
Abstract
Next-generation sequencing (NGS) data have been central to the development of targeted therapy and immunotherapy for precision oncology. In targeted therapy, drugs directly attack cancer, by altering the expression of critical cancer genes identified with cancer genome profiling. Immunotherapy drugs indirectly attack cancer, by inducing the immune system to attack and treat cancer. Harnessing genomic data for deployment and development of immunotherapy comprises the field of immunogenomics. The discovery of a link between cancer cells escaping immune destruction and cancer progression, led to extensive research into this mechanism and drug development. In the past few years, FDA has granted accelerated approval to several immunotherapy cancer treatment drugs, pembrolizumab, nivolumab, and atezolizumab, belonging to the class of checkpoint inhibitors. Utilization of pretreatment genomic cancer screening to identify patients most likely to respond to immunotherapy and to customize immunotherapy for a given patient, promises to improve cancer treatment outcomes. Recent advances in molecular profiling, high-throughput sequencing, and computational efficiency has made immunogenomics the major tenet of precision medicine in cancer treatment. This review provides a brief overview on the state of art of immunogenomics in precision cancer medicine.
Introduction
Cancer is a disease characterized by uncontrolled cellular growth that results in the formation of a tumor. Normal cells become cancerous due to genetic mutations and epigenetic modifications that result in spurious expression of genes that regulate cell growth and cell death. 1,2 Moreover, different cancers from different patients have different combinations of genetic mutations and epigenetic modifications, which increases cancer complexity and tumor heterogeneity. 3 Cancer heterogeneity increases during progression of the disease and makes cancer treatment especially challenging.
Conventional cancer treatment involves biopsy and laboratory tests, such as morphological and histological diagnosis of cancer, followed by a treatment regimen that involves a single or a combination of chemotherapy, surgery, and radiation therapy, decided based on the location and type of cancer. 4 This treatment pathway is not optimized on a case-by-case basis and therefore while some patients respond to the treatment, other patients remain unresponsive. Patients who are unresponsive to conventional treatments have poor prognosis (low survival rate) because they have aggressive cancers that are unresponsive to conventional treatments (refractory) or are minimally effected by conventional treatments, with high probability of reoccurrence (relapse). 5
Recent developments in next-generation sequencing (NGS) methods and bioinformatics tools have made an enormous amount of cancer genomics data available, which has spurred the development of targeted therapy and immunotherapy, especially in patients with aggressive cancers unresponsive to conventional treatment options. A recent study showed that in a breast cancer patient unresponsive to several chemotherapy treatments, immunotherapy resulted in complete disappearance of the tumor. 6 NGS technology was used to obtain massive amount of genomic data from cancer patients with acute myeloid leukemia and was later extended to different solid tumors in The Cancer Genome Atlas (TCGA) project. 7,8 NGS data from the TCGA project resulted in the development of a system of molecular classification for cancers, such as lung cancer and glioblastoma, to complement the conventional histology-based classification. 9,10
NGS profiles obtained from different cancers lead to the advent of targeted therapy, which involves identification of mutations in signaling pathways and blocking them with existing or newly developed drugs. The identified mutations were classified as druggable “driver” mutations, if they were essential for maintenance of cancer and nondruggable “passenger” mutations, if they had no clear role in cancer maintenance. The targeted therapy approach led to the development of imatinib, an inhibitor of driver constitutively active BCR-ABL kinase for the treatment of leukemia. 11 However, results from 21 different cancers showed that few of the druggable driver mutations were present in >20% of patients for a cancer type, while most of the druggable driver mutations were present only in 2%–20% of patients for a cancer type. 12 This low frequency of druggable driver mutations limits the effectiveness of targeted therapy for cancer treatment.
