
Abstract
Objective:
This study aims to investigate the expression changes of periostin (PN or OSF-2) in oral leukoplakia (OLK) and oral squamous cell carcinoma (OSCC), and analyze its significance in the development of OSCC.
Study Design:
The expression of periostin was detected from tissue specimens and serum obtained from normal mucosa, OLK and OSCC by immunohistochemistry, enzyme-linked immunosorbent assay, and quantitative polymerase chain reaction.
Results:
Periostin was significantly overexpressed in OLK and OSCC, when compared with normal controls (p < 0.05). Furthermore, the overexpression of periostin was positively correlated with TNM stage, depth of invasion, and lymph node metastasis (p < 0.05).
Conclusion:
The overexpression of periostin may be involved in the carcinogenesis process of OLK, which may be used as a marker for detecting OLK. In addition, periostin serum levels can be used as a potential indicator of invasion and a prognosis target for OSCC.
Introduction
Cancer incidence and mortality are rapidly growing worldwide. New global cases and deaths of lip and oral cancer account for 2% and 1.9%, respectively, of all site cancers in 2018. 1 Oral squamous cell carcinoma (OSCC) is one of the most common malignant tumors in head and neck cancer, and the 5-year survival rate remains below 50%, regardless of aggressive treatment modalities. 1 Oral leukoplakia (OLK) is a potentially malignant disorder with a high risk of transitioning to OSCC, and 9%–19% of white spots can potentially convert to OSCC. 2 A large number of clinical evidence and animal models have proven that oral cancer generally undergoes a regular change of normal mucosa-abnormal epithelial hyperplasia-carcinoma in situ. 3 OSCC can cause serious consequences. It not only reduces the patient's survival rate but also affects the patient's quality of life, in terms of appearance, aesthetics, chewing, and swallowing. The 5-year survival rate of patients remains at revise to 40%∼50%, 4 because the disease is usually diagnosed at an advanced stage. Hence, there is an urgent need to explore molecular biomarkers that can predict the malignant changes of oral precancerous lesions to oral cancers. Periostin (PN or OSF-2) is an extracellular matrix-secreted protein secreted by osteoblasts and osteoblast-like cells. It was first cloned as a kind of bone adhesion from the mouse osteoblastic cell line. 5 Periostin plays important roles in the regulation of most cellular processes, such as cell proliferation, differentiation, migration, and survival. It is expressed in the periosteum, periodontal ligament tissues, lung, skin, kidneys, heart valves, damaged muscles, and blood vessels. 6 –11
Although previous studies have demonstrated that periostin is significantly upregulated in cancer tissues and cell lines, 12 the expression level of periostin in patients with OSCC remains presently unknown, especially the serum expression level of periostin. Therefore, the aim of the present study was to evaluate the expression level of periostin in OLK and OSCC patients, and determine its potential clinical value.
Materials and Methods
Patients and tissues
Pathological wax blocks with OLK and OSCC were collected from patients who were diagnosed by the Department of Pathology, Union Hospital, Fujian Medical University, between September 2015 and February 2017, were collected. The diagnosis was based on the World Health Organization (WHO) oral mucosal precancerous lesions and oral cancer diagnosis and classification criteria. The specimens for immunohistochemistry (IHC) included hyperplastic OLK (15 cases), dysplastic OLK (25 cases), well-differentiated squamous cell carcinoma (19 cases), moderately differentiated squamous cell carcinoma (12 cases), and poorly differentiated squamous cell carcinoma (14 cases). A total of 30 samples of normal gingival mucosa obtained during the orthodontic tooth extraction were used as controls. For the polymerase chain reaction (PCR) assay, the surgical landmarks of the new cases from the Affiliated Union Hospital of Fujian Stomatological Clinic from March 2017 to March 2018 included dysplastic OLK (25 cases), well-differentiated squamous cell carcinoma (8 cases), moderately differentiated squamous cell carcinoma (10 cases), and poorly differentiated squamous cell carcinoma (27 cases). The source of the PCR control group was the same as that in the IHC experiment, and the cases for the enzyme-linked immunosorbent assay (ELISA) were homologous with the cases for the PCR assay. The ELISA control group was derived from the blood test of the orthodontic pre-existing patient in the IHC experimental control group. After obtaining a written informed consent from the participating patients, their detailed medical history, clinical details, and habit history regarding type, form, frequency, and duration of tobacco/areca nut/alcohol use were recorded. The present study was approved by the Scientific Research Project Ethics Committee of the Union Medical College Affiliated to Fujian Medical University (2017KY003).
