot be evaluated. Western blot is one of the semiquantitative methods, but distribution cannot be assessed. Del Vecchio and Reynolds 9 invented the measurement method of antigen concentration (in vitro quantitative autoradiography [QAR]], and some reports have confirmed the methods. 10 –12 In theory, the molar concentration and binding of antigen in tumor tissue can be identified by in vitro QAR, and molar concentration and distribution of local antibody in tumor tissue can be evaluated by ex vivo QAR. Until now, as far as we know, there is no report on binding and quantification studies of antibody according to antigen distribution and concentration.
In this study, we aimed to compare tumor antigen distribution and radiolabeled antibody-binding patterns in a nude mouse xenograft model of human melanoma. We quantitatively measured p97 antigen distribution and radiolabeled 96.5 antibody binding (targeting p97 antigen) in melanoma tissues and compared them by in vitro and ex vivo QAR, respectively.
Materials and Methods
MoAb and radioiodination
The 96.5 MoAb (Hybritech, Inc., San Diego, CA), a murine IgG2a antibody that reacts with the glycoprotein p97 antigen, is specific to human malignant melanoma. 13,14 The purified antibody was radioiodinated with 131I for ex vivo QAR and 125I for in vitro QAR studies (New England Nuclear, Boston, MA) using the chloramine-T method. 15 Specific activity of the labeled antibodies ranged from 0.68 to 0.86 mCi/mg.
Cancer cells and xenograft modeling
Human melanoma cells were purchased (FEM-XII; Frederick Cancer Research Center, Frederic, MD) and cultured in Dulbecco's modified Eagle's medium (DMEM; Invitrogen, Grand Island, NY) supplemented with 10% fetal bovine serum, 100 U/mL penicillin, and 100 g/mL streptomycin at 37°C in a humidified atmosphere containing 5% CO2. Subcutaneous injection of 107 FEM-XII human melanoma cells was administered in the right flank, and subcutaneous injection of 5 × 106 LS174T human colon cancer cells was performed in the left flank as a control for five 6-week-old nude mice. After 2 weeks, ex vivo QAR and preparation for in vitro QAR were performed.
Ex vivo QAR (measurement of 96.5 antibody binding and concentration)
The binding and concentration of 96.5 antibody binding in tumor was measured by ex vivo QAR. Mice were intravenously injected with 10 μCi (100 μg) of 131I-radiolabeled 96.5 MoAb (131I-96.5 MoAb). Seventy-two hours after 131I-96.5 MoAb administration, ex vivo QAR was performed for tumor tissues with diameters ranging from 0.5 to 1.1 cm, and excised melanoma tissues were weighed. We cut frozen 20 μm sections at −20°C in a cryomicrotome corresponding to the largest cross-sectional area of the tumor. Sections were dried by heating at 65°C and placed them in a light-tight cassette with 131I-calibrated standards and X-ray film (SB5; Kodak, Rochester, NY). We prepared 131I-calibrated standards using by modifying a previously described technique. 16 After 2 weeks of exposure, autoradiographic films were photographically processed, and images were digitized using a computerized scanning microdensitometer (P-1000 HS; Optronics International, Inc., Chelmsford, MA). We obtained optical density measurements within 50 × 50 μm elements of the autoradiographic images and stored via an online computer (POP 11/60; Digital Equipment Corp., Maynard, MA). Optical density measurements over the autoradiographed 131I standards were plotted against their respective levels of radioactivity, and a standard curve was generated using a polynomial fit of the data. 17
To quantify antibody concentrations, regions of interest were drawn over selected tissue areas and regional optical density measurements were converted to μCi/g of tissue using the standard curve. We drew a large region of interest over the entire tumor area to obtain the mean radioactivity count per gram of tumor (μCi/g). We selected two smaller areas around the tumor regions with the highest and the lowest optical density measurements, which corresponded to the highest and lowest levels of radioactivity in the tumor, respectively. Final autoradiographic results were decay corrected for the 72 hours of interval (between 131I-96.5 MoAb administration and ex vivo QAR) so that the values obtained reflected activity. The same analyses were performed on control tumors and normal tissues (muscle and blood) and calculated the tumor-to-control, tumor-to-muscle, and tumor-to-blood ratios. Concentration of estimated bound antigens in each tumor was determined by converting to moles of antibody per grams of tumor (pmol/g) from the specific activity of 131I-96.5 MoAb. In addition, we visually and quantitatively (using frequency histogram) evaluated the distribution of radiolabeled antibody.
