
Abstract
Osteosarcoma (OS) is one of the most common malignant tumors derived from mesenchymal tissue and is highly invasive, mainly in children and adolescents. Treatment of OS is mostly based on standard treatment options, including aggressive surgical resection, systemic chemotherapy, and targeted radiation therapy, but the 5-year survival rate is still low. MicroRNA (miRNA) is a highly conserved type of endogenous nonprotein-encoding RNA, about 19–25 nucleotides in length, whose transcription process is independent of other genes. Generally, miRNAs play a role in regulating cell proliferation, differentiation, apoptosis, and development by binding to the 3′ untranslated region of target mRNAs, whereby they can degrade or induce translational silencing. Although miRNAs play a regulatory role in various metabolic processes, they are not translated into proteins. Several studies have shown that miRNAs play an important role in the diagnosis, treatment, and prognosis of OS. Herein, the authors describe new advances in the diagnosis, prognosis, and treatment of miRNAs in OS.
Introduction
Osteosarcoma (OS) is one of the most common malignant tumors derived from mesenchymal tissue and is highly invasive, mainly in children and adolescents. 1 OS is mainly produced by transformed cells, which differentiate into osteoblasts and produce malignant bones. 2 Treatment of OS is mostly based on standard treatment options, including aggressive surgical resection, systemic chemotherapy, and targeted radiation therapy. Although surgical resection combined with neoadjuvant chemotherapy reduced mortality in OS patients, the 5-year survival rate was still low: 65%–70% in nonmetastatic patients and 10%–20% in metastatic patients. 3,4 Therefore, it is crucial to find new diagnostic biomarkers and therapeutic targets to achieve early diagnosis and effective treatment of the disease, especially for OS that has metastasized.
MicroRNA (miRNA), a highly conserved type of endogenous nonprotein-encoding RNA, about 19–25 nucleotides (nt) in length, 5 can degrade or induce translational silence by binding to the 3′-untranslated region (3′-UTR) of target mRNAs, thus affecting cell proliferation, differentiation, apoptosis, and ontogeny. 6 Transcription of miRNAs involves a highly conserved process that occurs independently of other genes. Notably, although miRNAs have been implicated in many metabolic processes, they are not translated into proteins. 7 Several studies have shown that miRNAs play an important role in the diagnosis, treatment, and prognosis of OS. Herein, the authors describe new advances in the diagnosis, treatment, and prognosis of miRNAs in OS.
