
Abstract
The optimal palliative treatment for unresectable intrahepatic cholangiocarcinoma (ICC) remains controversial. While selective internal radiation therapy (SIRT) using yttrium-90 microspheres is a well-accepted treatment for hepatocellular carcinoma, data related to its use for locally advanced ICC remain relatively scarce. Twenty-nine patients (mean age 66 ± 11 years; 15 female) with unresectable biopsy-proven ICC treated with SIRT between June 2008 and April 2015 were retrospectively evaluated for post-treatment toxicity, overall survival, and imaging response using response evaluation criteria in solid tumors (RECIST) 1.1 criteria. RECIST 1.1 response was evaluable following 26 treatments [complete response (CR):0, partial response (PR):3; stable disease (SD):16, progression of disease (PD):7]. Objective response rate (CR+PR) was 12%. Disease control rate (CR+PR+SD) was 73%. Median time to progression was 5.6 [95% confidence interval (CI): 0–12.0] months. Median survival following SIRT was 9.1 (95% CI: 1.7–16.4) months. Post-treatment survival was prolonged in patients with absence of extrahepatic disease (p = 0.03) and correlated with RECIST 1.1 response (p = 0.02). Toxicities were limited to grade I severity and occurred following 27% of treatments. These findings support the safe, effective use of SIRT for unresectable ICC. Post-treatment survival is prolonged in patients with absence of extrahepatic disease at baseline. RECIST 1.1 response following SIRT for ICC is predictive of survival.
Introduction
Intrahepatic cholangiocarcinoma (ICC) is a malignancy arising from intrahepatic bile duct epithelium and represents the second most common primary liver malignancy after hepatocellular carcinoma (HCC). Age-adjusted incidence of ICC is increasing within the United States, rising from 0.32 per 100,000 in 1975–1979 to 0.85 per 100,000 in 1995–1999. 1,2 Surgical management offers the only potential for cure. However, due to an often clinically silent course many patients have locally advanced disease upon diagnosis, precluding surgical resection, and disease recurrence rates may be as high as 58% following resection. 3,4
Unresectable ICC carries a poor prognosis, with historical median survival <8 months with single-agent chemotherapy. 4 –6 Combination chemotherapy using gemcitabine and cisplatin has demonstrated improved median survival of 11.7 months; however, toxicity remains a concern, with overall severe (defined as either grade 3 or 4) toxicities per the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) occurring in 71% of cycles, including neutropenia in 25%. 4
External beam radiation therapy (EBRT) is an option for disease confined to a relatively small fraction of the whole liver volume. However, its use is limited in the presence of significant liver tumor involvement due to the risk of radiation-induced liver disease at whole-liver radiation exposure levels exceeding 40 Gy. 7 A recent single-center study evaluating ablative doses (median 58 Gy) of EBRT in tumors with a median size of 79 mm found a median overall survival (OS) from diagnosis of 30 months. 8
Locoregional therapy may offer the advantage of achieving ICC tumor control while minimizing systemic toxicities. A recent meta-analysis found that intra-arterial chemotherapy (IAC) achieved a median overall post-treatment survival of 22.8 (9.8–35.8) months with a lower rate of severe toxicity (35%) than dual-agent chemotherapy. 9 A separate meta-analysis evaluating transarterial chemoembolization (TACE) for unresectable ICC in 542 total subjects found a median post-treatment survival of 13.4 months. Severe toxicity rates following TACE were lower than either dual-agent chemotherapy or IAC, occurring in 19% of patients. 10
The optimal palliative treatment modality for unresectable ICC remains controversial. While selective internal radiation therapy (SIRT) using yttrium-90 (Y90) is a well-accepted treatment for HCC, 11 –13 data related to its use for locally advanced ICC remain relatively scarce. The goal of the present study is to evaluate the safety and efficacy of SIRT for treating locally advanced ICC.