Exclusion criteria
The exclusion criteria were as follows: patients suffering from precancerous lesions with tumors on other sites; patients with immune system diseases, such as systemic lupus erythematosus and pemphigus; patients with allergic diseases, such as allergic rhinitis and bronchial asthma; and patients with diseases that are positively correlated to periostin protein levels, such as acute infectious diseases or acute myocardial infarction.
Immunohistochemistry
The biopsy samples were fixed in 4% paraformaldehyde, routinely processed for histology, and embedded in paraffin wax. Four-micrometer-thick sections were cut, and the SP method was used for the oral cancer surgical specimens [streptavidin-perosidas (SP) kit; ZSGB-BIO, China]. Then, the tissues were formalin fixed, paraffin embedded, and heated in an oven at 60°C for 2 h. Afterward, the tissues were fixed in 3% H2O2 solution in room temperature for 10 min to eliminate endogenous peroxidase. Next, a pH 6.0 citrate buffer was used for antigen retrieval, and 5% phosphate-buffered saline blocking agent and primary mouse monoclonal antibodies against humans (ab14041; Abcam Co, Ltd., Tokyo, Japan) were used at dilutions of 1:800. A DAB color microscope was used to observe the staining results. Afterward, the sections were counterstained with hematoxylin, dehydrated, and mounted.
Quantitative real-time PCR
RNA extraction
RNA was extracted from frozen tissue specimens using the RNAiso Plus reagent (Takara Bio, Shiga, Japan), according to the manufacturer's instructions. Complementary DNA (cDNA) was synthesized using a Prime Script RT Reagent Kit with a gDNA Eraser (Takara, Japan), according to the manufacturer's instructions.
Quantitative real-time PCR
The optical density (OD) 260/280 value was measured by ultraviolet spectroscopy, and the RNA concentration was calculated. Reverse transcription was performed, according to the instructions of the reverse transcription kit (Takara Bio), to synthesize the cDNA. The following primers were used to amplify the periostin gene (sense primer: TAAACTCCTCTATCCAGCAGAC, and antisense primer: CCACCTCCAGTAGAAATCCT). The GAPDH gene (sense primer: CAAGGTCATCCATGACAACTTTG, and antisense primer: GTCCACCACCCTGTTGCTGTAG) was used as an internal control. The reaction was performed in a LightCycler480 system (Life Technologies, Inc., Thermo Fisher Scientific, Waltham, MA) using SYBR Premix Ex Taq (Takara), according to the manufacturer's protocol. Briefly, the thermal cycling for all genes was initiated with a denaturation step at 95°C for 30 s, followed by 40 cycles at 95°C for 5 s and 60°C for 30 s, and 1 cycler at 95°C for 5 s and 60°C for 60 s. After obtaining the Ct value, the 2−ΔΔCt method was used to calculate the relative expression of the target genes.
Enzyme-linked immunosorbent assay
Empty venous blood samples (5 mL) were obtained from each subject. At 30 min before extraction, the blood was centrifuged at 3000 rpm for 15 min to separate the serum, and this was subsequently refrigerated at −80°C. Serum periostin was detected using an ELISA Kit (No. PG48T; Shanghai Yan Ji Bio Technology Co., China). Then, the serum samples were diluted at proper proportions, the standard (100 μL) and diluted samples (100 μL) were added into the ELISA plate, and this was covered by a membrane. The contents of the ELISA plate were discarded after the reaction, and 100 μL of ELISA reagent was added into each well for incubation at 37°C for 30 min. Then, 100 μL of chromogenic agent A and 100 μL of chromogenic agent B were mixed in each well after washing with phosphate-buffered saline for three times, and at that juncture, the chromogenic reaction was carried out at 37°C in the dark for 15 min, followed by the addition of 100 μL of stop buffer, to halt the reaction. The OD value was measured at a wavelength of 450 nm in a microplate reader. The calculation of the final density of samples was carried out using the corresponding concentration on the microplate reader, which was multiplied by dilution.
