
Abstract
Aim:
To define the role of 18F-flourodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) in the detection of bone marrow (BM) involvement in patients with diffuse large B cell lymphoma (DLBCL).
Materials and Methods:
Fifty-four (mean age: 55.5 ± 18.3 years, 20 female and 34 male) DLBCL patients who underwent pretreatment 18F-FDG PET/CT were included to the study. Focal or diffuse BM 18F-FDG uptake that is higher than mediastinal blood pool uptake was accepted as positive. After staging of disease by CT and 18F-FDG PET/CT, all the patients received R-CHOP treatment after diagnostic blinded bone marrow biopsy (BMB). Presence of positive BM uptake in 18F-FDG PET/CT and histopathological examination results of BMBs were analyzed by Chi-square test. Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of 18F-FDG PET/CT in the detection of BM involvement were calculated. Prognostic importance of the presence of BM 18F-FDG uptake was analyzed by Kaplan–Meier analysis.
Results:
BM 18F-FDG uptake was detected in 8 patients. Histopathological examination of BMB revealed BM involvement in 6 out of 8 patients. BMB was negative in all patients who have no 18F-FDG uptake in the evaluation of PET/CT images. Sensitivity, specificity, accuracy, PPV, and NPV of 18F-FDG PET/CT in the detection of BM involvement were calculated as 100%, 96%, 96%, 75%, and 100%, respectively. In the Kaplan–Meier analysis, we found that presence of pretreatment 18F-FDG uptake in BM has a prognostic importance. Whereas mean time to progression (TTP) in patients with BM uptake was 32.25 ± 10.9 months and mean TTP in those without was 51.69 ± 3.6 months (p = 0.013).
Conclusions:
BM uptake in pretreatment 18F-FDG PET/CT is an important prognostic factor in DLBCL patients. Moreover, in consideration of high NPV, 18F-FDG PET/CT could eliminate unnecessary BMB in FDG-negative patients.
Introduction
Diffuse large B cell lymphoma (DLBCL) is the most common non-Hodgkin lymphoma (NHL) subtype and it accounts to 30%–35% of the patients. 1 Presence of bone marrow (BM) involvement is an important prognostic factor because its presence effects disease stage and has a prognostic role. 2 BM assessment could be performed by bone marrow biopsy (BMB). European Society of Clinical Oncology (ESMO) guidelines recommend blind BMB in all patients who were diagnosed with DLBCLs and were candidates for curative treatments. 3 However, BMB is a painful and invasive process and it may be false negative because it represents a small proportion of BM. 4 –8 For this reason, its routine performance has been controversial. 9
18F-flourodeoxyglucose (18F-FDG) positron emission tomography (PET)/computed tomography (CT) is the method of choice in DLBCL patients to evaluate disease spread because most of the DLBCLs are FDG positive. 10 The role of 18F-FDG PET/CT in the evaluation of BM involvement is controversial. 11 –13 Some of the reported studies included were mixed types of NHLs with combination of low and high 18F-FDG avid tumors and some were performed by PET-only systems. 14 In a recent meta-analysis and review, Adams et al. reported that sensitivity and specificity of 18F-FDG PET/CT in the detection of BM involvement were 88.7% and 99.8%, respectively, from pooled data. They suggested that 18F-FDG PET/CT is accurate and complementary to BMB in the evaluation of BM involvement in DLBCL patients. 13
In this study, we aimed to review our results in the evaluation of BM involvement in DLBCL patients who underwent 18F-FDG PET/CT followed by BMB.
Materials and Methods
Patients
Retrospectively, 18F-FDG PET/CT images of 54 (mean age: 55.5 ± 18.3, 20 female and 34 male) patients who underwent PET/CT for staging of disease after histopathological confirmation of DLBCL were included in the analysis. Patient follow-up data were searched to detect presence of disease progression and progression-free survival times. Mean follow-up period was 66.57 ± 15.4 months.
Evaluation of BM 18F-FDG uptake
PET/CT images were acquired using a GE Discovery ST PET/CT (General Electric, Milwaukee, WI) scanner. Whole body 18F-FDG PET/CT imaging was performed ∼1 hour after an intravenous injection of 8–10 mCi 18F-FDG. Images from the vertex to the proximal femur were obtained while the patients were in the supine position. Emission PET images were reconstructed with noncontrast CT images that were also obtained from the patient's integrated 18F-FDG PET/CT with the use of a standardized protocol of 140 kV, 70 mA, tube rotation time of 0.5 second per rotation, a pitch of 6, and a slice thickness of 5 mm. PET/CT images were evaluated and confirmed visually and semiquantitatively with standardized uptake value by consensus of two experienced nuclear medicine specialists. Focal or diffuse BM 18F-FDG uptake that is higher than mediastinal blood pool uptake was accepted as positive.