In vitro QAR (measurement of p97 antigen distribution and concentration)
p97 antigen distribution and concentration of melanoma specimens were evaluated using 125I-radiolabeled 96.5 MoAb (125I-96.5 MoAb). 10 Sections collected for in vitro QAR were adjacent to those sampled for ex vivo QAR. Two months after ex vivo QAR, adjacent tissue slices were incubated in various concentrations of 125I-96.5 MoAb. We then divided the tissue sections from each tumor into two groups to be used in two different assays: (1) total binding of specific antibody and (2) nonsaturable binding of specific antibody. We fixed sections in 0.25% glutaraldehyde for 20 minutes. We incubated sections in the nonsaturable binding group with unlabeled antibody for 30 minutes (1.3, 2.6, 5.2, 10.4, 20.8, 41.6, and 83.3 nmol/L). We incubated all sections for 30 minutes in a solution containing 2% bovine serum albumin and 10% chicken serum albumin in phosphate-buffered saline (PBS) to reduce the radiolabeled antibody's nonspecific binding. We then incubated individual sections for 60 minutes in a solution of 125I-96.5 MoAb at concentrations ranging from 1.3 to 83.3 nmol/L (1.3, 2.6, 5.2, 10.4, 20.8, 41.6, and 83.3 nmol/L). After incubation, we washed all slides with PBS and dehydrated them with ethanol. We prepared an autoradiographic standard for each tumor specimen using 125I-labeled human serum albumin, as described in a previous study. 18 We exposed total antibody-bound and nonsaturable antibody-bound tissue sections to X-ray film (SB5; Kodak) for 2 days. We digitized autoradiographic films using a scanning microdensitometer (Amersham, Arlington Heights, IL). We plotted the optical density measured from the 125I-labeled human serum albumin standard against the specific activity of each standard and used polynomial fitting of these data to provide a standard curve. We obtained the mean optical density of the selected region and determined the concentration of the radiolabeled antibody in the tumor from the standard curve. We used computer analysis of specific antibody binding to quantitate the maximum value, which was the same as the p97 antigen concentrations in the whole tumor. In addition, we evaluated the distribution of the p97 antigen visually and quantitatively (using a frequency histogram).
Analysis of binding activity data
We analyzed the data from the saturation studies using the nonlinear least-squares fitting method.
