
Abstract
Background and Aim:
Pain is a prevalent and serious problem in patients with cancer. This study aimed to investigate the clinical value of the implantation of radioactive particle 125I in treating cancer and its pain.
Materials and Methods:
From February 2014 to February 2015, 38 patients with malignant tumor received computed tomography (CT)-guided 125I radioactive particle implantation to treat cancer pain in this hospital. Before surgery, the lesions were calculated by brachytherapy treatment planning system (TPS) to get the local number of particles that are required for implantation. For a period after implantation, TPS was used again to assess the effect of treatment. The 38 patients received 6-month follow-up, and the CT scan was used to evaluate the local tumor. The visual analogue scale (VAS) was used to assess the pain.
Results:
The curative effect was evaluated at postoperative 2, 4, and 6 months, and the curative effect was 34.2%, 73.68%, and 89.47%, respectively. The preoperative VAS score of the 38 patients was 5.48 ± 2.50 (13 cases of mild pain, 19 cases of moderate pain, and 6 cases of severe pain), and their pain was improved in different degrees after operation.
Conclusions:
CT-guided 125I radioactive particle implantation is a safe and effective treatment for cancer and its pain.
Introduction
T
Among the numerous interventional methods, interstitial implantation of radioactive 125I particles has the advantages of high intratumoral dose, low extracellular dose, high degree of adaptation, less complications, and good patient tolerance. Under the guidance of imaging equipment (most commonly used computed tomography—CT), 125I particles (a miniature radioactive source) are directly implanted into the tumor tissue through percutaneous puncture technique to achieve therapeutic objective.
In this study, CT-guided percutaneous puncture 125I particle interstitial implant for the treatment of tumor lesions achieved good results. The results are reported herein.
Materials and Methods
General information
From February 2014 to February 2015, a total of 38 patients (24 male and 14 female) with malignant tumor underwent CT-guided 125I particle implantation in this hospital.
Their average age was 55 years old (range from 42 to 77). In addition, 3 of them had pleural metastasis, 3 of them had chest wall metastases, 1 of them had pleural and chest wall metastasis tumor, 8 of them had vertebral metastases, 1 of them had metastases of the sacrum, 5 of them had soft tissue metastases, 6 of them had pelvic metastases, 2 of them had metastatic tumors of abdominal walls, and 9 cases had local invasion of primary tumor (including 4 cases with lung squamous cell carcinoma, 4 cases with adenocarcinoma, and 1 case with synovial sarcoma). The maximum diameter of the lesions ranged from 2.5 to 14.0 cm, and the Karnofsky Performance Status score ranged from 69 to 90 (median score was 80) (Table 1). This study was approved by the hospital ethics committee and all patients gave informed consent.
KPS, Karnofsky Performance Status.
Inclusion criteria: (1) The image data and/or clinical manifestation showed the treated lesions were the responsible lesion. (2) After surgery, patients did not receive analgesia treatment. (3) There is no important organ block in the puncture path of particle implantation. (4) The preoperative blood and electrocardiogram examinations were in accordance with the operation requirements.
Exclusion criteria: (1) Patients with poor general condition or some basic diseases cannot tolerate particle therapy. (2) It was expected that the needle would inevitably damage the important organs. (3) The hematology index did not meet the requirements of the operation.
Instruments and methods
The Philips Brilliance CT (Big Bore 16 CT) was used to scan with the following parameters: thickness was 5 mm, tube voltage was 20 kV, and tube current was 250 mA. The radioactive particle implantation treatment planning system (TPS), particle implantation gun, and particle push rod were purchased from Beijing Tian Hang Ke Lin Technology Development Co. Ltd. The 125I radioactive particle source was purchased from China Nuclear Industry Corporation, and the particle activity was 0.7–0.8 mCi. The 18G particle implanting needle was purchased from Japan Eight Light Co, and the length was 15–20 cm.
