
Abstract
Background:
Nearly 200 cancers repertories are rare, and more than 20% are pelvic neoplasia. Diagnosis and treatment are challenging, even in reference centers, and survival is influenced by the aggressiveness of certain histologies and absence of a standard of care.
Patients and Methods:
The authors report the results of a retrospective analysis of patients that attended the Institute of Oncology, Bucharest, between 2004 and 2015, for nonmetastatic pelvic malignant tumor treatment and follow-up. The outcomes are compared between the rare and common histology groups.
Results:
Of the 60 cases analyzed, 17 patients (28.33%) bore a rare tumor, 33 (55%) were women, and the median age was 59 years. The majority was concerned by bladder (41.66%, 25 patients) and cervix (23.33%, 14 patients) neoplasms. For a median follow-up of 27.5 months, relapse was registered in 27 patients (45%), of whom 9 (33.33%) were from the rare group (53% of this subpopulation). The highest relapse rates were recorded in patients with rare bladder tumors (66.7%, 4 patients) compared with 42.1% (8 patients) in the common group (p = 0.294) and in prostate localization (66.7%, 2 patients) compared with 16.7% (1 patient) (p = 0.134). Estimated median relapse-free survival (RFS) was 60, 12 months in the rare group and 67 months for common tumors.
Conclusions:
In nonmetastatic rare pelvic tumor patients, the outcome was found to be poorer than in those concerned by common histologies stratified by organ. A higher rate of relapse and the lowest median RFS were observed in bladder and prostatic cancers.
Introduction
Rare cancers are defined differently in Europe and the United States. A European working group defines rare cancers as those with an annual incidence lower than 6 in 100,000, 1 whereas the U.S. National Cancer Institute considers either an annual incidence lower than 15 in 100,000 or a prevalence of fewer than 5 cases out of a population of 10,000. 2 In Europe, 500,000 new cases of rare cancers are estimated each year, representing 22% of all diagnosed cancers. Nearly 200 cancers are indexed as rare, of which 18% concern the female genital tract. 1 There is a higher incidence of rare cancers in very young adults, in whom nearly 70% of cases of cancer can be classified; in those aged 20–39 years, the proportion of rare cancers is about 40% and the percentage is lower than 20% in adults older than 40 years. 3
The authors can distinguish four categories of rarity: rare tumors such as neuroblastoma, rare histological types such as alveolar rhabdomyosarcoma, rare locations such as cerebral lymphoma, and rare presentations in certain populations such as breast cancer in men. 2,4 Several uncommon histologies have been described in malignant pelvic tumors that have been reported with an incidence of <5 in 100,000 per year: cervical adenocarcinoma, uterine sarcoma, primitive neuroectodermal or small-cell neuroendocrine (NE) tumor of the prostate, and squamous cell carcinoma and adenocarcinoma of the bladder. 4 In comparison with common tumors, survival disadvantages increase with age. According to the 2011 report of the RARECARE working group, the 5-year survival rate increases from 17% in the 40–59 age group to 30% in the 75–99 age group. 1
These types of cancers are challenging for clinical practice, even in reference cancer treatment centers. Moreover, adequately powered trials are often lacking due to the small number of patients, which makes it difficult to define standard treatments in terms of either the sequence of multimodal approaches or the efficacy of a specific therapy. Survival is therefore affected by the aggressiveness of individual histologies, as well as the absence of a standard of care, since guidelines are usually developed for typical histologies. 5 According to the large-scale analysis involving 57,144 adults by the EUROCARE working group, involving 14 selected rare cancers diagnosed between 1983 and 1994 in Europe, 5-year relative survival was found to be lower than that for corresponding common cancers in general (47% vs. 65%). Nonetheless, the 5-year survival outcomes vary considerably in the early stages of some rare histologies: 65.5% in cervical adenocarcinoma, 43.5% in uterine sarcoma, and only 20.4% in squamous-cell carcinoma of the bladder. 4
Given the difficulties in running adequately powered trials, there have been initiatives to adapt the methodology for clinical trials in rare cancer populations, including the use of randomized phase II design instead of phase III, 6 a greater type I error, 7 and using the Bayesian approach as an adaptive framework. 8 Moreover, international organizations are encouraging contributions from case series or small retrospective analyses to help expand guidelines for diagnosis and treatment. With this in mind, the authors performed a retrospective analysis at the Institute of Oncology “Prof. Dr. Alexandru Trestioreanu,” Bucharest, Romania to compare outcomes between patients with rare pelvic tumors and nonrare controls, undergoing curative resection.
