
Abstract
Background:
Epidermal growth factor receptor (EGFR) mutations are associated with leptomeningeal metastases (LM) of nonsmall cell lung cancer and sensitivity to tyrosine kinase inhibitor (TKI) treatment. Owing to the difficulty of obtaining carcinomatous meningeal tissue for analysis, cerebrospinal fluid (CSF) might be an alternative.
Objective:
To investigate the EGFR mutation detection in the CSF of lung adenocarcinoma patients with LM.
Methods:
Twenty-five lung adenocarcinoma patients with LM diagnosed by CSF cytology were retrospectively evaluated. The results of EGFR mutation detection in CSF, the treatment plan, and clinical outcome information were recorded.
Results:
Nineteen patients had a known EGFR status in their primary tumors. Twenty patients received EGFR mutation analysis in CSF after LM diagnosis and 14 of them with a known EGFR mutation status of both primary tumors and CSF. Ten (71.4%) had the same EGFR gene status. In primary tumors, no T790M mutations were detected, whereas in CSF, 2 L858R cases and 1 19del case had T790M mutations at the same time. The detection rate of T790M mutations in CSF was 18.1% (2 of 11) in all cases with EGFR-sensitive mutations in the primary lesion.
Conclusions:
EGFR mutation detection in CSF of lung adenocarcinoma patients with LM might be an alternative when leptomeningeal biopsy cannot be applied and may help to guide TKI treatments.
Introduction
About 40% of lung adenocarcinomas may metastasize to the brain, and a substantial concordance of EGFR (epidermal growth factor receptor) mutation status between primary lung cancer and brain metastases (BMs) has been reported. 1,2 According to our previous study, it was found that 52% (26 of 50) NSCLC (nonsmall cell lung cancer) patients with BM harbored EGFR mutations in primary tumors, including 62.2% 19del mutation and 37.8% L858R mutation. 3 Li et al. 4 found that 19del had a trend of increasing the incidence of BMs than exon 21 mutation (odds ratio = 1.44; 95% confidence interval, 0.77–2.68; p = 0.252). The prognosis of NSCLC patients with brain parenchymal metastasis is significantly improved after TKI (tyrosine kinase inhibitor) treatment, but LM (leptomeningeal metastases) is still difficult to treat, with a reported median overall survival of <3 months. 5
In the era of targeted treatment, it is generally believed that a biopsy of progressive lesions should be performed to identify the gene status (including EGFR) and determine the expected efficacy or drug resistance to TKIs, to guide subsequent treatment. 6 Lung cancer patients with EGFR mutations 19del and L858R have been reported to show up to a 70% greater response rate to first and second generation TKIs, such as gefitinib, erlotinib, afatinib, and dacomitinib. 7 However, when a T790M mutation appears, these drugs lose their efficacy and the third generation TKI, osimertinib, is prescribed. 8 Therefore, analyzing the EGFR mutation status in lung cancer is crucial for selecting the most effective drug therapy.
However, in some patients, it might be difficult to obtain samples for EGFR status detection with biopsy procedures. For example, Hasegawa et al. 9 found that 11 lung adenocarcinoma patients with BM were not suitable for craniotomy, since the trauma of brain metastasis biopsy would have been too great. Exfoliated cells or free nucleic acids from cerebrospinal fluid (CSF) might substitute for biopsy, since meningeal tissue is in direct contact with CSF and has fewer background cells than plasma.
As the survival of advanced lung adenocarcinoma patients becomes longer and diagnostic accuracy improves, the diagnostic rate of LM will also increase. 10 Therefore, improving the survival of lung adenocarcinoma patients with LM is an urgent clinical need. The purpose of this study was to investigate EGFR mutation detection in the CSF of lung adenocarcinoma patients with LM.
Patients and Methods
Patients
This retrospective study was approved by the Ethics Committee of Huashan Hospital, Fudan University (No. KY2017-010). All of the patients read and signed the informed consent form. All lung adenocarcinoma patients diagnosed in the Department of Oncology, Huashan Hospital, Fudan University, Shanghai, China, from January 1, 2013, to December 31, 2016, were reviewed. Eligibility criteria were lung adenocarcinoma patients with cytopathology-confirmed tumor cells in the CSF.
Data from 25 lung adenocarcinoma patients with LM were included, which were gender, age, physical status, LM-related symptoms (meningeal irritation and intracranial hypertension), adverse reactions after lumbar puncture, pathological diagnosis of the primary tumor, routine biochemical examination of CSF, tumor markers of CSF supernatant and serum, affected extracranial organs, enhanced magnetic resonance imaging (MRI) of the brain and/or the spinal cord, the type of EGFR mutation in the CSF at the first diagnosis of LM, first-line treatment plan after LM diagnosis, time of stabilization of the neurological symptoms after first-line treatment, and overall survival after LM diagnosis. The follow-up ended on December 31, 2017.