In normal physiological conditions, the immune system identifies and removes mutated cells. However, cancer develops when the cancer cells evade the immune system by creating an immunosuppressive environment. 13,14 Therefore, recently the focus has shifted from targeted therapy to immunotherapy, with the hope that it can be used to treat more patients because evading the immune system is common to all cancers and restoring the immune system could help destroy the tumor. 15 Confirming the optimism around immunotherapy, anti-CTLA4 antibody ipilimumab showed that immunotherapy can successfully treat cancer patients, and Phase III trials further showed that it improved the long-term survival of patients in remission (patients with no evidence of cancer). 16
Due to the heterogeneous nature of cancer, patients respond differently to immunotherapy and other therapies. 3 It is therefore critical to assess the patient-specific characteristics of cancer to device a treatment plan with the greatest chance of success. By using NGS technology to obtain a cancer genomic profiling for the patient can help customize the treatment to target specific characteristics of cancer and increase probability of success. 17 This type of treatment tailored to the patient-specific characteristics of cancer, is the basis of precision or personalized medicine. By combining immunotherapy with one or more of the conventional therapies (chemotherapy, surgery, and radiation therapy), researchers hope to increase the benefits of immunotherapy and avoid the pitfall of single therapy approach, where the tumor can become resistant to a single treatment. 18,19
This review provides a brief overview of the potential of immunogenomics in personalized cancer treatment.
Precision Medicine
Current cancer treatments include chemotherapy, radiation therapy, surgery, and more recently immunotherapy. 4,20 However, with the same treatment different patients respond differently and this difference is due to heterogeneity, which arises from inherent genetic variations between humans and the evolving genetic variations between cancer types. 21 –23 Precision medicine is the development of a patient-specific treatment plan through integration of information from patient's Electronic Health Record, genetic and socioeconomic background, and genetic variations in the patient's tumor, a treatment regimen can be tailored for each individual cancer patient (Fig. 1). This approach has the potential to improve patient outcome and spare the patient from going through treatment procedures unlikely to have any effect on their cancer. 24 As a cost-effective approach to treatment, precision medicine ensures meaningful use of health care resources. 25

A Comparison of conventional cancer treatment and precision medicine in cancer. Conventional cancer treatment includes surgery, chemotherapy, and radiation therapy, which are given to all cancer patients alone or in combination. However, in precision medicine, the treatment pathway is optimized based on cancer patient-specific NGS and immunotherapy. NGS, next-generation sequencing. Color images are available online.
Precision medicine is a newer term that was adapted to replace personalized medicine. There is a lot of overlap between the terms “precision medicine” and “personalized medicine”. Based on the individual characteristics of the patient, precision medicine implies tailoring existing treatment regimens to best suit the patient and does not imply creating new treatment. However, personalized medicine is often misinterpreted to imply creation of new treatment based on patient characteristics. Creation and development of new treatments is a time-consuming process, and is unlikely to be completed soon enough to benefit the individual patient who already has the cancer. Therefore, in 2011, the U.S. National Research Council (NRC) that governs policies and governs advances in science, technology, engineering, and mathematics (STEM) adapted the use of the term “precision medicine” over “personalized medicine”. 26
NGS and Cancer
NGS or high-throughput parallel sequencing, is a technology that allows us to collect a large amount of genomic information. Soon after the completion of the human genome project, 33 different cancer types were sequenced to identify mutations and copy number variations associated with cancers, and the data were made publicly available on TCGA project and International Cancer Genome Consortium (ICGC). 27,28 The Cistrome Cancer project is a comprehensive database for prediction of transcription factor binding in cancer and combines the NGS methods of chromatin immunoprecipitation (ChIP-seq), and RNA-seq to unravel the mechanism of transcription-regulated gene expression in cancer. 29
MethyCancer database contains high-throughput cancer datasets of DNA methylation and CpG islands, and revealed the landscape of epigenetic regulation in cancer. 30 A recent study, which utilized gene expression from TCGA and transcription factor binding data from Cistrome, found that transcription factors SKI and RUNX1 occupy the same genomic sites to silence gene expression in acute myeloid leukemia. 31 This demonstrates the potential of publicly available NGS data to expand ones understanding of regulatory mechanisms in cancer.
