
Abstract
Purpose:
CD4+CD25+Foxp3+ regulatory T (Treg) cell-mediated immunosuppression has been implicated as a crucial mechanism of tumor immune cell escape in nonsmall cell lung cancer (NSCLC). However, little is known concerning the specific role of CD4+CD25−Foxp3+ Treg cells in NSCLC. The aim of this study was to investigate the frequency of circulating CD4+CD25−Foxp3+ Treg cells and their role in NSCLC.
Methods:
The frequencies of Treg, T helper (Th)1, Th2, and Th17 cells in peripheral blood were separately measured in 36 NSCLC patients and 20 healthy controls (HCs) using flow cytometry. Serum cytokine concentrations were determined using cytometric bead arrays.
Results:
The frequencies of circulating CD4+CD25+ T cells and CD4+CD25+Foxp3+ and CD4+CD25−Foxp3+ Treg cells were significantly higher in advanced-stage NSCLC patients compared with patients with limited-stage NSCLC. The frequencies of circulating CD4+CD25+Foxp3+ and CD4+CD25−Foxp3+ Treg cells were negatively correlated with interleukin (IL)-17, but positively correlated with serum IL-10 levels. In addition, the Th17/CD4+CD25−Foxp3+ Treg cell ratios were negatively correlated with serum cytokeratin 19 fragment (CYFRA 21-1) concentrations in patients with NSCLC. Moreover, coculturing CD4+CD25−Foxp3+ Treg cells and CD14+ monocytes in vitro resulted in a higher frequency of CD206+CD14+ M2-like monocytes compared with CD14+ monocytes.
Conclusions:
Elevated circulating CD4+CD25−Foxp3+ Treg cells may be involved in the pathogenesis of NSCLC.
Introduction
Lung cancer is one of the most common malignant tumors threatening human health in China and worldwide. 1 nonsmall cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancers, with a low 5-year survival rate (only 15.9%). 2 In recent years, along with advances made in tumor immunology and molecular biological research, immunotherapy has increasingly become a novel and prominent treatment for NSCLC. 3,4 Animal studies provide evidence that regulatory T (Treg) cells play an important role in cancer immune evasion. 5,6 Kwiecien et al. reported that detection of Treg cells in the bronchoalveolar lavage fluid (BALF) was useful for evaluating the immune response in lung cancer. 7 However, little is known concerning the biological features and function of circulating Treg cells in NSCLC.
Treg cells are typically defined as a group of CD4+CD25+ T cells that function indispensably in the maintenance of self-tolerance and immune homeostasis by inhibiting a variety of physiological and pathological immune responses. 8 Forkhead box P3 (Foxp3) transcription factor is essential for the development and inhibitory function of Treg cells. 9 –12 It has been shown that inducible Treg cells, developed from naive CD4+CD25− T cells, 13 consist of a major subset of CD4+CD25−FoxP3+ cells (with the stimulation of highly antigenic epitopes) and a relatively small subset of CD4+CD25+FoxP3+ cells (with the stimulation of weak antigenic epitopes). 14 Numerous studies have reported the presence of CD4+CD25+Foxp3+ Treg cells in NSCLC. 15,16 However, levels of CD4+CD25−Foxp3+ Treg cells in NSCLC patients are largely unknown. Activated CD4+ T helper (Th) precursor cells can differentiate into Th1, Th2, Th17, and Treg cells after encountering a specific antigen. 17,18 Bettelli et al. reported that there is a reciprocal relationship between Treg cells and Th17 cells. 19,20 Although further studies strengthened the idea of a reciprocal relationship between Treg and Th17 cells, 21,22 few studies have examined the levels and/or associations of Treg and Th17 cells in NSCLC patients.
In this study, the authors investigated the frequencies of CD4+CD25+Foxp3+ and CD4+CD25−Foxp3+ Treg cells and Th1, Th2, and Th17 cells in peripheral blood, as well as cytokine concentrations in serum obtained from NSCLC patients. The relationships of Treg cells with clinical parameters and the potential function of CD4+CD25−Foxp3+ Treg cells were also explored.
Materials and Methods
Patient selection and clinical characteristics
A total of 36 patients with confirmed primary NSCLC before any treatment were enrolled at the Inpatient Department of The First Hospital of Jilin University between June 2016 and February 2017. The diagnosis of NSCLC was confirmed by diagnostic bronchofiberoscopy. Patients were staged according to the TNM staging system of the 2012 National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines. In addition, 20 age-, gender-, and ethnicity-matched healthy controls (HCs) were recruited. All patients provided signed written informed consent. The exclusion criteria were (1) clinical suspicion of infection; (2) history of hypertension, cardiopathy, immune disorders, other cancers, chemotherapy, or radiation therapy; and (3) presence of other pulmonary diseases, or severe dysfunction of the heart, liver, or kidney. This study was approved by the Ethics Committee of The First Hospital of Jilin University.