Lumbar puncture
Lumbar puncture was used to obtain 5 mL of CSF after the clinical diagnosis of LM from lung adenocarcinoma. Two milliliters of CSF was used for routine biochemical tests and tumor markers detection in the CSF supernatant. The remaining 3 mL of CSF was rapidly centrifuged and analyzed by cytopathology. If tumor cells were found, LM from lung adenocarcinoma was diagnosed. 11 Next, lumbar punctures were conducted to obtain another 10 mL of CSF for EGFR mutation detection.
EGFR mutation analysis
EGFR mutation detections were performed using an amplification refractory mutation system (ARMS; Xiamen AmoyDx Biological Technology, Xiamen, China), droplet digital polymerase chain reaction (ddPCR; Bio-Rad Laboratories B.V.), or next-generation sequencing (NGS; Illumina, Inc., San Diego, CA).
Detection of CSF tumor markers and drug concentrations in CSF and serum
The tumor marker concentrations of carcinoembryonic antigen (CEA), cytokeratin 19 fragment (Cy-211), neuron-specific enolase (NSE), and cancer antigen 19-9 (CA19-9), were determined by immunoassay (Cobos 8000; Roche Diagnostics, Basel, Switzerland).
Drug concentrations in the CSF and serum during the same period were measured by reverse-phase high-performance liquid chromatography (Agilent 6410B, Santa Clara, CA).
Statistical analysis
All statistical analyses were performed using SPSS ver. 23.0. The mean ± standard deviation was used to describe data with a normal distribution, whereas the median was used to describe data with a skewed distribution. Counts and proportions were used to describe classified data, and Kaplan–Meier survival curves were constructed to calculate the median overall survival after LM diagnosis. A p-value <0.05 was considered to be statistically significant.
Results
Clinical characteristics of 25 lung adenocarcinoma patients with LM
Data from a total of 407 patients with lung adenocarcinoma were reviewed, of whom 25 were diagnosed with LM. The median age was 53 years and 56% of patients were men. Intracranial hypertension or meningeal irritation was the most common symptom. About 50% of the patients did not have extracranial metastases (Table 1).
Characteristics of 25 Lung Adenocarcinoma Patients with Leptomeningeal Metastases
Examination of 25 lung adenocarcinoma patients with LM
Five of the 25 (20%) patients had a typical meningeal enhancement on examination of the brain by MRI, and 2 of them had parenchymal brain metastasis at the same time. Of the remaining 20 patients, 5 received enhanced MRI of the spinal cord, and abnormal leptomeningeal enhancement was found in 4 cases. Seventeen patients received a test for CSF tumor markers, of which 16 (94.1%) had positive results including CEA (14 cases, 119 [12.75–4991 ng/L]), Cy-211 (3 cases), CA19-9 (2 cases, 283 and 66.24 ng/L, respectively), and NSE (2 cases) (Table 2). The levels of blood serum tumor markers in patients with positive CEA (32.8 [6.24–1638 ng/L]) and CA199 (46.23 and 106.84 ng/L, respectively) in CSF were also elevated.
Judging Criteria for Leptomeningeal Metastasis Diagnosis of Lung Adenocarcinoma Patients
+, Positive; −, negative; CSF, cerebrospinal fluid; empty, undetected; MRI, magnetic resonance imaging.
EGFR status of paired primary lesions and CSF of 25 lung adenocarcinoma patients with LM
Nineteen patients were EGFR-status known in their primary tumors, including 6 cases of wild type, 7 cases of L858R mutation, 5 cases of 19del mutation, and 1 case of L861Q mutation. Five of the 25 patients refused consent for EGFR mutation analysis, and the remaining 20 patients received EGFR mutation detection of CSF after LM diagnosis. Fourteen patients received EGFR mutation detection of both their primary cancer and CSF. Circulating tumor DNA (ctDNA) yields from CSF samples were between 9.5 and 50.5 ng/mL in our study. Of these 14 patients, 10 (71.4%) had the same gene status, including 1 case of wild type, 3 cases of 19del mutation, and 6 cases of L858R mutation.
Among the 4 cases of different EGFR gene status, EGFR wild type was detected in 2 cases of the primary lung cancer tissue, whereas 19del mutation and L858R mutations were detected in the CSF of the same patients with subsequent LM. The 2 other patients had L858R and 19del mutations in the primary tumors and L858R plus T790M as well as 19del plus T790M mutations in the CSF (Supplementary Table S1.