Before surgery, patients received routine CT scan, and the image information was transmitted into the TPS to make the preoperative plan for the responsible lesion. The clinical target volume (CTV) and planning target volume (PTV) were delineated. PTV was expanded about 0.5–1.0 cm from CTV. The tumor matching peripheral dose ranged from 90 to 120 GY. According to the preoperative plan, intraoperative actual situation, the shape of the tumor, and adjacent structures, the parallel or fan-shaped needle method was performed.
With the guide of CT, the puncture needle was tried to follow the long axis of the tumor. When bone or important structure blocked the needle position, the puncture needle inclined to a certain angle. The probe spacing was about 1 cm, and the spacing of each row of particles was 0.5–1.0 cm. Particle was located >1 cm from the radiation-sensitive organs. Target lesion CT scan was performed immediately after the operation. The image was transmitted into the TPS for quality verification. If there was some zone with little dose, patients might receive particle reseeding depending on the situation.
Curative effect evaluation
The CT and the efficacy were evaluated at 2, 4, and 6 months after operation. The size and density of the tumors were compared before and after operation. Efficacy was evaluated by Response Evaluation Criteria in Solid Tumors standard (Table 2). The local control rate was the proportion of complete remission (CR) and partial remission (PR).
CR, complete remission; PR, partial remission; PD, progressive disease; RECIST, Response Evaluation Criteria in Solid Tumors; SD, stabilized disease; VAS, visual analogue scale.
The visual analogue scale (VAS) (Table 2) was used to assess the pain degree before operation and 3 d or 1 month after operation. The effective rate of the cancer pain treatment was the proportion of CR and PR. Postoperative complications were observed and evaluated by the American/European Radiation Oncology Group (RTOG/EORTC) radiation injury classification program.
Statistical analysis
Statistical analysis was performed by SPSS 11.0 software, and data are expressed as mean ± standard deviation. The differences between groups were assessed by Student's t-test with a significance level of p-value <0.05.
Results
Postoperative CT features
CT-guided 125I radioactive particle implantation was successfully carried out in all the patients. About 25–130 particles were implanted into each patient. CT scanning showed that particles were uniformly distributed in the lesions, and consistent with lesion morphology, and the distance between particles and the important organs was >1 cm (Fig. 1 –5). CT examination at postoperative 2, 4, and 6 months showed that the volume of most of the lesions gradually reduced with time, and the particles gathered in the tumor (Fig. 6). Local control rates were up to 34.21% (13/38), 73.68% (28/38), and 89.47% (34/38), respectively (Table 3).
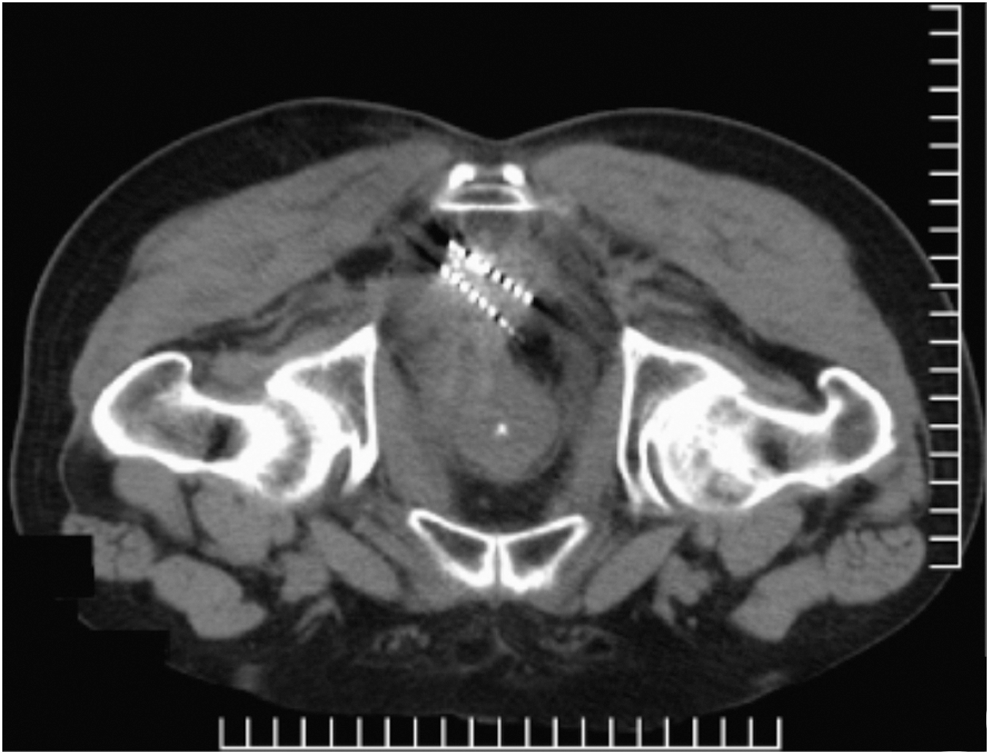
Metastatic adenocarcinoma in pelvis. The lesion located behind the anterior sacral rectum, and the particles were distributed in interior of tumor.
