
Abstract
Aim:
To evaluate the efficacy and safety of postoperative adjuvant immunotherapy with cytokine-induced killer (CIK) cells in combination with chemotherapy (CT) in colorectal cancer (CRC) patients.
Materials and Methods:
A total of 46 patients were randomly assigned to either group 1 (control group) or group 2 (CIK group) using blocked randomization. Both groups received the FOLFOX4 (5-fluorouridine, leucovorin, and oxaliplatin) CT. In the CIK group, patients were given CIK cell infusion after FOLFOX4 CT. Treatment efficacy, adverse effects, and quality of life (QOL) were assessed.
Results:
During the first 2 years of follow-up, the recurrence rate in the CIK group (26.1%, 6 in 23 cases) was significantly lower than the control group (43.5%, 10 in 23). The survival time was significantly longer in the CIK group (41.9 months, 95% confidence interval [CI]: 38.2–45.7) than in the control group (33.8 months, 95% CI: 28.4–39.2). Although QOL was reduced in both treatment groups, adjuvant CIK cell transfusion significantly improved the QOL in patients with CRC. Toxicity was mild in patients with CIK treatment.
Conclusions:
Immunotherapy with CIK cells may serve as an adjuvant treatment in patients with CRC after CT with prolonged survival of patients, limited side-effects, and improved QOL.
Introduction
Colorectal cancer (CRC) is the second most commonly diagnosed cancer in woman and the third in man worldwide. 1 It is also the fourth leading cause of global cancer-related death, accounting for >600,000 deaths annually. 2,3 Surgical resection is the first choice for CRC patients, which is normally followed by adjuvant chemotherapy (CT) or radiotherapy. Although the combined course of surgical resection and CT/radiotherapy leads to a 5-year survival rate of ∼80% for early staged CRC patients, 4,5 this combined treatment often caused severe side-effects such as infections, bleedings, myelosuppression, vomiting, nausea, and fever, which are poorly tolerated by patients. Thus, novel patient-friendly and effective therapeutic strategies are in urgent need to enhance the response rate to therapy and improve quality of life (QOL) for patients with CRC.
Cancer immunotherapy represents the most promising novel cancer treatment approach, and has drawn much attention over decades. 6 –8 It uses therapeutic modalities that simulate the host's antitumor responses through modifying the secretion of soluble mediators and the number of effector cells. 9 Cytokine-induced killer (CIK) cells, a heterogeneous subset of ex vivo expanded T-lymphocytes, are the main component of adoptive cell immunotherapy. CIK cells represent a mixed T-natural killer phenotype, and are endowed with unrestricted antitumor activity. Combination of CT and CIK cell treatment has shown to improve prognosis for patients with various types of cancers such as nonsmall cell lung cancer, hepatocellular carcinoma, and gastric cancer. 10 –16 Increasing evidence from retrospective clinical studies confirmed that CIK cell therapy could improve the prognosis of CRC. 11,13,15 However, few prospective studies have been reported regarding the efficacy and safety of CIK cell immunotherapy.
Serum baseline CEA (carcinoembryonic antigen) and CA 19-9 (carbohydrate antigen 19-9) are independent prognostic factors in CRC patients. 17 VEGF (vascular endothelial growth factor) and bFGF (fibroblast growth factor 2) play a vital role in tumor angiogenesis, which are also of great value to evaluate the prognosis. The purpose of this study was to evaluate the clinical efficacy and safety of CT (FOLFOX4) combined with CIK cell therapy in the treatment of postoperative CRC patients. In addition, the serum levels of prognostic factors (CEA, CA 19-9, VEGF, and bFGF) were measured. Our study provides useful data for the clinical application of CIK cell infusion in patients with CRC.
Subjects and Methods
Patients
This random and prospective study was performed aiming to evaluate the clinical efficacy and severity of CIK immunotherapy in combination with CT in patients with CRC after radical resection (
CRC, colorectal cancer; CT, chemotherapy; KPS, Karnofsky performance status.