Data and statistical analyses
SPSS software (version 20.0; SPSS, Inc.; Chicago, IL) was used for statistical analysis. Continuous data are expressed as the mean and standard deviation or as the median and interquartile range. Categorical data are presented as number of patients and percentages. Presence of positive BM uptake in 18F-FDG PET/CT and histopathological examination results of BMBs were analyzed by Chi-square test. Sensitivity, specificity, accuracy, positive predictive value (PPV) and negative predictive value (NPV) of 18F-FDG PET/CT in the detection of BM involvement were calculated. Prognostic importance of the presence of BM 18F-FDG uptake was analyzed by Kaplan–Meier analysis.
Results
While 34 out of 54 patients had been diagnosed with lymph node, 20 patients had been diagnosed with extra-nodal organ biopsies (soft tissue, 5 bowel, 5 stomach, 3 tonsil, 3 nasopharynx, 1 bone, 1 spleen, 1 and lung 1 ). Disease stages were I, II, III, and IV in 14, 10, 7, and 23 patients, respectively. Mean serum LDH level was calculated as 296 ± 43.7 U/L (range 82–1489). Demographic data of patients is demonstrated in Table 1.
LDH, lactate dehydrogenase.
In 18F-FDG PET/CT images, while extranodal FDG uptake was seen in 36 (67%) patients (stomach in 6, lung in 6, spleen in 6, skin soft tissue in 6, liver in 4, bowel in 4, tonsil in 4, nasopharyngeal region in 3, pancreas in 3, thyroid in 2, peritoneum in 1 patients), BM uptake was observed in 8 (15%) patients. BM 18F-FDG uptake was detected in 8 patients. Histopathological examination of BMB revealed BM involvement in 6 out of 8 patients. BMB was negative in all patients who have no 18F-FDG uptake in the evaluation of PET/CT images. Sensitivity, specificity, accuracy, PPV, and NPV of 18F-FDG PET/CT in the detection of BM involvement were calculated as 100%, 96%, 96%, 75%, and 100%, respectively. Findings of 18F-FDG PET/CT and BMB are summarized in Table 2. PET/CT images of patients with false and true positive BM 18F-FDG uptake are shown in Figures 1 and 2.