Tumor of vertebral metastases. The lesion destroyed vertebral bone and broken into the spinal canal. The particles were cross-distributed (sparse inside and dense outside), which protected the spinal cord to the greatest extent.
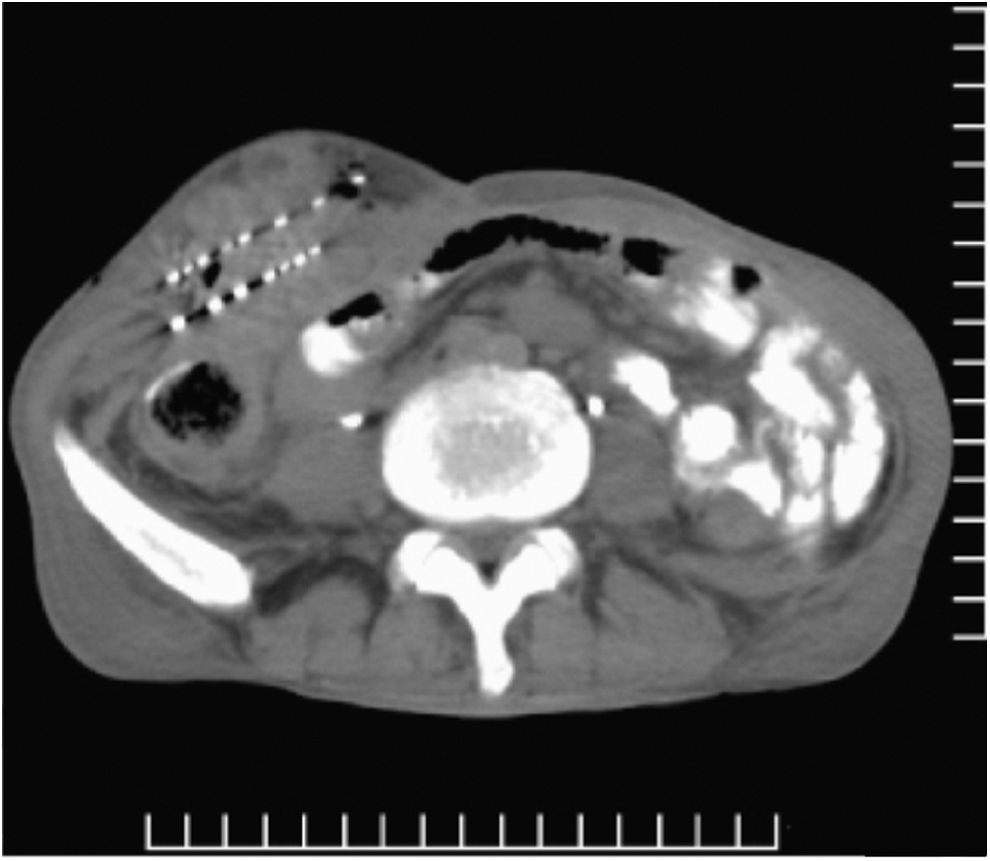
Metastatic tumors of abdominal walls. The particles were parallel distributed and keep safe distance from the skin or the intestines.