Generation and Biological Function of miRNAs
In 1993, Lee et al. first discovered the presence of small RNAs in Caenorhabditis elegans 8 and observed that they controlled biological processes such as regulation of gene expression. 9 –11 Around the same time, Wightman et al. reported the existence of small RNAs such as lin-4. 12 Reinhart et al. found another small RNA with post-transcriptional regulation in the C. elegans: let-7. 13 With deeper research, more than 1000 miRNAs have since been discovered, each of which regulates multiple mRNAs and is involved in regulation of biological processes. 14
Production of miRNAs is a very complex biological process that includes two parts—nuclear synthesis and cytoplasmic synthesis—and requires the participation of a variety of enzymes. First, the gene encoding the miRNA is transcribed into a pri-miRNA with special hairpin structures (AAAAA and 7MGpppG) by RNA polymerase II within the nucleus. Next, pri-miRNAs are microcleaved by the nuclease Drosha (ribonuclease III) and processed into miRNA precursors of 70–80 nt with a stem ring structure, that is, pre-miRNAs. Exportin-5, a cytoplasmic transporter, transports pre-miRNAs from the nucleus into the cytoplasm with the assistance of Ran-GTP, and then the pre-miRNA is cleaved by ribonuclease III (Dicerase) into a duplex structure miRNA of about 19–23 nt. After strand separation, the passenger strand miRNA usually degrades, and the guide strand miRNA binds to AGO (argonaute) protein to form a mature miRNA. 15 There are two processes by which mature miRNAs can form an RNA-induced silencing complex: (1) when the miRNA and target gene are fully complementary, the miRNA degrades the target gene; or (2) when the miRNA and target gene are not fully complementary, the combination of miRNA and 3′-UTR inhibits translation of the target gene. 16 miRNAs are involved in several physiological processes, such as development, proliferation, differentiation, and apoptosis of normal cells, as well as in the maintenance of cellular pluripotency (Fig. 1). 10,17
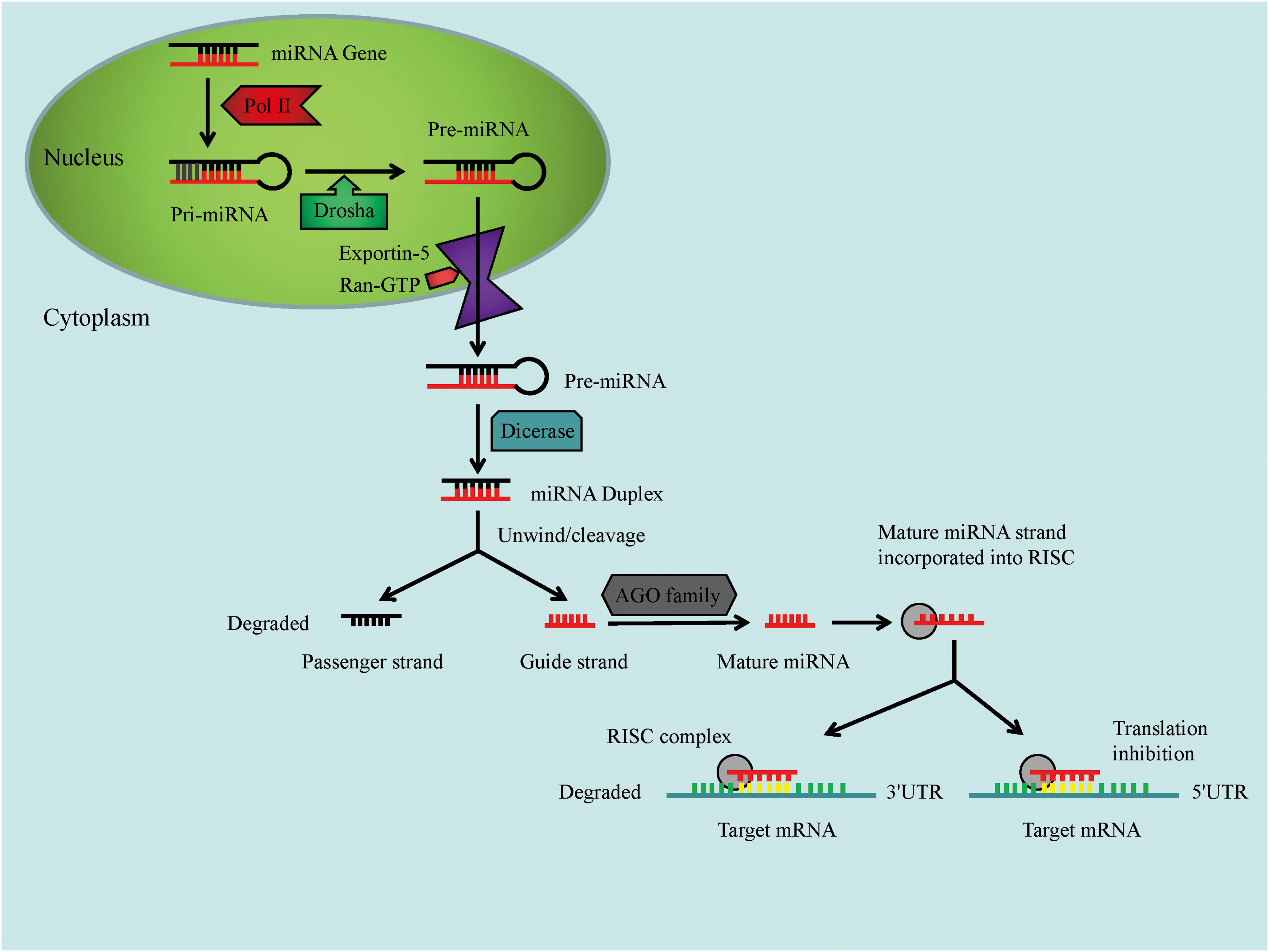
The biogenesis of microRNAs. AGO family, argonaute protein family; RISC, RNA-induced silencing complex. Color images are available online.