Study design
The patients were continuously recruited from May 6, 2012, to June 1, 2014, from CRC patients who underwent radical surgery in our hospital, and histologically diagnosed with adenocarcinoma CRC. A total of 46 patients were randomly assigned to either group 1 (control group) or group 2 (CIK group) using blocked randomization. Patients in group 1 received CT alone, whereas patients in group 2 received CT in combination with autologous CIK cells. The ratio of the number of patients is 1:1, which means each group included 23 patients. The primary end points of the study were relapse-free survival (RFS) in 2 years, and the secondary outcome measures were RFS in 3 and 5-year overall survival (OS).
Preparation of CIK cells and treatment
Peripheral blood mononuclear cells (PBMCs) were collected with a COBE spectra blood cell separator (Terumo BCT, Inc., Lakewood, CO). PBMCs (5.0 × 106 cells/mL) were cultured with TexMACS GMP medium (Miltenyi Biotec GmbH, Bergisch Gladbach, Germany) in the presence of 1.0 × 106 U/L human interferon-γ (Shanghai Fosun Pharmaceutical Group Co., Ltd., Shanghai, China). The cells were incubated for 24 hours in a humidified atmosphere containing 5% CO2 at 37°C. Monoclonal antibody against CD3 (MAB100; 50 μg/L; R&D Systems, Inc., Minneapolis, MN) and 5.0 × 105 U/L recombinant human interleukin (IL)-2 (Shandong Quangang Pharmaceutical Co., Ltd., Jinan, China) were added after 24 hours culture at 37°C. The medium was changed every 3 days with fresh IL-2 supplement. Cells were collected after 2–3 weeks of culture. Cell phenotypes of CIK cells were assessed by flow cytometry.
Treatment plan
Both groups received FOLFOX4 (5-fluorouridine [5-FU], leucovorin [LV], and oxaliplatin [OHP]) CT. In detail, patients were administrated with 2-hour intravenous injection of 130 mg/m2 of OHP on day 1, and with 200 mg/m2 of LV before 500 mg/m2 of 5-FU from day 2 to day 6. CT was administrated at 2-week intervals, and patients received four to six courses of FOLFOX4 according to the condition of disease. Ondansetron was administrated before CT to prevent gastrointestinal reaction. In the CIK group, PBMCs were collected by blood cell separator before CT, and were cultured, induced, and collected. After CT, patients were given an infusion of CIK cells once a day for 3 consecutive days as a course of treatment. The number of cells was between 2 × 109 and 6 × 109 for each infusion. All patients in group 2 received two courses of CIK therapy.
Follow-up and clinical assessment
All patients were followed up every 3 months during the first 2 years after the initial treatment at the outpatient clinic or through telephone. Regular re-examination of tumor biomarker (CEA, CA19-9), abdominal ultrasound, and abdominal enhanced CT was carried out to monitor the tumor recurrence. Patients were followed up from the date of initial treatment to September 15, 2014, or until the death of the patient. The definition of OS and RFS was based on the National Cancer Institute's Response Evaluation Criteria in Solid Tumors. Accordingly, the OS was calculated based on the time of first treatment till the end of follow-up or death. Meanwhile, RFS was assessed according to the date of initial treatment and the first relapse of disease or the end of follow-up.
Adverse effects were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events 4.0. Adverse reactions such as fever, rash, and allergy were observed after each infusion of CIK cells.
During follow-up, evaluation of QOL was done using the Karnofsky performance status (KPS) score. An increase of KPS score for ≥10 points was defined as an improvement of QOL for patients; a decrease of KPS score for ≥10 points was designated to a decline of QOL; changes within 10 points were regarded to be stable.
Detection of the level of VEGF and bFGF
Venous blood (5 mL) was collected 1 week before and after the treatment. The blood samples were immediately centrifuged at 3000 rpm for 10 minutes, and the supernatant was stored at −20°C for later use. The levels of VEGF and bFGF were detected by relative ELISA kits (Kokopille Biotechnology Co., Ltd., Beijing, China) following the manufacturers' instructions.