Flow cytometric analysis of peripheral blood mononuclear cells
Peripheral blood mononuclear cells (PBMCs) from blood samples were purified using density gradient centrifugation. Cells were then stained in duplicate with the following antibodies for 30 min: CD4-APC-CY7, CD25-APC, CD8-BV510 (BD Biosciences, Franklin Lakes, NJ), or isotype-matched control IgG (BD Biosciences). Next, cells were washed with phosphate-buffered saline (PBS), permeabilized using transcription factor Fix buffer (BD Biosciences), and subsequently stained with a Foxp3-PE-CF594 antibody (BD Biosciences). PBMCs (10 6 /tube) were also stained in duplicate with CD4-APC-CY7, permeabilized using transcription factor Perm buffer (BD Biosciences), subsequently stained with interleukin (IL)-10-PE, IL-17-APC, interferon (IFN)-γ-PE-CF594, or isotype-matched control IgG (BD Biosciences), and analyzed using the FACSCalibur flow cytometer (BD FACS Aria II). FlowJo software v7.6.2 was used to assess the expression level of each protein in each sample by analyzing ≥25,000 events per sample.
Flow cytometric analysis of CD4+CD25−Foxp3+ Treg cells in lung tissues
Lung tissues from 6 patients with NSCLC undergoing surgery were collected, and the excised tissues included tumor tissues and paracancer normal tissues. Blood and blood clots on the surface of the lung tissues were washed with sterile PBS. The tumor and normal tissues were separately crushed and centrifuged in a 15 mL tube containing 6 mL digestive fluid. Then, the tissues were digested at 37°C in a water bath with shaking for 45 min, followed by filtration and centrifugation at 1,000 rpm for 10 min. The supernatant was discarded and the red blood cells in the pellets were lysed with 3 mL 1 × lysing buffer (BD Biosciences) for 3 min. After washing with PBS (with 2% fetal calf serum) without calcium and magnesium ions, the resuspended cells were stained with CD4-APC-CY7, CD25-APC, CD8-BV510 (BD Biosciences), or isotype-matched control IgG (BD Biosciences). Then, cells were washed with PBS and permeabilized using transcription factor Fix buffer (BD Biosciences), subsequently stained with a Foxp3-PE-CF594 antibody (BD Biosciences), and finally analyzed using the FACSCalibur flow cytometer (BD FACS Aria II).
Cytometric bead array
The concentrations of serum IFN-γ, IL-10, and IL-17 cytokines were measured by cytometric bead arrays (CBA) 23 according to the manufacturer's instructions (BD Biosciences). Each serum sample (25 μL) was examined in duplicate using the FACSCalibur cytometer (BD Biosciences). 24 Serum cytokine concentrations were quantified and analyzed using the CellQuestPro and CBA software (Becton Dickinson).
Enzyme-linked immunosorbent assay
The CYFRA 21-1 concentration in serum samples of patients was determined using a CYFRA 21-1 enzyme-linked immunosorbent assay (ELISA) kit (DRG Instruments GmbH) according to the manufacturer's instructions, based on enzyme immunoassay technology, following a typical sandwich protocol. The detection limit was 0.15 ng/mL.
Human cell isolation and culture
The CD4+CD25−Foxp3+ Treg cells and CD14+ monocytes were isolated from PBMCs from six patients with primary NSCLC via staining with CD4-APC-CY7, CD25-APC, Foxp3-PE-CF594, and CD14-APC-CY7 (BD Biosciences) separately using flow cytometry. The cells were resuspended in D-10 (Dulbecco's modified Eagle's medium [DMEM] supplemented with 10% fetal calf serum, 100 U/mL penicillin, and 100 μg/mL streptomycin). The cells were cocultured in 24-well plates (Corning, Tewksbury, MA) at 0.5–2 × 10 5 cells per well, with CD4+CD25−Foxp3+ Treg cells and CD14+ monocytes at a ratio of 1:1; culture of the same amount of CD14+ monocytes was set as the control. After incubation at 37°C in a humidified atmosphere with 5% CO2 for 72 h, the cultured wells were harvested and stained with CD206-FITC (BD Biosciences) to determine the frequency of CD206+CD14+ M2-like monocytes.
Statistical analyses
Data are expressed as mean or median (range). Intergroup differences were analyzed using the Mann–Whitney U test. Correlations were assessed using Spearman's rank correlation test. All statistical analyses were performed using SPSS 19.0 software (SPSS, Inc., Chicago, IL). A two-sided p-value <0.05 was considered statistically significant.