Materials and Methods
Institutional review board approval was obtained before initiation of this review. All research-related activities were performed in compliance with Health Insurance Portability and Accountability Act. Informed written patient consent was obtained before all procedures.
Patient selection
Thirty-four patients with unresectable ICC were consecutively treated with selective internal radiation therapy (SIRT) using Y90 between June 2008 and April 2015. Of these, 5 patients without histopathological confirmation of ICC were excluded, yielding 29 patients (14 male, 15 female; age range 38–83 years; mean age 66 ± standard deviation 11 years) that were retrospectively reviewed.
Procedure details
All patients underwent standard planning arteriography to evaluate the vascular supply to the liver, including interrogation of the celiac and superior mesenteric arteries. Hepatoenteric anastomoses were coil embolized to prevent reflux of radioembolic material into nontarget viscera. Lung shunt fraction (LSF) was determined following administration of technetium-99-macroaggregated albumin, with a shunt fraction <20% considered acceptable for SIRT. 14
Y90 dosing was calculated using one of two methods, depending on which radioembolic agent was being employed. SIR-Sphere dose planning utilized the body surface area (BSA) method, which is based upon the assumption that liver size is proportional to total BSA (m2) and calculated as follows:
Where VTumor represents the tumor volume calculated from the baseline cross-sectional imaging and VLiver represents the liver volume free of tumor. The resulting raw calculated dose is then corrected for the degree of lung shunting by multiplying by a Lung Shunt Modifier (LSM) coefficient: LSM 1.0 for LSF <10%, LSM 0.8 for LSF 10%–15%, or LSM 0.6 for LSF 15%–20%. 15,16
TheraSphere dosimetry was calculated based upon a desired radiation treatment dose for a targeted portion of the liver (not necessarily equal to the tumor volume) using the following equation:
Where MLiver is the target liver mass in kg and R is the vial residual volume fraction following catheter administration of the radioembolic. 14
Administration of Y90 was accomplished during a second arteriography procedure and targeted either lobar, segmental, or subsegmental branches of the hepatic arteries depending on the tumor burden. Y90 radioembolic was injected through a microcatheter under intermittent fluoroscopic guidance, similar to the administration of chemoembolic. 17 The injection was considered to be complete when either the entire planned dose was successfully injected or vascular stasis was observed.
Following Y90 administration, patients underwent single-photon emission computed tomography (SPECT) within 6 hours to verify the target deposition of Y90 radioembolic as well as to quantify the actual radiation dose administered.
Radiation source
Y90 microspheres deliver radiation through the emission of β particles. Radioembolization of tumor arterial feeding branches using Y90 microspheres possesses the potential advantage of concentrating high radiation doses within the target lesion with relative sparing of normal liver parenchyma.
Two variations of Y90 microspheres are presently available in North America. SIR-Spheres (Sirtex Medical, Australia) are resin based and deliver 50 Bq per particle. TheraSpheres (BTG International, United Kingdom) are glass based and deliver 2500 Bq per particle.
In this series, 17 patients were treated with SIR-Spheres and 12 patients were treated with TheraSpheres. For each case, the selection of Y90 microsphere type was determined by operator preference.
Data collection: efficacy, toxicity, survival
All patients underwent an initial outpatient office visit, which included laboratory value assessment and imaging review. Treatment efficacy was determined by single observer (coauthor C.B.C.) blinded review of baseline and 90-day post-SIRT follow-up computed tomography (CT) and magnetic resonance (MR) imaging utilizing response evaluation criteria in solid tumors (RECIST) criteria version 1.1. Briefly, RECIST 1.1 defines four potential imaging-based outcomes, which are assessed by comparison of baseline and post-treatment surveillance imaging. Complete response (CR) is defined as complete disappearance of all lesions. Partial response (PR) is obtained with at least 30% reduction in sum of the longest diameter of all target lesions. Stable disease (SD) indicates a response meeting neither CR nor progression of disease (PD) criteria. PD is present when there exists at least a 20% increase in the sum of the longest diameters of all lesions. 18,19
Postprocedural adverse effects were assessed through 30 days from the date of Y90 administration by review of outpatient and inpatient medical records. OS was determined from medical records and calculated using Kaplan–Meier methodology. Survival data were censored for patient loss to follow-up or liver resection following SIRT. Median survival between subgroups was determined using the log-rank test.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20 (IBM Corp., Armonk, NY). A p-value <0.05 was considered to be statistically significant.