Statistical analysis
Data were analyzed using the SPSS 18.0 statistical software (SPSS, Inc.). All quantitative data were expressed as mean ± standard deviation, and the statistical difference within the group or between the two groups was calculated using the Student's t test. Statistical differences of qualitative data were compared using χ2 test. The survival of patients was analyzed using the Kaplan–Meier method, and the comparison of survival time was calculated using log-rank test. The probability value p < 0.05 was considered to be of significant difference.
Results
Patient characteristics
The characteristics of patients in both groups are described in detail in Table 2. In brief, there were 23 patients (male, 15) in group 1 with CT alone. The mean age of patients was 51.4 ± 8.5 years. In group 2 with CT and CIK treatment, there were also 23 patients (male, 14), with the mean age of 52.2 ± 7.9 years. There were no significant differences in basic characteristics such as age and sex. The TNM staging system is used to classify the progression of cancer established by American Joint Committee on cancer (AJCC, American Joint Committee on Cancer) and the International Union against cancer (UICC, Union for International Cancer Control). As shown in Table 2, there were no significant differences in the number of patients with staged II and III CRC between the CIK group and the control group.
CIK, cytokine-induced killer; KPS, Karnofsky performance status.
Prognosis of CRC in patients in the two groups
In this study, we evaluated the treatment effects of CIK cells as an adjuvant therapy in patients with CRC who simultaneously underwent CT after radical surgery. The period of follow-up was 11 to 47 months. During the first 2 years of follow-up, the recurrence rate in the CIK group (26.1%, 6 in 23 cases) was significantly lower than that in the control group (43.5%, 10 in 23 cases) (p < 0.05). The 1- and 2-year survival rates of the CIK group were 100% and 95.7%, respectively, whereas the 1- and 2-year survival rates of the control group were 100% and 87%, respectively. The median survival time of the CIK group was 41.9 months (95% CI: 38.2–45.7), whereas the median survival time of the control group was 33.8 months (95% CI: 28.4–39.2). The survival time was significantly longer in the CIK group than in the control group (p < 0.05) (Fig. 1).
