
Abstract
Background:
M5A is a humanized monoclonal antibody (mAb) directed against carcinoembryonic antigen (CEA) The purpose of this first in human phase I dose-escalation trial was to characterize the toxicities and determine the maximum tolerated dose (MTD) of yttrium-90 (90Y)-DOTA-M5A as a single agent and in combination with gemcitabine (gem).
Methods:
Patients with advanced metastatic CEA-producing malignancies who had progressed on standard therapies were first administered indium-111 (111In)-DOTA-M5A. If tumor targeting was observed, the patient then received the therapy dose of 90Y-DOTA-M5A. Serial scans, blood sampling, and 24 h urine collections were then performed to estimate radiation doses to organs and total body. Assays for human antihuman antibody (HAHA) responses were performed out to 6 months.
Results:
Of the 18 patients who received 111In-DOTA-M5A, 16 received 90Y-DOTA-M5A therapy; 1 patient at 14 mCi/m2 with gem (150 mg/m2 days 1and 3), 3 patients at 12 mCi/m2 with gem, 6 patients at 12 mCi/m2 without gem, and 6 at 10 mCi/m2 without gem. Prolonged cytopenias resulted in discontinuation of dose escalation with gemcitabine. A single agent MTD of 10 mCi/m2 was established based on dose-limiting hematopoietic toxicities. HAHA immune response was identified in 2 of 16 patients (12.5%). Stable disease at 3 months was seen in 10 patients and 2 patients demonstrated an 88% and 64% decrease in CEA back to normal levels. In 2 patients 111In-DOTA-M5A imaging revealed previously unknown brain metastases.
Conclusion:
This study demonstrates the potential utility of the 90Y-DOTA-M5A anti-CEA mAb as a therapeutic antibody. There is decreased immunogenicity compared with murine and chimeric mAbs, allowing for the potential of multiple administrations. Combined modality therapy approaches incorporating this agent should continue to be evaluated.
Introduction
Radioimmunotherapy (RIT), defined as the use of radiolabeled antibodies to specifically target therapeutic doses of radiation to tumor, offers a theoretically attractive delivery system for systemic-guided radiation therapy. Objective responses have been observed primarily in radiosensitive hematologic malignancies. 1,2 Radiolabeled antibodies have been successful in targeting comparable radiation doses with solid tumors as lymphomas, with estimated tumor doses capable of two to three log kill in solid tumors. However, objective responses have been limited when RIT is used as monotherapy due to the relative lack of radiosensitivity of these cancers. As a result trials have evaluated adding RIT to established single agent and multiagent chemotherapy regimens 3 –5 and more recently with other systemic therapies such as immunotherapy and biologic therapies. 6,7
At this institution an IgG1 murine monoclonal antibody (mAb) designated mT84.66 was developed with a high specificity and affinity (∼2 × 1010 M−1) for carcinoembryonic antigen (CEA). 8 The antibody has been conjugated to diethylenetriaminepentaacetic acid (DTPA) or tetraazacyclodocecane-tetraacetic acid (DOTA) and radiolabeled for clinical studies. Indium-111 (111In)-DTPA-mT84.66 demonstrated successful targeting and imaging of colorectal cancer. 9 The antibody was engineered to reduce immunogenicity by humanizing the nonantigen binding constant domains of the antibody creating a human/murine chimeric version, designated as chimeric T84.66 (cT84.66) mAb. A pretherapy imaging trial evaluating 111In-DTPA-cT84.66 demonstrated tumor targeting and minimal toxicity of the antibody. 10 A subsequent phase I trial of yttrium-90 (90Y)-DTPA-cT84.66 established a maximum tolerated dose (MTD) of 16.6 mCi/m2 with myelosuppression being dose limiting. 11 Thirteen of 22 (59%) developed a human antichimeric antibody (HACA) response, limiting the number of additional cycles of RIT. In a subsequent phase I trial with 90Y-DOTA-cT84.66, 12 dose-limiting hematologic toxicity was observed and an MTD of 13.4 mCi/m2 was established. Eight of 13 patients (62%) developed a HACA response preventing subsequent therapy cycles in 4 patients. Subsequent phase I trials demonstrated the feasibility of combining radiosensitizing single agent chemotherapy with 90Y-DOTA-cT84.66 RIT at 16.6 mCi/m2 with 1000 mg/(m2·d) 5-fluorouracil (5-FU) given as a 5-d continuous infusion 3 or with gemcitabine at 150 mg/m2 given on days 1 and 3 after RIT. 4
To further reduce immunogenicity of cT84.66 mAb a humanized version was engineered and designated hT4.66-M5A (M5A) mAb. A phase I trial of 90Y-DOTA-M5A anti-CEA RIT was then carried out to evaluate the immunogenicity of M5A and to determine the MTD and associated dose-limiting toxicities (DLTs), initially in combination with gemcitabine and then as a single agent.
