
Abstract
Background:
The aim of this study was to evaluate the safety and efficacy of repeated administration of 90Y-microspheres in intrahepatic cholangiocarcinoma (ICC) relapsed after the first radioembolization (RE).
Methods:
Nine patients with ICC relapsed after the first 90Y-RE were enrolled. Six patients presented recurrence in the right hepatic lobe, 3 in the left lobe. All subjects underwent a second administration of 90Y-resin microspheres. Toxicity was assessed according to Common Terminology Criteria for Adverse Events (CTCAE, version 4.02). After the repeated treatment, all patients were submitted to follow-up with laboratory, imaging, and clinical examinations.
Results:
The mean cumulative activity administered considering both treatments was 2.7 ± 0.5 GBq. After the second treatment, 3 patients presented complete metabolic response (33.3%) and 6 had partial response (66.6%). The following adverse events were registered: transient increased levels of liver enzymes (grade 1 = 4; grade 2 = 2), hyperbilirubinemia (grade 1 = 2), ascites (grade 2 = 1), and duodenal ulcer (grade 2 = 1). Two patients developed a significant shrinking of the targeted hepatic lobe, as for radiation lobectomy. No case of RE-induced liver disease was registered. Median overall survival was 16.5 ± 1.4 months after the first RE.
Conclusions:
The authors' results suggest that repeated administration of 90Y-microspheres may be considered in patients affected by ICC relapsed after the first 90Y-RE.
Introduction
Intrahepatic cholangiocarcinoma (ICC) is a rare and severe malignancy. 1 Surgery, the only curative approach, is often not practicable due to the extension of the tumor mass at diagnosis. Systemic chemotherapy with gemcitabine plus cisplatin is used as a first-line approach in patients with unresectable disease. 2 Locoregional treatments (such as transarterial chemoembolization [TACE], radiofrequency ablation, etc.) are other therapeutic options for ICC. 3,4 In particular, TACE has been applied for treating ICC with a satisfying rate of disease control. 5
Radioembolization (RE) is an emerging therapy for ICC 6,7 ; it is based on the selective transarterial delivery of 90Y-microspheres to the tumors. It has been reported that RE may significantly improve the outcome of ICC patients, indicating that this therapeutic approach might be particularly effective in those subjects, in which the administration of 90Y-micropsheres is not preceded by other treatments. 8
However, ICC is an aggressive malignancy and relapse can occur after locoregional treatments. In particular, in a cohort of 62 patients with ICC submitted to repeated TACE, it has been reported that 20 subjects (i.e., 32.2%) relapsed after the first cycle with median time to progression of 8 months and were therefore submitted to a second cycle of TACE. 9 Whether or not it is safe to repeat locoregional therapy with 90Y-RE in patients affected by ICC and relapsed after the first administration of 90Y-microspheres is a still debated and few explored issue. In this regard, Zarva et al. reported tolerable toxicity for repeated cycles of 90Y-RE in a cohort of 21 patients affected by primary or secondary hepatic tumors. 10 It has to be pointed out that, among the subjects included in the cited article, only 1 was affected by cholangiocellular carcinoma.
The aim of this study was to evaluate the safety and efficacy of repeated 90Y-RE in ICC patients with disease progression after the first RE.
Materials and Methods
Patients
The authors retrospectively evaluated the clinical data of 9 patients affected by unresectable and chemotherapy-refractory ICC and relapsed after a first treatment with 90Y-resin microspheres. The enrolment criteria were as follows: histologic proof of ICC; liver-only or liver-predominant disease; age ≥18 years; ability and willingness to provide written informed consent; life expectancy >3 months; Eastern Cooperative Oncology Group (ECOG) performance status ≤2; bilirubin <2.0 mg/dL, albumin >2.0 g/dL, international normalized ratio <1.5; creatinine <2.0 mg/dL; platelets ≥100,000/μL, Hb ≥9.0 g/dL, and white blood cell ≥1500/μL. Patients with predominant extrahepatic disease, active central nervous system metastases, or diffuse peritoneal metastases were excluded.
Study design
All patients provided written informed consent before procedure and associated risk. Preprocedural evaluation included baseline imaging studies, clinical, and laboratory examinations.