12
We used two separate equations to analyze the saturation curve to obtain values for the maximum amount of bound antibody (Bmax) and the dissociation constant (Kd). The parameters Bmax and Kd were made using the RS-1 curve modeling program (BBN Software Products Corporation, Cambridge, MA). The first equation was a saturation plot (Fig. 1A);
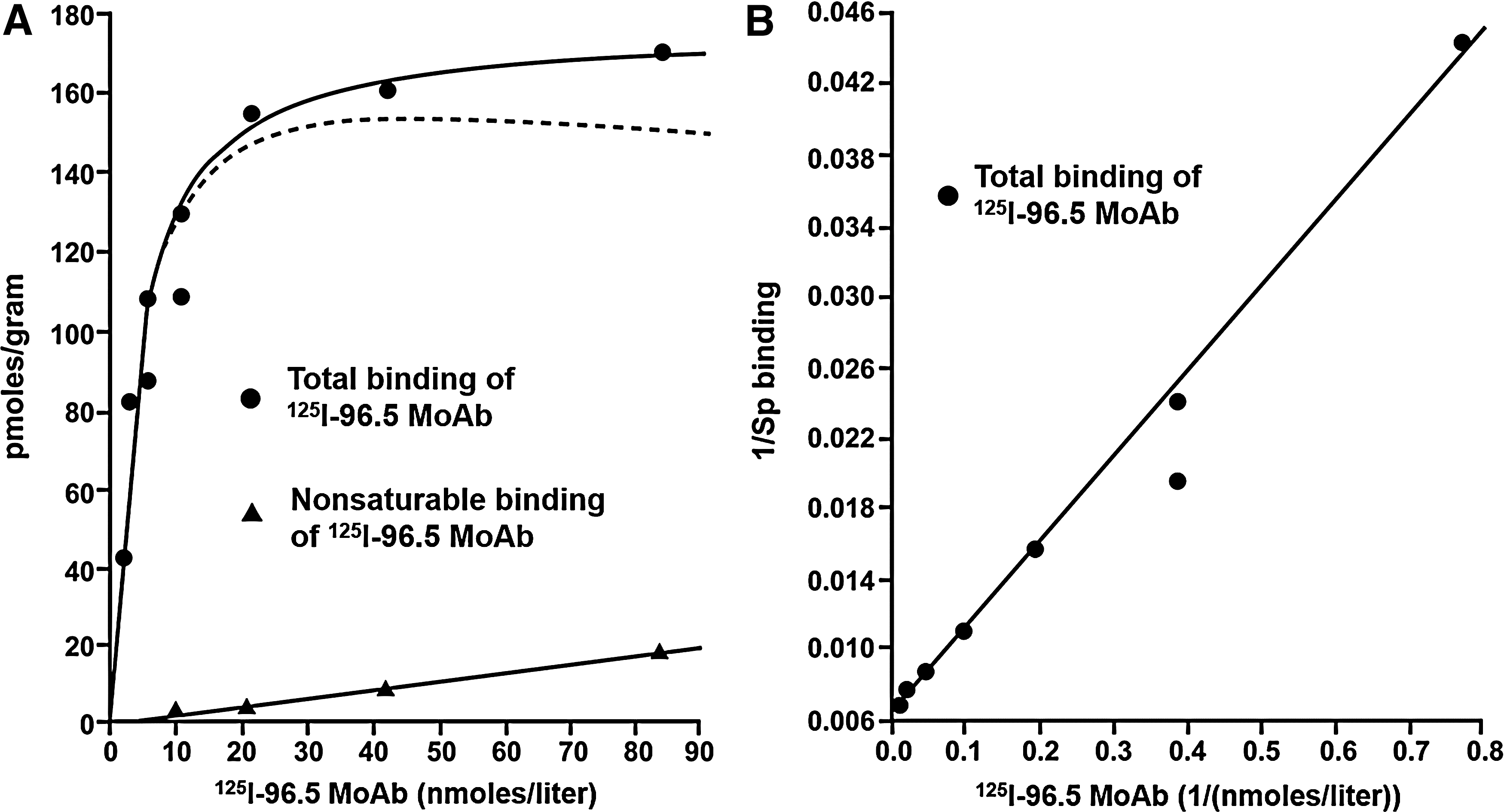
Analysis of binding activity data. Binding curves based on saturation studies
Bmax is the maximum amount of 125I-96.5 MoAb bound to the tissue; [Ab] is the concentration of 125I-96.5 MoAb in the incubation media; Kd is the antigen/antibody dissociation constant, and a is the slope of the nonsaturable curve. We obtained specific binding by subtracting the nonsaturable binding curve from the total binding curve.