Relationship Between miRNAs and Tumors
In 2002, Calin et al. first described that miRNA dysregulation may be converted to chronic lymphocytic leukemia, 69% of patients with silencing of miR-15a and miR-16 expression, which is the first evidence that miRNAs are involved in the pathogenesis of tumors. 18 Subsequently, researchers began analyzing how miRNAs cause cardiovascular disease, liver fibrosis, diabetes, neurodegenerative diseases, and cancer. 19 –23 miRNAs can act as oncogenes or tumor suppressors in tumors, and the function of miRNAs is also related to the action of their target mRNAs. 23
Volinia et al. analyzed the expression profiles of miRNAs in lung cancer, prostate cancer, and gastric cancer, etc., and found that the expression of miRNA-21 was significantly upregulated. 24 Some studies have found that miRNA-21 in hepatocellular carcinoma, esophagus cancer, kidney cancer, and cervical cancer also showed overexpression status. 25 –28 Wu et al. found that in nonsmall cell lung cancer, growth and proliferation of lung cancer cells are regulated by miRNA-25 by downregulating the proapoptotic gene MOAP1 29 ; studies have found that in glioma tissues, overexpressed miRNA-25 promotes tumor growth by inhibiting the expression of cyclin-dependent kinase inhibitor 1C (CDKN1C) after the action of the source miRNA-25 is released, CDKN1C expression is upregulated and participates in normal cell cycle progression. 30 Calin and Croce found that downregulation of miR-199a expression in cervical cancer cells can inhibit cell growth, and in cholangiocarcinoma cells, downregulation of miR-141 and miR-21 can also inhibit cell growth. 31 Liu et al. found that the expression level of miRNA-144 in cancer tissues and serum samples of gastric cancer patients was significantly downregulated; serum miR-144 can accurately distinguish gastric cancer patients and healthy controls in addition to cancer tissue and the serum miR-144 level. In association with clinical stage and lymph node metastasis, 5-year overall survival and disease-free survival rates were worse in patients with low expression of miR-144 in cancer tissues and serum. 32 Li et al. showed the presence of miRNA-144-3p in patients with pancreatic cancer. The expression level in cancer tissues and PCNA-1 cell lines was significantly downregulated. 33 Therefore, further research on the anticancer or cancer-promoting effects of different miRNAs in tumor tissues can provide new ideas for clinical diagnosis, prognosis, and biotherapy of tumors.
The Role of miRNA in Diagnosis and Prognosis of OS
OS is a highly malignant and metastatic tumor. Timely and correct diagnosis is key to successful treatment of the disease and also an important guarantee for prognosis and improvement of patient survival. 34 Based on the study of the function of miRNAs in diseases, scientists have realized that these small molecules can be used as biomarkers for diagnosing diseases and prognosis.
It has been reported that miRNAs exist in serum and bone tissue, which can provide a basis for the diagnosis and monitoring of changes in the condition of patients with OS by qualitative and quantitative analysis of miRNAs in the blood circulation system and bone tissue. 35 –37
Cong et al. found that miR-124 was significantly reduced in serum in patients with advanced or distant metastasis of OS, and patients with OS with lower serum miR-124 levels had lower 5-year overall survival and disease-free survival rates. Serum miR-124 is a valuable biomarker for the diagnosis and prognosis of OS. 38 Studies have shown that the expression of miR-221 in OS patients is significantly higher than the corresponding noncancerous tissues; miR-221 overexpression is significantly associated with tumor stage, metastatic state, and response to chemotherapy pretreatment; and miR-221 can be used as a novel marker for OS staging, tumor metastasis and prognosis. 39 Yao et al. found that miR-101 was significantly underexpressed in serum samples from patients with OS. After treatment, serum miR-101 expression was significantly higher than before treatment; serum miR-101 low expression and advanced clinical stage and distant metastasis positively correlated, and serum miR-101 may be a useful biomarker for clinical diagnosis and prognosis of OS. 40 Liu et al. found that the expression of serum miR-375 in OS patients was significantly lower than that in healthy people by analyzing serum samples from 95 patients with OS and 95 healthy individuals. Low serum miR-375 levels are associated with advanced clinical stage, tumor size, distant metastasis, and adverse effects on preoperative chemotherapy. Serum miR-375 can be used as a biomarker for OS diagnosis, prognosis, and chemosensitivity prediction. 41 A recent study showed that 15 miRNAs were differentially expressed in OS patients compared with healthy controls, and further studies confirmed that miR-215-5p and miR-642a-5p are overexpressed in serum of OS patients and these two miRNAs can be used as potential markers for the diagnosis of OS. 42 Huang et al. found that miR-487a, miR-493-5p, miR-501-3p, and miR-502-5p are upregulated in peripheral blood of patients with OS and they can be used as novel, potential diagnostic biomarkers for OS. 43
Zhao et al. found that miR-21, miR-221, and miR-106a are upregulated in OS tissues, while miR-143 is downregulated, and their differential expression is associated with pathological stage, tumor grade, and lung metastasis. Therefore, the levels of these miRNAs can serve as potential biomarkers for early diagnosis of OS and can be used as potential therapeutic targets. 44 Another study confirmed that miR-663a is significantly elevated in tissues and plasma of OS patients and miR-663a can be used to diagnose new potential biomarkers of OS. 45
These differentially expressed miRNAs in the serum and bone tissues of OS patients provide a new basis for early diagnosis, prognosis, and targeted therapy of OS.