Angiography with selective visceral catheterization was performed to evaluate the vascular and tumor anatomy and blood-flow dynamics, enabling a determination of the optimal placement of the catheter for selective treatment. 99mTc-macroaggregated albumin (99mTc-MAA) scan was performed to test gastrointestinal flow and to estimate the percent of injected activity shunted to the lungs. After 7- 10 d, the patients returned to the department for the treatment session performed by selective catheterization of the main hepatic artery by transfemoral approach, embolization of gastroduodenal, and gastric artery. After selective catheterization of the right/left hepatic artery, the patient, without sedation, was administered with by a slow, manually controlled injection lasting about 30 min, under intermittent fluoroscopic guidance, alternating the 90Y-microspheres suspended in 5% glucose solution with contrast medium for assessing persevered anterograde arterial flow. In all cases, resin spheres (SIR-Spheres; Sirtex Medical, Sydney, Australia) were administered.
The prescribed 90Y activity was calculated as the patient-specific activity according to the manufacturer's vial applying the body surface area (BSA) formula. 11 Before the repeated administration of 90Y-microspheres after progression, angiography and 99mTc-MAA scintigraphy were repeated to exclude extrahepatic accumulations caused by collaterals or shunts to the lung that have increased in the meantime. The prescribed activity was not reduced due to the repeated procedure, but only in case of significant (i.e., 10%–20%) hepatopulmonary shunt.
90Y positron emission tomography imaging
All subjects underwent positron emission tomography (PET) scan to evaluate the pattern of spheres distribution. 12
18 F-fluorodeoxyglucose PET imaging
All patients were submitted to PET-computed tomography (CT) scan 60 min after the intravenous administration of 3.7 MBq/kg of 18 F-fluorodeoxyglucose (FDG). FDG PET was performed at baseline for patients' restaging (i.e., 1 week before the procedure) and for the assessment of the response at 1 month and then every 3 months after 90Y-RE. The PET-CT device was a Discovery ST (GE, Milwaukee, WI) with bismuth germanate crystal units arranged to form 24 rings combined with a 16-slice Light Speed Plus CT scanner. The average full width at half maximum (FWHM) axial resolution of PET is 5.2 mm and system sensitivity 9.3 cps/KBq for three-dimensional (3D) acquisition mode. Scanning was performed from the neck to the proximal tight in 3D modality, with an acquisition time of 3 min per table position. Images were reconstructed by using an ordered subset expectation maximization iterative algorithm (OSEM-SV, VUEPoint HD, GE, 2 iterations, 15 subsets). The CT was performed immediately before PET in the identical axial field of view using a standardized protocol consisting of automatic tube current modulation with auto mA-tube rotation time of 0.5 s/rotation and slice thickness of 3,75 mm. The CT data were resized from 512 × 512 to a 256 × 256 matrix to match the PET data.
The data were transmitted to a nuclear medicine database, fused, and displayed using a dedicated software (Advantage, GE).
Assessment of response to treatment
Patients were restaged at 1 month after the procedure with FDG PET-CT and contrast enhanced CT, then repeated every 3 months. The follow-up PET-CT was compared to the pretreatment scan, and metabolic response was defined as a reduction of standardized uptake value according to the PET response criteria in solid tumors (PERCIST). 13 In 2 patients showing a significant volumetric reduction of the hepatic lobe targeted with repetitive 90Y-administrations, the change in the hepatic lobar volume (HLV) after the two RE procedures was calculated on the coregistered nonenhanced CT image.
Safety
Toxicity was evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE), version 4.02, on the basis of laboratory tests, CT or PET imaging, and clinical examinations. Before the procedure, all patients underwent physical examination; CT and FDG PET imaging; and laboratory tests, including total bilirubin, alanine transaminase, aspartate transaminase, alkaline phosphatase, γ-glutamyl transpeptidase. After treatment, all patients resumed a routine schedule of laboratory tests which were performed at 2 and 4 weeks after the procedure and repeated at 3-monthly interval. Clinical toxicities, including pain, fever, fatigue, and gastrointestinal adverse events, were assessed at the regular follow-up visits.
Survival
The overall survival (OS) was calculated by the Kaplan–Meier method (MedCalc 11.3.8.0; MedCalc Software, Mariakerke, Belgium), measured from the date of the first procedure to the death of the patients.