Materials and Methods
The authors analyzed cases of nonmetastatic pelvic cancers and compared them with corresponding nonrare counterparts (1–3). To achieve this, the authors used the medical records of adult patients with genital and gynecologic pelvic cancer referred to their academic institution for treatment between 2007 and 2012 and who had adequate follow-up. The designation of the case as rare was based on the local immunohistological assessment of either the biopsy specimen or the resected tumor in cases with primary surgery, following the new list of rare cancer types provided by the RARECARE network. 9 The study was approved by the Ethics Committee of the Institute of Oncology in Bucharest, and written consent was obtained from all patients for both invasive procedures and the prospective collection of their data. The study was conducted in accordance with the Declaration of Helsinki.
The principal exclusion criteria were the presence of metastatic disease or palliative resection of the primary tumor. The tumor stage was established according to the AJCC Seventh Edition Staging System, 10 and the radiological response criteria conformed to RECIST 1.1. 11 The therapeutic approach followed the National Comprehensive Cancer Network 12 and ESMO guidelines 13 at the time, as these are used in Romania in the absence of national protocols. Relapse-free survival (RFS) was the primary outcome measure, defined as the period from the first histological proof of cancer to any local or distant relapse, histologically documented or not, or death from any cause during follow-up.
The authors also identified the clinical, histological, and treatment-related prognostic factors in rare pelvic tumor cases, as well as their correlation with recurrence. A subanalysis was then carried out according to three therapeutic strategies as follows: patients who underwent upfront surgery, those who underwent sequential surgical treatment, and patients who benefited from nonsurgical multimodal approaches such as definitive concomitant radiochemotherapy.
The analysis was carried out using SPSS version 22. A chi-squared test was used to compare between-group differences in patients' categorical characteristics, and continuous variables were compared using independent t-tests. Survival curves were generated using the Kaplan–Meier method, and the differences between groups were assessed using the log-rank test. The two-sided p-value was considered to be significant if <0.05, and a 95% confidence interval (CI) was computed when appropriate.
Results
Of the 80 files analyzed, 60 cases were found to be eligible, of which 17 cases (28.3%) were of rare histologies. Thirty-three patients (55%) were women, and the median age was 59 years (range 31–86 years). The majority, 41.7% (25 patients), were affected by bladder cancer, 23.3% (14 patients) by cervix neoplasms, and 15% by uterine sarcoma and prostate cancer (9 patients each) localizations. Extraorganic tumors were poorly represented by 2 cases of extraperitoneal mature teratoma. Rare histologies were homogenously distributed: 6 cases (35.3%) of bladder carcinoma (1 NE, 1 mucinous, 3 squamous, 1 adenocarcinoma), 2 (11.8%) of extraperitoneal mature teratoma, 3 adenocarcinomas and 1 NE carcinoma of the cervix (23.5%), 3 prostate localizations (17.6%; 2 carcinosarcomas and 1 poor differentiated NE), and 2 uterine sarcomas (11.8%).
In the rare tumor group, the median age was 59.3 years, and women were mostly affected, representing 52.9% of cases (9 patients). Personal history of cancer was recorded in 4 cases (23.5%), with no cases of a family history of cancer (Table 1). The Charlson comorbidity index was used to measure the importance of the underlying diseases 14 : this ranged between 0 and 4 in 13 patients (76.4%) and was above 5 in 4 patients (23.5%; p = 0.184). In 14 cases (82.35%), the diagnosis was based on a tumor resection specimen. In only 1 case, the histopathological result of the biopsy specimen and postoperative tumor analysis corresponded. Histological stage was pT1 in 4 patients (23.5%), pT2 in 3 patients (17.6%), and pT3 in 4 patients (23.5%), and the lymph node's involvement was recorded as 11.7% (2 patients). The tumor's grade was III in 6 patients (35.3%) and II in 4 patients (23.5%) (Table 1).
Characteristics in Rare Tumor Population Versus Common Tumor Cases
NE, neuroendocrine; pT, histopathologic stage of primary tumor; pN, histopathologic regional lymph nodes involvement; G, histologic tumor's grade; RT, radiotherapy; RT-CHT, radio-chemotherapy; CHT, chemotherapy.
The rare phenotype was found to be nonsignificantly correlated with a personal history of cancer and pathologic stage of a tumor (p = 0.2). As a specific treatment, 13 patients (76.4%) underwent primary surgery, 2 patients sequentially (11.8%), and 2 patients (11.8%) had no surgical procedure. The type of sequence was found to be significantly correlated with the Charlson score (p = 0.017), primary site of a tumor (p = 0.001), and histology of the surgical specimen (p = 0.001).