Results
Patient characteristics
The characteristics of the patients in this study are shown in Table 1. There were no statistical differences among groups regarding age, gender, or lymphocyte count. There were 20 patients with limited-stage and 16 with advanced-stage NSCLC. With regard to histological types, 16 patients had adenocarcinoma and 20 had squamous cell carcinoma.
Characteristics of Participants in This Study
Data are shown as median (range), number (n), or percentage (%).
p < 0.05.
NSCLC, nonsmall cell lung cancer; HC, healthy controls; NA, not applicable.
Analysis of circulating Treg cells
The authors first analyzed the frequencies of circulating CD4+CD25+ and CD4+CD25− T cell subsets in patients and HCs. As shown in Figure 1B, NSCLC patients had significantly higher frequencies of circulating CD4+CD25+ T cells and CD4+CD25+Foxp3+ and CD4+CD25−Foxp3+ Treg cells compared with HCs (all p < 0.05). However, the frequency of CD4+CD25−T cells in NSCLC patients was significantly lower than that in HCs (p = 0.004). They also analyzed the frequencies of CD4+CD25−Foxp3+ Treg cells in tumor tissues, as shown in Supplementary Figure S1. The frequency of CD4+CD25−Foxp3+ Treg cells in tumor tissues was significantly higher compared with the frequency in normal tissues (p = 0.004). Thus, NSCLC patients exhibited high levels of CD4+CD25−Foxp3+ Treg cells in both peripheral blood and tumor tissues.
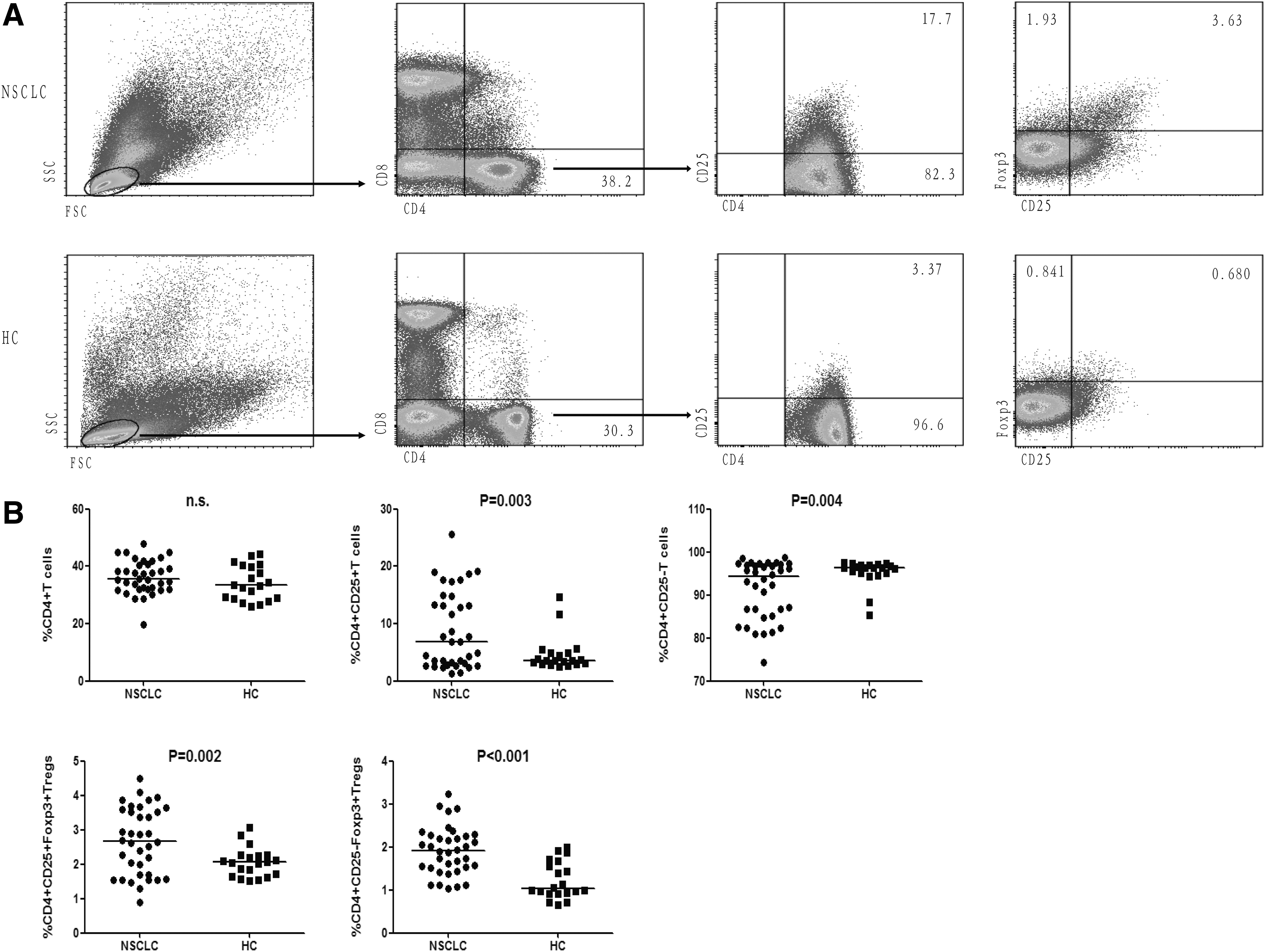
Flow cytometric analysis of Treg cells in peripheral blood. Treg cells were isolated from PBMCs of NSCLC patients and HCs, then stained with CD4-APC-CY7, CD25-APC, CD8-BV510, and Foxp3-PE-CF594 antibodies or isotype- matched control IgG for 30 min, and analyzed using flow cytometry.