Results
Table 1 summarizes the clinical features and the survival after repeated therapy with 90Y-microspheres. The authors enrolled 9 patients (5 male, 4 female, mean age: 65.4 ± 8.0). Among the subjects included in the study, 6 had received a first 90Y-RE to the right hepatic lobe, 2 to the left hepatic lobe, and the remaining 1 subject had received a separate sequential lobar 90Y-administration with a 6-week interval between the two procedures. Two patients presented extrahepatic disease with localizations in the abdominal nodes; in such cases, hepatic tumor involvement was considered the most relevant prognostic factor for survival. The mean interval of time between the first RE and relapse was 7.3 ± 1.5 months.
Patients' Clinical Features and Their Survival After Repeated Therapy with 90Y-Microspheres
Patients showing significant hypotrophy of the repeated treated lobe with compensatory hypertrophy of the contralateral one.
Y-RE, 90Y-radioembolization; BIL, bilirubin levels; CIS + GEM, cisplatin plus gemcitabine; CR, complete response, PR, partial response; F, female; G1, grade 1; G2, grade 2; GI tox, gastrointestinal toxicity; LHL, left hepatic lobe; M, male; RFA, radiofrequency ablation; RHL, right hepatic lobe; ΔHLV, decrease in hepatic lobar volume.
Six patients received repeated treatment with 90Y-microspheres to the right hepatic lobe and 3 to the left. The mean cumulative activity administered considering both treatments was 2.7 ± 0.5 GBq. Median OS was 16.5 ± 1.4 months (95% CI 13.8–19.3) calculated from the first 90Y-RE (Fig. 1).
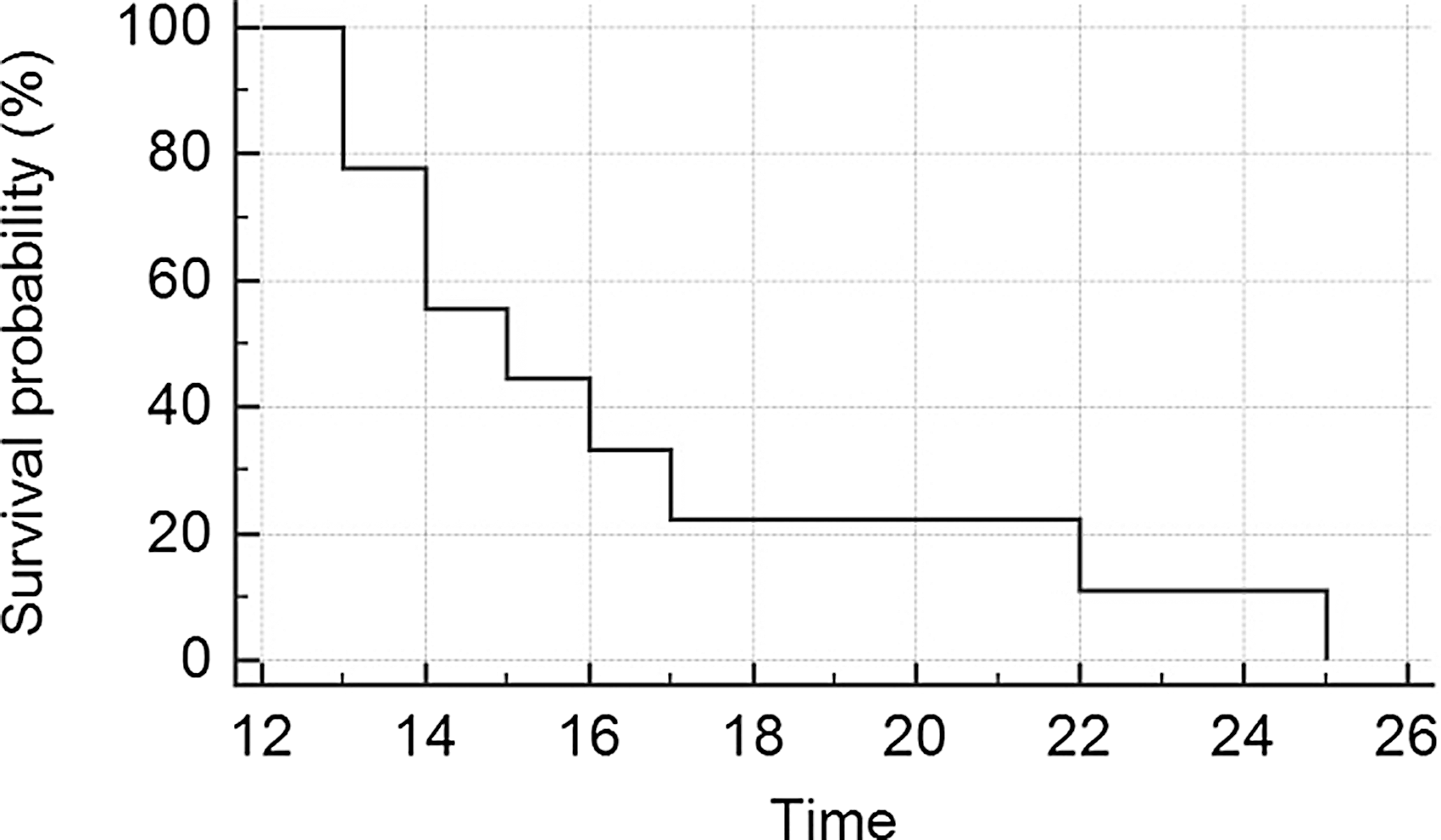
Overall survival of patients calculated form the first 90Y-RE as represented by Kaplan–Meier curve. RE, radioembolization.
