
Abstract
Objective:
To investigate and discuss the clinical value of positron emission tomography-computed tomography (PET-CT) combined with ultrasound in detection of primary tumors in patients with malignant ascites (MA).
Materials and Methods:
A total of 122 malignant tumor patients with ascites as the initial symptom and 48 patients with benign ascites were enrolled in this study. All patients underwent PET-CT and abdominal B-ultrasound examinations. The corresponding specificity, sensitivity, accuracy rate, positive predictive value, and negative predictive value of PET-CT, abdominal B-ultrasound, and combined detection group were recorded, respectively, with pathological findings as the gold standards. Statistical Product and Service Solutions 17.0 software was used for statistical analysis. p < 0.05 suggested that the difference was statistically significant.
Results:
The detection rate of primary foci through PET-CT was 79.5%, of which the detection rate of primary foci of MA derived from gastric cancer was the highest. The detection rate of primary foci through B-ultrasound was 62.5%, which is the highest for MA derived from ovarian cancer. B-ultrasound had the highest specificity in diagnosing the primary foci of MA (73.2%), PET-CT had the highest sensitivity in diagnosing the primary foci of MA (91.7%), and PET-CT combined with abdominal B-ultrasound had the highest sensitivity and accuracy in diagnosing the primary foci of MA (98.1% and 89.1%, respectively). The diagnostic accuracy rate of B-ultrasound was the highest in detecting tumors >5 cm (77.0%), whereas that of PET-CT was the highest in detecting tumors of 3–5 cm (84.2%).
Conclusion:
The PET-CT combined with ultrasound is conducive to improving the diagnostic efficiency for primary tumors in patients with MA.
Introduction
Ascites, a common symptom in clinic, is caused by colitis, peritoneal malignancy, hepatopathy, tuberculous peritonitis, cardiac insufficiency, nephropathy, and so on, which can be divided into benign and malignant types. Clinically, the treatment protocol and prognosis of ascites induced by malignant tumors are significantly different from those by benign lesions, so it is of great significance to define the cause of ascites. Malignant ascites (MA) is a common complication of advanced cancers, mainly indicating the metastasis, relapse or progression of intra-abdominal or extraperitoneal malignant tumors such as gastric cancer, ovarian cancer, and osteosarcoma. MA patients usually have poor survival and quality of life due to such complications as abdominal distension or pain, dyspnea, malnutrition, and sepsis. These patients are not considered suitable for surgical resection, whereas their survival and quality of life are ameliorated very little by means of traditional palliative treatments, including conservative treatment, abdominal paracentesis, and systemic chemotherapy. However, how to distinguish benign and MA, especially the early diagnosis of MA, is still a problem in clinical practices. Currently, in terms of the identification and diagnosis of ascites, its cytological examination has become the gold standard for definite diagnosis of MA. 1 Despite high specificity, this examination possesses a relatively low sensitivity and can easily result in missed diagnosis and repeated detection after multiple ascites acquisition, delaying the best timing for treatment to some extent and increasing the patients' pains due to repeated abdominal paracentesis. No tumor markers with high sensitivity and specificity have been discovered among various complex causes of MA. Some scholars 2 argue that the combined detection of tumor markers in the serum and ascites can increase its diagnostic value. Studies 3 –5 have manifested that laboratory indexes such as vascular endothelial growth factor, matrix metalloproteinases, deoxyribonucleic acid aneuploid, and human leukocyte antigen have certain clinical values in MA diagnosis, which, however, have limitations in clinical application. The tumor markers have certain sensitivity and specificity in diagnosing MA, but the diagnostic value varies greatly from indexes to indexes, and some limitations exist in the diagnosis of primary foci. 6
18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) is a kind of noninvasive diagnostic technique utilizing the difference in biochemical metabolism of benign and malignant tissues, which is widely applied to identify benign lesions and malignant tumors. 7 The integrated functional imaging and anatomical imaging of PET-computed tomography (CT) have increased the diagnostic accuracy. Since metabolic changes of the malignant tumors may occur before gross anatomical changes, PET-CT can complement conventional imaging and possess high sensitivity. 8 Nevertheless, FDG may accumulate not only in malignant tumors but also in some benign lesions, thus restricting the specificity of FDG PET-CT imaging. Transabdominal ultrasound is also regarded as an effective diagnostic tool for MA detection. 9
So far, there have been few research reports on the role of PET-CT in assessing the primary foci of MA, and the clinical value of PET-CT combined with ultrasound in detecting primary tumors in MA patients has been not reported. In this research, a group of patients who had ascites as the initial symptom, tumor cells found in the ascites and primary tumors ultimately detected were observed, so as to investigate the clinical value of PET-CT combined with ultrasound in detecting primary tumors in MA patients.