Analysis of circulating Th1, Th2, and Th17 cells
The authors also analyzed the frequencies of CD4+IFN-γ+ Th1 cells, CD4+IL-10+ Th2 cells, and CD4+IL-17+ Th17 cells in PBMCs from patients with NSCLC using flow cytometry. As shown in Figure 2B, the frequency of Th2 cells was significantly higher in patients with NSCLC compared with HCs (p = 0.002). However, the frequencies of Th1 and Th17 cells were significantly lower in patients with NSCLC compared with HCs (all p < 0.05). In addition, the Th1/Th2 cell ratio was significantly lower in NSCLC patients compared with HCs (p = 0.002), while the Th17/CD4+CD25−Foxp3+ Treg cell ratio was significantly lower in NSCLC patients compared with HCs (p < 0.001).

Flow cytometry analysis of Th cells in peripheral blood. PBMCs collected from patients were stained with CD4-APC-CY7, CD3-BV510, IL10-PE, IFN-γ-PE-CF594, and IL-17-APC antibodies or isotype-matched control IgG for 30 min and analyzed using flow cytometry.
Correlation analysis of Treg cells with clinical parameters in patients
As observed above, the frequencies of CD4+CD25+ T cells and CD4+CD25+Foxp3+ and CD4+CD25− Foxp3+ Treg cells were significantly elevated in peripheral blood obtained from NSCLC patients. Hence, the authors further analyzed the potential association of various clinical parameters, as well as tumor staging, to understand the role of CD4+CD25−Foxp3+ Treg cells in the pathogenesis of NSCLC. They classified NSCLC patients into two groups based on the latest TNM staging system of the American Joint Committee on Cancer (AJCC): (1) limited stage (including stage 0, I, II, and IIIA); and (b) advanced stage (including stage IIIB and IV). As shown in Figure 3, patients with NSCLC advanced stage had significantly higher frequencies of circulating CD4+CD25+ T cells, CD4+CD25+Foxp3+ Treg cells, CD4+CD25−Foxp3+ Treg cells, CD4+IL-10+ Th2 cells, and CD4+IL-17+ Th17 cells compared with patients with limited stage (all p < 0.05). However, the frequency of circulating CD4+IFN-γ+ Th1 cells was significantly lower in NSCLC patients compared with HCs (p = 0.041). CYFRA 21-1, as a preferred marker for NSCLC, has great significance in the early diagnosis, monitoring treatment efficacy, and prognosis assessment of lung cancer. 25,26 Of interest, the authors analyzed the relationship between the Th17/Treg cell balance and the Th1/Th2 cell balance with serum CYFRA 21-1 concentrations. As shown in Figure 3, the Th17/CD4+CD25−Foxp3+ Treg cell ratios and serum IL-17 levels were negatively correlated with serum CYFRA 21-1 concentrations in patients with NSCLC (all p < 0.05), while the serum IL-10 levels were positively correlated with serum CYFRA 21-1 concentrations in NSCLC patients (p = 0.0032). In addition, the ratio of Th1/Th2 cells was significantly higher in patients with limited-stage NSCLC (p = 0.049).