Increased efficiency and reduced cost of sequencing has resulted in comprehensive whole genome sequencing (WGS) of cancer, for identification of cancer mutations to help improve cancer subtype molecular classification and drug discovery. 32 For example, genetic test to detect BRCA1 and BRCA2 mutations is now a standard procedure to test for risk of breast cancer in individuals with a family history of breast cancer. 33 SNP500 Cancer and Catalogue of Somatic Mutations In Cancer (COSMIC) are large databases that contain a comprehensive collection of genetic variations in cancer and associated deidentified patient information. 34,35 These genetic variation open source cancer databases have the major goal to encourage comprehensive research into identification and experimental validation of cancer mutations for diagnostic and therapeutic applications. 1
Integration of datasets from different NGS techniques profiling cancer genetic sequence, gene expression and epigenome, and its changes in response to small molecules or drugs, is aimed to facilitate rational drug design targeting various aspects of cancer biology. The NCI-60 panel database and its newest extension CellMinerCDB, is such a comprehensive resource that contains genome-wide RNA expression, cancer mutation, enzyme activity, and drug interaction data for 60 human cancer cell lines from NCI and other cell lines in CellMinerCDB, totaling to around 1000 cell lines. 36,37 There is limited data on combinatorial drug response in cancer. In a recent study, deep learning computational modeling was applied to NCI-60 drug perturbation genomics data to predict combinatorial drug genomic response. 38 This shows the power of NCI-60 and CellMinerCDB databases, and advanced computational tools to predict responses of combinatorial drugs in cancer treatment in the absence of experimental data.
Taken together, the comprehensive evaluation of cancer with high-throughput NGS methods, has revealed extensive molecular complexities in cancer and has paved the path for applying this information for development of new therapies and precision medicine. Presently, NGS or genomics is transforming immunotherapy-based precision treatment of cancer, which will be discussed below.
NGS-Guided Immunotherapy for Precision Medicine in Cancer Treatment
The immune system is the defense system of the body, which has the inherent ability to recognize and remove disease-causing agents and mutated cells. 39 However, occasionally the cells of the body mutate to proliferate uncontrollably and develop mechanisms to evade recognition by the immune system. 13 Unchecked by the immune system, these mutated cells proliferate uncontrollably resulting in cancer. Immunotherapy is a strategy used to restore and potentiate the patient's immune system, so that it can recognize, attack, and remove cancer cells. 40
Immunotherapy alone or immunotherapy in combination with conventional cancer therapies can be used to improve cancer treatment outcomes. Radiotherapy damages cancer cells and its surrounding microenvironment to trigger an immune response, which can be further potentiated by including immunotherapy in the treatment plan. 41 –43 Surgery is used as a treatment option for most solid tumors and resection of tumor leads to suppression of the immune response, allowing for development of cancer from the remaining cancer cells that escape into the blood after surgery. 44 Therefore, it is speculated that applying immunotherapy after surgery can be an effective method to destroy cancer cells that remain after surgery. 45
However, immunotherapy is not equally effective in all cancer types and efficacy varies between patients. 46 The probable reasons that are preventing widespread success of immunotherapy to stimulate an immune system attack on cancer, is potentially the heterogeneity that exists in both T cells and cancer cells, and the complex interactions between them in the tumor microenvironment. Immunogenomics, is a relatively new field of cancer research, wherein NGS is utilized to obtain genomic profile of both cancer and immune cells. 47
Recent advances in single-cell RNA-seq and ChIP-seq techniques, promise to uncover at single-cell level the transcriptomic and epigenetic heterogeneity in cancer cells and the immune cells. 48,49 Single-cell RNA-seq in glioblastoma showed extensive heterogeneity in cellular gene expression levels for genes belonging to proliferation, immune response, and hypoxia. 50 The genomic profile of cancer and immune cells can expand ones understanding of their molecular heterogeneity and their interactions in the tumor microenvironment, which can be translated to increase efficacy of immunotherapy.