Materials and Methods
Clinical case data
A total of 122 malignant tumor patients (gastric cancer, ovarian cancer, and intestinal cancer) with ascites as the initial symptom, admitted in the hospital from January 2017 to January 2018, were enrolled in this study. The inclusion criteria included a confirmed pathological diagnosis of ascites with gastric or gastroesophageal junction adenocarcinoma, ovarian cancer, or intestinal cancer but without prior systemic medical therapy for cancer. The exclusion criteria included any other previous malignancy. All patients underwent PET-CT and abdominal B-ultrasound examinations. Tumor cells were detected in the ascites and finally determined as primary foci. The clinical characteristics of enrolled patients are shown in Table 1. Another 48 patients who were diagnosed with benign ascites were also recruited. The ascites in all patients was cytology positive. All the involved patients or their family members signed the informed consent, and the study was approved by the Ethics Committee of The Affiliated Hospital of Chengdu Medical College.
Clinical Case Data of Enrolled Tumor Patients
PET-CT examination
The scan was performed from the skull base to the proximal femur using the PET-CT scanner manufactured by GE Company (model: Discovery LS, GE Healthcare). All the patients were intravenously injected with FDG imaging agent (3.7–7.4 MBq/kg) as per the body mass after fasting for 6–8 h, followed by image acquisition after the patients rested in a quiet and dark condition for 1 h. As for the image analysis, the imaging results were separately analyzed by two experienced nuclear medicine physicians, and, in case of disagreement, the analysis results were determined by superior physicians through consultation.
Analysis of diagnostic efficiency
The corresponding specificity, sensitivity, accuracy, positive predictive value and negative predictive value of PET-CT, abdominal B-ultrasound, and combined detection group were recorded, respectively, with pathological findings as the gold standards. Finally, the PET-CT maximum standardized uptake (SUVmax) and abdominal B-ultrasound were subjected to logistic regression analysis, and the area under curve of receiver operating characteristic was utilized to compare the diagnostic efficiency of tumor marker, PET-CT, and combined detection group in primary foci of MA.
Statistical analysis
Statistical Product and Service Solutions 17.0 software was used for statistical analysis. The measurement data were expressed by mean ± standard deviation (SD) (
Results
Detection of primary foci of MA through PET-CT
Among the 122 MA patients, the detection rate of primary foci through PET-CT was 79.5%, and the detection rates of different types of primary tumor were different, of which the detection rate of primary foci of MA derived from gastric cancer was the highest (81.3%) (p = 0.000) (Table 2 and Figure 1).

Detection Rate of Different Primary Tumors of Malignant Ascites Through Positron Emission Tomography-Computed Tomography
PET-CT, positron emission tomography-computed tomography.
Detection of primary foci of MA through abdominal B-ultrasound
Among the 112 MA patients, the detection rate of primary foci through abdominal B-ultrasound was 62.5%, which was different among varying types of primary tumor, and the detection rate of primary foci of MA derived from ovarian cancer was the highest (62.9%) (p = 0.000) (Table 3).
Detection Rate of Different Primary Tumors Through B-Ultrasound
Diagnostic efficiency of PET-CT combined with abdominal B-ultrasound for primary foci of MA
The diagnostic efficiency of the three groups of diagnostic methods was compared. The results indicated that the B-ultrasound had the highest specificity in diagnosing the primary foci of MA (73.2%), PET-CT had the highest sensitivity in diagnosing the primary foci of MA (91.7%), and PET-CT combined with abdominal B-ultrasound had the highest sensitivity and accuracy in diagnosing the primary foci of MA (98.1% and 89.1%, respectively) (p = 0.05) (Table 4 and Fig. 2).