The second equation was a double inverse plot between the specific binding data and the concentration of the labeled antibody (Fig. 1B);
Ka is the antigen/antibody affinity constant. A plot of 1/specific binding versus l/[Ab] will produce a straight line with the value at the y-intercept being equal to l/Bmax. Computer fitting of the curve gave the Bmax value, which is the maximum concentration of 125I-96.5 MoAb specifically bound to the tumor. We used the specific activity of 125I-96.5 MoAb to calculate the maximum pmol/g of antibody bound to the tumor (Bmax). We considered the concentration of bound antibody to be the same as the concentration of the total antigenic epitope.
Statistical analysis
Correlations between the concentration parameters of the antibody (e.g., specific activity, tumor-to-control ratio, tumor-to-muscle ratio, and tumor-to-blood ratio, estimated bound antigen concentration) and total antigen concentration (Bmax) in melanoma tissues were tested using Spearman's test. We considered p-values lower than 0.05 as significant.
Results
p97 antigen distribution and concentration
Distribution of the p97 antigen was generally homogeneous in melanoma tissue (Fig. 2A, C, E, G). Bmax (equivalent to total antigen concentration) of 125I-96.5 MoAb to sections of the melanoma tissues ranged from 17.36 to 38.69 pmol/g.

Autoradiographic images of melanoma tissues using radiolabeled (131I or 125I) MoAb 96.5 of mouse no. 1
96.5 antibody binding and concentration
Distribution of 96.5 antibody was heterogeneous in melanoma tissue. Even in samples with low antibody binding, some focal accumulation was observed (Fig. 2B, D, F, H). In addition, 96.5 antibody concentrations varied between tumors (0.14–1.24 μCi/g) (Table 1). We could not find any reasonable explanation for the antibody binding patterns observed. Estimated bound antibody concentrations ranged between 0.7 and 6.6 pmol/g.
Comparison of pathology, p97 antigen distribution and 96.5 antibody binding
