
Abstract
Background:
Novel hormonal therapies (NHTs) have enriched the therapeutic armamentarium available for patients with castration-resistant prostate cancer. However, there is a need for clinical indicators able to drive treatment decisions and timing. The aim of this report is to perform a pooled analysis based on all available literature focused on prediction of efficacy and survival in patients treated with NHTs before and postchemotherapy.
Methods:
After reviewing the studies included in this work, the efficacy and the survival of NHTs according to age and Gleason score (GS) was focused.
Results:
A total of eight studies were included in the analysis. With regard to age, the survival hazard ratio shows a better outcome, for both elderly and young patients, in postchemotherapy studies. With regard to progression-free survival, the subgroup analysis of pre- and postchemotherapy studies demonstrates the effect of NHTs on the reduction of risk of progression is greater in prechemotherapy studies irrespective of age. With regard to GS, NHTs show higher efficacy when administered postchemotherapy in patients with GS <8, whereas in patients with GS ≥8 NHTs are more effective in the prechemotherapy setting.
Conclusion:
Given the limitations of a meta-analysis of data from the literature, the results show that progression-free survival is always higher when NHTs are administered prechemotherapy in comparison with postchemotherapy. This benefit, however, translates in a reduction of risk of death only in patients with GS ≥8. In the other patients, the risk of death decreases when NHTs are administered postchemotherapy.
Background
Recently, novel hormonal therapies (NHTs) have enriched the therapeutic armamentarium of the castration-resistant prostate cancer (CRPC). 1 Abiraterone acetate and enzalutamide have been shown to increase the survival in CRPC irrespective of the timing of administration. 2 –5 Moreover, other agents with different mechanisms of action, including chemotherapy or bone targeted agents, have been approved in CRPC resulting in a total of five novel treatments available for CRPC. 6 Unfortunately, the optimal therapeutic sequence for these agents remains unknown 7,8 and new biomarkers are needed to aid the right therapy selection and/or timing of administration. For instance, the presence of an androgen-receptor splice variant, mainly version 7 (AR-V7), coincides with loss of efficacy of two consequently NHTs.
In the absence of randomized trials of standard chemotherapy versus NHTs, a pooled analysis was performed based on all the published literature data focused on the therapeutic efficacy and on the survival in patients treated with NHTs before and postchemotherapy. In particular, the impact of the NHTs on their therapeutic efficacy and on the survival in CRPC according to the patients' age and the Gleason score (GS) have been analyzed.
Methods
The methodology adopted is detailed in Roviello et al. 1 and reported in the Supplementary Data. Supplementary Figure S1 presents the systematic literature review results along with the selection of randomized controlled studies. The studies for the analysis were identified according to the following inclusion criteria: (1) participants with metastatic CRPC, (2) an NHT as the experimental drug, (3) the presence of a control arm for comparison, and (4) possibility to assess hazard ratio (HR) for survival and progression according to pre- or postchemotherapy. The following exclusion criteria were used: (1) insufficient availability of data estimating the outcomes, (2) animal studies, (3) the size of each arm based on <10 participants, and (4) the presence of a single-arm study.
The search yielded 1505 potentially relevant articles. A total of 339 studies were excluded as duplicates. After reviewing the titles and abstracts of the 1166 remaining studies, the full texts of 49 studies were retrieved, and 8 studies (Supplementary Fig. S1) were included in the analysis (Supplementary Table S1). Six of these are phase III studies and two phase II studies (Supplementary Table S1). The median Jadad score was 5.