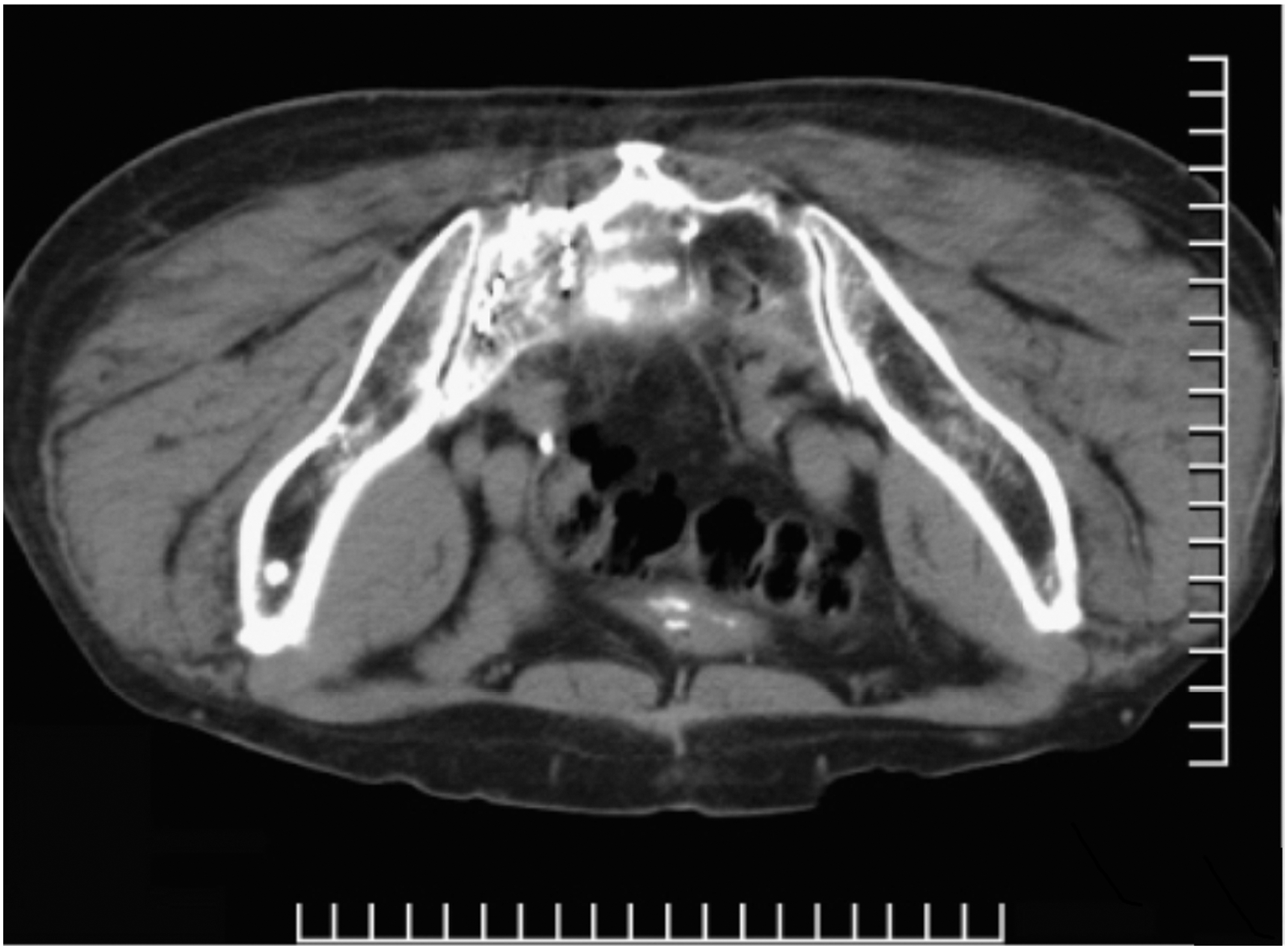
Tumor of sacral bone metastases. After drilling by medullopuncture needle, the particles were implanted into sacrum by coaxial technology.