The Role of miRNA in Treatment of OS
Treatment of OS is mostly based on standard treatment options, including aggressive surgical resection, systemic chemotherapy, and targeted radiation therapy. Studies have shown that miRNA is related to the chemosensitivity and chemical resistance of OS. 46 It has also been reported that miRNA is involved in the antiradiation of OS and reduces the sensitivity of radiotherapy. 47 Therefore, it is especially important to reduce the chemical resistance of OS and improve its sensitivity to chemotherapy and radiotherapy.
Yang et al. found that miR-328-3p is downregulated in HOS-2R cells by in vivo and in vitro studies, and overexpression of miR-328-3p enhances the radiosensitivity of OS cells and miR-328-3p enhances irradiation-induced inhibition of proliferation and promotion of apoptosis in OS cells. The study also found that histone H2AX is a direct target of miR-328-3p; miR-328-3p enhances the radiosensitization of OS after X-ray irradiation and it was determined that it directly targets H2AX to modulate radiosensitization. 48 It has been reported that miR-513a-5p is downregulated in OS, and overexpression of miR-513a-5p can make cells sensitive to ionizing radiation. Human depurination/depyrimidine endonuclease/redox effector 1 (APE1) is its direct target. miR-513a-5p negatively regulates APE1, and decreased expression of APE1 enhances radiosensitivity and induces apoptosis. 49
Adjuvant chemotherapy based on cisplatin (Cis), doxorubicin (Dox), methotrexate (Met), and doxorubicin (Adr) is another treatment for OS. Similar to radiotherapy, many OS patients begin to exhibit chemical resistance to chemotherapy. Therefore, scientists have begun to study the causes of this phenomenon and the role of miRNAs in sensitivity of OS chemotherapy drugs.
Zhang et al. found that miR-19a-3p was overexpressed in OS and the tumor suppressor PTEN was its direct target. During cisplatin treatment, downregulation of miR-19a-3p increased PTEN expression and inhibition of cell proliferation, promoted apoptosis, and enhanced the chemical sensitivity of OS cells to cisplatin. 50 Studies have shown that miR-92a inhibits the growth and migration of OS cells by targeting Notch1 and enhances the sensitivity of OS cells to cisplatin. 51 Li et al. showed that miR-34a inhibits OS cell proliferation and induces apoptosis by upregulating c-Myc and Bim pathways and increases sensitivity of OS cells to cisplatin. 52 Recent studies have found that miR-29 family expression decreased in OS cells, and overexpression of miR-29abc can inhibit COL3A1 or MCL1, reduce the chemical resistance of OS cells to MTX, and promote apoptosis. COL3A1 and MCL1 are direct targets of the miR-29 family. 53 Long and Lin found that miR-590 can target p53 and enhance the effect of Dox on OS cell proliferation inhibition and apoptosis through the miR-590/WIP1/ATM-p53 signaling pathway. 54 It has been shown that overexpression of miR-340 inhibits OS cell viability, promotes apoptosis, and reduces the chemical resistance of OS cells to cisplatin by targeting ZEB1. 55 Studies have shown that after treatment of OS cells with doxorubicin and cisplatin, miR-140-5p expression increased and targeted inositol 1,4,5-triphosphate kinase 2 (IP3k2), stimulated autophagy, inhibited cell survival, and reduced chemical resistance (Table 1). 56
Roles of miRNAs in Radiotherapy and Chemotherapy in Osteosarcoma
Cis, cisplatin; Dox, doxorubicin; Met, methotrexate; Adr, adriamycin; H2AX, histone H2AX; APE1, apurinic/apyrimidinic endonuclease 1; PTEN, phosphatase and tensin homolog deleted on chromosome 10; Notch1, Notch1 signaling pathway; c-Myc, a proto-oncogene; Bim, Bcl-2 interacting mediator of cell death; COL3A1, collagen III alpha-1 chain; MCL1, myeloid cell leukemia-1; p53, a tumor suppressor gene; ZEB1, zinc finger enhancer-binding protein 1; IP3K2, 1,4,5-trisphosphate kinase 2.