Statistical analysis
Statistical analysis was performed using SPSS 18.0 (SPSS, Inc., Chicago, IL). The expression of periostin in different tissues was expressed as mean ± standard deviation, and the difference in expression was compared by t-test. The relationship between the expression of periostin and the clinicopathological parameters was analyzed by χ 2 test. A p-value of <0.05 was considered statistically significant.
Results
Periostin expression in OLK and OSCC specimens
The IHC staining revealed that periostin was expressed in the basal layer and part of the spinous layer of the oral normal mucosa and OLK, and was mostly located in the interstitial or scattered interstitial cells of cancer cells in squamous cell carcinoma (Fig. 1). Furthermore, periostin expression gradually increased with the degree of dysplasia. Except for the hyperplastic OLK and normal oral mucosa, the difference in the rest of the groups was statistically significant (p < 0.05, Table 1). The expression in OSCC was significantly higher than that in simple hyperplastic OLK and dysplastic OLK (p < 0.01). Furthermore, in OSCC, the expression quantity of periostin was dependent on the tumor differentiation degree of patients, and TNM staging and lymph node metastasis were also taken into account (p < 0.05, Table 2).
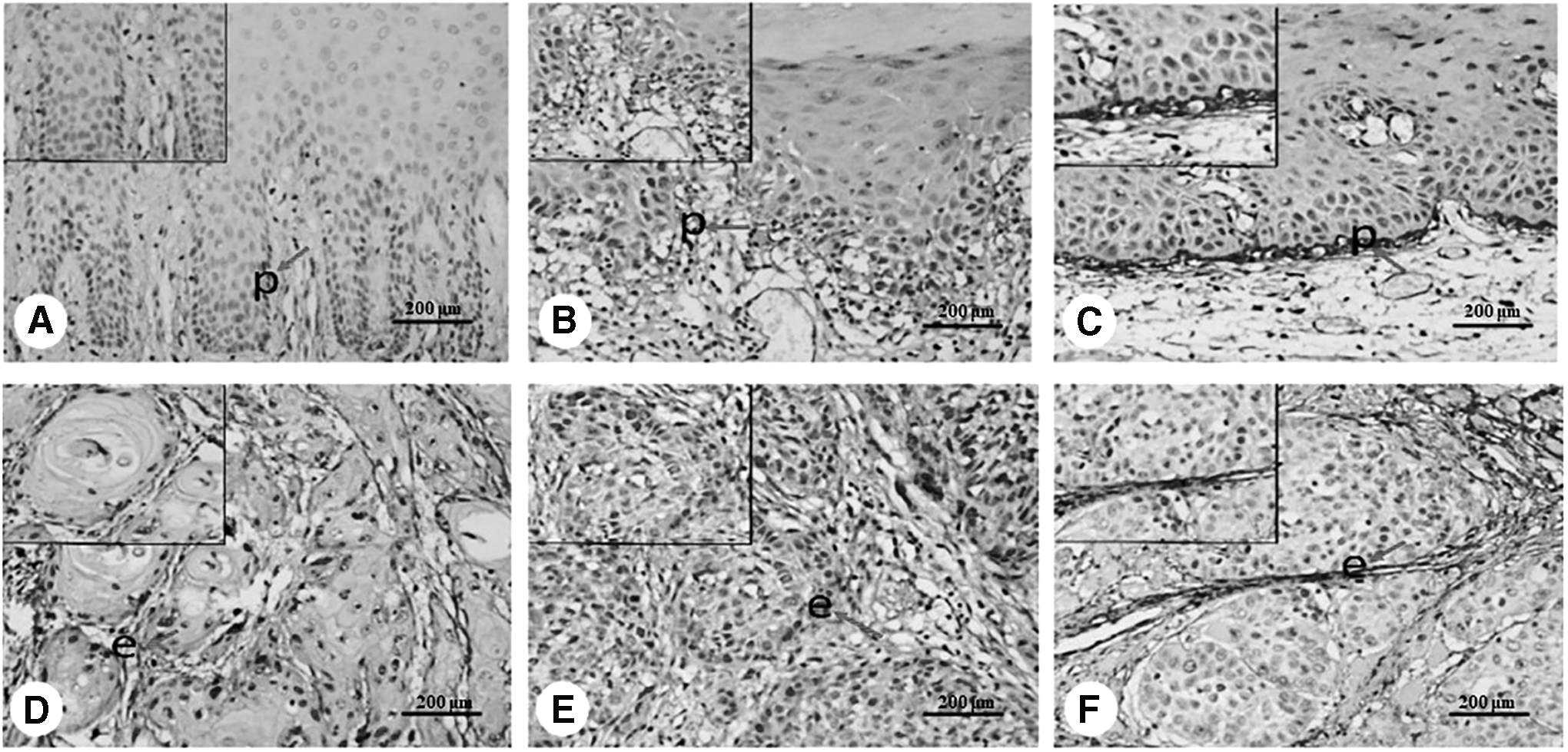
Periostin is expressed in the basal and suprabasal layers of the epithelium as “p” in normal oral mucosa