Surgical approach
Altogether, 37 patients (60%) underwent upfront surgery, 23 (62.2%) of them for bladder cancer, of which 13 belonged to the rare tumor group (76.5%). In 18 cases (63.2%), the intervention was conservative, leading to an R0 resection in 14 patients (37.8%) and R1 or R2 in 8 patients (19.6%; p = 0.52) (Table 2).
Characteristics in Patients That Underwent Upfront Surgery in Rare Versus Common Groups
NE, neuroendocrine; pT, histopathologic stage of the primary tumor; pN, histopathologic regional lymph nodes involvement; G, histologic tumor's grade; RT, radiotherapy; RT-CHT, radio-chemotherapy; CHT, chemotherapy.
In the R0 conservative surgery subgroup, histological tumor stage was pT1 in 42.9% (6 patients) and pT3 in 35.7% (5 patients) (p = 0.186), nodal involvement was recorded in four cases, and the tumor's grade was principally G2 and G3 in 40% and 50% cases, respectively. In only T3 NE bladder carcinoma was necrosis observed. There were five cases of rare tumors (35.7%) and nine cases of common histologies (64.3%; p = 0.003), and the localizations in which the complete resection was obtained were uterine in 6 cases (42.9%), bladder in 5 cases (35.7%), cervix uteri in 2 cases (14.3%), and 1 case of teratoma (7.1%; p = 0.436).
In the rare tumor group, surgery was the main upfront approach (76.5%), principally in bladder cancers (46.2%, 6 patients), uterine and prostate localizations (15.4%, 2 patients each), and uterine neoplasm (7.7%, 1 patient). The surgery was R0 in 5 patients (62.5%) and R2 in 3 patients (37.5%); the tumor's histological stage was pT1 in 15.4% (2 patients), pT2 in 23.1% (3 patients), and pT3 in 30.8% (4 patients), while lymph node involvement was recorded in half of the examined samples (15.4%). Tumor grade was II in 30.8% of cases (4 patients) and III in 38.5% of cases (5 patients).
Of the 35 patients (58.3%) of the general population that further benefited from an adjuvant treatment, 11 cases (31.4%) belonged to the rare tumor group, 20 patients (60.6%) underwent irradiation, 4 patients (11.4%) had systemic treatment exclusively, and 19 patients (54.3%) had sequential radiotherapy and chemotherapy. In the rare tumor group, of the 11 patients (64.7%) that received subsequent postoperative treatment, 8 patients (72.7%) were irradiated, in both the tumor bed and the lymph node field (in 1 case concomitant with cisplatin [CDDP], with the dose varying between 30.6 and 59.4 grays [Gy]). In 6 patients, cytotoxic systemic treatment was provided sequentially, alongside radiotherapy, of which 5 cases were bladder cancer, the regimen being gemcitabine platinum-based treatment (carboplatin [CBDCA] in 3 cases and CDDP in 2 cases). The other regimen was ifosfamide-CDDP (the only case of uterine stromal sarcoma). A 100% dose intensity was provided in only 1 case, and the median duration of treatment was 60 d (range 21–161 d).
Multimodal treatment
Combination treatment comprising surgery as a second or third option (14 patients, 23.3%) or as a nonsurgical approach (10 patients, 21.7%) was recorded in 24 cases (40%) (Table 3). Radiotherapy was provided in 22 cases, comprising tumor volume and lymph node fields; the median dose was 52.1 Gy, ranging between 39.6 and 70 Gy, and fractionation was 1.8 Gy. In this study, concomitant chemotherapy was given in 7 cases, while a complementary systemic treatment was also prescribed in 15 cases. The regimens used were 5-fluorouracil (FU) 1000 mg/m 2 d1–5+CDDP 100/m 2 d1 q3–4w (3 patients), paclitaxel 175 mg/m 2 +CBDCA AUC6 d1 q3w (4 patients), gemcitabine 1000 mg/m 2 d1, d8 + CDDP 75 mg/m 2 q3w (1 patient), epirubicin 60 mg/m 2 +CDDP 50 mg/m 2 q3w (1 patient), M-VAC (1 patient), ifosfamide 1500 mg/m 2 d1–4, CDDP 20 mg/m 2 d1–4 q3w (1 patient), and 5-FU+bleomycin+CDDP (1 patient); 4 patients were recommended hormonal treatment. A 100% dose intensity was reached in only 3 patients (12.5%), 1 belonging to the rare group and 2 to the common group.
Characteristics in Patients Exposed to Multimodal Treatment in Rare Versus Common Groups
NE, neuroendocrine; ypT, histopathologic stage of the primary tumor after neoadjuvant treatment; ypN, histopathologic regional lymph nodes involvement after neoadjuvant treatment; Gy, grays.