Taken together, these studies have found that miRNAs are involved in the sensitivity of OS cells to several therapeutic agents, with the ultimate goal of understanding which molecular mechanisms confer chemical resistance to treatment and determining which miRNAs may be biomarkers of chemical resistance to develop new therapies based on increased sensitivity to chemotherapy and radiotherapy.
Based on the study of the function of miRNAs in disease, scientists have realized that these small molecules can be used not only as biomarkers for diagnosing diseases and prognosis but also as targets for development of new therapies.
In all kinds of tumors, the tumorigenic miR-21 is abnormally expressed, which can negatively regulate the phosphatase and tensin homolog deleted on chromosome ten (PTEN) and apoptosis protein 4 (PDC4), which in turn induces tumor cell growth, migration, invasion, and metastasis. 16 Studies have shown that miR-21 is considered a marker for many diseases and is upregulated in many cancers, including OS. In addition, it plays a major role in cell proliferation, migration, invasion, and apoptosis. 57 Inhibition of miR-21 expression delays progression of OS and is an excellent tool for treating diseases. 57 Ziyan et al. showed that miR-21 was significantly overexpressed in OS tissues; knocking out miR-21 can greatly reduce cell invasion and migration of the OS cell line MG-63; and RECK (a protein rich in reversal-inducing cysteine with a kazal motif) is a direct target of miR-21. 58 Another study also confirmed that knockdown of miRNA-21 inhibits OS cell proliferation by targeting PTEN and regulating the transforming growth factor-β1 signaling pathway. 59 MiR-21 can be a potential target for the treatment of OS.
Liu et al. found that miR-29 is highly expressed in OS, and overexpression of miR-29 promotes OS cell proliferation. PTEN is a direct target of miR-29, and PTEN overexpression inhibits proliferation and migration of OS cells and can attenuate the promotion of miR-29 on OS progression, suggesting that the miR-29/PTEN pathway is a potential therapeutic target for treatment of OS. 60 Studies have shown that miR-590-3p overexpression can inhibit U2OS cell viability, and miR-590-3p mimic transfection can inhibit the expression of PCNA, cyclin D1, and CDK4 and increase the expression of p53 and p21 and inhibition of OS cell proliferation. The study also found that SOX9 is a potential target of miR-590-3p, SOX9 is upregulated in OS, and miR-590-3p mimic transfection significantly inhibits the expression of SOX9 mRNA and protein levels. 