Results
Patient characteristics
Twenty-nine patients with unresectable histopathologically proven ICC were treated with SIRT. Eight patients were treatment naive upon undergoing SIRT. The remaining 21 patients had collectively received 25 prior treatment modalities before SIRT: surgery in 7 patients, chemotherapy in 15 patients, TACE in 1 patient, and EBRT in 2 patients. Mean time from the date of ICC diagnosis to Y90 treatment was 10.3 ± 11.3 months. Eastern cooperative group (ECOG) scores were 0 in 11 patients, 1 in 13 patients, and 2 in 5 patients.
Baseline and post-SIRT follow-up imaging were available in 26 of 29 patients for this retrospective review. The patients lacking available baseline and follow-up imaging could not be assessed with respect to RECIST 1.1 tumor response to Y90 treatment, but were included for the evaluation of safety and median OS. Disease burden included left hepatic lobe only in 4 patients, right hepatic lobe only in 12 patients, and bilobar disease in 13 patients. Extrahepatic disease was absent in 17 patients and present in 11 patients (all of whom had previously failed systemic chemotherapy). Mean longest tumor diameter was 68 ± 41 mm (Table 1).
Baseline imaging was unavailable for 1 patient.
Laboratory value was unknown for 1 patient.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ECOG, eastern cooperative group; ICC, intrahepatic cholangiocarcinoma; SD, standard deviation; TACE, transarterial chemoembolization; ULN, upper limit of normal.
There was no incidence of Y90 treatment abandonment or decrease in planned dosing due to excessive lung shunting. A total of 30 SIRT treatments were performed, with 1 patient undergoing two separate SIRT procedures. Mean radiation dose delivered was 1.64 ± 0.91 GBq.
Efficacy
Mean follow-up time was 8.4 ± 12.9 months. Treatment efficacy was assessed at 90 days post-SIRT with contrast-enhanced CT or MR, with baseline and post-treatment surveillance imaging available for comparison following 26 of the 30 treatments. PR was observed following 3 treatments (11.5%), SD following 16 treatments (61.5%), and PD following 7 treatments (26.9%).
One patient underwent post-SIRT ICC tumor resection, necessitating censoring from OS analysis at that time point. Eighteen patients (62%) had died at the time of study completion. Median OS from SIRT was 9.1 [95% confidence interval (CI): 1.7–16.4] months. Median OS from ICC diagnosis was 26.1 (95% CI: 12.8–39.4) months. Median OS was longer in patients with intrahepatic-only disease at baseline (13.9 months) as compared with patients with extrahepatic disease (6.8 months; p = 0.04). Median time to progression (TTP) was 5.6 (95% CI: 0–12.0) months (Table 2). Kaplan–Meier estimates of OS are included for the entire cohort (Fig. 1) and compared with respect to baseline metastatic disease (Fig. 2) and RECIST 1.1 response to SIRT (Fig. 3).