Periostin's Index of Positive Cell Vessels and the Integrated Optical Density Value in Oral Normal Mucosa, Oral Leukoplakia, and Squamous Cell Carcinoma (
Normal mucosa compared with hyperplastic leukoplakia, * p > 0.05; dysplastic leukoplakia compared with hyperplastic leukoplakia, & p < 0.05; moderate/severe leukoplakia compared with well-differentiated OSCCs, Φ p < 0.05; well differentiated compared with moderately/poorly differentiated, Δ p < 0.05.
IA, integrated optical density; OSCC, oral squamous cell carcinoma.
The Relationship Between Periostin Expressions and Clinical Pathological Parameters in Oral Squamous Cell Carcinoma
The mRNA expression of periostin was detected in all three groups (Fig. 2). The mRNA expression of periostin in normal oral mucosa, dysplastic OLK, and OSCC was 0.326074 ± 0.412194, 0.751156 ± 0.250896, and 1.37044 ± 0.500052, respectively. Compared with normal oral mucosa, the mRNA expression of periostin in oral OLK and OSCC also significantly increased, and this expression increased during the progression from abnormal hyperplasia to squamous cell carcinoma (p < 0.01, Fig. 3).
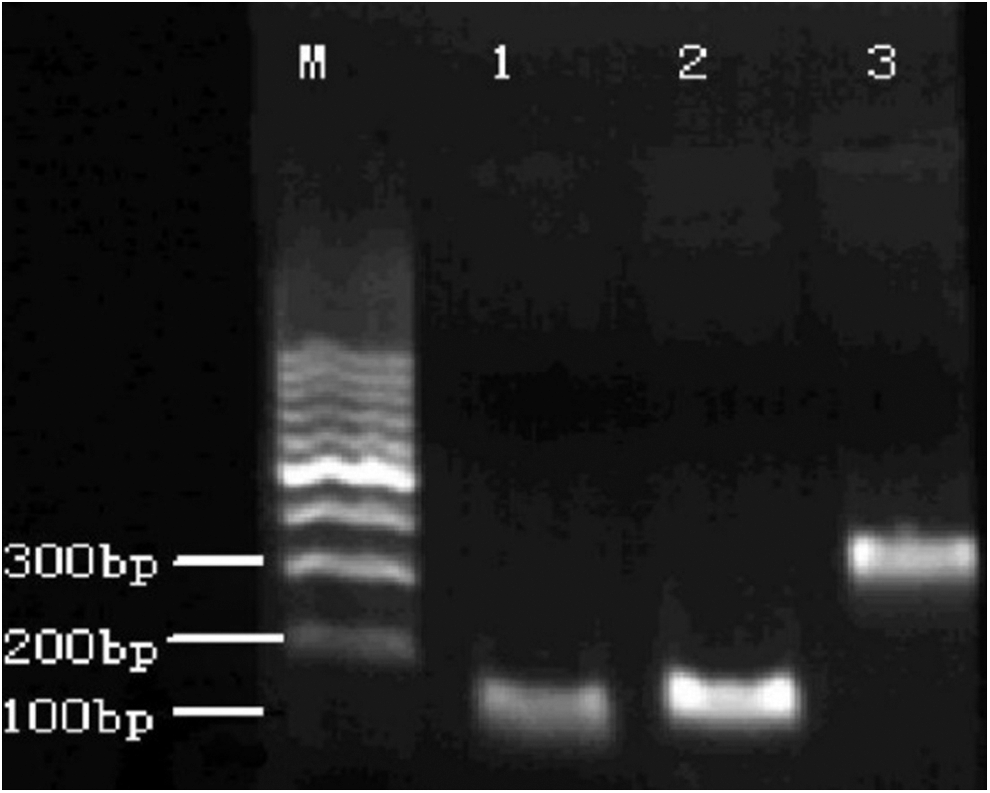
Using the marker as a standard, the length of the GAPDH-amplified fragment was 397 bp, while the length of the amplified fragment of the target gene periostin was 132 bp. Periostin gene expression was present in OLK and OSCC in the experimental group. OLK, oral leukoplakia; OSCC, oral squamous cell carcinoma.