61 Wu et al. found that miRNA-25-3p overexpression significantly inhibited proliferation, migration, and invasion of OS cells in vitro, and SOX4 is a direct target gene of miRNA-25-3p. miRNA-25-3p may act as a tumor suppressor by targeting SOX4 expression in bone tissue and thus miRNA-25-3p may have potential as a new therapeutic target for treatment of OS patients. 62 It has been reported that overexpression of miR-33b inhibited U2OS cell proliferation and anaerobic glycolysis; lactate dehydrogenase-A (LDHA) is a direct target of miR-33b in OS tissues and cells; LDHA low expression significantly inhibited glycolysis and cell proliferation in OS cells; and LDHA mRNA and miR-33b were significantly negatively correlated in OS tumors. This study revealed that miR-33b inhibits OS cells by directly targeting LDHA. Proliferation and the miR-33b/glycolysis/LDHA axis can help develop therapeutic antitumor agents for OS. 63 Studies have shown that miR-338-3p acts as a tumor suppressor in OS cells by targeting runt-related transcription factor 2 (RUNX2) and cyclin-dependent kinase 4 (CDK4) and inhibiting the MAPK pathway (Fig. 2). 64
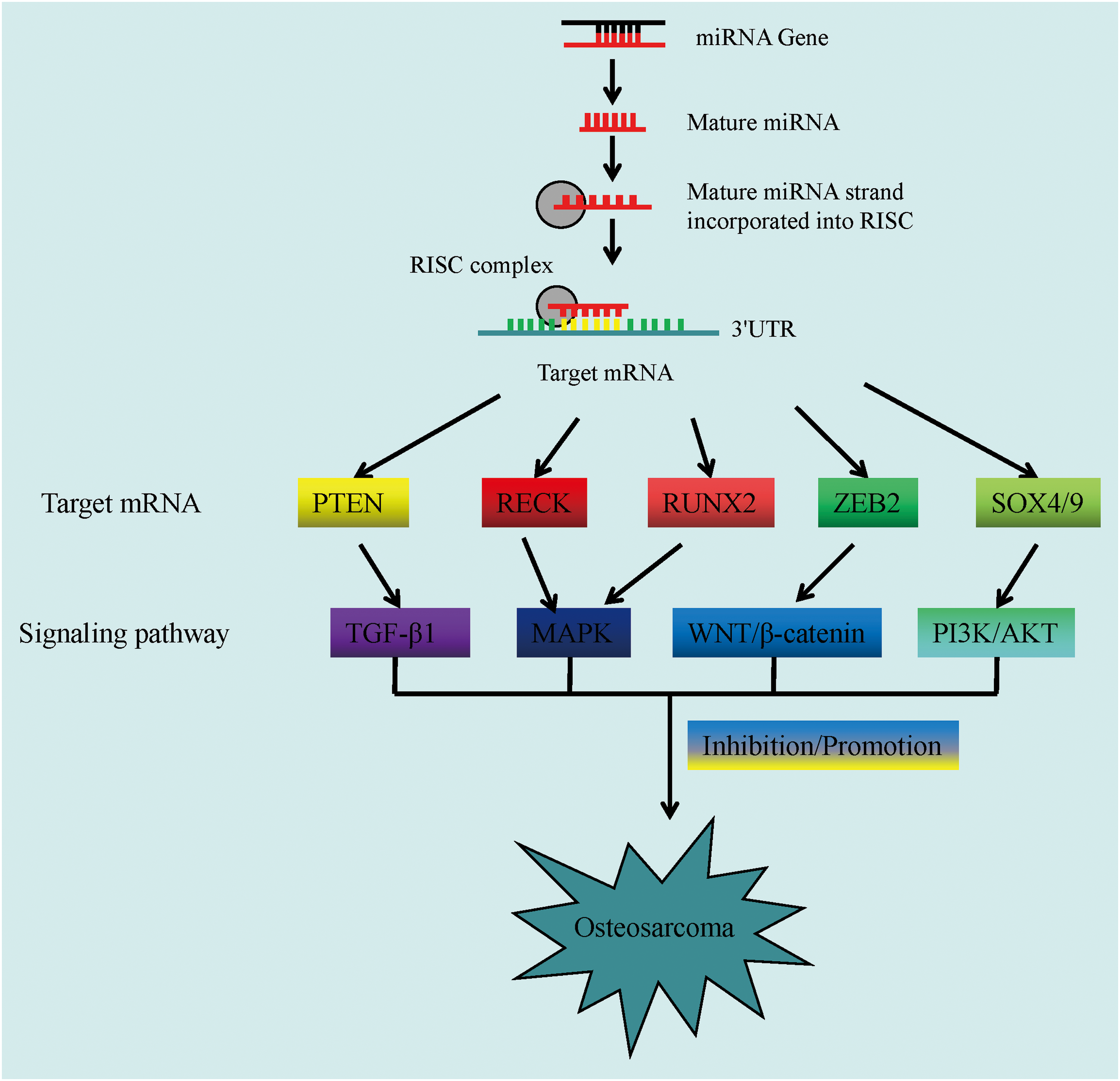
The role of microRNAs in osteosarcoma cells. PTEN, gene of phosphatase and tensin homolog deleted on chromosome 10; RECK, a protein rich in reversal-inducing cysteine with a kazal motif; RUNX2, runt-related transcription factor 2; ZEB2, zinc finger E-box-binding homeobox 2; SOX4/9, SRY-box transcription factor 4/9; TGF-β1, transforming growth factor-β1; MAPK, mitogen-activated protein kinase; WNT/β-catenin, Wnt gene/β-catenin; PI3K/AKT, phosphatidylinositol-3-kinase/serine/threonine kinase AKT. Color images available online.
In recent years, in addition to surgery, chemotherapy, and radiotherapy, the comprehensive treatment of OS includes molecular targeted therapy, immunotherapy, gene therapy, embolization, radiofrequency ablation, and stem cell therapy.