Results
Age
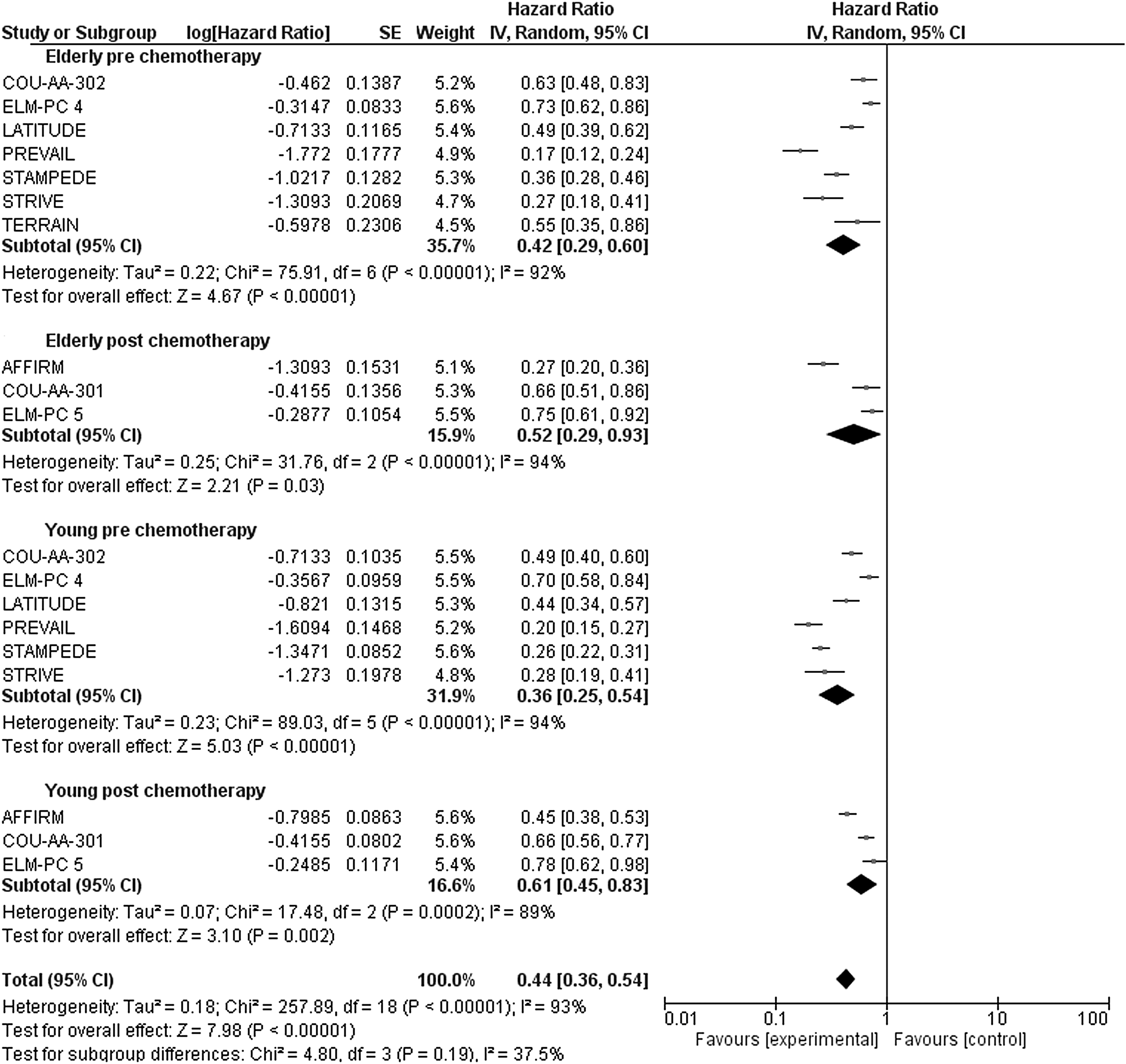
With regard to age, six studies 2 –5,9,10 were included in the meta-analysis according to the inclusion and exclusion criteria. For the COU-AA-301, the COU-AA-302, the AFFIRM, and the PREVAIL trials, a subsequent subgroup analysis was performed to evaluate the survival endpoint in patients treated pre- and postchemotherapy. 11 –14 A total of 7857 cases were included; 3077 cases were elderly, whereas 4780 cases were young (see Supplementary Table S2 for definitions). The subgroup analysis of pre- and postchemotherapy studies, summarized in Figure 1, demonstrates the effect of NHTs on the reduction of risk of death is greater in postchemotherapy studies. The survival HR shows a better outcome, for both elderly and young patients, in postchemotherapy studies (Table 1).