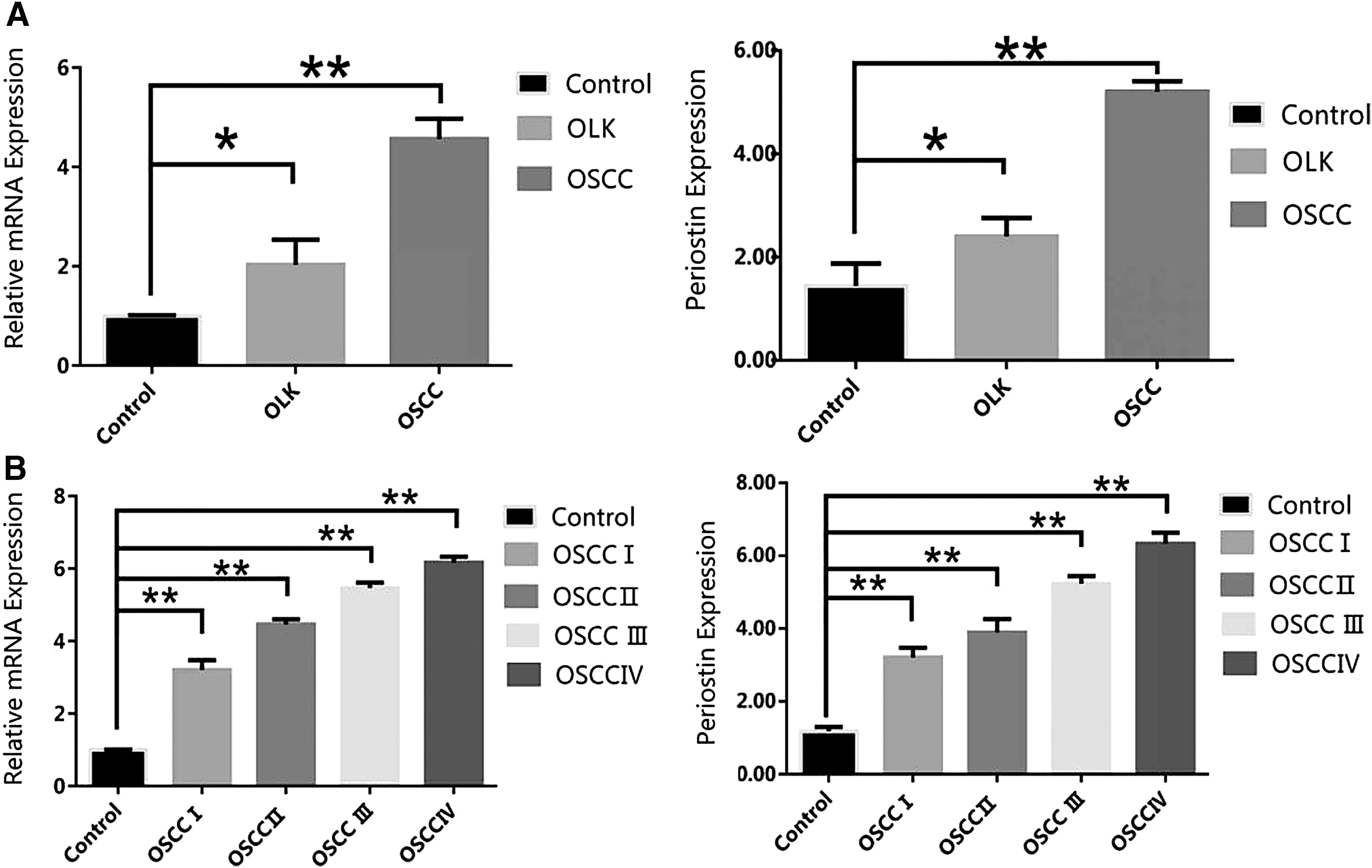
Periostin mRNA expression in different tissues. Data are presented as mean ± SEM; periostin mRNA expression in OLK and OSCC
Expression level of serum periostin in patients with OSCC and patients with OLK
Periostin concentrations in the normal healthy group, dysplastic OLK group, and OSCC group were 20.64 ± 5.3, 54.23 ± 3.8, and 81.06 ± 10.1 ng/mL, respectively. The serum periostin levels in patients with oral OLK and squamous cell carcinoma were significantly higher, when compared with those in healthy subjects (p < 0.05), which was a gradually increasing process. An increased expression of periostin in serum during the development of squamous cell carcinoma from dysplastic OLK was also found (Fig. 4).