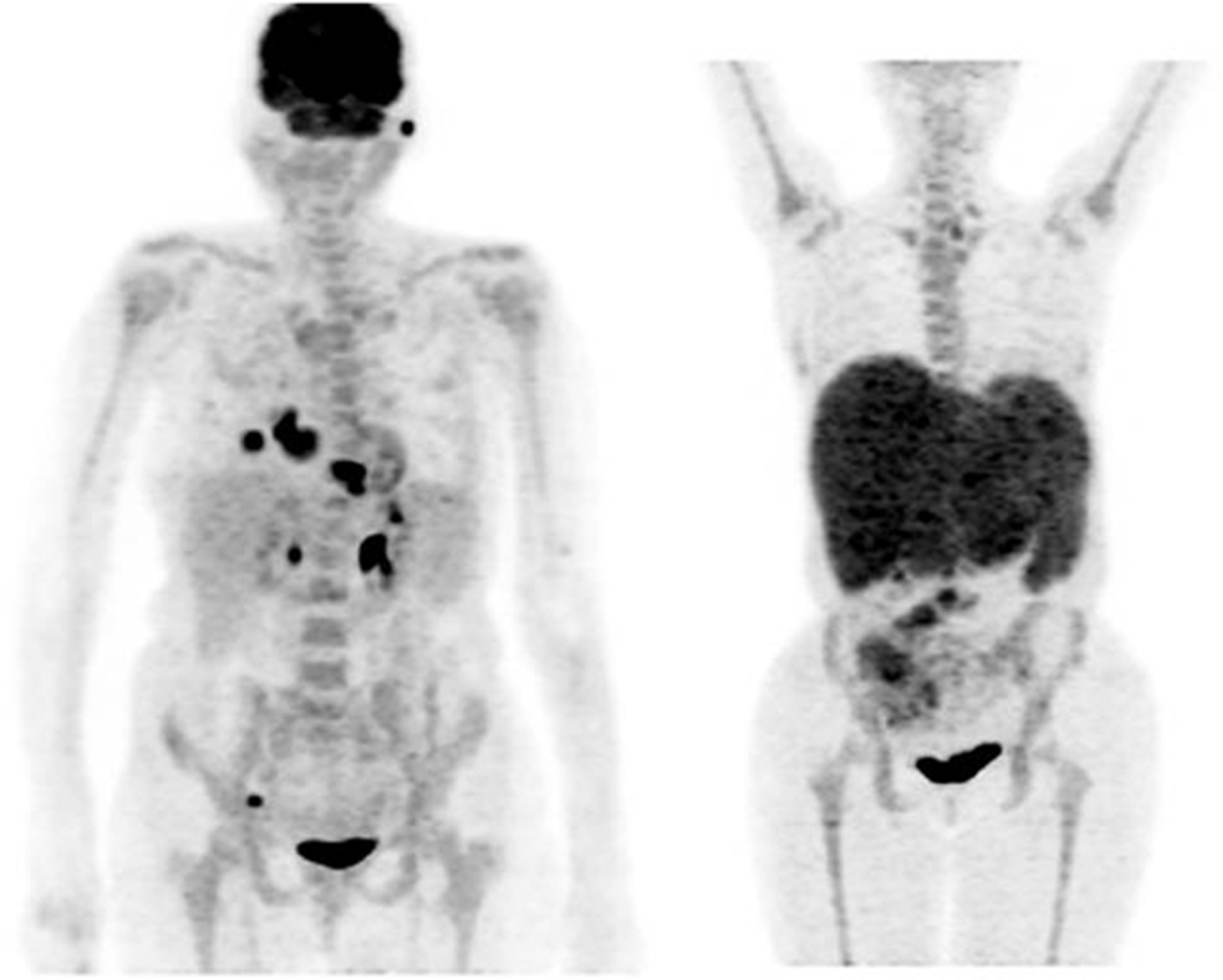
Maximum intensity projection PET/CT images of two patients with true positive BM 18F-FDG uptake. BM, bone marrow; 18F-FDG, flourodeoxyglucose; PET/CT, positron emission tomography/computed tomography.

Maximum intensity projection PET/CT image of one patient with false positive bone marrow 18F-FDG uptake.
BMB, bone marrow biopsy; 18F-FDG, flourodeoxyglucose; PET/CT, positron emission tomography/computed tomography.
Disease progression was seen in 14 (25%) patients during the 66.57 ± 15.4 months mean follow-up period. In Kaplan–Meier analysis, we found that presence of pretreatment 18F-FDG uptake in BM has a prognostic importance. Whereas mean time to progression (TTP) in positive BM patients with bone uptake was 32.25 ± 10.9 months and mean TTP in those without was 51.69 ± 3.6 months (p = 0.013) (Table 3 and Fig. 3).
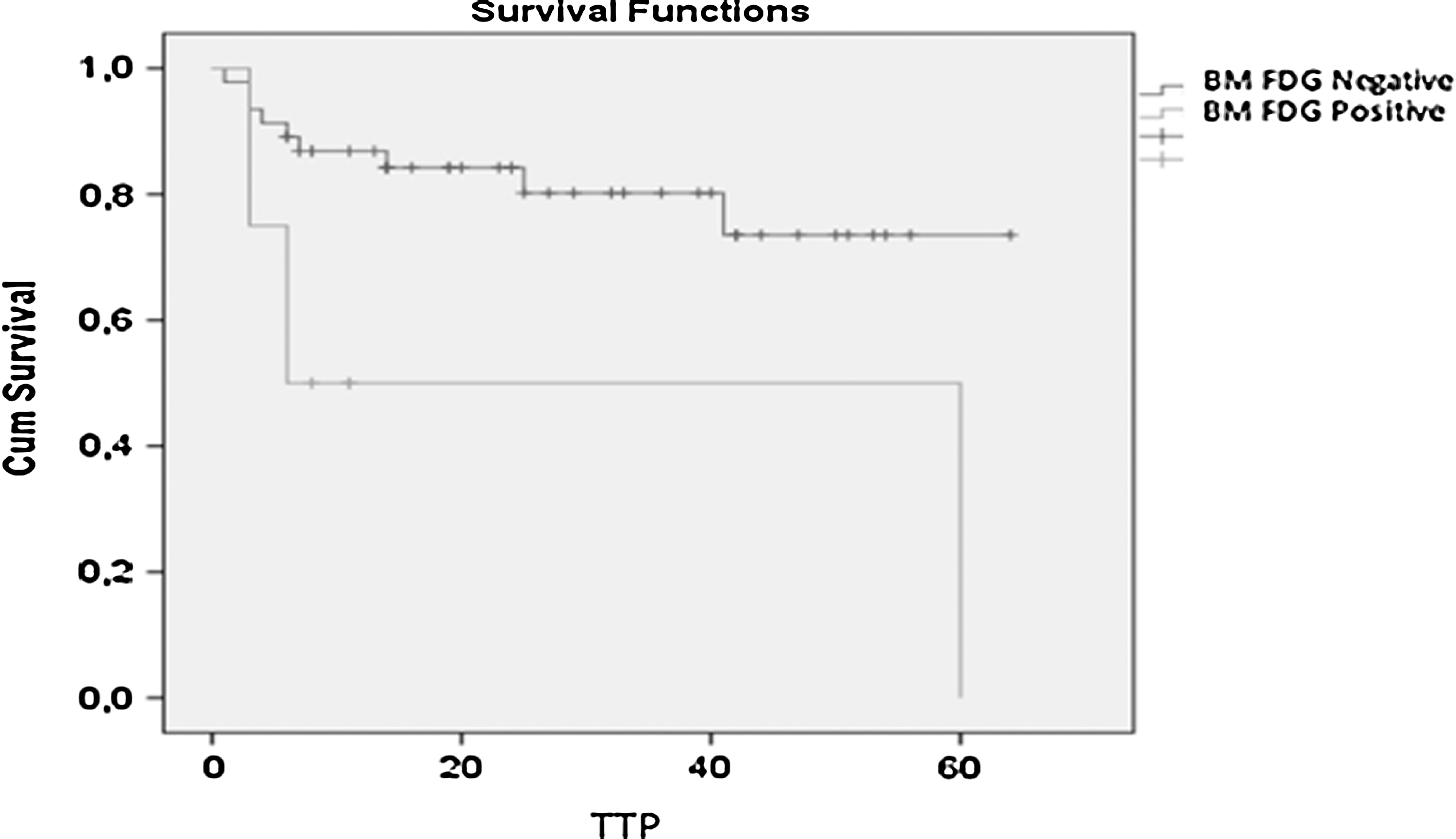
Survival cures for TTP in BM FDG (+) and (−) groups. TTP, time to progression.
BM, bone marrow; FDG, flourodeoxyglucose; TTP, time to progression.
Discussion
Presence of BM involvement is an important prognostic factor in NHL patients. For this reason, current ESMO guideline recommends blinded BMB in all new diagnosed DLBCL patients. But, BM infiltration by DLBCLs can be patchy, and because of the skip areas, it is really difficult to document BM involvement by routine BMB. Performing that invasive and painful intervention in all patients is controversial and has been the subject of debate in the past decade. 9 Adams et al. reviewed studies in this subject and published their meta-analysis. They found that 18F-FDG PET/CT achieves good sensitivity and almost perfect specificity in the detected of BMB in new diagnosed DLBCL patients. However, they revealed that 18F-FDG PET/CT can miss bone marrow involvement (BMI) in ∼3.1% of patients. Finally, they concluded that if 18F-FDG was negative in patients, BM involvement cannot be excluded. 