90Y PET imaging
No extrahepatic sites of 90Y microspheres uptake were registered.
Assessment of response to treatment
According to PERCIST, after the second treatment, 3 patients presented complete metabolic response (33.3%) and the remaining 6 had partial response (66.6%). Two of the 3 subjects with complete response after the second treatment also presented a significant hypotrophy of the targeted lobe, with a decrease in the HLV value of, respectively, 67% and 71%, and compensatory hypertrophy of the contralateral one (Fig. 2).
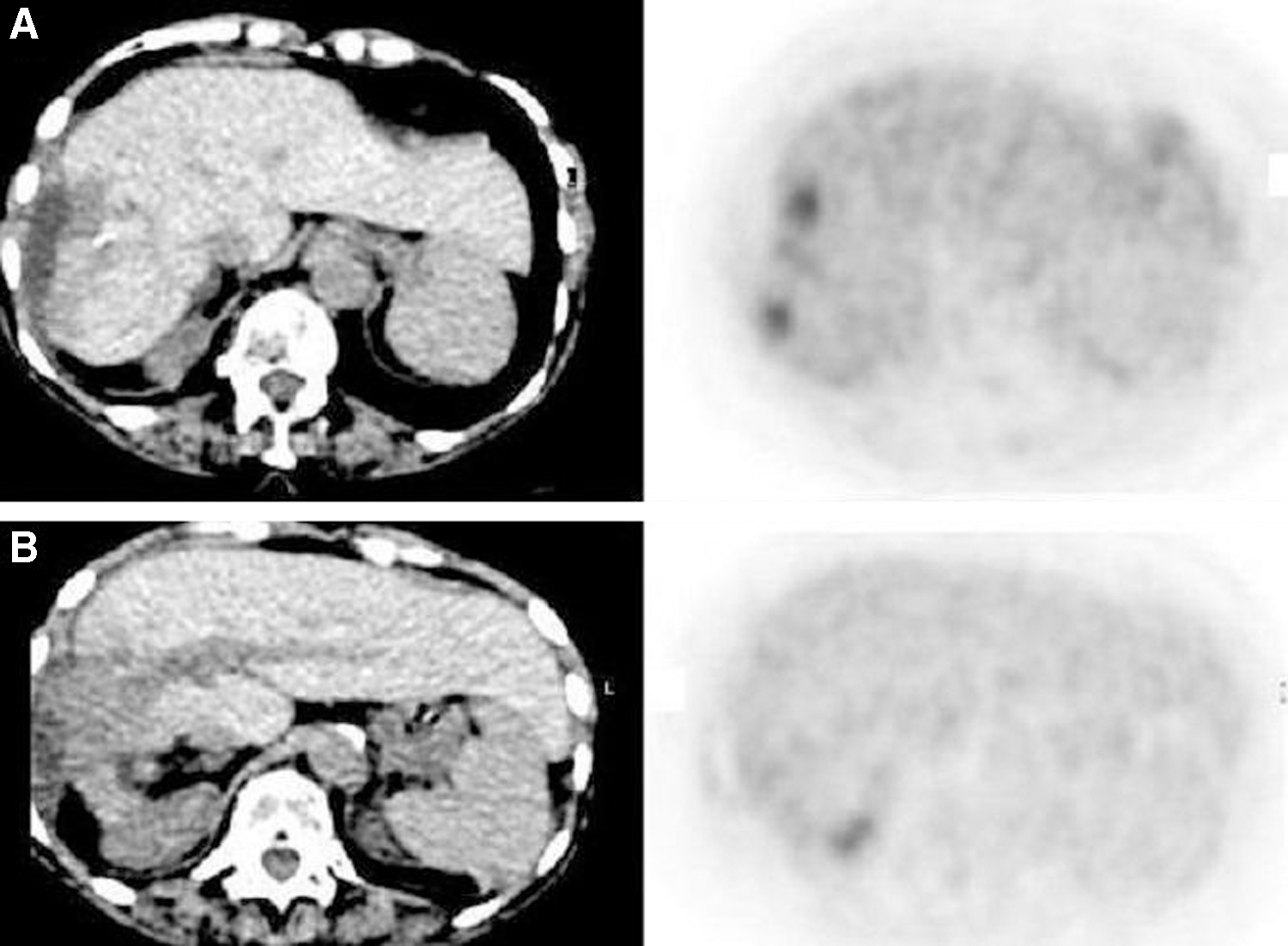
Eighty years old female patient affected by ICC and relapsed 9 months after the first 90Y-RE.