In the rare tumor group, the multimodal approach was recommended for 4 patients representing 23.5% of this subpopulation (3 cases of cervix uteri neoplasm and 1 of NE prostatic carcinoma). Radiotherapy was provided in all cases, with the dose ranging between 39 and 70 Gy; the proportion was 1.8 Gy (2 patients) and 2 Gy (2 patients). Brachytherapy was recommended in 1 case (cervix uteri neoplasia), and concomitant CDDP-based chemotherapy was provided in all 3 cases of cervix uteri cancer. Sequential chemotherapy was prescribed in three cases; the mean duration of systemic treatment was 200 d, and a 100% dose intensity was reached in only one case. A second surgery was necessary in two cases of cervix uteri, leading to an R0 excision (Fig. 1).
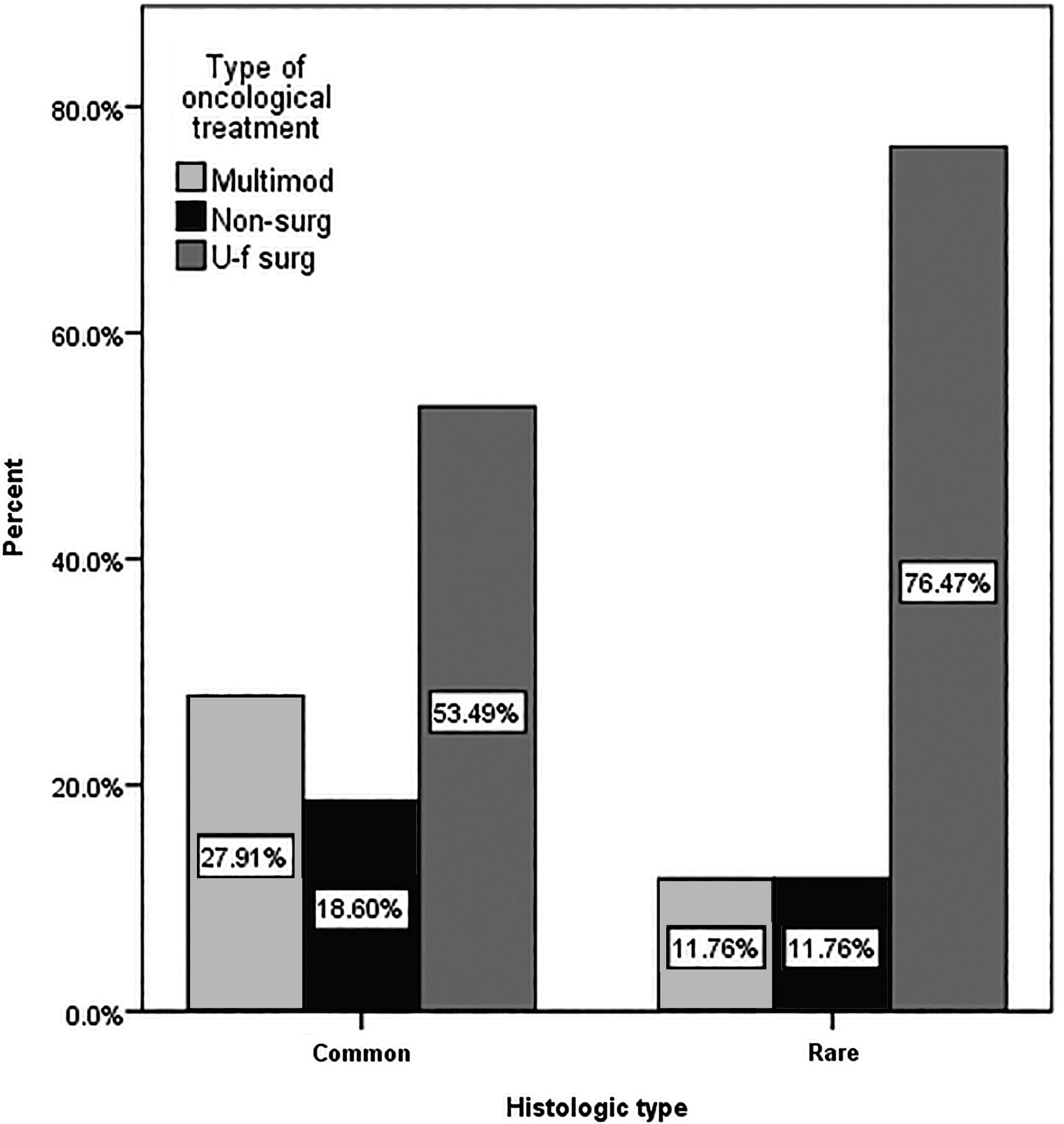
Type of therapeutic sequence according to a rare/common type of tumor. Multimod, multimodal treatment; Non-surg, nonsurgical treatment; U-f surg, upfront surgical treatment.