Materials and Methods
Antibody production and conjugation
The hT84.66-M5A (M5A) mAb is a humanized IgG1 mAb derived from the murineT84.66 mAb by CDR grafting based on structure design. 13 The M5A mAb was expressed, purified, and conjugated to the macrocyclic chelate 1,4,7,10-tetraazacylcodecane-N, N′,N,″N′″-tetraacetic acid (DOTA) at the City of Hope Center for Biologics and Genetics under cGMP regulations in accordance with FDA Investigational New Drug application. The antibody was labeled with 111In and 90Y to form the imaging or therapeutic agent, respectively. 12
Clinical trial design
The primary objective of this trial was to establish the MTD of 90Y-DOTA-M5A humanized anti-CEA antibody and to characterize associated toxicities initially in combination with gemcitabine and then as a single agent. Patients with advanced chemotherapy refractory metastatic CEA producing malignancies for which no standard therapies were available were eligible. Patients were required to have at least one measurable site of disease. Patients with untreated brain metastases were excluded. CEA expression was documented by either an elevated serum CEA level or positive immunohistochemistry. Other eligibility criteria included measurable disease; Karnofsky performance status of ≥60%; no therapy in the 4 weeks before study entry; adequate bone marrow function as defined by WBC ≥4000/μL, absolute neutrophil count ≥1500/μL, and platelet count ≥125,000/μL; creatinine <1.5 mg/dL or creatinine clearance >60 cc/min; bilirubin ≤1.5 mg/dL; and liver transaminases no greater than two times the upper limit of normal. This study was reviewed and approved by the City of Hope Institutional Review Board (IRB) and all patients were consented to the study.
Before treatment, each patient received 5 mCi/5 mg 111In-DOTA-M5A infused intravenously for 25 min. This was followed by planar γ camera imaging at 1–3 h, 1 d, 2 d, 3–5 d, and 6–7 d postinfusion. Single photon emission computed tomography imaging was also performed at 2 and 3–5 d postinfusion. Serial blood samples were collected at ∼0, 1, and 4–6 h as well as in conjunction with the 2, 3–5, and 6–7 d scans. Round-the-clock urine collections were performed for five consecutive days beginning immediately after infusion.
Patients went on to receive the planned therapy dose of 90Y-DOTA-M5A, if antibody imaging of at least one known tumor site was observed. The therapy dose was administered no more than 2 weeks after the 111In-DOTA-M5A antibody infusion. The infusion of 90Y-DOTA-M5A RIT included 5 mCi of 111In-DOTA-M5A. The total amount of antibody protein infused was kept constant at 5 mg. As in prior studies, to minimize any free 90Y targeting to bone (thus increasing bone marrow toxicity) patients received a Ca-DTPA infusions after 90Y-DOTA-M5A administration at a dose of 250 mg/(m2 per 24 h) for 3 d given in equally divided doses every 12 h. Serial γ camera scans, blood sampling, and urine collections were performed at the same time points as for the pretherapy infusion. If no DLTs were observed and toxicities returned to grade 1 or less, a second cycle of 90Y-DOTA-M5A was delivered 6–10 weeks later. A maximum of two therapy cycles were allowed on study. Blood samples were also collected before each therapy cycle and at 3 and 6 months after RIT completion to assess for human antihuman antibody (HAHA) response using a method previously described. 14 Initially, for the first two cohorts, gemcitabine was given on days 1 and 3 at 150 mg/m2; however, on subsequent cohorts only the single agent 90Y-DOTA-M5A was delivered.