Cytokines occur naturally in the body and regulate homeostasis of the immune system. This has given rise to a type of immunotherapy, where cytokines are administered to the patient for systemic modulation of the host immune system. 51 IL-2 is a cytokine that is FDA approved for use in high doses for treatment of melanoma and renal cell carcinoma. 52 However, due to the dual role of cytokines as immune response activators and repressors, and toxicity at higher doses, its application has been limited in cancer therapy. 53 Monoclonal antibodies are used in targeted therapy to block abnormal proteins expressed by the cancer cells, such as the FDA-approved cetuximab and panitumumab that inhibit epidermal growth factor receptor. 54 Recently, monoclonal antibodies have gained widespread interest and application in checkpoint inhibitor immunotherapy for cancer treatment. 55
Three types of immunotherapy approaches, checkpoint inhibitors, vaccine immunotherapy, and CAR T cell therapy, have emerged as forerunners of cancer immunotherapy due to their ability to specifically target and induce an immune response in cancer. 56 These three immunotherapy methods, have greatly benefited from advancements in NGS and immunogenomics has the potential to further propel their development as discussed in the sections below.
Checkpoint inhibitors and NGS
T cells are a key component of adaptive immunity and are activated by a two-step process (Fig. 2). 57 In the first step of T cell activation, T cell receptor (TCR) binds to an antigen on major histocompatibility complex (MHC) of antigen-presenting cells (APCs), such as macrophages. In the second step of T cell activation, stimulatory interactions occur between CD28 receptors on T cells and B7 ligands on APCs. The immune system has inbuilt checkpoints that prevents activation of T cells or immune attack on normal cells. Cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) and programmed cell death protein 1 (PD-1) are receptors expressed on the surface of T cells to inhibit T cell activation. CTLA-4 negatively regulates activation of T cells by competing with CD28 for B7 ligands on APCs. 58 Normal cells in the body express Programmed Death Ligand 1 (PD-L1) on their surface to interact with Programmed Death 1 (PD-1) on T cells at the immune checkpoint to signal T cells not to attack. 57 Unfortunately, many cancer cells mimic normal cells by expressing PD-L1 or other mutations of their cell surface proteins and thereby escape T cell attack. 59

Checkpoint inhibitor-based immunotherapy, NGS and immunogenomics. Cancer cells express PD-L1 antigens on cell surface to escape the immune response by binding with PD-1 receptor on T cells. Checkpoint inhibitors are monoclonal antibodies that bind to PD-1 on T cells (shown in this figure) or PD-L1 on cancer cells (not shown in this figure) to remove this blockade of immune response. Thus, reactivated T cells attack and remove cancer cells by apoptosis or programmed cell death and curing the patient. NGS methods of WGS, Exome sequencing and transcriptome analysis (RNA-seq) of T cells and cancer cells, facilitates development of effective checkpoint inhibitors. PD-L1, programmed death-like1; WGS, whole genome sequencing. Color images are available online.
A class of cancer drugs called checkpoint inhibitors have emerged that help remove the immune checkpoint inhibition induced by cancer cells, to restore normal immune function and allow the T cells to remove cancer cells. 60 Monoclonal antibodies have been used as immune checkpoint inhibitors for targeting CTLA-4, PD-1, and as PD-1 ligand. FDA-approved immune checkpoint inhibitors include ipilimumab an anti-CTLA-4 agent, nivolumab and pembrolizumab anti-PD-1 agents, and atezolizumab anti-PDL-1 agent. 61 However, this cancer cell and T cell response is highly dynamic at the molecular level and does not always work in all cancers. Less than 25% of melanoma patients treated with ipilimumab benefited from the treatment, while an additional 64% experienced adverse side effects. 62,63
NGS methods of exome sequencing and RNA-seq of tumors can help prescreen patients at the molecular level to identify patients who will be responsive to the checkpoint inhibitors, thereby increasing the benefit and reducing side effects. Whole exome sequencing (WES) data from melanoma patients showed that the number of mutations in the cancer and presence of cytolytic markers in the cancer microenvironment were strongly correlated with the therapeutic benefit of anti-CTLA-4 agents. 64 This study also obtained transcriptome data and found that high expression of granzyme A (GZMA) and perforin (PRF1), improves response to checkpoint inhibitor-based immunotherapy. 64 The cancer microenvironment consists of different types of cells that support cancer growth and prevent immune attack on the tumor. NGS techniques can be used to identify and characterize the cells in the tumor microenvironment, to enable development of strategies for blocking their immunosuppressive function. 65
A recent study utilized exome sequencing, RNA-seq, and a machine learning computational pipeline, to reveal that a complex heterogeneous microenvironment exists within the same lung cancer tumor, such that each region of the tumor has a different microenvironment composed of distinctly different cancer cell and T cell profiles. 66 Taken together, these studies demonstrate the benefit and need for cancer NGS data, to better understand cancer, tumor microenvironment, and T cells for improved checkpoint inhibitor immunotherapy.