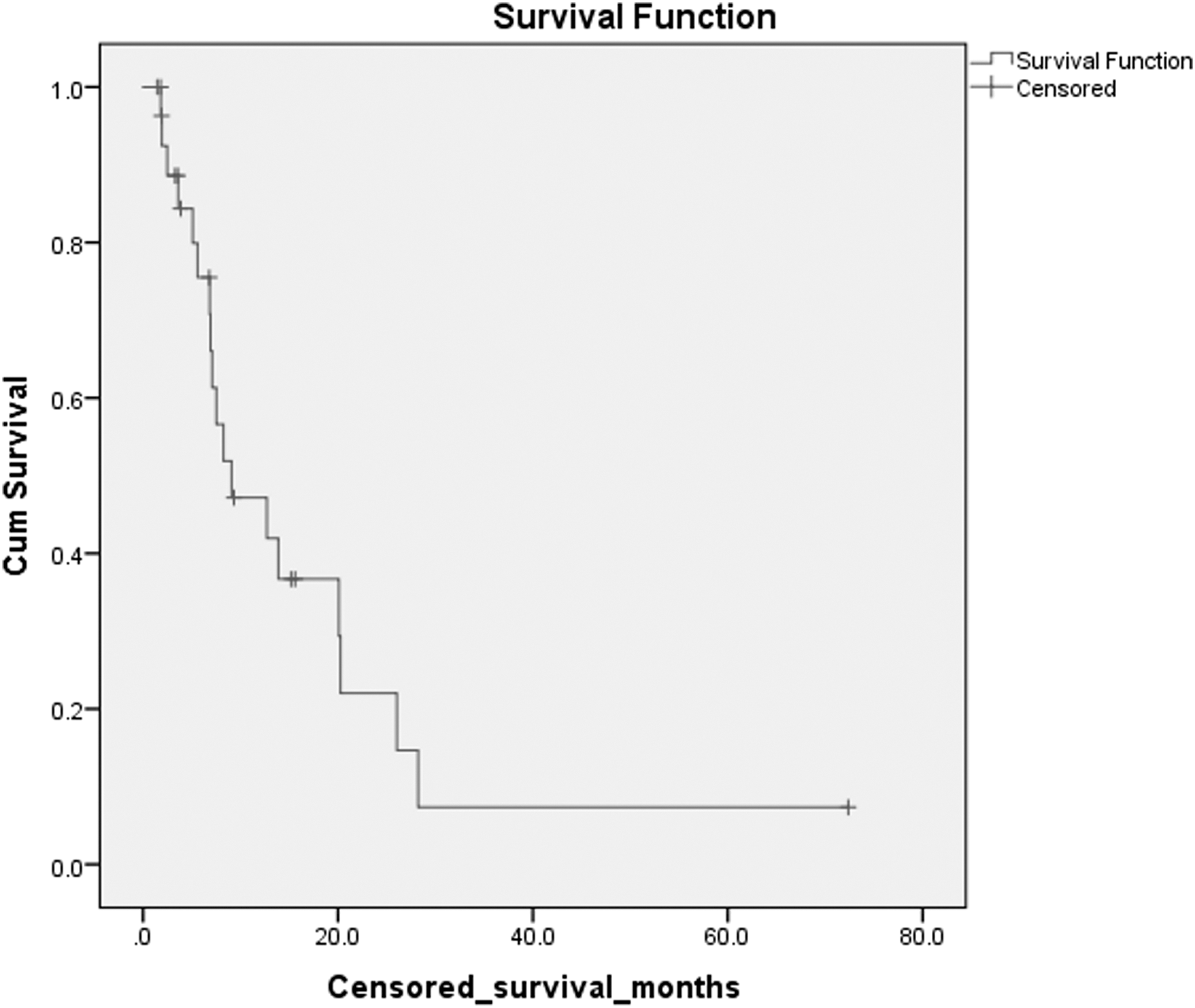
Kaplan–Meier curve for censored overall survival from first SIRT in 29 patients with unresectable ICC. ICC, intrahepatic cholangiocarcinoma; SIRT, selective internal radiation therapy.

Kaplan–Meier curve for censored overall survival from first SIRT in 26 patients with unresectable ICC stratified by RECIST 1.1 response. Curves 1, 2, and 3 represent partial response, stable disease, and progression of disease, respectively. Note that baseline and follow-up imagings were available for 26 of 29 patients; RECIST 1.1 response was unevaluable for 3 patients. PD, progression of disease; PR, partial response; RECIST, response evaluation criteria in solid tumors; SD, stable disease.