Toxicity
Figure 3 represents the adverse effects registered after the repeated administration of 90Y-microspheres. Immediate complications such as vomiting and nausea (grade 2) were registered in 3 patients in the 6 h following RE. Routine medications were administered for obtaining a complete remission of these symptoms. The lung-shunt fraction was calculated to be less than 10% in all patients both at first and second procedure and no pulmonary toxicity was registered during follow-up. The following adverse events were registered: transient increased levels of liver enzymes (grade 1 = 4; grade 2 = 2) and hyperbilirubinemia (grade 1 = 2). One subject showed moderate ascites (grade 2 = 1) as depicted in Figure 4. One patient developed duodenal ulcer (grade 2). Among patients receiving the repeated administration of 90Y-microspheres, none presented a significant worsening of the liver function as assessed according to the Child-Pugh class. No case of radioembolization-induced liver disease (REILD) was registered.
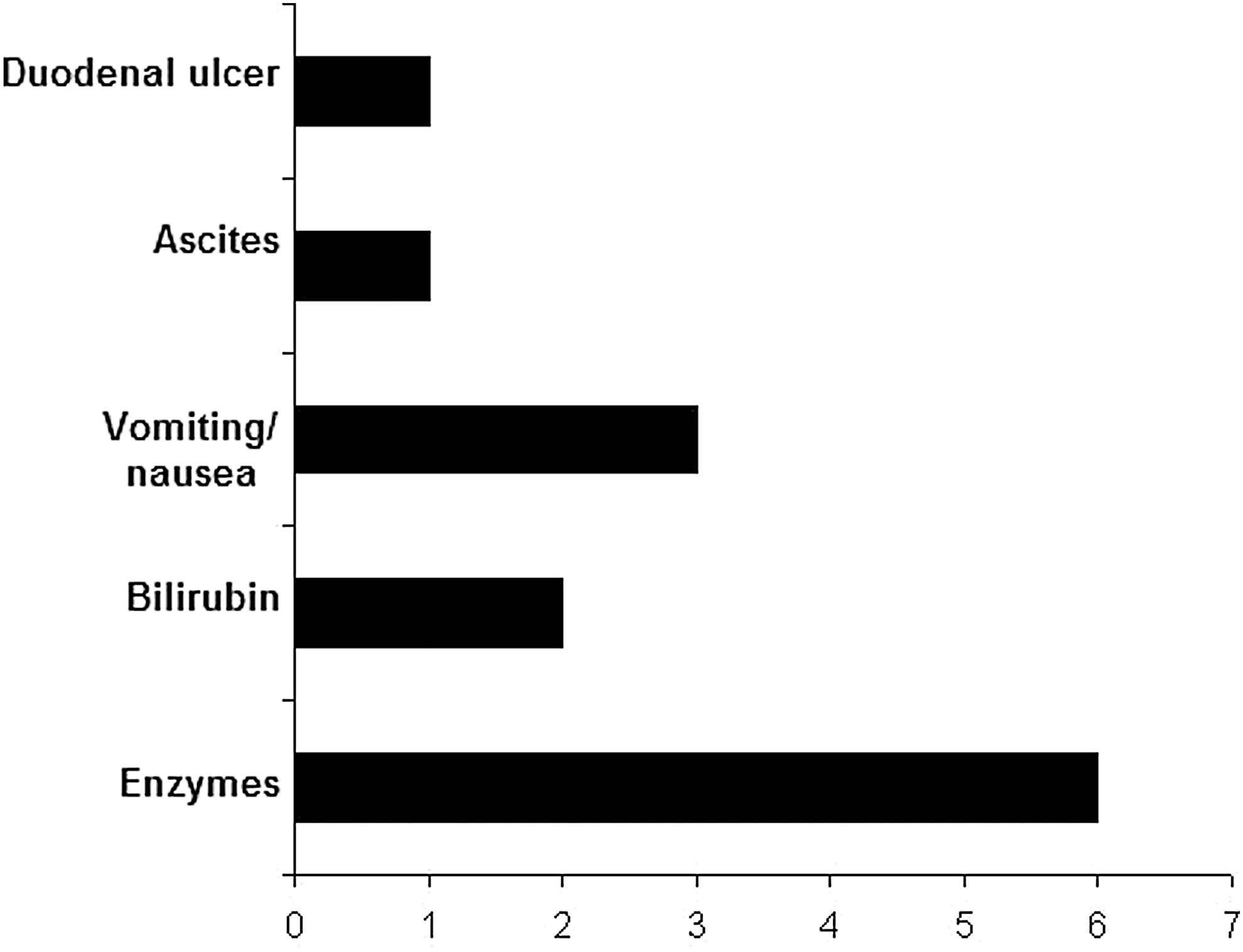
Histogram representation of the adverse reactions after repeated administration of 90Y-microspheres.
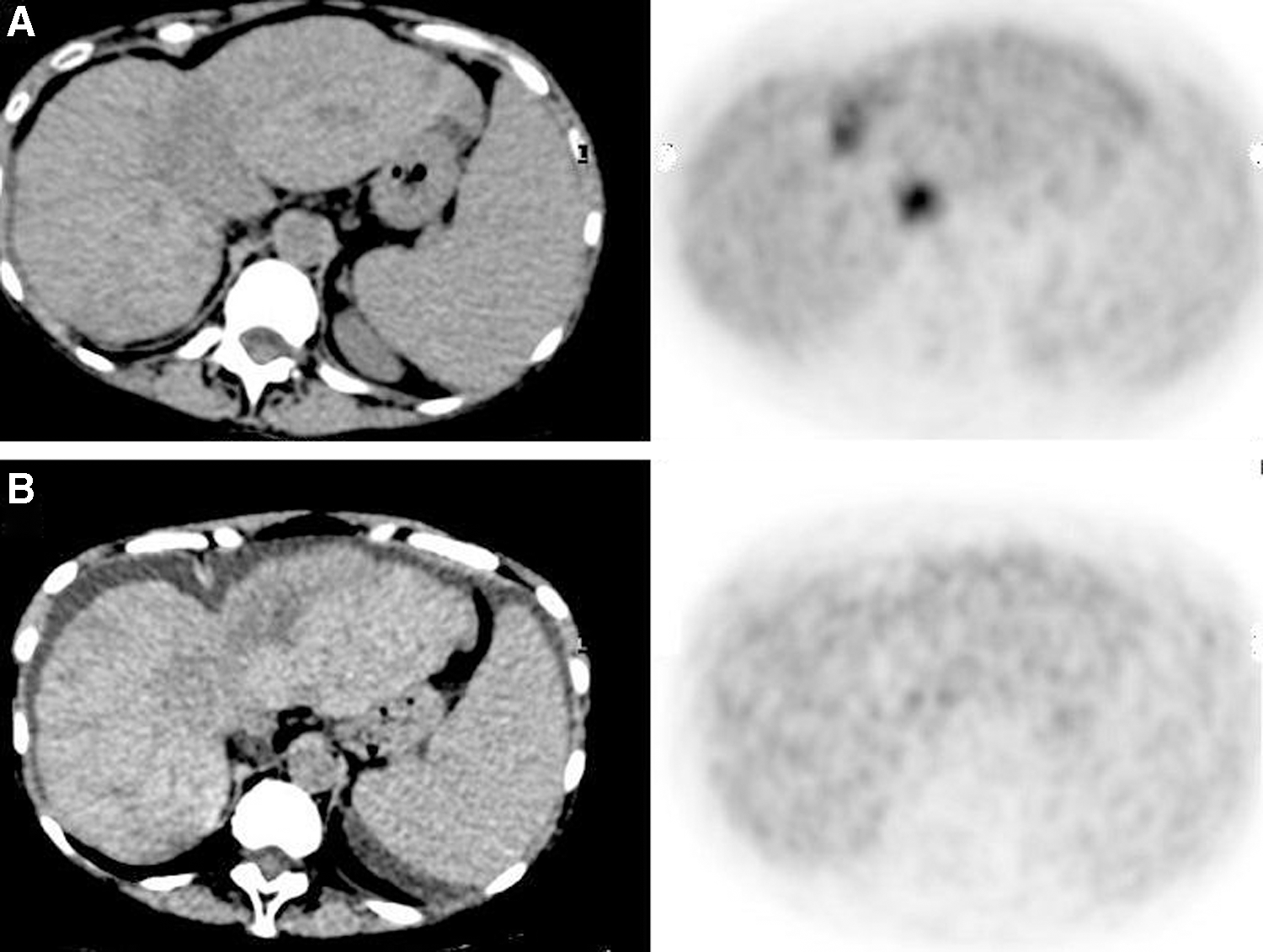
Fifty-five years old female patient affected by ICC relapsed 6 months after the first sequential lobar 90Y-RE.