Vaccines for immunotherapy and NGS
The immune system attacks and removes foreign antigens and APCs (Fig. 3). This feature of immune cells is what makes vaccines effective because the vaccine trains the immune system to develop antibodies against the foreign antigen, so that the immune system can recognize the foreign antigen and attack the antigen-producing foreign cells. Cancer cells often express mutated cell surface proteins and secrete mutated proteins, called neoantigens. 67 These mutated epitopes are processed and presented by MHC molecules for recognition by the T cells. 67 Therefore, one approach of immunotherapy is to develop vaccines, which are putative antigens that the cancer cell is likely to express or secrete. This putative antigen is then used to train the immune system, so that it can develop antibodies to recognize and attack the cancer cells. 68
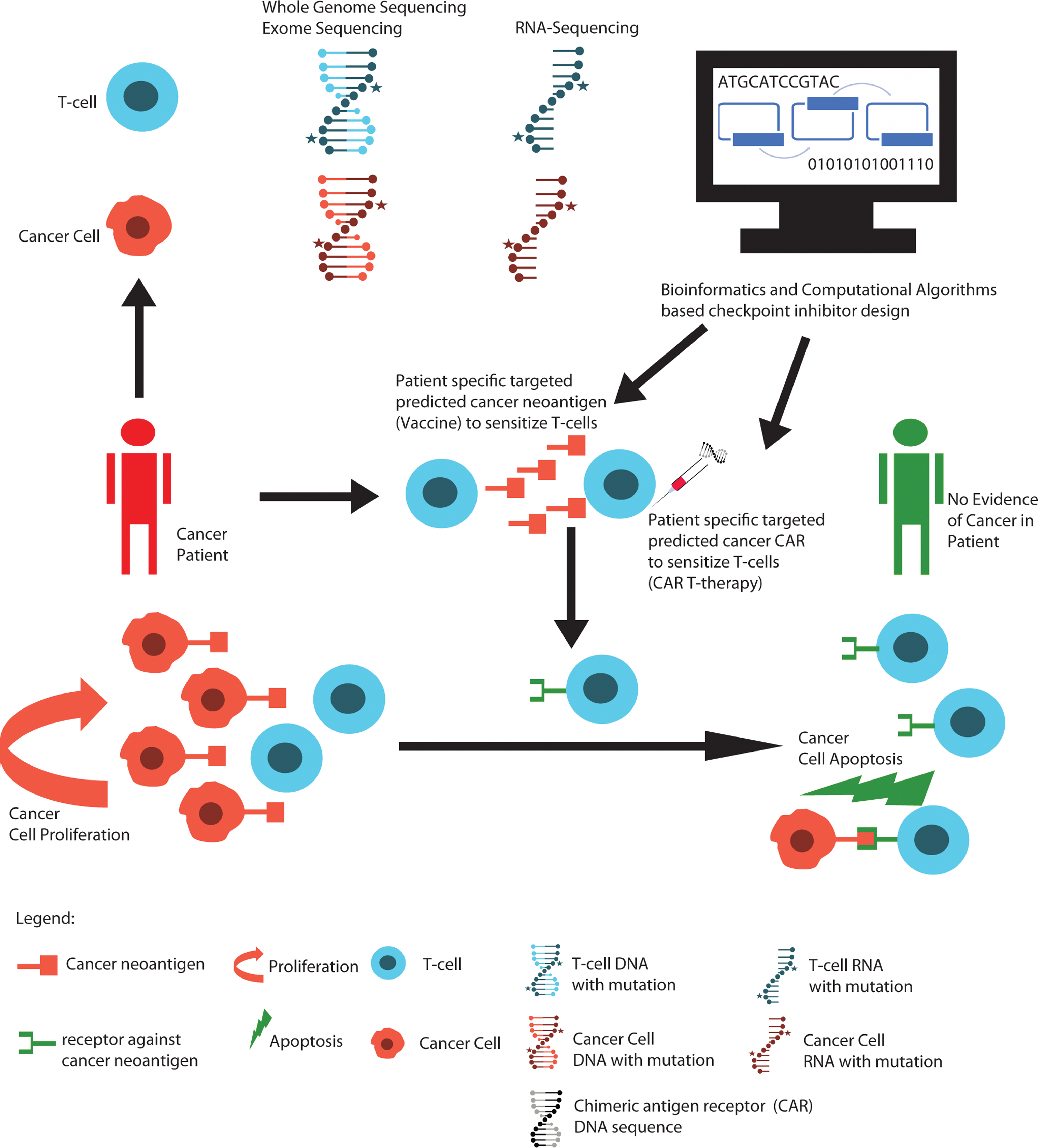
Cancer vaccines, CAR T cell immunotherapy, next-generation sequencing and immunogenomics. Cancer cells secrete and express on cell surface neoantigens that evade recognition by T cells in the patient. Patient-derived T cells can be grown outside the body and treated with these neoantigens to stimulate a robust T cell response (vaccine immunotherapy). To further potentiate the ability of the T cells to recognize cancer, CAR coding DNA is introduced into the T cells (CAR T cell therapy). Once the T cells are thus potentiated they are transferred back into the patient, where they now recognize the cancer antigens with increased effectiveness to induce cell death and removal of cancer. NGS methods of WGS, exome sequencing and transcriptome analysis (RNA-seq) of T cells and cancer cells, facilitate improvement in design of CAR T cells and selection of neoantigen. CAR, chimeric antigen receptor. Color images are available online.
NGS techniques aid in identification and prediction of antigens from cancer cell by mapping all mutations present in the cancer genomic profile to the normal genome, and applying bioinformatics tools to identify variations. The antigen can then be synthetically made using recombinant proteins, to vaccinate and activate an immune response. 