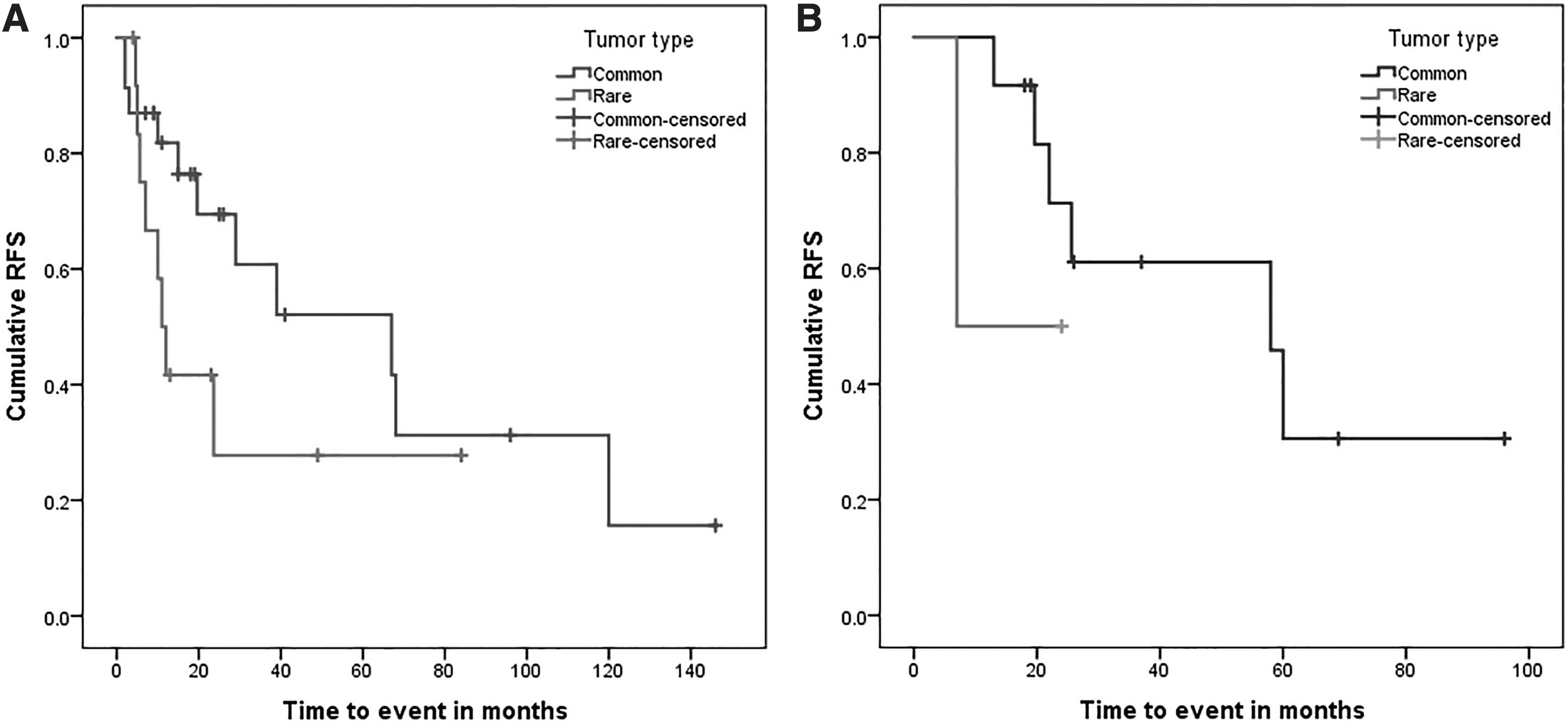
For a median follow-up of 27.5 months (range 2–146 months), relapse was registered in 27 patients (45%), of whom 9 had rare tumors, representing 52.9% of this subpopulation compared with 41.9% (18 patients) in the common group (p = 0.437). By primary tumor site, the relapse rate in patients with bladder tumors was 66.7% (4 patients) in the rare group compared with 42.1% (8 patients) in the common one. In patients with the rare histotype of prostate cancer, the relapse rate was 66.7% (2 patients) compared with 16.7% (1 patient) in the common group, while in cervix uteri the percentages were 25% (1 patient) and 30% (3 patients) and in uterine localization 50% (1 patient) and 71.4% (5 patients; p = 0.356). The estimated median RFS in all the population was 60 months (95% CI: 21.097–98.903); it was 67 months (95% CI: 54.813–79.187) for common histologies and 12 months (95% CI: 0.000–25.74) for rare tumors (log-rank test 4.652, p = 0.031) (Fig. 2).