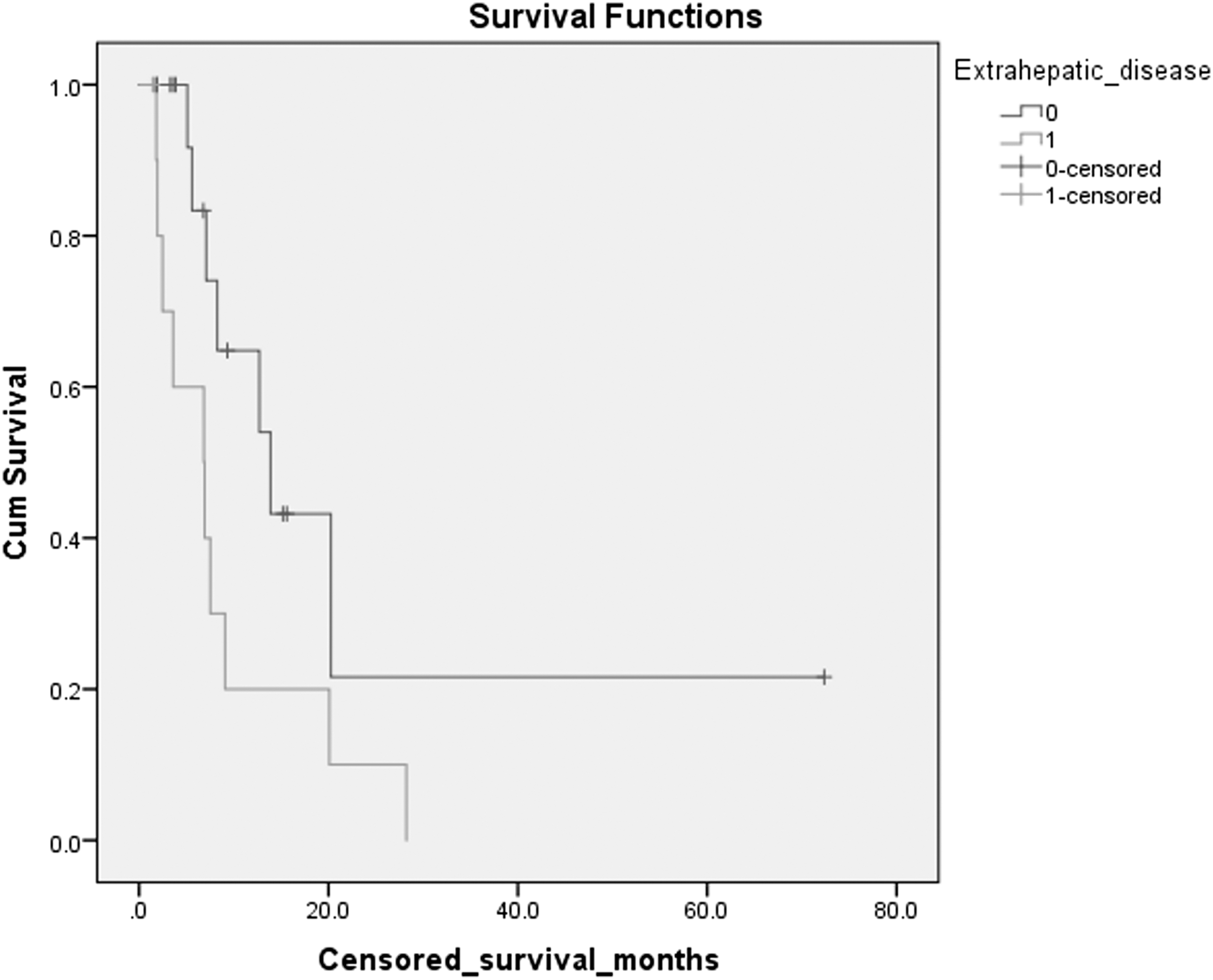
Kaplan–Meier curve for censored overall survival from first SIRT in 26 patients with unresectable ICC stratified by extrahepatic disease at baseline. Curves 0 and 1 represent absence and presence of extrahepatic disease, respectively. Note that baseline and follow-up imagings were available for 26 of 29 patients; RECIST 1.1 response was unevaluable for 3 patients.