Following a standard phase I dose escalation design, 3–6 patients were entered per dose level. The MTD was defined as the highest dose level at which <33% of patients at that dose level experienced DLTs. DLT in a given patient was defined as any grade 3 nonhematologic toxicity or any grade 4 toxicity hematologic or nonhematologic toxicity related to the study drug. DLT was based on the first course of treatment. Toxicity was graded according to the NCI common toxicity criteria version 3.0.
Radiologic studies, including computed tomography (CT) scans, were repeated at 5–6 weeks post-therapy to assess tumor response. Response evaluation criteria in solid tumors were used. Response criteria were defined as follows: complete response: disappearance of all measurable and evaluable disease and no new lesions; partial response: at least a 30% decrease in the sum of the longest diameter (LD) of all measurable lesions, with no progression of evaluable disease and development of new lesions; stable disease: does not qualify for complete response, partial response, or progression; progressive disease: at least a 20% increase in the sum of LD of all measurable lesions or the appearance of one or more new lesions. Response endpoints also included overall survival (OS) and progression-free survival (PFS).
Pharmacokinetic analysis and absorbed dose estimates
Biodistributions and radiation doses for 90Y-DOTA-M5A were estimated based on the measured pharmacokinetics of 111In-DOTA-M5A, corrected for the difference in physical decay rates for the two radionuclides. Blood and urine samples were assayed for 111In activity with a γ counter. Samples containing both 111In and 90Y were counted sequentially in γ and β well counters. In the latter case, Cerenkov radiation was used, with quench correction, to determine the amount of 90Y present. Samples were homogenized in aqueous media and bleached before counting. Standards were used to calibrate the absolute accuracy of the counting systems.
Biodistributions of 111In-DOTA-M5A were determined by planar γ camera imaging. For features seen in both projections, 111In activity was estimated as a function of time using nonoverlapping regions of interest drawn on the geometric mean of parallel-opposed images. Otherwise, single-view images were used to estimate region of interest activity versus time. Image-derived 111In fraction of injected activity curves [FIA(t) = total activity content/injected activity] were determined for kidneys, spleen, liver, whole body, and whole body remainder (i.e., whole body minus measured organs). Organ FIAs (which included activity in blood contents) were corrected for background counts, counts from overlying tissue (estimated from thigh muscle), and photon attenuation in tissue. Corrections for attenuation and overlying activity employed measurements of body and organ thicknesses obtained from patients' CT scans. Attenuation coefficients were derived from experiments that determined γ camera counting efficiency for a planar 111In phantom source as a function of tissue-equivalent absorber thickness. Image-derived whole body FIAs (also corrected for background counts) were evaluated assuming that no activity was excreted until after the first imaging time point. 111In whole body and liver FIAs, as well as directly measured urine FIAs and blood activity concentrations versus time, were used as inputs for a five compartment modeling analysis to estimate mutually consistent FIAs and residence times (i.e., time-integrated FIA curves) for 90Y in blood, urine, liver, and whole body. 10 FIAs and residence times for red marrow were estimated based on the model-derived FIAs for blood. 15 Residence times for 90Y-DOTA-M5A in kidneys, spleen, and whole body remainder were calculated from the image-derived 90Y-decayed FIAs. Residence times for 90Y-DOTA-M5A were input to OLINDA/EXM v.1.0 16 and used in conjunction with OLINDA's male and female numerical phantoms to calculate tissue, organ, and total body absorbed doses.
