
Abstract
Objective:
This study aims to test the treatment effect of endobronchial ultrasound (EBUS)-guided interstitial iodine-125 (125I) seed implantation for mediastinal lymph node metastasis or advanced mediastinal lung cancer.
Materials and Methods:
The patients with mediastinal lymph node metastasis or advanced mediastinal lung cancer, who had undergone surgery for resection of primary lesions and repeated chemotherapy or external radiotherapy, were selected and scheduled to undergo EBUS-guided 125I seed implantation from December 2015 to May 2017. Forty patients were included into this study. Clinical data of these patients were collected and the short-term effects were observed. Then, the feasibility for treating mediastinal tumors was retrospectively analyzed. The follow-up period ranged within 1–6 months.
Results:
The procedure was successfully completed, and all patients well tolerated the procedure without any major complications. The response evaluation criteria in solid tumors were utilized to test the treatment effect, and the overall response rates (complete remission + partial remission) at postoperative 2, 4, and 6 months were 65.00% (13/20), 80.00% (16/20), and 85.0% (17/20), respectively. All patients of this study survived throughout the follow-up period.
Conclusions:
This experience revealed that EBUS-guided 125I radioactive seed implantation is effective and safe, and is a prospective approach for treating patients with mediastinal lymph node metastasis or advanced mediastinal lung cancer.
Introduction
In recent years, with the development of nuclear medicine and the treatment planning system (TPS) for iodine-125 (125I), the advent of interstitial implant brachytherapy has been widely used in various malignant solid tumors, such as prostate cancer, pancreatic cancer, liver cancer, peripheral lung cancer, cancers of the head and neck, and other malignant tumors, and this has been proven to exhibit significant efficacy. 1 –9 To date, the treatment of 125I seed implantation has been mostly guided by computed tomography (CT). However, CT-guided percutaneous 125I implantation remains limited for mediastinal lymph node metastasis and lung cancer due to the distance of the tumor from the skin, high risk of pneumothorax, and massive hemorrhage. For mediastinal tumors, endoscopic bronchial ultrasonography-guided 125I radioactive seed implantation is a novel therapy that appears to be a good choice. 10,11 In this study, a retrospective analysis was performed for nonresectable stage III/IV mediastinal lung cancer or mediastinal lymph node metastasis patients treated with ultrasound bronchoscope-guided 125I seed implantation, and no other therapies of tumor were given after the 125I seed implantation procedure. The safety, effectiveness, and potentiality for the clinical applications of 125I seed implantation are discussed.
Materials and Methods
Forty selected patients with mediastinal lymph node metastasis or advanced mediastinal lung cancer, who had undergone surgery for resection of primary lesions and repeated chemotherapy or external radiotherapy, underwent endobronchial ultrasound (EBUS)-guided 125I seed implantation between December 2015 and May 2017. The patient population consisted of 22 males and 18 female, with a median age of 65.3 years old (range: 45–78 years old). In all patients, patients with squamous cell carcinoma accounted for 45% (n = 18), patients with adenocarcinoma accounted for 25% (n = 10), and patients with small cell lung cancer accounted for 30% (n = 12). The tumor diameter varied within 15–45 mm, with a mean diameter of 27.4 mm. All patients previously received different therapies, including surgical resection, chemotherapy, external radiotherapy, or comprehensive treatment. The tumor node metastasis (TNM) stage of the tumors was assessed according to the 7th edition of the TNM Classification of Malignant Tumors: stage III, 22 patients (27.5%) and stage IV, 18 patients (46.25%). The clinical characteristics of these patients are listed in Table 1.
Patient Demographics
TNM, tumor node metastasis.
The exclusion criteria were as follows: (1) patients with tumors that have widely spread; (2) severe malfunction of the heart, kidney, or liver; (3) cachexia; (4) a large amount of hydrothorax; and (5) unable to tolerate anesthesia. The inclusion criteria were as follows: (1) the diagnosis of lung cancer or mediastinal node metastasis confirmed by needle biopsy; (2) no contraindication for CT; (3) ability to undergo CT for 4–6 weeks after treatment during the follow-up period; (4) a Karnofsky performance scale score of 70% or greater; and (5) lack of severe unstable hematogenic parameters and active infection.
The study plan was designed according to the Consolidated Standards of Reporting Trials guidelines, and was approved by the Ethical Committee of Yinzhou People's Hospital (Yinzhou Hospital Affiliated to the Medical School of Ningbo University). Written informed consent was provided by all 40 patients participating into this study.
The implantation of radioactive 125I seeds was guided by an ultrasonic bronchoscope (Olympus Corporation). The puncture needle used was an 18G ultrasonic endoscope needle produced by Cook Company. The chest CT scan was actualized for all 40 patients to obtain information on their tumor characteristics at 1–2 weeks before brachytherapy. According to the preoperative CT images, TPS (76633QD; Beijing, China) was used to calculate the number and distribution of seeds. The TPS ensured a minimal peripheral dose of 144 Gy to the target volume. The rotatable implantation gun, implantation needle, and 125I seeds were all provided by Beijing ZHIBO Bio-Medical Technology Co., Ltd. (Beijing, China). The diameter of each seed was 0.8 mm and the length was 4.5 mm. The half-life period of each seed was 59.6 d, the mean energy was 27–35 keV, and the tissue penetration distance was 1.7 cm. The activity of the 125I seeds was 0.6–0.8 mCi.