At present, the research results of OS immunotherapy mainly include dendritic cell (DC) therapy and cytokine therapy. With the deepening of research, immunological checkpoints that block tumor growth and chimeric antigen receptor T (CAR-T) cellular immunotherapy are also research hotspots. Fang et al. produced the DC-osteosarcoma fusion (DOF) tumor vaccine by electrofusion of bone marrow-derived DCs with the rat OS cell line UMR106 and injected it into a rat OS model. It was found that the DOF vaccine can effectively stimulate T lymphocyte proliferation and induce tumor cytotoxic activity of cytotoxic T cells (CTL), resulting in tumor atrophy or disappearance. 65 Cytokines participate in regulation of various cellular physiology and immune response functions by inducing the body to synthesize and secrete small molecular peptides. It has been reported that the combination of IL-2 and NK cells in a mouse model of human OS lung metastasis is more effective in the treatment of OS lung metastasis and local organ infiltration is stronger and systemic toxicity is lower. 66 In clinical applications, Meazza et al. treated patients with primary pulmonary metastatic OS with chemotherapy and IL-2, and results confirmed that IL-2-related immunotherapy has a potential role in improving patient survival. 67 Interferon is used earlier in the treatment of cancer and studies have shown that it can achieve the purpose of treating OS by enhancing the sensitivity of chemotherapy drugs. 68,69 TNF can be divided into TNF-α and TNF-β according to the source, both of which can participate in immune regulation and kill tumor cells. Gamie et al. reported that TNF-related apoptosis-inducing ligand (TRAIL) can induce apoptosis in cancer cells, showing low- and medium-efficiency effects in the treatment of OS. 70 It has been found that miRNA-138 overexpression inhibits TNF-α-induced protein 8 (TNFAIP8) production, which in turn inhibits OS cell proliferation and induces apoptosis. 71
OS is caused by changes in the process of differentiation into bone after mesenchymal stem cells are influenced by genetic or other factors. Mesenchymal stem cells have the ability to transform into tumor stem cells (TSCs), which bridges the gap between TSCs and OS. 72 TSC is closely associated with tumorigenesis, proliferation, recurrence, and chemoresistance. 73 Therefore, TSC treatment of OS solves the problem of recurrence and metastasis of OS from the source. Li et al. confirmed that TSCs in a hypoxic environment promote the formation of metastatic tumors by increasing the expression of hypoxia-inducible factors and activating lysyl oxidase. Changing the TSC survival microenvironment opens up another avenue for treatment of OS. Introduction of the TSC theory has pushed diversification of OS treatment methods to new heights (Fig. 3). 74
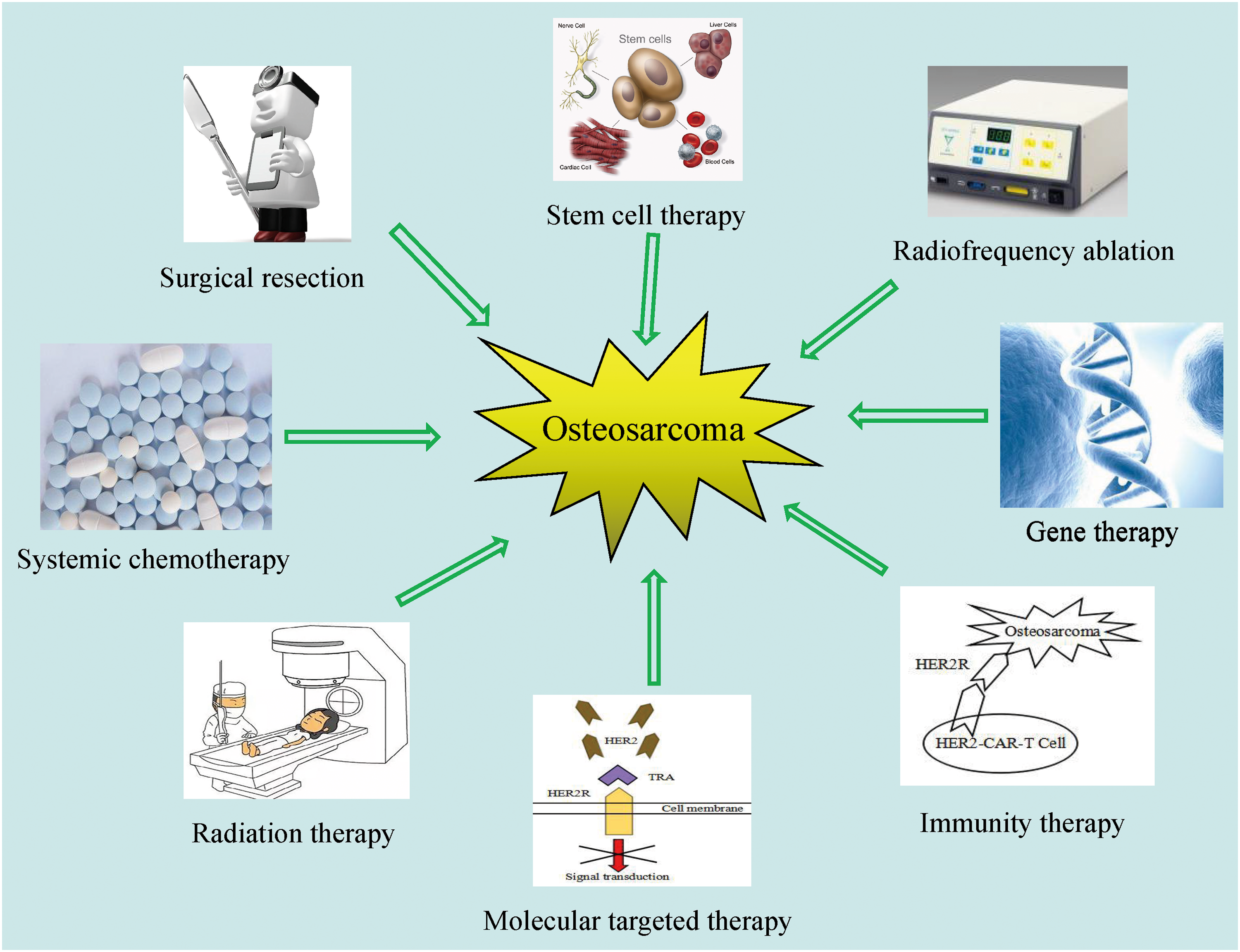
Treatments of osteosarcoma, including surgical resection, systemic chemotherapy, radiation therapy, molecular targeted therapy, immunotherapy, gene therapy, radiofrequency ablation, and stem cell therapy. Color images available online.
Future Directions and Clinical Significance