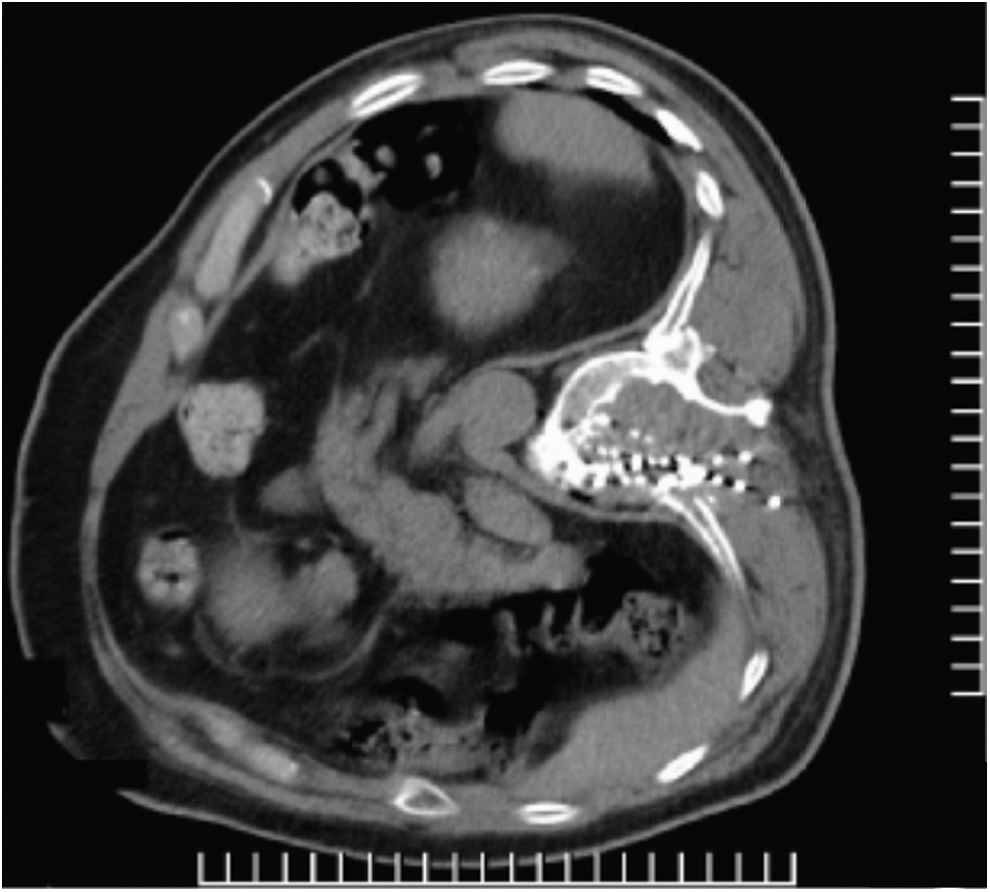
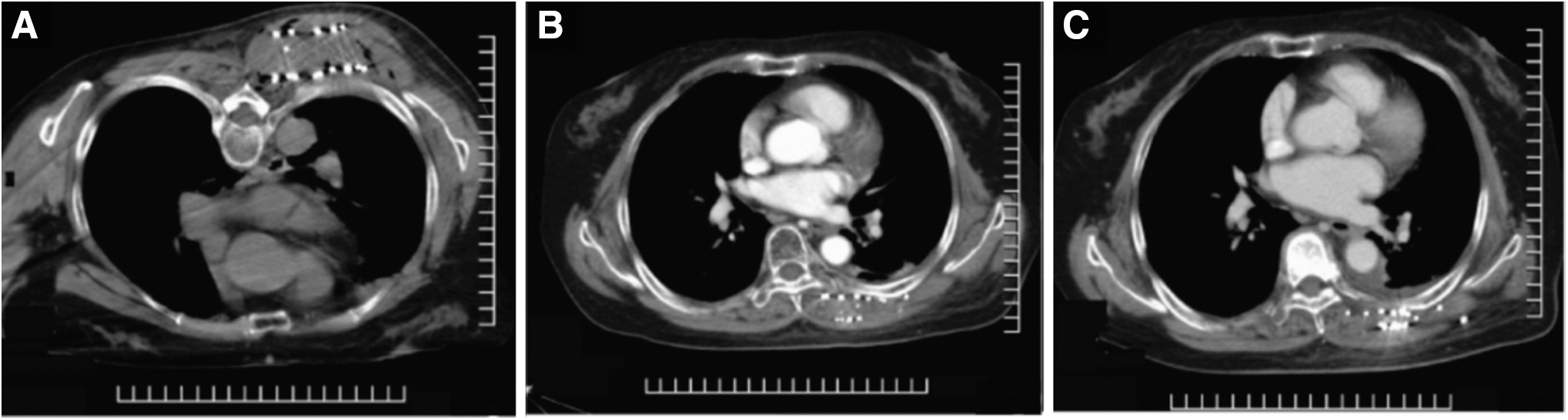
Pleural and chest wall metastasis tumor. The lesions were spread out in the inside and outside of the rib, and the multiangle of the needle is used to make the particle well distributed in the tumor.