EGFR status-based treatment
Twenty patients with known EGFR status in the CSF were treated with corresponding systemic EGFR-TKI therapy (for patients with EGFR-sensitive mutations), or cytotoxic drugs (for patients without EGFR-sensitive mutations). Two patients with L861Q and L858R mutations preferred chemotherapy and one 19del patient diagnosed with LM also chose to have chemotherapy after receiving several different TKIs (Table 3).
Epidermal Growth Factor Receptor Status of Primary Lesions and Cerebrospinal Fluid of 25 Lung Adenocarcinoma Patients with Leptomeningeal Metastasis
Still alive at last follow-up.
Double dose of TK.
ARMS, amplification refractory mutation system; chemo, chemotherapy; ddPCR, droplet digital polymerase chain reaction; EGFR, epidermal growth factor receptor; LM, leptomeningeal metastases; NGS, next-generation sequencing; OS, overall survival; RT, radiotherapy; TKI, tyrosine kinase inhibitor; UA, unavailable.
Up to the end of the study (December 31, 2017), the median time of stabilization of neurological symptoms after first-line treatment was 4 months (range, 0–18 months), whereas the neurological symptoms of 4 patients were not relieved. The median overall survival after LM (post-LM survival) was 10 months (range, 1–47 months) (Fig. 1).
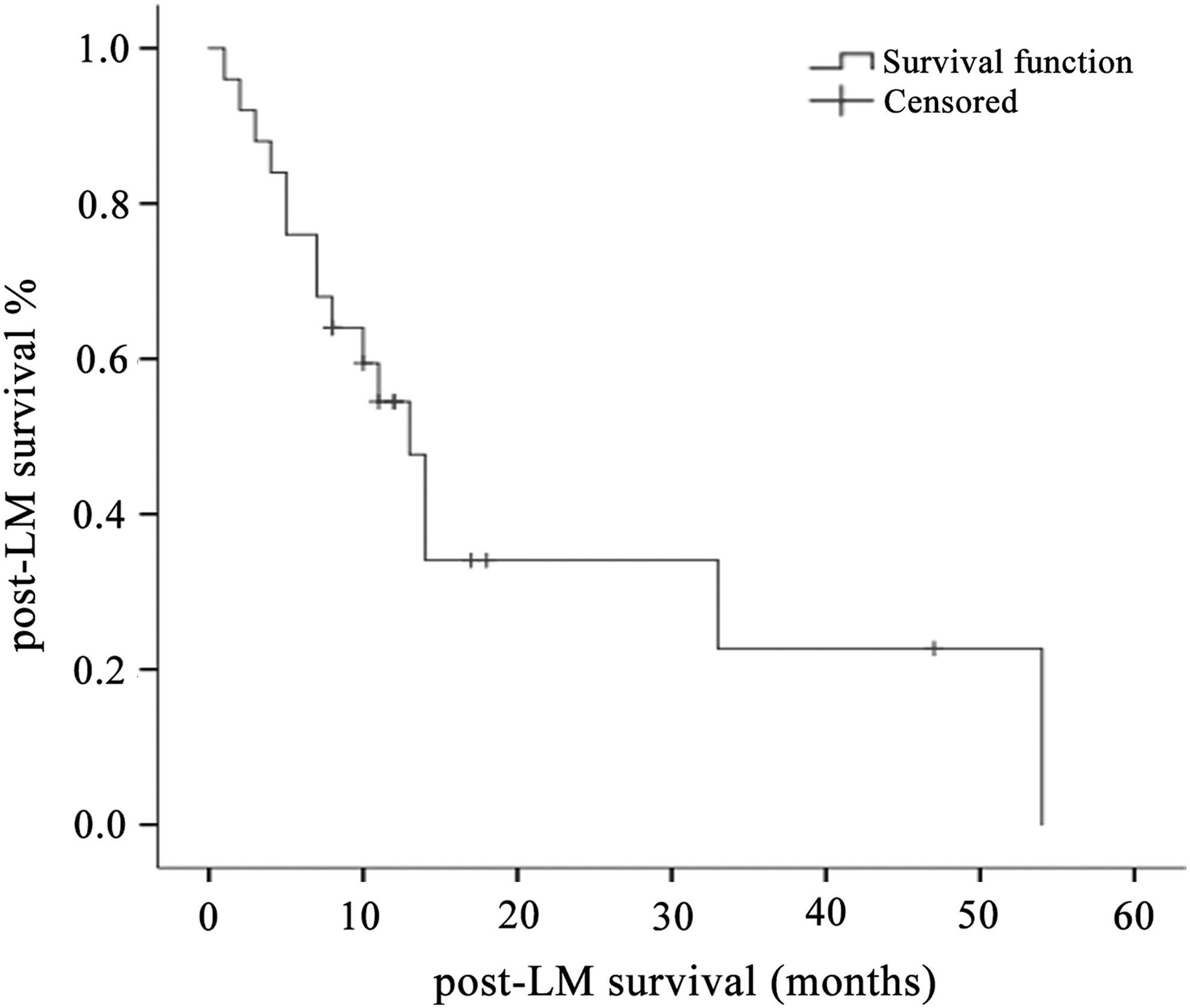
Kaplan–Meier curves for lung cancer patients with LM. LM, leptomeningeal metastases.