Results
Eighteen patients with CEA producing malignancies were enrolled and received a pretherapy infusion on 111In-DOTA-M5A. Median age was 67.5 years (49–78). Two patients with colon cancer did not go on to receive 90Y-M5A therapy. One patient failed to demonstrate tumor targeting. In a second patient 111In-DOTA-M5A imaging identified a brain lesion confirmed to be a brain metastasis on subsequent brain magnetic resonance imaging scan (Fig. 1). Of the remaining 16 patients who received therapy, 10 patients had colon cancer, 2 rectal cancer, 1 nonsmall cell lung cancer, 2 breast cancer, and 1 medullary thyroid cancer (Table 1). One of these 16 patients also had a previously unknown solitary brain metastasis seen on 111In-DOTA-M5A imaging, which was treated with stereotactic radiosurgery. Subsequent restaging demonstrated control of her brain metastasis allowing her to receive therapy on trial.
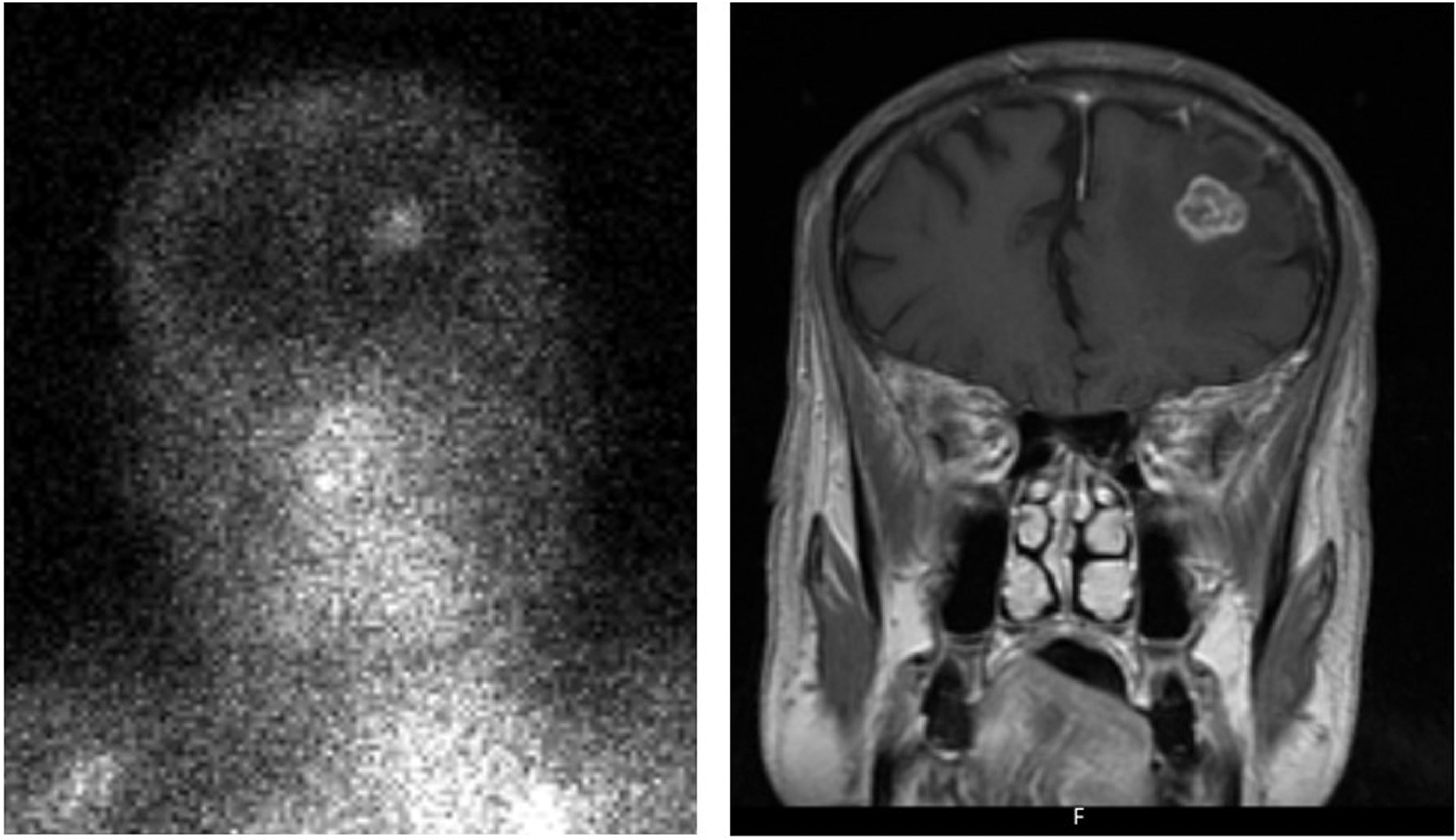
Detection of brain metastasis by 111In-DOTA-M5A (left) confirmed on subsequent magnetic resonance imaging scan (right). 111In, indium-111; DOTA, tetraazacyclodocecane-tetraacetic acid.