69 Neoantigens hold enormous potential for development of customized vaccines for precision oncology. However, WES of epithelial cancer patients and experimental validation of T cell responsiveness to neoantigens, showed that patients responded to less than 1% of neoantigens developed based on the cancer mutation profile. 70 Larger cohort NGS studies will be needed to know if these results are consistent in other types of cancers. Therapeutic cancer vaccines have also been shown to improve the treatment outcome of chemotherapy and checkpoint inhibitors. 71
Advances in NGS technologies, computational algorithms, and bioinformatics tools, are expected to improve identification of neoantigens and improve the outcome cancer vaccine for precision oncology. 72,73 Single-cell genomics will be particularly useful to uncover the heterogeneity of cancer gene expression, mutations, and new types of immune cells within the same tumor, which could then be applied for development of cancer vaccines targeting distinct clonal populations within the tumor. 74,75
CAR T cell therapy and NGS
In vaccines for immunotherapy, the immune system is stimulated to produce antibodies inside the body or in vivo, while in adoptive T cell therapy (ATCT), the T cells are isolated from the body, expanded, and stimulated ex vivo before being infused back to the patient (Fig. 3). 76 A type of ATCT, where the heightened immune response of T cells is achieved by genetic modification of T cells with chimeric antigen receptors (CAR-T cells), has generated great interest in recent times. 77 In the CAR T cell therapy approach, T cells are altered ex vivo or outside the body to express a novel protein or a CAR directed to the antigen expressed on the cancer cell surface. The CAR protein fuses an extracellular single-chain fragment variable monoclonal antibody-derived domain, with an intracellular TCR-derived domain, which results in heightened T cell antigen recognition and binding. 78 Next, these modified T cells are returned into the patients' body, where the T cells can recognize the surface antigen on the cancer cell or secreted antigens from the cancer cells, and attack the tumor.