Melanoma tissues were weighed between 330.2 and 807.2 mg. Individual distributions of antigens and antibodies differed based on frequency histogram analysis (Fig. 3). We could not find any significantly correlated parameters between total antigen concentration (Bmax; between 17.36 and 38.36 pmol/g) and antibody-bound antigen concentration (e.g., specific activity of antibody, tumor-to-control ratio, tumor-to-muscle ratio, tumor-to-blood ratio, and antibody-bound antigen concentration). Ratios of antibody-bound antigen to total antigen (100 × estimated bound antigen divided by Bmax) were quite variable (ranged between 2% and 38%) (Table 2).
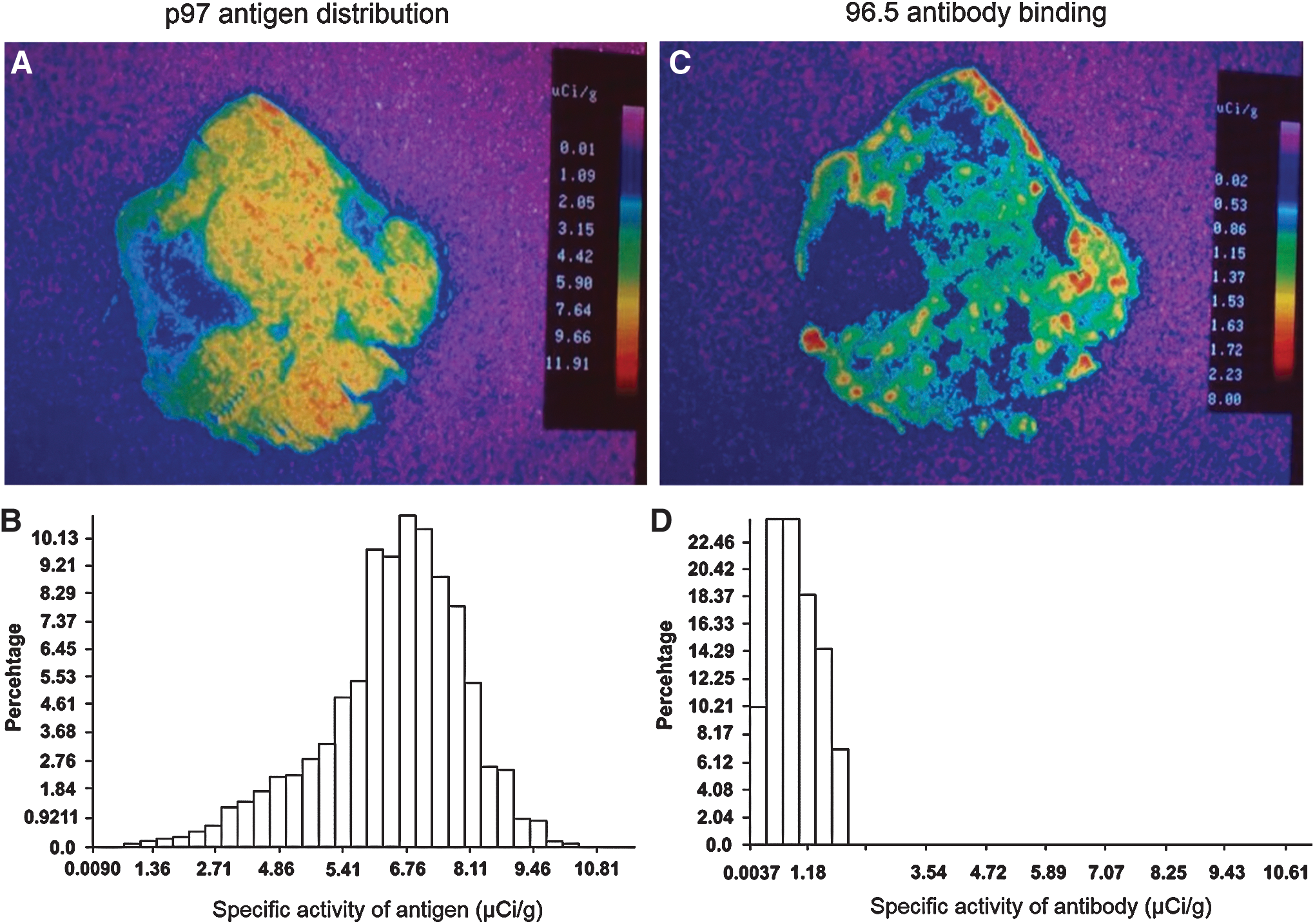
Comparison of in vitro and ex vivo QAR using frequency histogram (mouse no. 3). Distribution of p97 antigen in melanoma tissue was generally uniform based on in vitro QAR
(-) means could not calculate tumor-to-control ratio due to no growth of control.
Discussion
In this study, we found that 96.5 antibody binding was heterogeneous even though p97 antigen distribution was generally homogenous in human melanoma tissue. In addition, 96.5 antibody and p97 antigen concentrations in melanoma tissue did not correlate. Tumor antigen concentration, which has been considered to affect absolute antibody uptake, did not influence antibody uptake. This study was a basic research of targeted therapy for treatment response prediction.
Autoradiography can provide information regarding antibody distribution. Photosensitive regions of autoradiographic images reflect the location of radioactive material. 18 QAR is an established method to perform quantification with less than 5% of coefficient of variance. 19 And QAR can detect local concentrations of antigen (in vitro) 20 and radiolabeled antibody (ex vivo) 21 in tumors, which cannot be assessed by IHC analysis. Especially, QAR is helpful to compare directly between antigen and antibody concentration in the same tissue using dual radiotracers.