Patient Summary Demographic Data
F, female; M, male.
A previous phase I trial demonstrated the feasibility of 90Y-DOTA-cT4.66 RIT at 16.6 mCi/m2 (day 1) combined with gemcitabine (days 1 and 3) reaching a gemcitabine MTD of 150 mg/m2. 4 Therefore, per trial design the initial cohort of 3 patients received 12 mCi/m2 90Y-DOTA-M5A on day 1 followed by gemcitabine at 150 mg/m2 on days 1 and 3. A subsequent patient received 14 mCi/m2 90Y-DOTA-M5A followed by gemcitabine. Three of these 4 patients (2 at 12 mCi/m2 and 1 at 14 mCi/m2) demonstrated count nadirs occurring at week one and more prolonged grade 3 thrombocytopenia and leukopenia compared with prior experience with 90Y-DOTA-cT84.66 alone. The trial was, therefore, amended to eliminate gemcitabine for subsequent patients. Six patients were then treated at 12 mCi/m2 90Y-DOTA-M5A without gemcitabine. Two of the 6 demonstrated DLTs with grade 2 leukopenia and thrombocytopenia not returning to grade 1 by 10 weeks post-RIT. For the next cohort of 6 patients the dose was reduced to 10 mCi/m2. None of these 6 patients experienced a DLT. Details of toxicities are described in Table 2. Table 3 displays estimated radiation doses to critical organs and total body from 90Y-DOTA-M5A and compared with those previously seen with 90Y-DOTA-cT84.66. 12 No differences were observed between the two agents.
Toxicities
With gemcitabine 150 mg/m2 on days 1 and 3.
Estimated Radiation Yttrium-90 Doses to Normal Organs (cGy/mCi)
Data are means and ranges of intrapatient average doses determined from pre- and cotherapy administrations of 111In-DOTA-M5A.
Y, yttrium-90; 111In, indium-111; DOTA, tetraazacyclodocecane-tetraacetic acid.
In summary, 16 patients received 90Y-DOTA-M5A therapy, 6 at 10 mCi/m2, 9 at 12 mCi/m2, and 1 at 14 mCi/m2. Total administered activity ranged from 14.4 to 26.5 mCi of 90Y (Table 4). Six patients received two cycles of therapy. Seven patients completed treatment, whereas 5 patients were taken off protocol due to disease progression. Two patients (12.5%) were taken off protocol due to development of HAHA, which is less (p < 0.01, Fisher's exact test) than the 60% (21/35) patients with HACA previously treated with 90Y-DOTA-cT4.66 RIT. 11,12 One patient declined a second cycle (Table 5).
Summary of Yttrium-90 M5A Dose Escalation and Administered Activity
gem, gemcitabine.
Patient Outcomes
CI, confidence interval; HAHA, human antihuman antibody; OS, overall survival; PFS, progression-free survival; RIT, radioimmunotherapy.