RFS in rare pelvic cancer patients versus common histologies. RFS, relapse-free survival.
By type of oncological treatment, in all the population, in cases treated by upfront surgery, the median RFS was 29 months (95% CI: 4.83–53.17); by contrast, in patients undergoing sequential surgical treatment, the median RFS was 39 months (95% CI: 0.0–82.14; p = 0.045). In cases treated by nonsurgical multimodal treatment, the comparison could not be run due to the small number of cases (2 patients in the rare group and 8 patients in the common group) (Table 4). The long-rank test was 3.628 (p = 0.163) (Fig. 3).
Estimated RFS in patients that underwent upfront surgery
Median Relapse-Free Survival According to Therapeutic Sequence and Common or Rare Tumor Type
According to primary tumor localization, the median RFS was 29 months (95% CI: 0.76–57.24) for common histology uterine neoplasms compared with 5 months (p = 0.581) in rare cases. In patients with bladder localization, the mean was 68 months (95% CI: 56.59–74.40) in the common group and 11 months (95% CI: 3.32–18.68) in the rare group (Fig. 4).

Estimated RFS in common pelvic cancer patients according to therapeutic approach in common
Relapse was found to be marginally correlated with the type of treatment strategy (p = 0.051), chemotherapy dose intensity (p = 0.058), and irradiation field (only pelvic vs. pelvic and lymph nodes; p = 0.03) where applicable. In the univariate analysis, it was correlated with the histology of the surgical specimen (p = 0.081) and pathologic stage (p = 0.156). Regarding the type of therapeutic sequence, relapse was recorded in more than half of the patients that primarily underwent surgical treatment (19 patients, 51.4%), in 7 patients (53.8%) treated secondarily by surgery, and only in 10% (1 patient) of those under nonsurgical multimodal treatment.
As for patients that experienced relapse, in all the population, 13 cases (51.9%) displayed a bulky disease and 14 cases (48.1%) a nonbulky one; this was confined to one organ in 16 cases (59.3%) and concerned more than two sites in 11 patients (40.7%), principally the lymph nodes (29.6%, 8 patients) and lungs (22.2%, 6 patients) (Table 5). Locoregional recurrence was registered in 6 cases (22.2%). The first line treatment for the recurred disease was chemotherapy or hormonal therapy in 66.7% of cases (16 patients), radiotherapy in 20.8% (5 patients), and salvage surgery in 3 patients (12.5%). Second line chemotherapy was given to 9 patients (56.3%).
Demographics in Relapsed Population Versus Patients Without Recurrence
pT, histopathologic stage of the primary tumor; pN, histopathologic regional lymph nodes involvement; G, histologic tumor's grade; RT, radiotherapy; ypT, histopathologic stage of a primary tumor after neoadjuvant treatment; ypN, histopathologic regional lymph nodes involvement after neoadjuvant treatment.
Nine patients belonged to the rare tumor group: 33.3% (3 patients) presented a low tumor burden, while in 66.7% (6 patients) the relapse was bulky. In the common group, in 61.1% (11 patients), the tumor's load was low compared with high in 38.8% (7 patients; p = 0171). The relapse concerned at least two sites in 6 patients (66.7%) and one site in 3 patients (33.3%) of the rare group and a single organ in the 13 patients (72.2%) of the common group (p = 0.053). In the rare histology group, the recurrence affected the lungs in 2 patients, the liver in 2 patients, and was locoregional in 4 patients; it concerned the lymph nodes or peritoneum in 7 patients and the bones in 4 patients in the common group (p = 0.089). The first line treatment was principally chemotherapy in the rare and common groups: 66.6% (6 patients) compared with 55.5% (10 patients; p = 0.248). Radiotherapy was given to 27.7% (5 patients) in the common group. The second line of systemic treatment was provided to 3 patients in the rare group and 6 patients in the common group.
In patients that recurred, the time to first progression was 4 months with a mean of 6.2 months (95% CI: 2.93–9.36). In the rare group, this was 5 months (mean of 7.8 months, 95% CI: 1.25–16.92). In the common group, this was 4.5 months (mean of 5.23 months, 95% CI: 2.04–8.41; p = 0.517).
Discussion
In their analysis, from a demographic point of view, the authors found 28.3% of cases bearing a rare pelvic malignant tumor similar to the incidence of 20% reported at the European level. 1 While in the same large report, the average age of diagnosis seems to be slightly lower than that for common malignancies localized to the pelvis (60 vs. 69 years) 1 ; in their study there was no difference (59.9 vs. 59.3 years), probably because of the high proportion of cases of cervix uteri and bladder neoplasms, which are more frequent at younger ages.