The patient with synovial sarcoma of the back. The preoperative visual analogue scale pain score suggested complete remission, and the pain eased gradually.
CR, complete remission; PR, partial remission; SD, stabilized disease; PD, progressive disease.
VAS score
The preoperative VAS score of the 38 patients was 5.48 ± 2.50 (13 cases of mild pain, 19 cases of moderate pain, and 6 cases of severe pain), and their pain was improved in different degrees after operation. Three days after operation, the completely relieved pain rate and improvement rate was 7.89% (3/38) and 63.15% (24/38), respectively. The effective rate and the invalid rate were 73.68% (28/38) and 26.31% (10/38), respectively. One month after operation, the completely relieved pain rate and the improvement rate were up to 47.37% (18/38) and 47.37% (18/38), respectively. The effective rate and the invalid rate were 94.74% (36/38) and 5.26% (2/38), respectively (Table 4).
VAS, visual analogue scale.
Complications
The main complications contained local pain (4 cases), fever (4 cases), swelling in soft tissue (2 cases), pneumothorax (1 case), and local hemorrhage (3 cases). In addition, there were 33 cases with acute radiation pneumonitis at grade 0, 30 cases with advanced radiation pneumonia at grade 0, and 3 cases with advanced radiation pneumonia at grade 1. There was no radiation damage at grade 2 or more.
Discussion
For patients with metastatic tumors, the traditional treatment concept suggests that systemic vein chemotherapy should be used. For the local lesions that are difficult to control, adjunct radiotherapy can be given. With the development of medical technique and the changes in the idea of tumor treatment, the local treatment is gradually subjected to patients' and doctors' attention and recognition, and the tumor therapy tends to be more efficient, minimally invasive, and individualized. In China, about 60% cancer patients have pain. In the patients with medium and advanced cancer, the proportion is as high as 80%. 4
Cancer pain seriously affects the patients' quality of life and the treatment effect of antitumor drug. The standard treatment for cancer pain is called “three steps therapy,” that is, patients receive different intensities drug therapy according to different pain levels. However, the “three steps therapy” cannot achieve satisfactory results for many cancer patients in clinical practice, especially for patients with advanced cancer. Therefore, the local minimally invasive interventional therapy, known as the fourth step therapy, is considered to be performed in the patients with advanced cancer. 5,6
This therapy can suppress tumor growth and eliminate cancer pain through local treatment of the responsible lesions. Previously, the implantation was performed by surgeons, so the artificial operation was random and the curative effect was limited. With the development of image guidance technology and particle implantation planning system, interventional therapy has been developed rapidly. At present, many studies have reported the application of 125I radioactive particles implantation in various cancers, including prostate cancer, 7 –11 rectal cancer, 12 cervical cancer, 13 gastric cancer, 14 liver cancer, 15 and nonsmall cell lung cancer. 16 The results of clinic showed that 125I radioactive particles implantation was efficacious in the treatment of cancer.