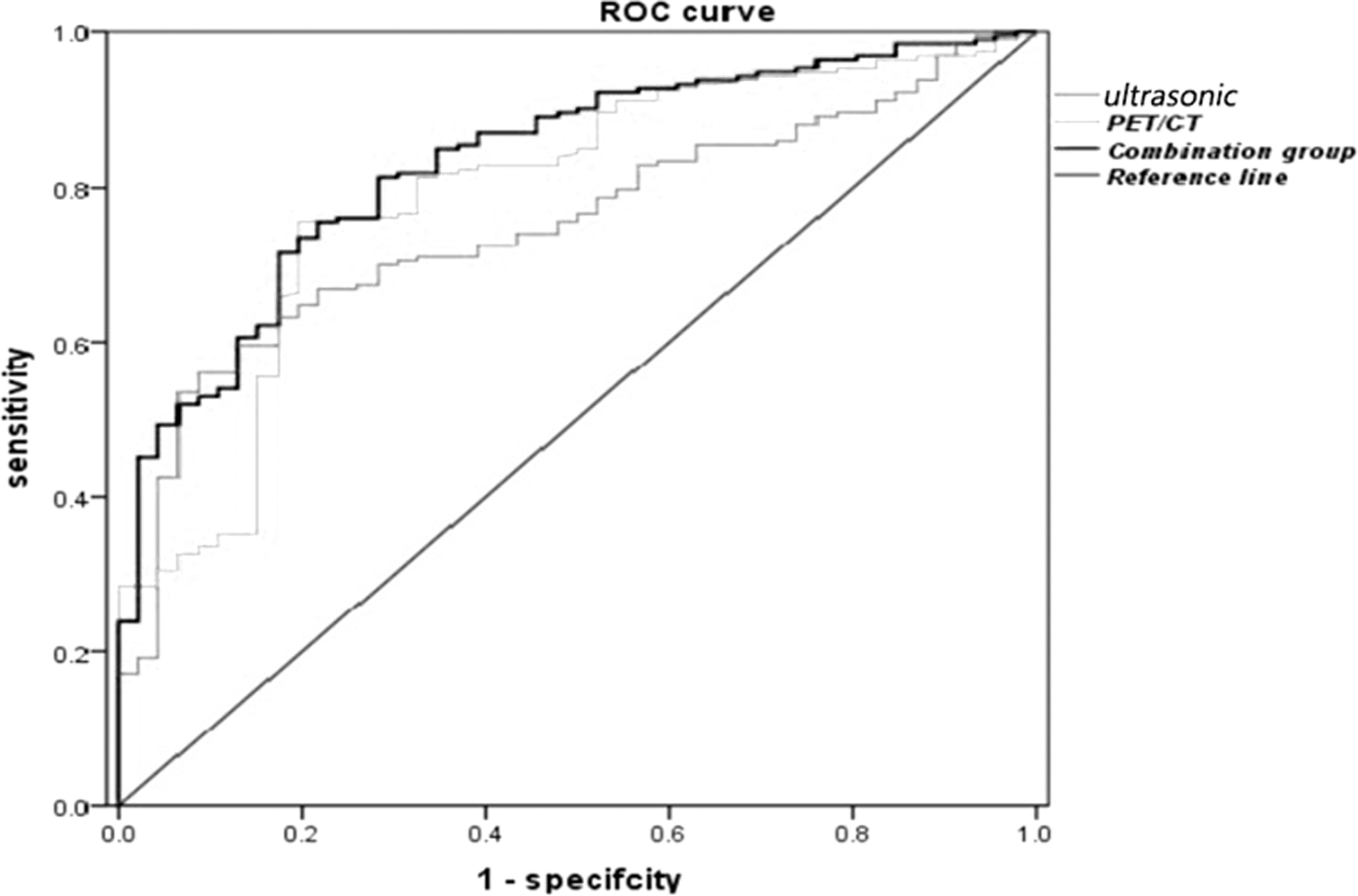
Comparison of diagnostic efficiency among groups through ROC curve. ROC, receiver operating characteristic.
Comparison of Diagnostic Efficiency Among Groups
p < 0.05.
Comparison of accuracy rate in different tumor diameters among groups
The primary tumors were divided into different groups according to the diameter of masses, and the accuracy rate in different tumor diameters was compared in each group. It was revealed that the diagnostic accuracy rate of B-ultrasound was the highest in detecting tumors >5 cm (77.0%), whereas that of PET-CT was the highest in detecting tumors of 3–5 cm (84.2%). However, the accuracy rate of combined detection in diagnosing different sizes of tumor was higher than that of single detection (p = 0.05) (Table 5).
Comparison of Accuracy Rate in Different Tumor Diameters Among Groups
AUCROC, area under curve of receiver operating characteristic.