13 Similarly, their pooled data results we calculated high sensitivity and specificity of 18F-FDG PET/CT in the detection of BMI in their series. Differently from their suggestion, in our series, 18F-FDG PET/CT did not miss BMI in any patient. This may be related to difference between criteria for BM positivity during design of the studies. Although interpretation criteria have not been reported in some studies, they have been accepted BM uptake higher than liver in the others. 14 –19 In our analysis, we accepted positive BM uptake higher than mediastinal blood pool. For this reason,18F-FDG PET/CT could have missed the BMI in those cases. In contrast, our lower threshold could increase false positivity of 18F-FDG PET/BT. Therefore, we recommend BMB for confirmation of positive BM 18F-FDG PET/BT in case of possible false positivity.
Cheson et al. reported the recommendation of an international multidisciplinary workshop. They suggested incorporation of 18F-FDG PET/CT into standard staging of FDG avid lymphomas. Moreover, they reported that BMB is no longer indicated for the routine staging of Hodgkin lymphomas and most DLBCLs. Results of our analysis may reveal that patients without BM 18F-FDG uptake could be treated and followed up without BMB. 20
The low and statistically significant TTP in BM FDG-positive patients in our study can also emphasize the importance of close follow-up in these patients. With further evaluation, BM involvement may be considered as a risk factor for early relapse and a closer follow-up schedule can be offered for these patients. New studies are needed to support this hypothesis.
Conclusions
BM uptake in pretreatment 18F-FDG PET/CT is an important prognostic factor in DLBCL patients. Moreover, in consideration of high NPV, 18F-FDG PET/CT could eliminate unnecessary BMB in FDG-negative patients.
Footnotes
Disclosure Statement
No competing financial interests exist.