Radioactive particle implantation belongs to brachytherapy, and its advantage is that the radiation radius is short, the intratumoral dose after implantation into the tumor is high, and it has little influence on the surrounding tissue. 17 –19 However, the implanted particles need to achieve dosimetric distribution requirements within the tumor. If small dose area appears, the surgical outcomes will be affected. In this study, according to the shape of tumor and adjacent relationships, the puncture needle was arranged through proper guidance and certain surgical techniques and TPS were used to make the particle be well distributed in the tumor. After operation, the TPS proved that the method obtained the satisfactory curative effect.
A total of 38 patients were included, and the responsible lesions for the pain were located at different sites. One case was found to have metastatic adenocarcinoma in pelvis, whose lesion was located behind the anterior sacral rectum that was adjacent to the bowel and bladder, and the particles were distributed in the interior of the tumor and stayed away from important organs more than 1 cm (Fig. 1). Vertebral metastases was diagnosed in 3 cases, and the lesion destroyed the bone, entered the spinal canal, and compressed the spinal cord. The particles were cross-distributed, which maximally protected the spinal cord (Fig. 2). One case was found to have tumors of abdominal walls. The image showed that the tumors were large, the outer edge was extended to the subcutaneous wall of the abdomen, and the interior was close to the intestinal tube.
The particles were implanted and kept within a safe distance (Fig. 3). One case was found to have tumor of sacral bone metastases, and bone puncture needle was used to drill in lesions. Then, 125I particle implantation was carried out by medullopuncture needle, and the particles were well distributed in the tumor (Fig. 4). One case was found to have pleural and chest wall metastasis tumor, and the lesions were spread out in the inside and outside of the rib. Therefore, the multiangle of the needle was used to make the particle be well distributed in the tumor (Fig. 5).
All patients were followed up for 6 months. As time proceeded, the lesion volume and intensity gradually decreased, and the particles gather to form a pile in the tumor (Fig. 6). The score of pain was decreased in 3 d and 1 month after operation, and the effective rate was 73.68 and 94.74%, respectively. These results suggested that the longer the time, the more obvious analgesic effect of particles was exerted. Three days after operation, the effective rate was 92.30%, 63.15%, and 50% in patients with mild pain, moderate pain, and severe pain, respectively. One month after operation, the effective rate was 100%, 94.73%, and 83.33% in patients with mild pain, moderate pain, and severe pain, respectively.
These results indicated that the less the pain before operation, the better the effect of analgesia after operation. The local control rates were 34.21%, 73.68%, and 89.47% at 2, 4, and 6 months after operation, respectively, which implied that radioactive particles implantation not only controlled tumor growth effectively but also alleviated cancer pain. The main complications are local pain, fever, swelling in soft tissue, pneumothorax, and local hemorrhage, and all the symptoms improved markedly after symptomatic treatment. There was no acute or chronic radiation pneumonitis at grade 2 or higher. Intraoperative complications were mainly related to puncture and postoperative complications were mainly related to radiation injuries.
Most of the patients were well tolerated during the operation and without obvious discomfort. Only 3 patients suffered from local irritation pain due to bleeding into the pleural cavity. Skilled and standardized puncture skills can effectively prevent intraoperative complications. When making TPS plan before operation, the actual operation should be considered, and the feasibility of dosimetry and operation should be highly unified. According to the location of the lesion and adjacent structure, parallel puncture combined with fan-shaped puncture technique can improve operation efficiency and reduce complications.
When planning for operation, attention should be paid to radiation protection of adjacent important organs of the lesions. Moreover, the tolerated dose of the surrounding tissues should be considered and the effect of dose redistribution on surrounding tissues after the lesions reduced, which is designed to reduce postoperative radiation-related complications. In this study, the particles kept away >1 cm from the peripheral important organs, and no serious radiation-related complications occurred during long-term follow-up.
In conclusion, radioactive 125I implantation, as a local minimally invasive treatment, has good tolerability, accurate curative effect, and less complications. The particles implantation into the responsible lesions of patients with malignant tumor can effectively relieve pain, control tumor growth, and has good clinical value.
Ethical Approval
The study was approved by ethics committee of Navy General Hospital.
Footnotes
Disclosure Statement
No competing financial interests exist.