Subgroup analysis of overall survival in pre- and postchemotherapy studies according to age.
Data on Favored Hazard Ratio According to Age and Gleason Score in Pre- and Postchemotherapy Studies
With regard to progression-free survival (PFS), the subgroup analysis of pre- and postchemotherapy studies demonstrates the effect of NHTs on the reduction of risk of progression is greater in prechemotherapy studies irrespective of age, as reported in Figure 2. HR of PFS showed a better outcome for both elderly and young patients in the prechemotherapy studies (Table 1).
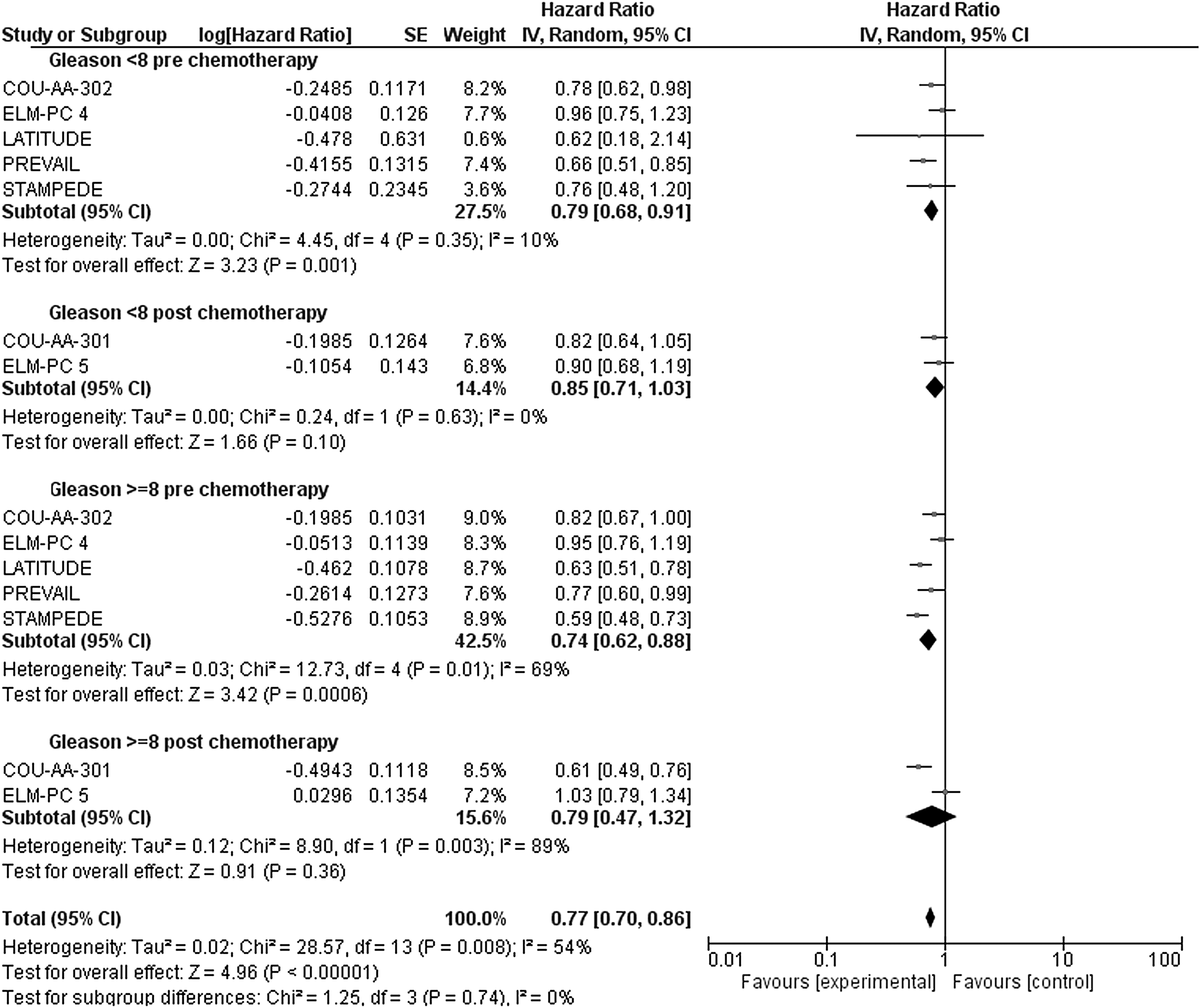
Subgroup analysis of overall survival in pre- and postchemotherapy studies according to GS. GS, Gleason score.