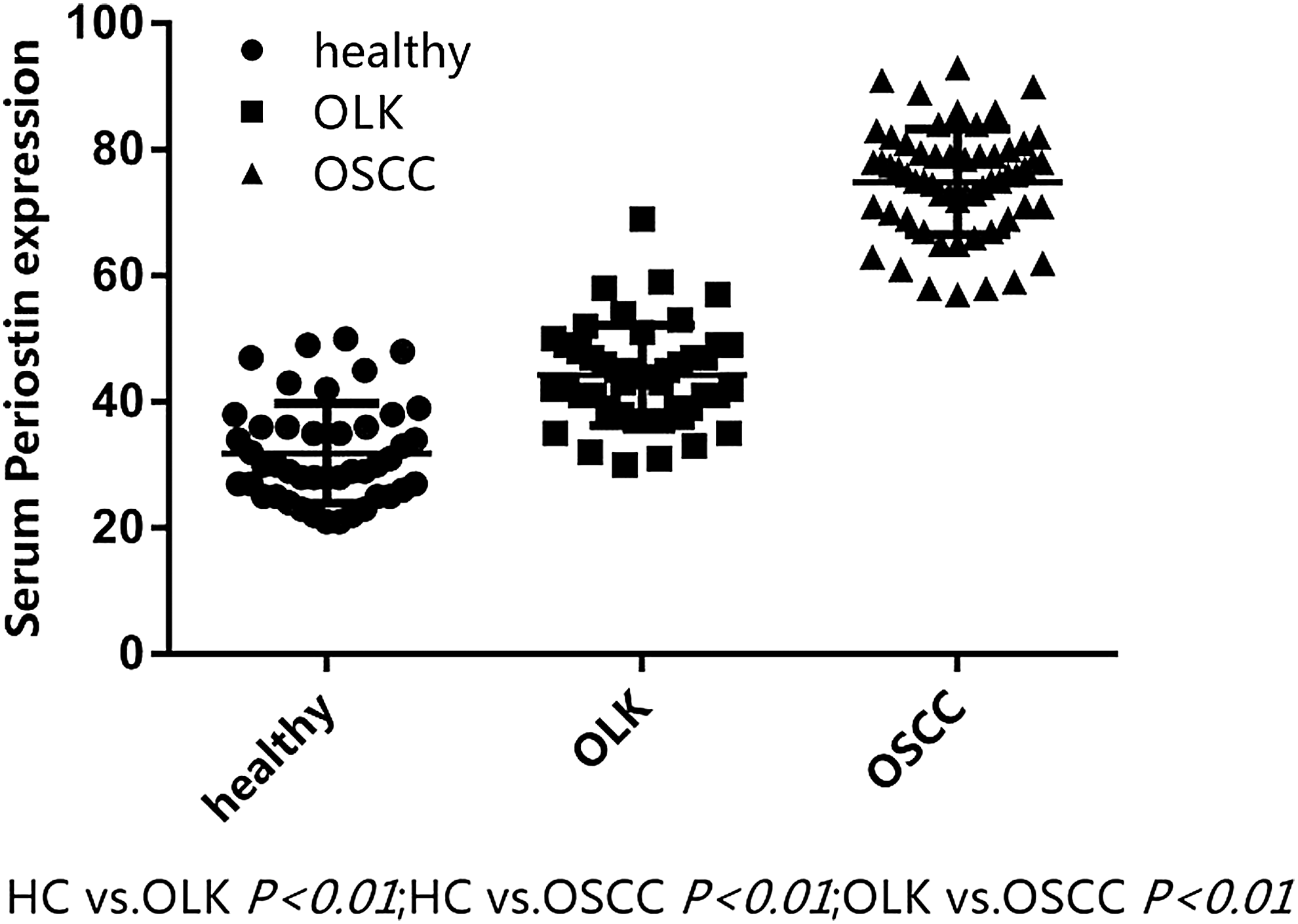
Periostin serum expression in patients with OLK and OSCC (ng/mL). Compared with normal subjects, the expression level of serum periostin protein in patients with leukoplakia and squamous cell carcinoma significantly increased. The process from leukoplakia to squamous cell carcinoma was a step-up process. OLK, oral leukoplakia; OSCC, oral squamous cell carcinoma.