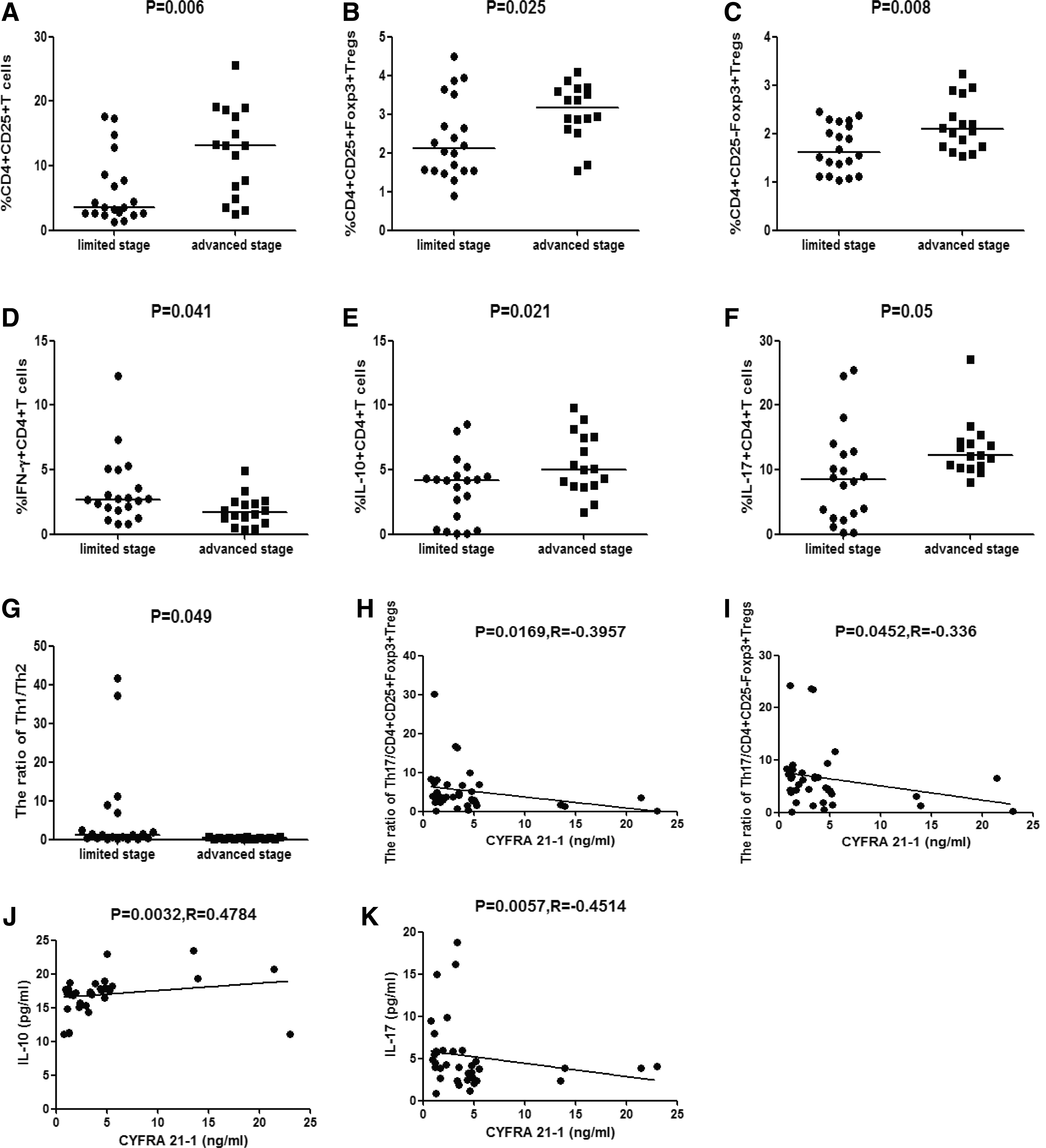
Correlation analysis between clinical parameters of patients and Treg and Th cells.
Analysis of serum cytokine concentrations
The levels of systemic cytokine responses were examined using the CBA method. As shown in Figure 4, IL-10 levels were significantly elevated in the NSCLC patients compared with HCs (p = 0.001). In contrast, IFN-γ and IL-17 levels were significantly lower in NSCLC patients compared with HCs (all p < 0.05).