Gleason score
The role of GSs in the context of NHTs has been previously reported. 15 A total of 6187 cases were included in this study; 2982 cases (1654 in the experimental and 1328 in the control arm) had GS <8, whereas 3205 cases (1797 in the experimental and 1408 in the control arm) had GS ≥8 (Supplementary Table S3). Subgroup analysis of pre- and postchemotherapy studies is summarized in Figure 3. After stratification according to GS, NHTs show higher efficacy when administered postchemotherapy in patients with GS <8, whereas in patients with GS ≥8 NHTs are more effective in the prechemotherapy setting (Table 1).
Subgroup analysis of progression-free survival in pre- and postchemotherapy studies according to age.
With regard to PFS, a total of 6791 cases were included; 3261 cases (1788 in the experimental and 1473 in the control arm) had GS <8, whereas 3530 cases (1958 in the experimental and 1572 in the control arm) had GS ≥8 (Supplementary Table S3). Subgroup analysis of pre- and postchemotherapy studies, reported in Figure 4, demonstrates a higher reduction of the risk of progression when NHTs are administered before chemotherapy, irrespective to the GS. The PFS HR shows a better outcome in the prechemotherapy setting for both GS <8 and GS ≥8 patients (Table 1).
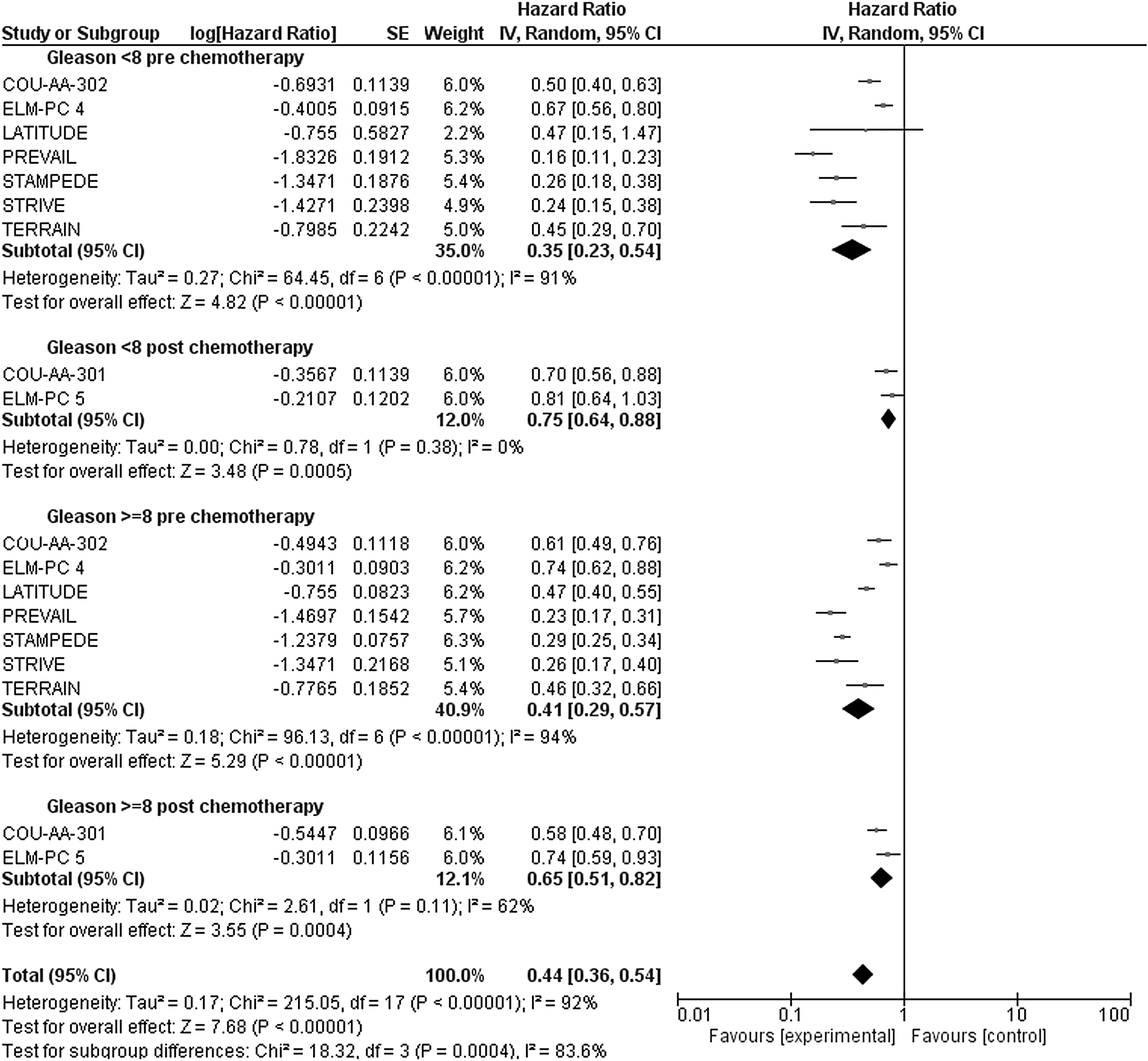
Subgroup analysis of progression-free survival in pre- and postchemotherapy studies according to GS.
Conclusion
It is well known that NHTs are effective regardless of the age or the GS and the analysis showed that PFS is always increased when these novel agents are used before chemotherapy compared with their administration as postchemotherapy.
Moreover, regardless of the age of the patients with CRPC, this benefit seems to reduce the risk of death in patients with GS ≥8 if administered before chemotherapy. In patients with GS <8, the reduction in the risk of death seems to be confined when NHTs are administered after chemotherapy only.
It is noteworthy that these data need to be considered with caution as the analysis performed presents limitations mainly related to the source of data as it is literature based rather than an analysis of the raw data. This implies a high heterogeneity mainly due to the several studies with different patients' characteristics, or due to the different experimental agents with regard to the considered different control arms; therefore, definitive conclusions need to be considered carefully.
However, in the absence of a direct comparison between chemotherapy and NHTs in randomized trials with regard to the timing of administration, a greater advantage of the use of NHTs in CRPC seems to be obtained in patients treated before the standard chemotherapy and with a GS ≥8. In the meanwhile, randomized studies in this setting are awaited to confirm this clinically important address; in oncological routine, the GS could help in the proper therapeutic decision-making/clinical algorithm for any single patient with CRPC with regard to the new armamentarium of therapies.
Footnotes
Authors' Contributions
G.R. performed the protocol/project development, data collection/management, and data analysis; all authors wrote and edited the article.
Disclosure Statement
There are no existing financial conflicts.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.