In vitro QAR has unique features. This is the only method to estimate the antigen concentration. It can determine the total antigen concentration and can observe the distribution of antigens (homogeneity or heterogeneity) within tumors. We also found that in vitro QAR showed homogenous expression of p97 in tumor tissue (Bmax range = 17.36–38.36 pmol/g). Results of immunoscintigraphy and immunotherapy might be affected by antigen density and distribution, which influence the tumor uptake of injected radiolabeled antibodies. Previous studies indicated that antibody localization is directly related to antigen concentration. 22,23
Ex vivo QAR yields useful data, which can define specific activity of antibody and provide information about antibody localization. We showed that tumor uptake of 131I-96.5 MoAb on melanoma tissue was not uniform, but patch and heterogenous. 96.5 antibodies were more concentrated in certain areas. Variability in tumor uptake of injected radiolabeled MoAb, which could account for differences in sensitivity, was reported by many authors in clinical studies using several types of MoAbs, according to antibody dose, interstitial pressure, and so on. 24 –28 In addition, the difference of tumor uptake and penetration according to different forms of radiolabeled antibodies also should be considered. 29
Our direct comparison study of antigen distribution and antibody binding showed no significant correlations, and ratios between antibody-bound antigen and total antigen were small and variable between mice (range = 2%–38%). In addition, 96.5 antibody binding was localized, while p97 antigen distribution was homogenous in frequency histogram analysis. Possible reasons for these findings included mainly vascular factor, such as nonuniformity of tumor vascularization, low vessel permeability due to large molecular weight antibodies, and low blood flow in the interstitial tissue due to large tumor size. We thought that vascular factor is especially important for discrepancy of antigen distribution and antibody binding. When tumor enlarges, tissue pressure might inhibit the effective antibody binding to tumor. Another possible reason might be due to nonsatisfactory immunological factors such as low avidity of antibody and low expression of antigen. The usual MoAbs have around 109 mol/L affinity constant. In this study, affinity constant was around 108 mol/L (between 0.78 × 108 mol/L and 1.70 × 108 mol/L). In addition, the usual concentration of tissue antigen was around 150–600 pmol/g in our previous in vitro QAR study. 20 In this study, tissue concentration was less than 50 pmol (between 17.36 and 38.36 pmol/g).
We suggest that antibody binding studies can be performed for targeted antibody therapy, and methods to improve targeted antibody binding should be considered in low efficiency cases. Smaller molecular weight antibodies, such as diabody or minibody, can be used rather than whole antibody when size of the antibody is an issue. And local thermal therapy and/or local radiation therapy can be performed to improve permeability. Recent ex vivo autographic studies on microdistribution and the kinetics of intratumoral penetration can be alternatives for accurate analysis of tumor antibodies. 30 In the aspect of antibody affinity, there are many studies that higher affinity antibody may not lead to greater tumor uptake, 31 and can cause lower tumor penetration due to binding-site barrier, 32 which we should consider for the future study. In the future, therapy based on lesion characteristics (lesionalized therapy) in addition to personalized therapy should be determined based on the heterogeneous, discordant features of tumor antibody distribution. 33
There are some limitations to our study. First, the number of studied mice was small, which induces large variation of radiolabeled antibody uptake compared with previous study. 34 Second, optimal dose and timing should be evaluated for ex vivo QAR. Although we used 10 μCi of 131I-96.5 MoAb (equivalent or more to maximum dose to human) and performed ex vivo QAR after 72 hours of injection (same imaging time with human 131I treatment), somewhat different result could be drawn using other dose and timing. Finally, the effect of deiodination, which could disrupt the relationship between tumor uptake of radiolabeled antibody and p97 antigen expression, can be a confounding factor. Direct in vitro and ex vivo comparison study with a larger subjects are required in the future to confirm our results.
Conclusion
In conclusion, p97 antigen distribution and concentrations did not reflect the 96.5 antibody binding and concentration. 96.5 antibody localization varied between tumors and was locally different within individual tumors.
Footnotes
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant for the Global Core Research Center (GCRC) funded by the Korean government (Ministry of Science, ICT & Future Planning; MSIP) (No.2011-0030001). The authors thank James C. Reynolds (Department of Nuclear Medicine, National Institutes of Health) for assistance with our study.
Disclosure Statement
No competing financial interests exist.