Defined as a decline in CA 19-9 level from the pre-SIRT baseline. These values were available for 14 of 29 patients.
CA, carbohydrate antigen; CI, confidence interval; CR, complete response; OS, overall survival; PD, progression of disease; PR, partial response; RECIST, response evaluation criteria in solid tumors; SD, stable disease; SIRT, selective internal radiation therapy; TTP, time to progression.
Table 3 includes the results of univariate analysis of median TTP and OS.
Defined as the administration of systemic chemotherapy and/or external beam radiation therapy during the post-SIRT follow-up period.
Baseline imaging was unavailable for 1 patient.
Baseline and follow-up imaging were available for 26 of 29 patients; RECIST 1.1 response was unevaluable for 3 patients.
EBRT, external beam radiation therapy; N/A, not available.
p-values less than 0.05 (bolded text) are considered statistically signficant.
Safety
Clinical and biochemical toxicities are displayed in Table 4. All clinical and biochemical toxicities were Grade 1 by NCI CTCAE criteria.
Grade 1 by National Cancer Institute Common Terminology Criteria for Adverse Events criteria.
Discussion
Several series have investigated SIRT for unresectable ICC. A meta-analysis of 12 studies pooling 298 total subjects found a median post-SIRT OS of 15.5 months. 20 There was heterogeneous reporting of toxicities across the studies included in the meta-analysis, rendering toxicity summarization difficult. The largest study included in the pooled analysis, by Mouli et al., describing SIRT for unresectable ICC in 46 patients, demonstrated severe toxicities in 14% of patients, including albumin toxicity (9%), bilirubin toxicity (3%), and gastroduodenal ulcer requiring antrectomy (2%). 21 However, this study reported toxicities occurring at any point after SIRT during a median follow-up period of 29 months, rendering direct comparison difficult.
In the present retrospective review evaluating SIRT for unresectable ICC, median survival post-treatment was 9.1 months. The shorter post-treatment survival as compared with the meta-analysis may have been a result of a relatively lengthy time from diagnosis to first Y90 treatment (mean 10.3 ± 11.3 months) due to the novelty of SIRT for treating ICC during the center's early experience. Accordingly, 8 of 29 patients were treatment naive at the time of SIRT; the remaining 21 patients were refractory to treatment (chemotherapy, surgery, EBRT, and/or TACE) at the time of SIRT, with a median OS from ICC diagnosis of 26.1 months. This relatively lengthy lead time from diagnosis to first Y90 treatment in 21 of 29 patients may underestimate the potential survival benefit from SIRT.
Overall toxicity from SIRT was low, occurring after 26.7% of treatments, and was limited to grade 1 severity. No deaths occurred within 30 days of treatment. OS was significantly longer in patients with intrahepatic-only disease at baseline as compared with patients with extrahepatic disease. The absence of significant correlation between other baseline characteristics, such as ECOG, and post-treatment OS, may reflect type II error secondary to power limitations related to the cohort size.
The optimal imaging criteria for evaluating ICC treatment response remain controversial. Several studies have suggested that metabolism-based treatment response criteria using positron emission tomography response criteria for solid tumors may outperform response criteria based upon target lesion size, demonstrating that the change in tumoral 18-FDG activity correlates with response irrespective of tumor size. 22 –26 In practice, however, post-treatment surveillance is often conducted using conventional contrast-enhanced CT and MRI, as in the present series.