The association between serum periostin expression levels and the clinical parameters of OSCC
The expression of periostin in serum in patients with OSCC was mediated using the median 68.64 ± 3.3 ng/mL as the cutoff value between the high-expression group and low-expression group. The statistical results revealed that the protein expression of periostin correlated with tumor infiltration, lymph node metastasis, and TNM staging, regardless of the patient's gender, age, smoking history, tumor location, and degree of differentiation (Table 3).
Serum Periostin Protein in Oral Squamous Cell Carcinoma of Pathological and Clinical Features of the Expression
Discussion
Oral cancer is one of the common malignant tumors of head and neck cancer. Squamous cell carcinoma is the main pathological type, 13 and its etiology and pathogenesis remain unclear, at present. The periostin gene is located on the long arm of chromosome 13, and contains a typical signal sequence and four cysteine-rich repeat domains with a C-terminal domain. It is homologous to fasciculin I, which is a protein expressed on the surface of axons in an insect's central nervous system embryo. 14 Periostin is a TGF-β-induced extracellular matrix protein that is overexpressed in various types of cancer tissues. Furthermore, it is closely correlated to a patient's prognosis, 15,16 such as in the lung, 17 brain, 18 ovary, 19 breast, 20 colon, 21 and oral cavity. 22 These reports suggest that periostin is involved in cell survival, tumor spreading, angiogenesis, invasion, and metastasis. 23 At the molecular level, periostin activates the Akt/PKB signaling pathway 24 through avβ3 or β425 integrins, to increase cell survival. The research results of the investigators were similar to the present findings. The IHC results revealed that the expression of periostin gradually increased in the histological changes of the oral mucosa to oral OLK to OSCC. The positive expressive intensity of periostin was positively correlated to the degree of malignancy (p < 0.05). This result is consistent with that reported by Dong and J.M. Brown. 26,27 At this point, periostin significantly increased in oral mucosal epithelial cells, abnormal epithelial cells, or malignant hyperplasia, indicating that periostin expression accumulated in the premalignant lesion of the oral lesion. This coincides with the theory of cell proliferation during carcinogenesis, and strongly confirms that periostin does play a role in the carcinogenesis of OSCC. Epithelial abnormalities gradually increased with the increase in periostin expression, which is consistent with a study on periostin in the gastric normal mucosa, gastric ulcer tissues, and gastric paracancerous tissues. 28 It was speculated that during this process, periostin is involved in the remodeling of the peritumoral matrix, weakening of adhesion between cells, and the regulation of epithelial cell proliferation. Epithelial cells secrete inflammatory factors, such as TGF-β, TNF-α, and FGF. These factors act on normal epithelial cells in a paracrine manner, allowing normal epithelial cells to proliferate and evolve. 29 Meanwhile, the periostin expressive intensity in OSCC tissues was significantly different from that in the oral normal mucosa and OLK group (p < 0.01). These results also revealed that periostin positive expression was significantly higher in poorly differentiated squamous cell carcinoma (p < 0.01). That is, the lower the degree of tissue differentiation, the higher the periostin expression. This indicates that periostin, to a certain extent, predicts the invasiveness and metastasis of OSCC. Furthermore, quantitative real-time PCR (qRT-PCR) results revealed that the normal oral mucosa, dysplasia tissues, squamous cell carcinoma periostin DNA amplification curve, and the normal oral mucosa in the amplification curve were not significantly different with the abnormal proliferation of leukoplakia tissue amplification curve. However, an obvious amplification curve can be observed for squamous cell carcinoma. Hence, it can be observed that periostin mRNA expression levels gradually increased from normal oral mucosa, dysplasia leukoplakia, to squamous cell carcinoma, and the difference was statistically significant (p < 0.05). The present study demonstrated that the IHC and qRT-PCR performed to detect the expression of periostin in oral mucosa could also be performed to detect oral precancerous lesions.