Regarding the female–male distribution, the literature indicates a twice as high incidence in men based on the mean of the relative incidence of prostate cancer compared with cervical and uterine corpus cancers. 15 In their study, the incidence rate was nearly equal, possibly due to the relatively small number of prostate cancer patients. In both their subgroups, the bladder and female genital tract were most affected, corresponding to global reports. 1,16 In their rare tumor cases, the more frequently encountered histopathological subtypes were NE (prostate and cervix uteri) and carcinosarcoma (uterine corpus). The RARECARE report found high incidences of the infiltrating duct carcinoma of the prostate (0.47/100.000), squamous-cell carcinoma variants of the bladder (0.43/100.000), and soft tissue sarcoma of the uterus (0.50/100.000). 1
In their target population, 76.4% (13 patients) underwent primary surgery and 11.8% (2 patients) received surgery as a second sequence; 2 patients also received nonsurgical multimodal treatment. The type of treatment strategy was found to be significantly influenced by the Charlson score (p = 0.017), site of the primary tumor (p = 0.001), and histopathological type (p = 0.001), as expected.
Concerning the type of therapeutic approach and impact on survival, the authors examined every rare histological subtype in their analysis and compared their findings with the literature. Of the 4 cases of adenocarcinoma of the cervix uteri, representing 23.5% of their subgroup of rare cancers, 1 proved to be an adenosquamous subtype on surgical resection, of stages IIB to IIIB; 3 underwent multimodal treatment; and only 1 was treated by upfront surgery. Median survival was 15.5 months with a range from 2 to 84 months, and relapse was recorded in 1 multimodal treatment case within a year of diagnosis.
In the literature, adenocarcinoma is reported to be 5%–20% of cervical malignancies, mostly at a young age. 17 The 5-year overall survival rates range from 80% in the early stages to 10% in locally advanced disease, 18 the worst prognosis reported for the adenosquamous subtype. 19
For the therapeutic strategy, based on the standard of care in early stages (stages IB-IIA), consisting in radical hysterectomy, regional lymph node dissection, and adjuvant irradiation or concomitant radio-chemotherapy, cervical adenocarcinoma is considered to lack sensitivity to cytotoxic or radiation treatment. 20 In a large analysis (n = 880) of early-stage cervical cancers (IA-B), there was no distinction in the rate of 5-year RFS in squamous carcinomas and adenocarcinoma histologies; however, a difference was observed for the adenosquamous subtype (81% vs. 86%, respectively, p < 0.03). 21 In more advanced stages (n = 1323) with upfront surgery followed by adjuvant treatment, the worst 5-year RFS rate was registered in the adenocarcinoma subtype (66.5%) compared with the squamous and adenosquamous subtypes of carcinomas (83.7% and 79.6%, respectively, p < 0.0001). 22
On the response to radiotherapy or chemotherapy, the rate reported in locally advanced cervical adenocarcinomas (n = 229) was lower than that in their squamous subtype counterparts, reflected by a rate of residual disease of 28.6% compared with 12.9% (p = 0.018) and a 5-year progression-free survival rate difference as well (30% vs. 47.6%, p = 0.044). 23
In their target subgroup, 2 cases were treated by upfront surgery and adjuvant chemotherapy (ifosfamide-CDDP): 1 of carcinosarcoma and 1 of stromal sarcoma. In 1 case, metastatic lung relapse was recorded 5 months after diagnosis. In the literature, leiomyosarcoma is the most common histologic subtype of uterine sarcoma, representing about 1% of all uterine malignancies. Radical hysterectomy is the standard treatment from the early stages, 24 and due to the hematogenous spread pattern, the 5-year relapse rate hardly reaches 70% 25 despite pelvic irradiation, with a high frequency of relapses outside the irradiation field or distant metastases. 26 In the literature, the findings are in favor of performing chemotherapy after surgery. One meta-analysis (n = 360) found a lower risk of distant metastases by adding adjuvant chemotherapy compared with patients exposed to radiotherapy alone (odds ratio = 0.49, 95% CI: 0.24–1.03). 27 Furthermore, in a randomized phase III trial, multimodal treatment led to a borderline 3-year disease-free survival advantage compared with radiotherapy alone in localized uterine sarcomas (n = 81; 55% vs. 41%, p = 0.048). 28
Two of the 9 prostatic cancer cases bore a carcinosarcoma subtype. The patients were aged 51 and 59 years: 1 was treated primarily by surgery followed by gemcitabine-CDDP chemotherapy and 1 by nonsurgical multimodal treatment consisting of external beam radiotherapy (70 Gy) and the triptorelin–bicalutamide combination. A bulky pulmonary metastatic recurrence was registered 28 months after diagnosis in the first case, with a time to progression of 7 months.