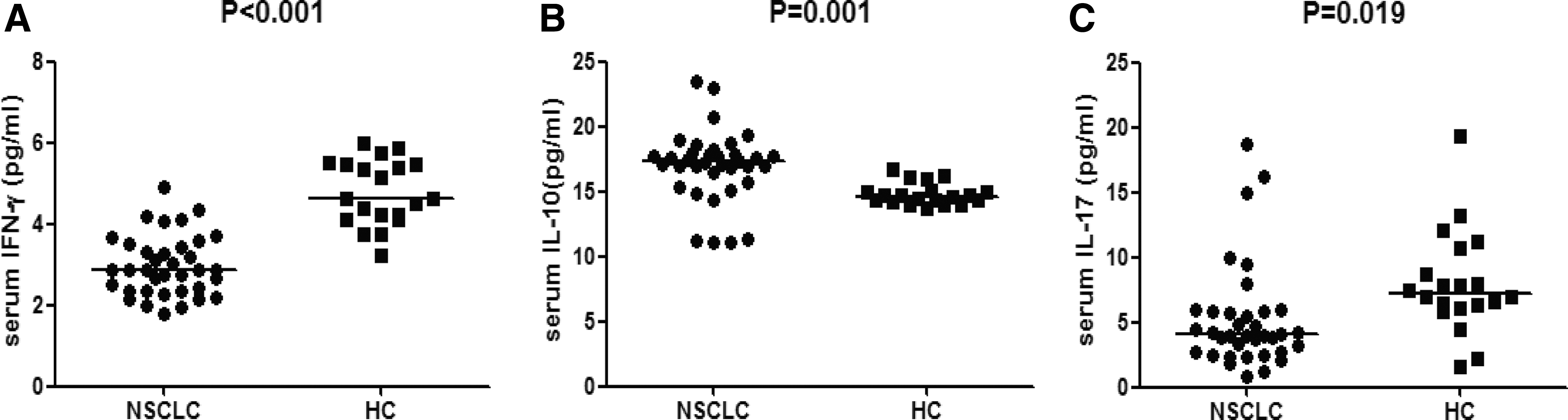
Analysis of serum cytokine concentrations. Serum concentrations of IFN-γ
Correlation analysis of the Treg cell subset with Th1, Th2, Th17 cells and cytokines
Next, the authors analyzed the relationship between the frequencies of cell subsets and cytokine levels. As shown in Figure 5, the frequencies of CD4+CD25+Foxp3+ and CD4+CD25−Foxp3+ Treg cells were positively correlated with IL-10 levels (all p < 0.05). However, the frequencies of CD4+CD25+Foxp3+ and CD4+CD25−Foxp3+ Treg cells were negatively correlated with IL-17 levels (all p < 0.05). In addition, the frequency of Th17 was positively correlated with IL-17 (p = 0.0031), and the frequency of CD4+CD25+Foxp3+ Treg cells was positively correlated with the frequency of CD4+CD25−Foxp3+ Treg cells (p = 0.0005).
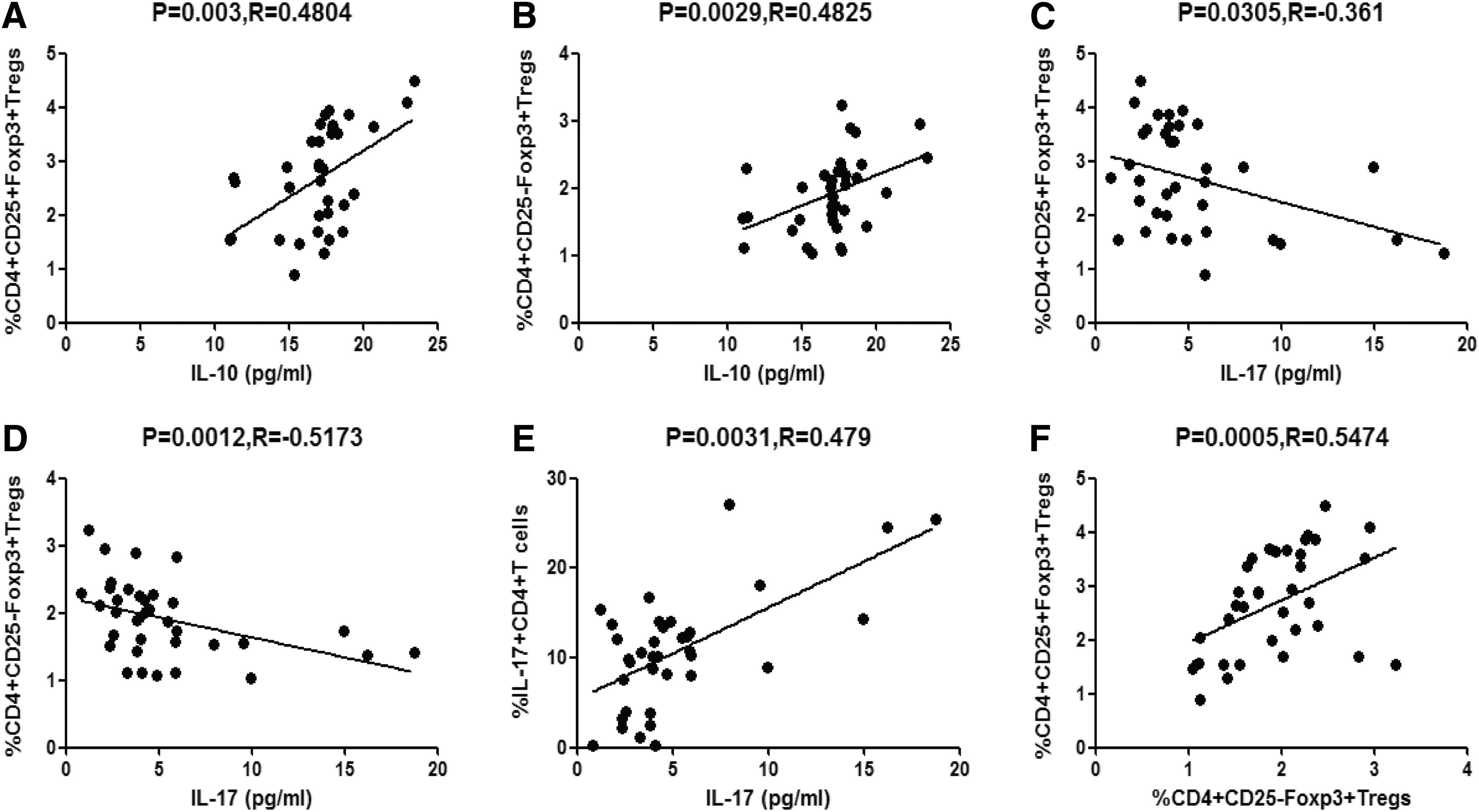
Correlation analysis among Treg cells, Th cells, and cytokines. The frequencies of CD4+CD25+Foxp3+ Treg cells
Effect of CD4+CD25−Foxp3+ Treg cells on monocytes
To explore the potential effect of CD4+CD25−Foxp3+ Treg cells on monocytes, isolated CD4+CD25−Foxp3+ Treg cells and CD14+ monocytes were cocultured in vitro. The results showed that the frequency of CD206+CD14+ M2-like monocytes in the coculture group was significantly higher compared with the CD14+ monocyte culture group (Supplementary Fig. S1B, p = 0.014). These data revealed that CD4+CD25−Foxp3+ Treg cells can skew the differentiation of CD14+ monocytes into CD206+CD14+ M2-like monocytes.
Discussion
Previous studies have revealed that the frequency of CD4+CD25+Foxp3+ Treg cells increased significantly in peripheral blood of NSCLC patients 15 and contributed to the immunopathology of NSCLC. 16 The present study demonstrated that elevated circulating CD4+CD25+Foxp3+ Treg cells, which were related to the severity of NSCLC, negatively correlated with IL-17, but positively correlated with IL-10 levels. Together with the findings of previous studies, 16,27 these data reveal that there is an imbalance of Th17 and CD4+CD25+Foxp3+ Treg cells in peripheral blood of patients with NSCLC.