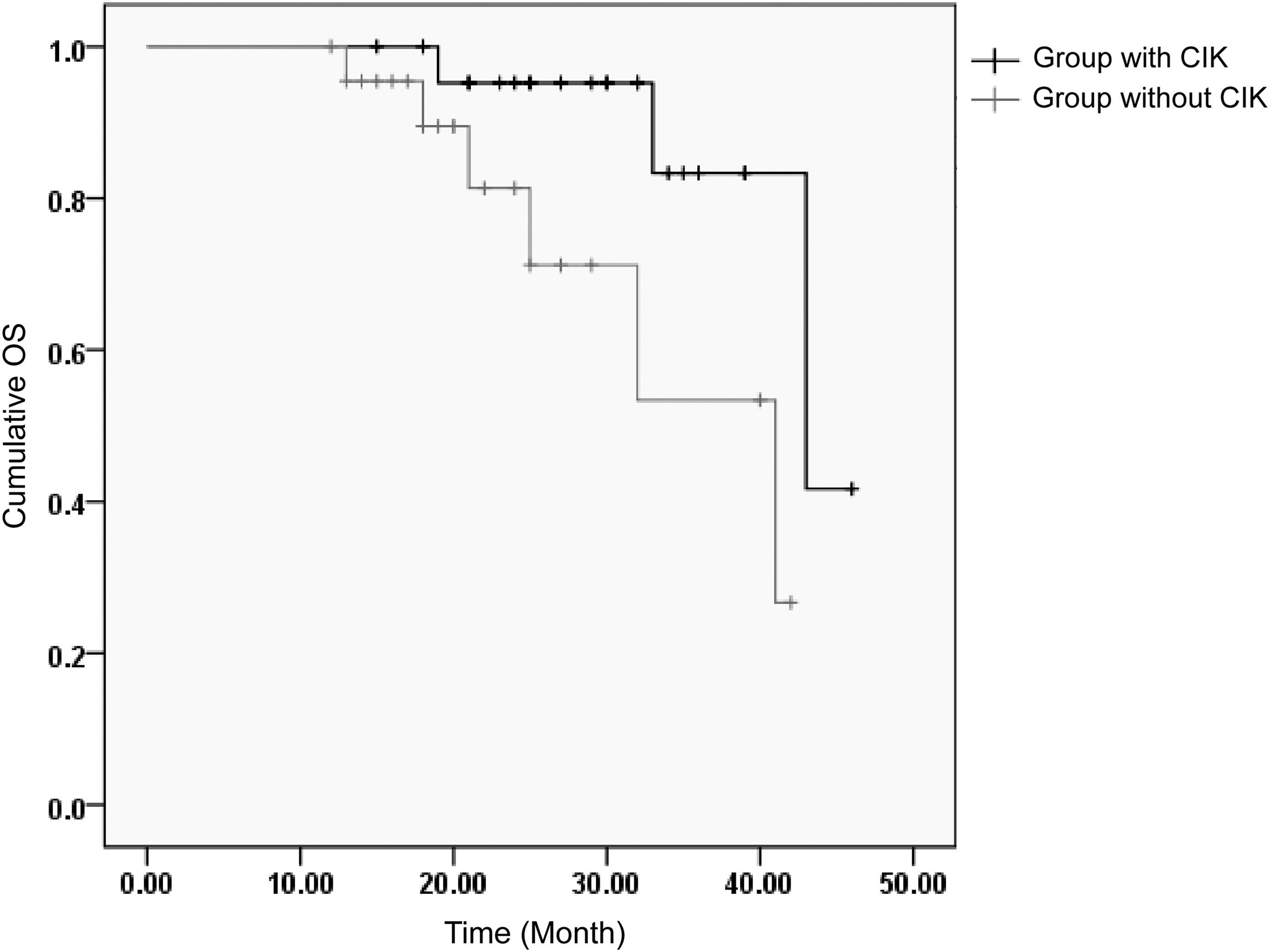
OS of patients in the CIK group (with CIK treatment) and the control group (without CIK treatment). Kaplan–Meier curves for OS in patients of the CIK group and the control group. An event is defined as death in OS. CIK, cytokine-induced killer; OS, overall survival.
Quality of life
The QOL of patients in both groups was assessed using the KPS score. As compared with KPS score before treatment, KPS score of patients in both groups was decreased after treatment. However, there was no significant difference in the CIK group after treatment, whereas a significant decrease was observed in the control group (Table 3). Moreover, KPS score in patients in the CIK group was significantly higher than that in the control group after treatment (Table 3). These results suggested that, although QOL was reduced in both treatment groups, adjuvant CIK cell transfusion significantly improved the QOL in patients with CRC.
p < 0.05, compared with KPS score in the control group after CT.
p < 0.05, compared with KPS score before treatment within each group.
CIK, cytokine-induced killer; CT, chemotherapy; KPS, Karnofsky performance status.
Adverse effects
In general, the main toxic reaction after treatment was myelosuppression, neurotoxicity, and gastrointestinal reaction (such as nausea, anorexia, and diarrhea), which were mainly grades I–II. Severe myelosuppression (grade III or IV) was only observed in three patients with CIK cell therapy. No patients were with severe liver and kidney dysfunction. The adverse effects (myelosuppression, neurotoxicity, and nausea) in the CIK group were significantly lower than those in the control group. There was no significant difference regarding the incidence rate of abnormal liver function (Table 4). During infusion of CIK cells, two cases developed fever with body temperature below 38.5°C. Both cases were successfully treated with physical cooling. One case developed low-grade fever 1 hour after infusion of CIK cells, and returned to normal without treatment. None of the cases developed rash and allergy.