Discussion
Ascites may be triggered by various diseases. In this research, the most common causes of ascites were gastrointestinal carcinoma, peritoneal tuberculosis, and ovarian cancer. Although biochemical examination, cytological examination, ultrasonic examination, and CT examination are the most frequently applied diagnostic methods for ascites, they all have some limitations. As a multisystem disease, ascites can be caused by a variety of diseases all over the body. Previous studies have reported that PET-CT has the advantage of positioning primary and metastatic foci due to its high sensitivity to multiple tumors and function of whole body imaging.
Most studies 10,11 focus on the capability of PET-CT in detecting peritoneal cancer at present. The role of PET-CT in diagnosing the primary foci of MA is rarely discussed in published literature, whereas early diagnosis of the cause of primary MA is crucial to formulate appropriate clinical treatment protocols and predict the prognosis. Therefore, it is necessary to first evaluate the effect of PET-CT on locating the site of primary diseases of ascites. Existing studies 12 –14 have manifested that FDG PET is able to identify the primary tumors in 6%–55% patients with unknown primary and metastatic carcinomas. In addition, ultrasound examination has also been demonstrated to have several advantages in the diagnosis of tumor differentiation as it can be used to categorize ovarian and adnexal masses, and pattern recognition can accurately diagnose some of the classic-appearing nonneoplastic entities, benign neoplasms, and malignancies. However, the sonographic appearance of an ovarian mass is not pathognomonic. Therefore, a multiparametric model for risk assessment is appropriate and more accurate in distinguishing between benign and malignant ovarian masses. 15 In this research, the sensitivity of PET-CT in detecting the primary lesions of MA was 91.7%, which is higher than that in previous findings. In addition, PET-CT combined with B-ultrasound had higher sensitivity in detecting the primary foci of MA.
The sensitivity of PET-CT in detecting primary lesions was also higher than that of simple B-ultrasound, of which the diagnostic rate of MA derived from gastric cancer was the highest (81.3%), higher than those of MA derived from ovarian cancer and intestinal cancer. It is possibly related to feces in the intestine and limited density resolution. However, false negative or false positive results of PET-CT still exist. According to this research, there were 16 false negative results of PET-CT for primary lesions. The sensitivity of PET-CT is mainly determined by the FDG accumulation in tumor and tumor size, based on which there might be three reasons for the false negative results in this research. First, several special histologic subtypes were determined, which manifested poor FDG accumulation and led to false negative results. There were false negative results in 16 cases of sigmoid colon cancer, gastric cancer, and poorly differentiated ovarian adenocarcinoma. The low expression of glucose transporter-1 is one reason for low FDG uptake, namely low ratio of hexokinase to glucose phosphatase, in those cases. 7 Second, it was shown in this research that tumor size also affected the sensitivity of PET-CT in detecting primary causes. According to previous reports and this research, the FDG accumulation in tumors is correlated with the tumor size. 16 The false negative rate increases along with the decreased tumor size. 8 Third, the PET-CT may be unable to discover primary lesions because of slow growth of tumor or tumor growth restrained by the immune system. The mechanism of metastasis in the abdomen still remains controversial, and it was reported in previous research that 17,18 the metastasis is transmitted in the peritoneum in many ways, such as transmission directly along with the peritoneal ligament, mesentery, and omentum, seeding through ascites, as well as dissemination through lymph node extension and embolus blood. Some studies have also described the FDG PET images of typical abdominal metastasis. 19 As shown in this research, defocus, nodules, or diffuse infiltrating high uptake were displayed on the characteristic patterns, and smudged signs, nodular opacities, and omental lumps were formed.
The analysis of SUVmax, a semiquantitative index for consumption of glucose, may be conducive to differentiating malignant and benign ascites because the SUVmax of MA is remarkably higher than that of physiological peritoneal uptake (healthy volunteers) and benign ascites. Nevertheless, it was found that the SD of SUVmax was relatively high in malignant diseases, which overlapped in benign and MA, indicating the complexity and difficulty of PET-CT diagnosis. SUVmax has a correlation with tumor size, and it was revealed in this research that the accuracy rate of PET-CT was the highest in diagnosing primary foci of 3–5 cm, whereas that of B-ultrasound was the highest in diagnosing primary foci >5 cm. Therefore, it is helpful to combine the PET-CT with B-ultrasound, tumor markers, and other examinations under certain conditions.
Conclusion
In this research, although FDG PET-CT possessed the limitation of high cost, it was helpful for differential diagnosis and detection of primary foci of MA. The PET-CT combined with B-ultrasound can accurately and timely diagnose the primary foci, which can lower the costs and benefit patients in the long run.
Footnotes
Disclosure Statement
No competing financial interests exist.