Treg cells consist of two subsets: CD4+CD25+Foxp3+ and CD4+CD25−Foxp3+ cells. A study has shown that CD4+CD25−Foxp3+ T cells in untreated new-onset lupus patients are phenotypically and functionally different from CD4+CD25+Foxp3+ Treg cells. 28 However, levels of CD4+CD25−Foxp3+ Treg cells and their role in NSCLC patients remain largely unknown. The present data demonstrated that the frequency of CD4+CD25−Foxp3+ Treg cells is elevated in both tumor tissues and peripheral blood, and that the circulating CD4+CD25−Foxp3+ Treg cells were significantly higher in patients with advanced-stage NSCLC compared with those with limited-stage NSCLC, suggesting the importance of CD4+CD25−Foxp3+ Treg cells in the pathogenesis of NSCLC. Functionally, suppressing circulating Treg cells depends on the inhibitory cytokine IL-10. These data revealed that elevated circulating CD4+CD25−Foxp3+ Treg cells in patients with NSCLC were positively correlated with serum IL-10 levels, implying that these CD4+CD25−Foxp3+ Treg cells are a source for serum IL-10. Combined with the result that serum IL-10 levels positively and significantly correlated with clinical parameters of serum CYFRA 21-1 levels in NSCLC patients, the increased CD4+CD25−Foxp3+ Treg cells within the peripheral circulation, and specifically upregulation of IL-10 levels, suggest control over the development of NSCLC. Coculturing CD4+CD25−Foxp3+ Treg cells and CD14+ monocytes in vitro resulted in a higher frequency of CD206+CD14+ M2-like monocytes compared with CD14+ monocytes in culture, suggesting that CD4+CD25−Foxp3+ Treg cells can skew the differentiation of CD14+ monocytes into CD206+CD14+ M2-like monocytes. 29 A previous study revealed that CD4+CD25− T cells could differentiate into CD4+CD25+Foxp3+ T cells on homeostatic proliferation in vivo. 30,31 In this study, the frequency of CD4+CD25+Foxp3+ Treg cells was positively correlated with the frequency of CD4+CD25−Foxp3+ Treg cells in the peripheral blood of NSCLC patients. These data support the possibility that CD4+CD25−Foxp3+ Treg cells differentiate into CD4+CD25+Foxp3+ Treg cells.