All patients were scanned with 5 mm thin slices to measure the volume of the tumors before the procedure. Three-dimensional reconstruction was conducted, and the CT scan images were transferred to a radiotherapy planning system. The matched peripheral dose was calculated on the basis of the target volume and activity of the 125I seeds, the position of the implantation needle, and the number of seeds. The implantation procedure was performed under conscious sedation in an operating room. The echoendoscope was inserted, and the gross tumor volume (GTV) was clearly identified. The clinical target volume (CTV) was defined as GTV plus 5-mm margins in all directions. The insertions and path of the needle were determined to avoid damage to vital structures, such as coronary circulation and large vessels. According to the number and spatial distribution of particles determined by TPS before the operation, the 125I seeds were placed using an 18G ultrasonic endoscope needle under ultrasound bronchoscope guidance with the center-to-center space between seeds maintained at 0.5 cm.
All patients were well tolerated and had no complications. There was no massive hemorrhage observed at the puncture site. Perioperative prophylactic antibiotics were provided to all patients. Within 1 month, CT scan was utilized to verify the position and intensity of the 125I seeds based on the TPS. Meanwhile, more 125I seeds were implanted into radioactive insufficient tumors. After the operation, the CT images were guided to TPS for quality verification, and the eligibility criterion is at least 90% image coverage of the CTV by the prescription dose (D90).
The follow-up duration was 6 months. All patients underwent CT scans every 2 months, or earlier when new clinical symptoms appeared. The physical status of these patients and the diameter of the tumors were recorded during the follow-up period. The response evaluation criteria in solid tumors were selected to evaluate the therapeutic effect. According to the World Health Organization criteria, treatment efficacy was classified as follows: complete remission (CR), partial remission (PR), stable disease (SD), and progression disease (PD). CR+PR were defined as a treatment-related response.
All results are presented as mean ± standard deviation. Statistical analysis was performed by SPSS version 17.0 (SPSS, Chicago, IL).
Results
All patients well tolerated the brachytherapy, and no severe complications occurred, such as massive bleeding and pneumothorax. During the procedure, 1 patient presented with minimal bleeding at the puncture site. Furthermore, 3 patients had low-grade fever in 2 d, whereas 2 patients exhibited a mild decrease in white blood cell count. One patient died of hepatic metastasis and hepatic failure at the 4th month after brachytherapy, which was considered a cancer-related death. Three patients died of respiratory failure in the 6th month. Figure 1 presents the therapeutic effect of a 61-year-old patient. CR was achieved in 9 patients (22.5%), PR was achieved in 21 patients (52.5%), SD was achieved in 4 patients (10%), and progressive disease occurred in 6 patients (15%), with a local control rate (CR+PR+SD) of 85%. The 2-, 4-, and 6-month overall response rate (CR+PR) was 82.5%, 77.5%, and 75%, respectively. The results of the association analysis are summarized in Table 2.
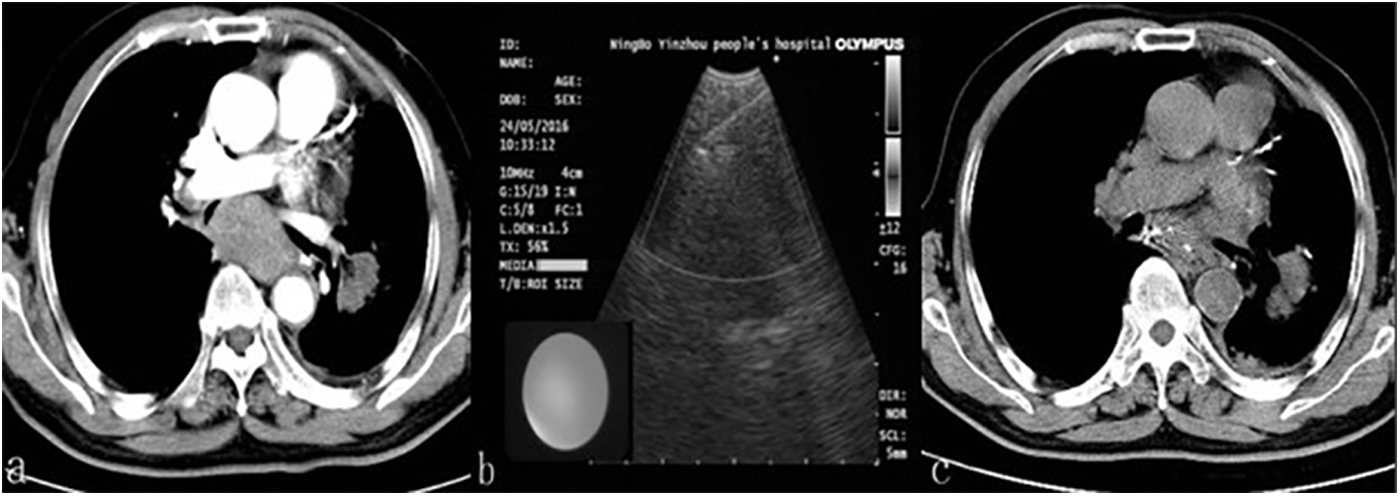
Implantation of radioactive 125I seeds in a 62-year-old male patient with mediastinal metastasis of small cell lung cancer after chemotherapy.