Carcinosarcoma of the prostate is a very rare neoplasia, described in about 50 cases in the literature. 29,30 This histology might appear after radiation therapy for a prostate adenocarcinoma 31 ; the mean age of diagnosis is around 66 years. The particularities are normal prostate-specific antigen values and a relatively modest prognosis; the 5-year survival rate is 41% and only 14% at 7 years. 32 Multimodal treatment is started in the early stages, with anthracycline-based perioperative chemotherapy appearing to be beneficial. 33
Another rare histology registered in 2 of their patients with bladder neoplasm is squamous carcinoma (one was a pT4N1 stage and the other pT2Nx). Both were treated first by surgery, followed by gemcitabine-platinum chemotherapy and irradiation. The case without lymph node dissection relapsed in the peritoneum within 1 year of diagnosis, and survival without recurrence in the other case was 69 months.
In the literature, the squamous-cell carcinoma is bilharzial (Schistosoma) infection related in 20%–30% of cases, representing 2%–5% of bladder cancer and affecting patients aged around 70 years; the standard treatment is radical cystectomy. 34 The 5-year survival rates are about 50%, and relapse is mostly local. 35 In a meta-analysis of 10 studies of the localized disease, even though this histological subtype is recognized as chemotherapy resistant, the multimodal approach seems to bring about a survival benefit. Perioperative radiation was found to confer a survival advantage compared with radical cystectomy alone (disease-free survival: 48% vs. 29%). 36
The last rare pelvic histology pointed out in this section is small-cell NE. This represents 0.3%–1% of all prostatic carcinomas de novo and ∼10% after androgen deprivation therapy, usually in castration-resistant prostate tumors. 37,38 About 50% of NE prostate tumors have pure small-cell carcinoma at initial diagnosis; the rest develop NE differentiation once a tumor recurs after androgen deprivation therapy. 39 Usually metastasized in the liver, this does not correlate with the serum PSA level and has a median progression-free survival of <12 months. 40,41
There is no specific standard of care regarding NE prostate carcinomas: transurethral resection of the prostate and the wait-and-see attitude are not recommended. 40 As in small-cell pulmonary carcinoma, aggressive multimodal treatment is indicated; etoposide–platinum chemotherapy following surgical treatment or definitive radio-chemotherapy 42 can lead to an improvement in disease-free survival of 12–15 months. 43 –45 As regards hormonotherapy, a 1994 review showed that NE prostate carcinoma is a rather hormonal-resistant tumor. 46
The bladder is affected in ∼1% of NE, usually in older male patients. 47 Neoadjuvant platinum-containing chemotherapy followed by either radical cystectomy or radiotherapy alone, regardless of the stage, is recommended 48 compared with surgery alone. A 78% 5-year disease-specific survival rate (vs. 36%, p = 0.026) was reported in 26 patients, 49 as well as a median overall survival of 159.5 months (vs. 18.3 months, p = 0.03) in patients exposed to four courses of etoposide and CDDP (n = 48). 50 In their small sample, the authors registered only 1 case of NE differentiation of a prostate carcinoma (11% of all the cases of prostatic cancers) in a patient of 62 years treated by radical surgery, followed by bicalutamide and in whom a bulky local relapse was registered 9 months after diagnosis, with the next progression of 10 months after chemoradiotherapy.
As regards small-cell bladder cancer, the authors also found only 1 case (4% of all the cases of bladder cancer), in a male patient of 76 years treated by upfront radical cystectomy. Early relapse occurred in the liver 7.6 months after diagnosis, during his adjuvant etoposide–platinum chemotherapy, with a second progression of 3 months.
Conclusions
Their report represents a small contribution to the unofficial database of rare cancers. Although the study was run in a specialized center, the number of cases able to be included was low partly due to the absence of a national registry. The survival outcomes followed the findings in the literature. In rare pelvic tumor patients, the outcome seems to be poorer than those affected by common histologies, mostly in the bladder, while multimodal treatment appears to be beneficial. Besides the limitation of the small number of localized rare pelvic cancer cases, anal, vaginal, and testicular localizations were excluded because of the lack of rare histologies in the analyzed files.
Footnotes
Acknowledgment
The authors thank Mr. Sorin S. Opris for the preparation of the article for submission (layout, chart, and table preparation).
Disclosure Statement
The authors declare their responsibility for the content of this publication. All the authors contributed to the conception and content of the article and approved the final version, as well as submission. No competing financial interests exist.