CAR T cell therapy has been highly effective in clinical trials of leukemia patients and are being developed for other cancer types. 79,80 Treatment of acute lymphoblastic leukemia patients with CAR T cells targeting CD19, which is expressed in high levels specifically in B cells, was highly successful and >90% of patients entered remission. 81 A major challenge for application of CAR T cell therapy in precision medicine is the limited information on cancer-specific target antigens or neoantigens, similar to the challenge faced in application of cancer vaccines for immunotherapy. Additionally, the lack of information about T cell heterogeneity resulting from differences in sequences of TCRs called TCR repertoire analysis, further deters CAR T cell immunotherapy.
Recently, a breakthrough came in the understanding of T cells heterogeneity and TCR repertoire, when single-cell RNA-seq revealed at least 11 types of T cells in liver cancer, which had distinct molecular and functional properties. 82 This new-found realization of the complexity of T cells has the potential to facilitate improvement of CAR T cell and other T cell-based immunotherapies. NGS and bioinformatics algorithms have the potential to profile and analyze T cells, cancer cells, and develop more effective CAR T cell therapy.
Deep Learning for Immunogenomics
Cancer genomics data have grown both in content and complexity, with TCGA alone housing ∼2.5 pentabytes of cancer data from RNA-seq, WES, WGS, and other NGS techniques. 83,84 This growth of genomics data has stimulated the growth of computational methods to improve one's ability to integrate and interpret these data for new insights into cancer biology for innovations in cancer treatment. Machine learning involves the use of algorithms to analyze and learn from a vast amount of data called training data, to predict values that may be acquired in the future. Deep learning is a subset of machine learning that utilizes multilayered neural networks, inspired by biological neural networks of human brain, to extract useful conclusions and predictions from input data or training data analysis in an automated manner. 85 Deep learning is especially useful when large amount of data or big data is available, which is the case for genomics cancer data and could potentially be used to predict the best therapeutic agent for a patient given their cancer genomic profile.
As proof of concept, a recent study applied deep learning and other machine learning methods to develop a predictive model for drug efficacy when cancer genomic profile is available. 86 Publicly available genomics data collected from 624 cancer cell lines for 140 drugs were obtained from Genomics of Drug Sensitivity in Cancer. 87 This gene expression data, which were measured using Affymetrix array were normalized and the selected 3080 gene expression values were used for deep learning for all samples. To train the deep learning algorithm, 520 samples were utilized and the remaining 104 samples were utilized to test the predictive ability of deep learning model. The authors showed that even after adding some complexity from genetic variations, such as copy number variations, deep learning could predict most effective drugs on a cancer cell line with 0.82 sensitivity and specificity. 86 These results are promising and pave the path for development of more high-throughput NGS-based development of deep learning models that could be used to predict not only sensitivity of cancer cells to conventional drugs, but also to immunotherapy.
It will be interesting to train deep learning models using available genomics profile from cancer-targeted immunotherapy, and test its ability to predict the most suitable cancer cell surface antigens and neoantigens to use for development of CAR T cells and immunotherapy vaccines, respectively. Although deep learning based on neural networks have an incredible ability to integrate complex information, one of the caveats of deep learning predictions is that it is not easily interpretable compared with its more simplistic counterparts, such as linear or logistic regression models. Therefore, deep learning predictions should be developed using large datasets to avoid skewing the model and predictions should be experimentally validated before application to real patients.