The median post-LM survival of the 20 patients who received EGFR mutation detection in the CSF was 10.5 months (range, 1–47 months), and 5 patients without EGFR mutation detection in the CSF had a median survival of 5 months (range, 2–18 months). Among them, patient No. 3 and patient No. 5 were originally treated with icotinib and received EGFR mutation detection in CSF after the diagnosis of LM. The drug concentration of the CSF increased correspondingly after the dose of icotinib was doubled, and patients achieved stable disease for another 4 and 12 months, respectively (Table 4).
Drug Concentrations of Cerebrospinal Fluid and Serum Before and After the Double Dose of Icotinib (ng/mL)
Kaplan–Meier survival curves for lung cancer patients with LM.
Lumbar puncture-related complications
Two of the 25 patients experienced headache related to intracranial hypotension after lumbar puncture, which was completely relieved after 2 d of bed rest and rehydration. Three patients experienced pain in the waist near the puncture site, which was completely relieved within 1 week of treatment with nonsteroidal drugs and bed rest. None of the patients suffered serious complications.
Discussion
In this study, 20 patients with LM received EGFR mutation detection in CSF, and 14 of them also received gene detection in the corresponding primary lesion, with a coincidence rate of 71.4%. It was in good agreement with previous studies, which noted that the EGFR mutation status in lung adenocarcinomas was relatively consistent between primary and metastatic sites. 12 In our study, 6 patients did not receive EGFR mutation detection in the primary lesion, but their EGFR status was analyzed after LM was diagnosed. Detection of EGFR mutations in the primary lesion was not performed at the onset of the disease because of various factors, including the lack of patient consent. Therefore, EGFR mutation detection in the CSF of patients with LM can be used as a supplement when the EGFR mutation status of the primary tumors is not available.
Patients No. 3 and No. 5 progressed after icotinib treatment. No T790M mutations were detected in the CSF of them, but the sensitive L858R mutation was still detected. The patients were treated with a double dose of icotinib subsequently and the drug concentration of CSF was increased correspondingly. Stable disease of another 4 months and 12 months was achieved, which supported the nonexisting T790M mutations.
In this study, T790M mutations in CSF samples was in 2 of 11 (18.1%) of the cases with EGFR-sensitive mutations (including 19del and L858R mutations) in the primary lesion, which is similar to a previous study of 17%. 13 However, it was higher than in other studies that reported 4% 14 and 7.2%. 15 In the latter two studies, there were high discrepancies between T790M mutations in samples derived from CSF and brain tumor biopsies, since T790M percentages were 80% and 78% in biopsy samples, respectively. There were three possible reasons. First, incomplete penetration of TKIs into the CSF; second, spatial and temporal heterogeneity of T790M mutations; and third, difficulties with CSF cancer cell isolation. 15 In a previous report, it has been suggested that T790M mutations may be associated with a better prognosis of LM patients, but it could not be confirmed in our study. 13
This study had a number of weaknesses. First, the disease is so rare that it is not really suitable for a prospective study; therefore, a retrospective analysis was used. The results were also affected by the small cohort size and various sources of bias. Furthermore, the nucleic acid content of CSF was as low as 9.5 and 50.5 ng/mL in this study, and the amount of CSF that could be collected was usually <10 mL. So genes such as ALK and ROS1 cannot currently be detected. In addition, different methods for EGFR mutation detection were used, including ddPCR, NGS, and ARMS. The authors tried their best to reanalyze all of the samples with ddPCR at the same time, Yet 5 of 20 patients' nucleic acid content of CSF were too low to reanalyze. Now direct comparative studies of three EGFR mutation detection methods in CSF are being conducted, and adopting a unified detection method in future studies is being attempted.
Conclusions
The present results suggest that EGFR mutation detection in CSF of lung adenocarcinoma patients with LM might be an alternative diagnostic tool in cases where a leptomeningeal biopsy cannot be performed and also help to guide TKI treatment regimes.
Footnotes
Acknowledgments
Baoshan District Committee of Science and Technology (14-E-28), Shanghai Municipal Committee of Health and Family planning (201440584), Shanghai Municipal Natural Science Foundation (16ZR1404300), and Scientific Research Foundation Huashan Hospital (787) are thanked for funding this study.
Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table 1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.