With the deepening of miRNA research, a better understanding of miRNA biogenesis and function will certainly accelerate development of miRNA-based targeted therapies. The miRNA effect is mainly caused by post-translational inhibition or degradation of the target by miRNA-mRNA 3′-UTR interaction, so it is important to identify the optimal miRNA candidate or mRNA target for each disease type and prevent off-target effects. 75
miRNA targets can be more accurately identified by using miRNA and mRNA data in the Cancer Genome and Proteomics Data (TCGA) public repository and the miR-CLIP seq technology to prevent off-target effects. Another challenge in miRNA-targeted therapy is the design of miRNA delivery vectors. Conventional vectors have low bioavailability; poor cell uptake, resulting in poor delivery efficiency; and include off-target effects and potential toxicity problems. Recent, new miRNA vectors can be used to overcome these problems, such as nanoparticles and polymers, lipid carriers, and adeno-associated viruses. It is well known that OS has high chemical resistance to chemotherapeutic drugs. In vitro and in vivo studies have shown that certain miRNAs can increase the chemosensitivity of cancer cells. The mimics of these miRNAs can be combined with chemotherapeutic drugs to improve the chemosensitivity of OS. 76,77
In summary, miRNA-based, molecular targeted therapy is the future direction of development; identifying the best miRNA and target mRNA, developing a safe and efficient delivery system, and improving the chemosensitivity of OS are the focus areas of future research. The ultimate goal is to apply the research results of miRNAs to the clinic, improve the sensitivity of OS to chemotherapeutic drugs, and use these targets to develop antitumor drugs to improve the survival rate of OS patients.
Conclusions
In summary, since the discovery of miRNAs, researchers around the world have begun to study the role of these small molecules in human cancer. miRNAs have been used as biomarkers for the diagnosis, metastasis, and prognosis of many cancers. For rare and aggressive cancers (e.g., OS), miRNAs offer a novel therapeutic approach that will focus on inhibiting miRNAs or inducing expression of tumor suppressor miRNAs.
Obviously, the association between miRNAs and OS has achieved unprecedented success, but more in-depth research is needed to solve current challenging problems, such as identifying standardized protocols for detecting miRNAs and establishing ideal in vivo delivery systems to regulate the expression of miRNAs. There are still some problems in the clinical application and promotion of new therapies: lack of clear indications and contraindications; and the introduction and response mechanisms of adverse effects have not been perfected. The ultimate goal is to apply results of miRNA research to the clinic and use these targets to develop antitumor drugs.
Authors' Contributions
J.W. and S.Z. drafted the manuscript and revised the manuscript. S.L., J.S., H.L., and Z.Y. contributed to manuscript conception. S.W., K.D., X.P., and J.L. provided the financial support. All coauthors have reviewed and approved the manuscript before submission.
Footnotes
Acknowledgment
The authors thank Professor Zhi Yi for his careful guidance in the process of writing articles and also thank him for his understanding and support.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Shaanxi Provincial Science and Technology Department (2018ZDXM-SF-054).