Levels of CEA, CA19-9, VEGF, and bFGF
The levels of CEA, CA19-9, VEGF, and bFGF were detected by ELISA. Our results showed that the levels of CEA, CA19-9, VEGF, and bFGF were significantly decreased in both groups after treatment as compared with the levels before treatment (Table 5). Moreover, the levels of CEA, CA19-9, VEGF, and bFGF were further decreased in the CIK group than those in the control group after treatment (Table 5).
p < 0.05, compared with KPS score in the control group after CT.
p < 0.05, compared with KPS score before treatment within each group.
bFGF, fibroblast growth factor 2; CA 19-9, carbohydrate antigen 19-9; CEA, carcinoembryonic antigen; CIK, cytokine-induced killer; CT, chemotherapy; VEGF, vascular endothelial growth factor.
Discussion
Prognosis of patients with CRC remains poor, despite various therapeutic options such as adjuvant CT and radiotherapy after surgery, and tumor recurrence happens within 2 years after surgery in most of the cases. 18 –20 Moreover, CT/radiotherapy often causes severe side-effects such as myelosuppression, vomiting, nausea, and fever, which are poorly tolerated by patients. Thus, novel patient friendly and effective therapeutic strategies are in urgent need to enhance the response rate to therapy and improve QOL for patients with CRC. Over the past decade, cell immunotherapy has drawn great attention and has been reported to be able to cause more favorable treatment outcomes for a variety of cancers, and therefore, may serve as a promising approach to treat CRC after surgery in combination of CT/radiotherapy. 6
In this study, we evaluated the clinical efficacy and safety of CT (FOLFOX4) combined with CIK cell therapy in the treatment of postoperative CRC patients. The systemic CT regimen FOLOFOX is the standard chemotherapeutic regimen for CRC. 21 Our results showed that the recurrence rate in patients treated with the combination of FOLFOX4 and CIK cells (26.1%, 6 in 23 cases) was significantly lower than that in patients treated with CT alone (43.5%, 10 in 23 cases), during the first 2 years of follow-up. The survival time was significantly longer in patients treated with the combination of FOLFOX4 and CIK cells (41.9 months, 95% CI: 38.2–45.7) than in patients treated with CT alone (33.8 months, 95% CI: 28.4–39.2). Our results agreed with other studies. Zhang et al. retrospectively reported significant longer progression-free survival and OS in CRC patients treated with CT plus CIK cells. 13 Similarly, adjuvant transfusion of CIK cells has been reported to prolong disease-free survival in patients with CRC. Moreover, we also found that the combination of FOLFOX4 and CIK cells could significantly improve the QOL in patients. The results of our study suggest that adjuvant transfusion of CIK cells prolongs OS for patients with CRC after radical resection.
Serum baseline CEA and CA 19-9 levels and their kinetics have been demonstrated to be independent prognostic factors in CRC patients. 17 It has been reported that the increase of serum CEA and CA 19-9 levels is considered to be a signal of tumor progression in advanced CRC patients, who receiving treatment of monoclonal antibody bevacizumab. 22 Our study found that adjuvant transfusion of CIK cells plus FOLFOX4 could significantly reduce the level of serum CEA and CA 19-9 levels, as compared with FOLFOX4 alone. VEGF and bFGF play a vital role in tumor angiogenesis, and the levels of serum VEGF and bFGF have been elevated in patients with CRC. Bestas et al. revealed that serum VEGF was closely related with tumor stage and metastasis, and VEGF might serve as a prognosis marker for CRC patients. 23 However, less has been known about the levels of VEGF and bFGF in CRC patients after the combined treatment of FOLFOX4 and CIK cell immunotherapy. Our results showed that adjuvant transfusion of CIK cells plus FOLFOX4 could significantly reduce the level of serum VEGF and bFGF levels, as compared with FOLFOX4 alone. These results suggest that besides effective therapeutic effects, adjuvant transfusion of CIK cells could also reduce the serum level of prognostic factors in CRC patients.
In conclusion, our study showed that postoperative adjuvant transfusion of CIK cells in combination of CT could prolong survival in patients with CRC, with limited side-effects and improved QOL. Our study provides useful data for the clinical application of CIK in patients with CRC.
Footnotes
Disclosure Statement
No competing financial interests exist.