Discussion
Despite many advances in diagnosis and therapy, the management of ICC still remains a challenge for physicians. Furthermore, the incidence of ICC is increasing worldwide and now represents the second most primary liver tumor in the United States. 14 When surgery is unfeasible, locoregional therapies should be considered for contrasting disease progression and reducing tumor-related symptoms. In such cases, both TACE and 90Y-RE have been demonstrated effective for treating patients affected by unresectable ICC. 15 However, while several published articles suggest that TACE can be safely used as a repetitive procedure, 16 the scientific data focusing on the repeatability of 90Y-RE are really limited. 10
Lam et al. evaluated 247 patients with hepatic tumors submitted to 90Y-RE between 2004 and 2011, 8 of whom underwent repeated treatments of a targeted part of the liver with resin microspheres. 17 Among subjects submitted to repeated 90Y-administrations, the authors registered 2 cases of death after the second treatment due to REILD. Repeated RE resulted to be the only independent risk factor for REILD in multivariate analysis. REILD is the most severe complication after 90Y-RE: it was described for the first time by Sangro et al. in 2008 as a distinct clinical picture appearing 4 to 8 weeks after treatment, characterized by veno-occlusive features at the histologic examination and a poor prognosis. 18 As concerns toxicity after 90Y-RE, Seidensticker et al. evaluated 34 patients with noncirrhotic liver and hepatic malignancies submitted to locoregional therapy with 90Y-microspheres as either whole liver or sequential lobar treatment. Three months after whole liver RE, the authors registered 14 liver-related grade 3/4 events. Of note, 3 patients treated with whole liver RE suffered from REILD. 19
The safety of repeated administration of 90Y-microspheres has been more recently assessed by Zarva et al. in a cohort of 21 patients with hepatic tumors. 10 It has to be pointed out that the majority of the enrolled subjects were affected by metastases from breast or colorectal cancer, 8 had hepatocellular carcinoma, and only 1 presented ICC. In contrast to the results reported by Lam et al., the authors did not register any case of REILD after the second session of 90Y-RE. Most frequent adverse events were ascites, elevation of bilirubin or liver enzymes, and decrease of serum albumin levels.
Mosconi et al. evaluated the safety and the efficacy of RE in 23 patients affected by ICC. 8 Among these subjects, 3 patients (13%) repeated the locoregional treatment with 90Y-microspheres without any relevant toxicity. In the authors' study, the most common late adverse effect was represented by transient and self-limiting increasing of hepatic enzyme value. It has to be pointed out that, both in their cohort and in that of the previously cited article, 8,10 there was no grade 4 or 5 toxicity. Of their patients, one developed a duodenal ulcer despite no extrahepatic deposition of the microspheres detected at the 90Y-PET-CT. Thus, they hypothesized that the ulcer might have been due to transient ischemic injury occurred in the periprocedural phase.