Although no objective responses were observed in this patient population with chemotherapy refractory disease, stable disease at 3 months was seen in 10 of 16 patients (62.5%), including 5 of 6 treated on single agent 90Y-DOTA-M5A at the MTD. In addition, 2 patients demonstrated a reduction of serum CEA levels back to normal, 1 who received two cycles of RIT at 10 mCi/m2 demonstrated an 88% decrease in CEA, and another who received two cycles at 12 mCi/m2 and gemcitabine demonstrated a 64% decrease in CEA. Two other patients had 21% and 12% decreases in CEA. The median OS was 8.7 months (95% confidence interval [CI]: 5.8–29.2) and the median PFS was 2.8 months (95% CI: 1.2–5.8). Three patients who received 90Y-DOTA-M5A as a single agent had prolonged survival of 29.2, 39.7, and >53.1 months.
Discussion
Radiolabeled antibodies have demonstrated potential for diagnostic and therapeutic purposes. The purpose of this first in human phase I trial was to evaluate the safety and to determine the MTD and associated DLTs of 90Y-DOTA-M5A anti-CEA RIT initially with gemcitabine and subsequently as a single agent. One limitation of earlier mAbs used for RIT was the development of human anti-marine antibody (HAMA) or HACA responses, limiting multiple administrations. Murine mAbs typically result in HAMA responses in 80%–100% of patients after single administration. 17 –20 Chimeric mAbs reduce immunogenicity with HACA responses ranging from 40% to 80%. 21 –24 With the cT84.66 mAb 13 of 22 patients (59%) developed HACA in a phase I trial of 90Y-DTPA-cT84.66. 11 In another phase I trial of 90Y-DOTA-cT84.66, 8 of 13 patients (62%) developed HACA. 12 This was the main impetus for development the humanized M5A antibody, which demonstrated significantly lower immunogenicity with only 2 of 16 patients (12.5%) developing HAHA.
As with most
Although this study was primarily to characterize immunogenicity, toxicities, and define an MTD, there was evidence of antitumor effects in this heavily pretreated population with advanced disease. Ten of 16 patients (62.5%) demonstrated stable disease. In addition, 2 patients demonstrated an 88% and 64% decrease in CEA to within normal limits. These results are similar to other RIT agents directed against stolid tumors and reflect tumor doses achievable by RIT alone. Median and mean doses have been reported to be ∼10–20 Gy. Although these doses will have limited impact on bulky macroscopic disease, they can potentially result in clinically important antitumor effects, particularly in subclinical or microscopic disease settings. Future studies should, therefore, evaluate RIT as part of a combined modality approach in combination with established systemic chemotherapy, biologic therapy, or immunotherapy. Radiolabeling M5A with other radionuclides, such as lutetium-177 or α emitters, may have greater therapeutic potential and should also be evaluated in preclinical models and in clinical trials in the future.
This study also demonstrated the imaging potential of 111In-DOTA-M5A with only 1 out of 18 patients not demonstrating tumor targeting. 111In-DOTA-M5A also detected a previously unknown brain metastasis in 2 patients. Radiolabeling of M5A with a PET emitting radionuclide has the potential to further improve the imaging potential of this antibody.
In conclusion, this phase I study demonstrates that M5A, a humanized version of the cT84.66 anti-CEA mAb, has reduced immunogenicity compared with cT84.66, promising tumor imaging capabilities, and when labeled with 90Y is associated with some therapeutic effect in heavily pretreated patients with advanced refractory disease.
Footnotes
Disclosure Statement
No competing financial interests exist.
Authorship Confirmation Statement
D.A. performed data compilation, data analysis, and article preparation; D.Y. did scan interpretation; J.S. did data collection and data compilation; P.H.F. did the trial design, statistical analysis, and article preparation; K.P. did antibody radiolabeling; J.B. did radiation dose estimates; P.Y., A.W., D.C., and J.S. were in charge of antibody design, antibody production, antibody conjugation, and IND submission; Y.C., D.L., and M.C. performed patient accrual and trial execution; J.Y.C.W. was responsible for trial design, IND submission, trial implementation and execution, patient accrual, data compilation, data analysis, and article preparation. All coauthors have reviewed and approved the article before submission.
Funding Information
This study was supported by NIH PO1 43904 and NIH Cancer Center Core Grant 33572.