While imaging response for hypervascular liver malignancies such as HCC is generally assessed using modified RECIST, arterial enhancement-based criteria, ICC demonstrate a more variable enhancement pattern than HCC. A retrospective radiology–pathology correlation by Valls et al. evaluating histopathologically proven cholangiocarcinoma found a wide variation in degree of enhancement on postcontrast CT obtained during the arterial, portal venous, and delayed venous phases. In each phase, some tumors demonstrated no enhancement. 27,28
Due to this variable enhancement pattern characteristic of ICC, RECIST 1.1, which is determined using overall lesion size irrespective of enhancement pattern, was selected. A previous study by Camacho et al. found no significant correlation between objective response as determined by RECIST and median OS in patients undergoing LRT for ICC. 29 In the present series, disease control was significantly associated with longer median OS (13.9 vs. 5.6 months; p < 0.01), reaffirming a significant correlation found between RECIST disease control and median OS in a study by Hoffmann et al. 30 More significantly, there was a strong correlation between individual RECIST 1.1 response categories and median OS (PR 20.3 vs. SD 12.7 vs. PD 5.6 months; p = 0.02). These findings affirm the validity of applying RECIST 1.1 criteria for evaluating treatment response in ICC tumors following SIRT.
The optimal imaging interval for assessing tumor response to locoregional therapy also remains controversial. Per RECIST 1.1 criteria, treatment response should be assessed within 4 weeks of treatment. However, due to the nature of radioembolization, which induces cell death over time by radiation necrosis, some authors have advocated for determining treatment response at 3 months, as opposed to 1 month, following SIRT. 31 A review by Hipps et al. evaluating SIRT for colorectal liver metastases found that a slight majority of studies reported RECIST response at 3 months following treatment. 32 In the present study, RECIST 1.1 response at 90 days (3 months) was chosen to allow comparison with the two published series evaluating RECIST response after SIRT for ICC 30 (Rafi et al.) 33 and demonstrated a statistically significant correlation with OS. The 90-day imaging interval represents a de facto standard, however, and the optimal interval for assessing tumor response following SIRT warrants additional study.
Median TTP in this cohort was 5.6 months, in comparison with the other two published studies reporting post-SIRT TTP using RECIST: Hoffmann et al. 30 (4.8 months) and Rafi et al. (9.8 months). Baseline characteristics did not significantly correlate with TTP in the present series.
A strength of this study is that all included patients had biopsy-proven ICC. In the absence of histopathological sampling, a diagnosis of ICC is often made based on imaging characteristics, which carries a risk of misdiagnosing lesions that actually represent HCC, mixed HCC-ICC, inflammatory pseudotumor, or metastases. Valls et al. 28 found that the most frequent CT finding in pathology-proven ICC was biliary dilatation, occurring in only 52% of tumors. A study by Rimola et al. concluded that in the setting of liver cirrhosis, intrahepatic lesions smaller than 20 mm demonstrating progressive enhancement without washout on delayed phases may represent either HCC or ICC and require biopsy for differentiation. 34
There are several limitations to this study. First, its retrospective design limits the ability to control for confounding variables. Second, toxicity rates may be underestimated due to incomplete documentation in patient medical records, although it is less likely that severe (CTCAE grade 3 or 4) toxicities would have gone unrecorded. Third, the heterogeneity of the patient population, which had received varying treatments for ICC before SIRT and during post-SIRT follow-up, limits overall generalizability and conclusions about SIRT as a first-line therapy for unresectable ICC.
SIRT represents a palliative treatment option for unresectable ICC. SIRT safety and tolerability appear to be superior to dual-agent chemotherapy, IAC and TACE. OS following SIRT for ICC is significantly prolonged in patients with the absence of extrahepatic disease at baseline and correlates with RECIST 1.1 response evaluated at 90 days after treatment. Additional study with prospective randomized controlled trials comparing SIRT to systemic chemotherapy and TACE is required.
Footnotes
Disclosure Statement
The authors disclose the following potential conflicts of interest: R.S.P., Consulting: Sirtex, Inc. G.G., Industry-Sponsored Lectures: BTG International, Ltd. E.K., Consulting: BTG International Ltd.; Industry-Sponsored Lectures: BTG International Ltd.