The potential repeatability of 90Y-RE is of particular interest in the case of ICC, as this neoplasia has a significant rate of recurrence with limited therapeutic options. To the authors' knowledge, their report is the first specifically focused on the safety and efficacy of repeated administrations of 90Y-microspheres in ICC relapsed after the first session of RE. Two of their patients presented a significant hypotrophy of the hepatic lobe submitted to repetitive 90Y-RE with compensatory hypertrophy of the controlateral lobe. This clinical feature, also called radiation lobectomy, has been previously described by Gaba et al. who evaluated the hepatic volumetric changes in 315 patients treated with 90Y-microspheres. 20 In their cohort, 20 of the treated patients (i.e., 6.4%) presented a dramatic reduction in HLV with high response rate and prolonged survival. Among their patients, they registered 2 cases of radiation lobectomy. Both subjects received repeated unilobar administrations of 90Y-microspheres and, in agreement with the results reported by Gaba et al., showed complete response after the 2 consecutive procedures and were characterized by longer OS. It might be reasonable to hypothesize that the repeated administration of 90Y-microspheres may have triggered the phenomenon of radiation lobectomy in the targeted hepatic lobe.
TACE and 90Y-RE both represent transarterial locoregional procedures. In which sequence (i.e., TACE before 90Y-RE or vice versa) these two treatments should be placed in the therapeutic algorithm of ICC is a still unclear and debated argument, also due to the rarity of the neoplasia and the lack of randomized controlled clinical trials. 21 As concerns, the impact of TACE on survival, Kiefer et al. performed lobar or segmental chemoembolization with cisplatinum, doxorubicin, mitomycin-C, ethiodol, and polyvinyl alcohol particles in a cohort of 62 patients for an overall number of 122 procedures with a median survival from time of first chemoembolization of 15 months. 9 It is worth noting that, although there is a significant variability in the survival reported after TACE, a recent meta-analysis performed by Ray et al. reported a cumulative OS of 13.4 months from the first TACE treatment. 22 In their cohort of patients, they registered an OS of 16.5 ± 1.4 months, slightly higher than the median OS of 15.2 months reported in a recently published review collecting the data on the use of 90Y-microspheres for the treatment of ICC. 7 However, it has to be stressed that none of the aforementioned reports was specifically focused on ICC patients relapsed after a first administration of 90Y-microspheres, most probably affected by more aggressive and therapy-resistant lesions. In this regard, the survival data in the authors' cohort are substantially in line with those reported by Zarva in patients with advanced primary and secondary liver tumors and progressive disease after first selective internal radiotherapy. 10
This study presents several limitations. The main limitation concerns patients' dosimetry: in the authors' cohort of ICC patients submitted to repeated administrations of 90Y-microspheres, BSA method was used for activity calculation. Although currently applied in clinical practice, BSA method represents a semiempirical approach and does not provide a previsional calculation of the effective dose delivered to tumor and nontumoral liver tissue. 23 On the contrary, the so-called partition model based on the count ratios from the 99mTc-MAA pretreatment scan, describes the distribution of the microspheres into three compartments (lung, tumor, and nontumoral liver parenchyma) thus allowing predictive dosimetry to be performed for the each of the aforementioned compartments before 90Y-RE. 6 This issue is of great importance, as it has been fixed at 52 Gy the tolerance dose of the whole liver leading to a 50% complication probability (i.e., toxicity> grade 2). 24 Therefore, their preliminary results need to be confirmed implementing a previsional dosimetric approach. Furthermore, the small sample size of the patient population did not allow a statistically robust examination of the safety and efficacy of repeated 90Y-RE in ICC. Finally, it is worth mentioning that there are two commercially available medical devices for the locoregional treatment of liver tumors through RE. 25,26 The authors limited their analysis to the resin spheres, but it would be worthwhile to evaluate also the effects of repetitive administrations of glass spheres, which differ in the size of the single spheres, base material, and specific activity.
Conclusions
This study suggests that repeated administration of 90Y-microspheres in patients affected by ICC and relapsed after the first 90Y-RE may have a favorable impact on survival with a tolerable profile of toxicity. These preliminary results need to be confirmed implementing a personalized and previsional dosimetric approach. Furthermore, studies with larger series are needed to better define the potential benefits of repetitive 90Y-RE in ICC also taking into consideration the different commercially available 90Y-labeled microspheres.
Footnotes
Authors' Contributions
L.F.: Treatment and follow-up of patients, assessment of response and toxicity, and writing of the article. G.G.D.C.: Enrollment and follow-up of patients and assessment of toxicity. R.T.: Enrollment and follow-up of patients and assessment of toxicity. G.P.: Interventional procedure and assessment of response. R.C.: Interventional procedure and assessment of response. O.S.: Review of the clinical data and editing of the article. O.B.: 90Y-PET Imaging and assessment of the response.
Disclosure Statement
There are no existing financial conflicts.