Current Challenges in Immunogenomics
In the immunosuppressive cancer microenvironment, normal T cells gradually become partially or fully dysfunctional and this process is called T cell exhaustion. 88 Immunotherapy approaches discussed above, such as checkpoint inhibitors and CAR T cell therapy, are geared toward restoration of the function of T cells. However, checkpoint inhibitors are successful in restoring function of only partially exhausted T cells and are ineffective against fully exhausted T cells. 89 Other studies have shown that CAR T cells generated from T cells potentially exhausted by the presence of PD-1 in the tumors are less effective in cancer treatment, and the CAR component itself can induce exhaustion of T cells. 90,91 The incomplete restoration of T cell function by checkpoint inhibitors and exhaustion of CAR T cells could account for limited success of immunotherapy and restoration of exhausted T cells could be key to improving efficiency of immunotherapy.
Single-cell RNA-seq revealed several differentially expressed genes between functional and exhausted T cells, and they experimentally showed that overexpression of a relatively unknown gene LAYN (Layilin) in a retroviral vector, was sufficient to suppress the function of functional T cells. 82 It can be speculated that future advances in their understanding of T cell exhaustion with genomics and experimental techniques, will facilitate development of novel solutions to overcome the challenges associated with low immunotherapy efficiency caused by T cell exhaustion.
Although CAR T cell therapy is one of the most promising immunotherapy methods, its usage is accompanied by the adverse side effects of cytokine release syndrome (CRS) and CAR-related encephalopathy syndrome. 92 Recently, it has been shown that CAR T cells indirectly cause CRS by inducing macrophages to release IL-6, IL-1, and nitric oxide. 93 One approach to minimize the side effects of CAR T cell therapy could be to decrease the CAR T cell persistence and requirement in the body by making CAR T cells more efficient. CRISPR/Cas9 genome editing presents a unique opportunity to engineer different batches of CAR T cells, each with a different modification on the genomic sequence of the CAR T cells so that the most efficient CAR T cells can be selected.
The advantage of CRISPR/Cas9 genome editing for generation of CAR T cells over the currently used virus-based genome modification process, is that CRISPR/Cas9 is more precise and quicker. In a mouse model of lymphoblastic leukemia, CRISPR/Cas9-edited CAR T cells were shown to reduce T cell exhaustion relative to conventional CAR T cells. 94 However, due to potential off-target effects of CRISPR/Cas9, which may change based on the context of genetic background, it has been challenging to apply CRISPR/Cas9-edited CAR T cells to human cancer patients. 95
It is anticipated that WES and WGS type of NGS data will need to be obtained from patient tumor samples to determine its unique genetic variations, which can help the design of customized CRISPR/Cas9-edited CAR T cells with minimal side effects and increased efficiency. Future studies that integrate genomics, computation, and experimental research will need to be conducted to further understand the therapeutic potential and safety concerns associated with CRISPR/Cas9-edited CAR T cells in treatment of cancers in humans.
Concluding Remarks
Future studies are required to determine effects of combinatorial treatments and dosing of immunotherapy drugs. With decreasing cost and increasing accuracy of NGS applications, such as WGS, WES, RNA-seq, and ChIP-seq at the bulk tissue and single cell level, our understanding of the immune cell and tumor interaction is expected to improve and be translated for development of personalized medicine. These NGS datasets will be especially useful if they are collected for many patients to increase statistical power and the patients are followed up over an extended period to track temporal changes in genomic profile. Toward this direction, a longitudinal study of cancer called TRACERx has been established to obtain cancer genomic profiles from many patients across different cancer types. 96
Additionally, new NGS technologies are also rapidly evolving, with NICHE-seq generating much excitement among cancer researchers due to its ability to add spatial information to single-cell RNA-seq data obtained from tumors engineered to express photoactivable GFP protein. 97 This rapid increase in NGS data content and dimensions will require an equal evolution of high-performance computational methods and algorithms, for us to synthesize this information into experimentally testable and translationally applicable knowledge for personalized medicine.
Footnotes
Acknowledgments
This work was conducted at the author's home in Garland Avenue, Downtown Los Angeles, Los Angeles, U.S. on personal laptops (MacBook Pro and Windows OS) with high-speed internet connection. The author is most grateful to NIH/NLM (U.S. National Institute of Health's National Library of Medicine) for access to free full-text scientific publications on PubMed Central
Disclosure Statement
No competing financial interests exist.