Clinical Efficacy of Iodine-125 Seeds Implantation in Patients
CR, complete remission; PD, progression disease; PR, partial remission; SD, stable disease.
Discussion
It has been reported that 125I radioactive seed implantation has unique advantages in the treatment of mediastinal lung cancer and mediastinal metastatic lung cancer. 12 –14 At present, CT-guided percutaneous puncture implantation remains as the most common procedure. However, due to the distance from the mediastinum to the chest wall, the percutaneous puncture needs to pass through more lung tissues, which can easily cause pneumothorax. Meanwhile, the anatomical structure in the mediastinum is complex, and some lesions are adjacent to the pericardium and large blood vessels. Hemorrhage often occurs during CT-guided percutaneous puncture implantation. Therefore, high puncture risk limits the application of 125I radioactive particles in the treatment of patients with advanced central type of lung cancer.
It is well known the endoscopic ultrasonography has been widely used in the world in recent years. Martínez-Monge et al. reported that when 125I seeds were implanted under ultrasonic gastroscopy in the treatment of patients with mediastinal metastatic tumors, the result was significant. 15 During the 10-month follow-up, the patient was well without relapse. 15 The technique of EBUS, which has been gradually popularized, is a kind of endoscopic technique that combines ultrasound imaging with bronchoscopy. The operator can accurately puncture the mediastinal mass under the guidance of ultrasound in real time, effectively avoiding the surrounding blood vessels and important organs. To date, EBUS, as a mature technique, has been widely used for the transbronchial needle aspiration of mediastinal lymph nodes or masses, which has been confirmed to be an ideal approach to make a tissue diagnosis. 16 –18 However, EBUS, as a therapeutic method, has been rarely reported at present. The major purpose of this study is to improve the treatment of 125I radioactive seed implantation by using EBUS.
In this study, 125I particles were successfully implanted in 40 patients under EBUS real-time guidance, and there were no serious complications. After the operation, the therapeutic effect was significant. As the results show, the patients who were followed up for an average duration of 6 months had 22.5% CR, 52.5% PR, 10% SD, and 15% PD. Thus, the 125I implantation treatment was effective for these patients.
EBUS-guided 125I radioactive seed implantation for the treatment of mediastinal lymph node metastasis has its unique advantages: (1) real-time ultrasound intraoperative monitoring can improve the accuracy of the localization and ideal spatial equilibrium of the distribution of particles; (2) the location of the lesion can be clearly shown and the complications of the treatment are mild; (3) there is no wound on the surface of the body with endoscopy of the bronchus; (4) it can be safely performed as a conscious sedation procedure; and (5) the cost is low and the effect is obvious in a short period of time.
The reasonable quality control of dosimetry is an important step in the course of radioactive seed implantation. 19,20 Radioactive particles need to be implanted accurately and evenly into the tumor tissue to ensure that the target area is exposed to an effective dose. At the same time, radiation damage to the surrounding normal tissue should be avoided as much as possible. A TPS should be used to formulate a reasonable implantation plan before the operation. Dosimetry verification must be immediately performed after the implantation. Blind areas should be replanted to ensure that it is in accordance with the preoperative plan.
There were a few limitations of this study. First, the operator should have skilled bronchoscope and particle implantation techniques. Second, since the location of trachea was limited, the puncture path was affected and the particle distribution was uneven, and this may have affected the therapeutic effect. Third, the sample size was small, since merely 40 patients were included into this study group. Fourth, although this study was retrospective in nature, the possibility of data bias is present. Hence, the practitioner should have rich clinical experience and be well prepared for every procedure. Large sample multicenter randomized trials need to be conducted to explore the efficacy and safety of this treatment approach in the future.
Conclusions
In summary, ultrasonic bronchoscope-guided 125I radioactive particle implantation is operable for the treatment of patients suffering lung cancer, which have received other multiple therapy modes. The short-term effect is obvious and highly safe.
Footnotes
Acknowledgment
The authors of this study thank W.Y. for remarkable technical support.
Authors' Contributions
T.X. drafted the article. W.P. played important roles in interpreting the results. W.Y. approved the final version.
Disclosure Statement
Authors have no conflict of interests and the study was not supported or funded by any drug company. I declare that no part of the article was presented in conference proceedings.
Funding Information
This study was supported by the project supported by Medical and Health Research Foundation of Zhejiang Province, China (Grant No. 2017KY615).