Previous studies showed that IL-17 is involved in lung cancer, 27,32 and additional functional studies revealed that IL-17 mediates immune responses via inducting tumor-promoting microenvironments at tumor sites. Enhanced tumor development and IL-17-mediated regulation of myeloid-derived suppressor cells are a primary mechanism for the tumor-promoting effects. 33 However, other studies have shown that IL-17 may have antitumor activity and inhibit tumor growth. 34,35 Th17 cells, as the main source of IL-17, have a reciprocal relationship with Treg cells and their physiological functions in cancer immunity remain largely unknown. These data showed that Th17 cells were significantly decreased in NSCLC patients compared with HCs, and were positively correlated with serum IL-17 levels, which negatively correlated with serum CYFRA 21-1 levels. In addition, the authors observed a negative significant correlation between circulating CD4+CD25−Foxp3+ Treg cells and serum IL-17 levels, which is consistent with a previous study. 7 Collectively, these data revealed the importance of circulating Th17 cells in regulating serum IL-17 levels and the development of NSCLC.
To explore the reciprocal relationship between circulating Th17 cells and Treg cells, they further analyzed the ratio of Th17 cells to Treg cells and found that the ratio of Th17/CD4+CD25−Foxp3+ Treg cells was significantly lower in NSCLC patients compared with HCs. This shift was negatively correlated with serum CYFRA 21-1 concentrations, suggesting the significance of Th17/CD4+CD25−Foxp3+ Treg cells in NSCLC pathogenesis. With these novel findings, they showed the imbalance and relationship between these two cell-type subsets.
IFN-γ-expressing Th1 cells play an important role in combating infections caused by viruses, bacteria, and parasites. 36 IL-10-expressing Th2 cells participate in humoral immunity to mediate differentiation and antibody production of B cells. 37 For decades, Th1 immunity has been considered a key mechanism in the host defense against tumors, while a Th2-dominant environment has been considered to promote tumor growth. 38 Ma et al. observed a shift of Th1/Th2 cells in patients with NSCLC after treatment with ginseng polysaccharides and dendritic cells. 39 In this study, the authors showed that the frequency of Th2 cells was higher, while the Th1/Th2 ratio was significantly lower, in NSCLC patients compared with HCs, suggesting a Th2-dominant environment in NSCLC. Although the Th1/Th2 ratio was significantly higher in limited-stage compared with advanced-stage NSCLC, they did not observe any relationship between the Th1/Th2 ratio and serum IFN-γ and IL-10 levels. Similarly, Adurthi et al. revealed that the microenvironment of cervical carcinomas harboring both Th1 and Th2 cells was functionally active, but that the effects of Treg cells interfered with the functionality. 40 Therefore, further studies are needed to understand the mechanisms leading to the imbalance of Th1/Th2 cells and their functional role in NSCLC.
In summary, these data revealed that elevated circulating CD4+CD25−Foxp3+ Treg cells and an imbalance of Th17/CD4+CD25−Foxp3+ Treg cells contribute to the occurrence and development of NSCLC. Measuring levels of these T cell subsets will provide valuable information to assess the severity of NSCLC. These findings may also provide a useful clinical reference for NSCLC immunotherapy that could be accomplished by targeting these alterations. However, there are several limitations in this study: the authors included a relatively small sample size and the roles of circulating CD4+CD25−Foxp3+ Treg cells in the pathogenesis of NSCLC need to be further investigated.
Footnotes
Acknowledgments
This study was supported by grants received from the National Natural Science Foundation of China (No. 30972610, 81273240, 91742107, 81570002, and 81700027), the National Key Research and Development Program (No. 2017YFC0910000 and 2017YFD0501300), the Jilin Province Science and Technology Agency (No. 20160101037JC, 20170622009JC, 2017C021, 2017J039, SXGJXX2017-8, JJKH20180197KJ, DBXM154-2018, and 2018SCZWSZX-015), the Norman Bethune Program of Jilin University (2012206), and the State Key Laboratory of Kidney Diseases in PLA General Hospital.
Disclosure Statement
The authors declare no potential conflicts of interest.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.