Furthermore, studies have found that in asthma patients who received glucocorticoid therapy, 30 serum periosteal protein was significantly reduced, lung function was improved, and eosinophils, tracheal wall thickness, and the tracheal wall area in sputum were reduced, thereby indicating that periostin in serum can be a biomarker of eosinophilic inflammation and tissue remodeling in asthma. OLK is the most common precancerous lesion in the oral cavity. In monitoring the development of OLK to OSCCs, biopsy is the gold standard, but repeated biopsy causes great pain to the patient. A number of these patients refused to undergo multiple painful biopsies, which cause them to miss the early monitoring of disease progression. A serological, relative, and meaningful tumor marker (TM) examination would be simpler with less pain. The detection of serological-related molecules in precancer lesions has been a research hotspot.
In the present study, it was found that serum periostin protein levels were significantly high (81.06 ± 10.1 ng/mL) in patients with OSCC, and this was significantly higher than those in oral OLK (54.23 ± 3.8 ng/mL) or healthy controls (28.64 ± 5.3 ng/mL). These data enhance the diagnostic value of periostin protein in OSCC. Detecting the protein expression of periostin in the serum of patients with precancerous OLK may help in screening and identifying potential high-risk OSCC patients.
Tumor metastasis is not only correlated to tumor cell invasion and metastasis but also dependent on the target organ tissue microenvironment. However, the metastasis only forms when the target organ tissue microenvironment is conducive to the attachment and survival of tumor cells. Growth factors and hydrolases involved in the extracellular matrix modification act on distant target organ interstitial cells through the circulatory system. In particular, fibroblast plays a key role in this mechanism. It maintains the tumor microenvironment of target organs by releasing extracellular matrix proteins, such as periostin and tenascin-C, into the tissue microenvironment, promoting the formation and growth of metastatic carcinomas. 31,32 Periostin is a major extracellular matrix protein and its mechanism of regulating the tumor microenvironment remains unclear. In the study conducted by the investigators on the clinicopathological factors of OSCC patients, it was found that periostin expression was significantly higher in OSCC patients with lymph node metastasis than in patients without lymph node metastasis. This indicates that periostin expression may correlate with the invasion and infiltration of patients with OSCC. The higher the invasion and infiltration are, the higher the periostin expression is.
In conclusion, the abnormal expression of periostin appears in the early stage of the morphological changes of oral OLK, suggesting that the increase in periostin expression may be an early event in the carcinogenesis of oral OLK. Periostin may thereby serve as a molecular biomarker for the early detection of oral OLK. Periostin expression in patients with oral OLK and OSCC is higher, when compared with normal people, and the expression of periostin in serum is correlated with the late stage and poor prognosis of OSCC. The abnormal expression of periostin may be correlated to the development and progression of OSCC, suggesting that it may also be a potential molecular target for antitumor therapy. Due to the complex biological characteristics of tumors, the antigens that these express are characterized by polymorphism. It is difficult to make a diagnosis for a disease with only one marker in serum, and accurate judgments are used to guide clinical treatment. Therefore, multiple TMs in serum should be combined to improve the accuracy and sensitivity of the diagnosis of the disease, 33,34 which needs to be further studied through more cases.
Footnotes
Acknowledgment
This work was supported by the Fujian Foundation for Medical Innovation (No: 2018-CXB-7).
Disclosure Statement
There are no existing financial conflicts.