
Abstract
Accumulating data showed that cancer stem cells (CSCs) identified by cell surface markers contribute to the initiation, progression, and prognosis of human cancers. In this study, the expression of CSC candidates CD166, CD44, and Lgr5 in 65 cases of esophageal squamous cell carcinoma (ESCC) and 16 cases of control esophageal tissues were examined with immunohistochemistry (IHC). The correlation between tumoral expression levels of these CSC candidates and clinicopathological variables was analyzed. IHC results showed that the expression of CD166 in esophageal control tissues was completely negative, but it was in 87.69% (57/65) ESCC tissues. The expression of CD44 and Lgr5 did not differ between esophageal control tissues and ESCC tissues (p > 0.05). In addition, there were not correlations found among the expression levels of CD166, CD44, and Lgr5 in ESCC tissues. Clinicopathological analysis revealed that the tumoral expression level of CD166 correlated with lymph node involvement and TNM staging in patients with ESCC, and lower tumoral expression of CD44 was found in patients with advanced TNM staging. Kaplan–Meier survival curves suggested that expression level of CD166 appeared to have a negative impact on overall survival rate after surgery in patients with ESCC. Such impact was not found in other two CSC candidates. The authors therefore conclude that CD166 is a potential prognostic biomarker and correlates with advanced progression features in patients with ESCC.
Introduction
Esophageal cancer is a highly lethal malignancy. Histologically, most of the esophageal cancer in China are esophageal squamous cell carcinoma (ESCC). In the authors' location (Henan province, Central China), the incidence of ESCCs is particularly high and remains one of the most common malignances in this region.
Epidemiological investigation revealed that the incidence of ESCCs in Henan province was 39.46/100,000 (for both sex) and 47.61/100,000 (for male), respectively. 1 The incidence and mortality of ESCCs are both listed in the third place of cancers in Henan province. 1 The prognosis of ESCCs is very poor because metastasis has often occurred in many ESCC patients at initial diagnosis, and therefore, curative surgery becomes impossible. Therefore, there is great interest in clarifying the mechanisms of cancer progression, metastasis, and prognosis in patients with ESCC. 2 –8
It is now generally accepted that the initiation of ESCC is originally from cancer stem cells (CSCs), which can be identified by a variety of cell surface markers. 9 –11 In addition to its role in initiating human cancers, CSCs may also significantly contribute to progression, metastasis, and recurrence of tumors after initially successful chemotherapy and/or radiation therapy. 12 Clinically, due to the high incidence of metastasis and therapeutic resistance, prognosis of patients with ESCCs remains poor. Increased understanding of CSCs in ESCCs may result in the improvement of cure rate and reduction of recurrence rate and finally prolong patients' survival. The well-defined markers for CSCs in ESCCs not only can increase the detection rate of cancer recurrence but also can be further applied to targeted therapy for cancer. Indeed, targeting CSCs populations have been shown to prevent recurrence and improve the efficacy of current anticancer therapies in various types of cancers. 13 However, clinical studies showed debatable results regarding the significance of CSC markers in human ESCCs. 14 Some studies demonstrated that CSCs in ESCCs are potentially associated with tumor growth, disease stage and metastasis, 15 –17 and chemotherapy 18 or radio resistance. 19 However, other studies could not confirm such a positive association. 17,20 One of the possible reasons for such conflicting reports may be that each CSC marker only labels a small subpopulation of CSCs, and there is a lack of agreement on the best markers for CSCs in cancers, including ESCC that doubts about the real phenotype of the CSCs. Among diverse types of CSC markers, CD44 is a group of distributed cell surface transmembrane glycoproteins and frequently used as a stem-like marker in identifying the CSCs in various types of human cancers, including ESCC. 9,21 –24 However, there was no consensus regarding the clinical significance of CD44 in patients with ESCC. 10,22,25 Some studies showed that CD44-positive CSCs in the ESCC tissues may have a higher tumorigenic potential in vivo, 23 and correlated with advanced features in patients with ESCC. 10,25,26 But it was not confirmed by other studies. 22
Lgr5 is a member of the G-protein coupled receptor family and binds to ligands to potentiate the Wnt/β kinase signaling pathway. Lgr5 is first identified to be a stem cell marker in the intestine, 27 and after, that has been reported to be the marker of CSCs in other types of human cancers. 28 –34 Recently, one study characterized the expression of Lgr5 in human esophageal adenocarcinoma and its premalignant lesion Barrett's esophagus. 28 The results revealed that the expression of Lgr5 was increased from Barrett's esophagus to advanced dysplastic lesions and esophageal adenocarcinoma. The intensity of Lgr5 expression in high-grade dysplasia and esophageal adenocarcinoma was significantly higher than that in Barrett's esophagus, esophageal adenocarcinoma patients with higher Lgr5 expression had a worse survival than those with lower expression. 28 Burkhard H.A. von Rahden et al. confirmed the expression of Lgr5 in Barrett's esophagus and esophageal adenocarcinoma tissues, but not in ESCC tissues. 35 However, Lv et al. more recently reported that Lgr5 is overexpressed in tumoral tissues and correlated with a poor prognosis in patients with ESCC, 36 while silencing of Lgr5 inhibits the proliferation, migration, and invasion of ESCC cell lines. 36 Thus, the clinical significance of Lgr5 in patients with ESCC remains in debate.
CD166 is an immunoglobulin superfamily cell adhesion molecule and widely expressed in various tissues, such as neurons, fibroblasts, endothelial cells, and keratinocytes. It has been reported that CD166 can be a putative biomarker for both mesenchymal stem cells and CSCs. 33,37 –39 In addition, it could also contribute to cancer cell invasion and associated with progression and prognosis in patients with cancers. 21,37,40 –44 Studies have shown that the expression of CD166 in the ESCC is highly expressed in tumor epithelium, 44,45 The clinicopathological analysis revealed that the expression level of CD166 is closely associated with advanced characteristics and high expression level is associated with poor prognosis in patients with ESCC. 44,45 Interestingly, CD166 is not expressed in normal human esophageal epithelium. This finding provides a possibility to use it as an additional factor to differentiate the ESCC CSCs from normal stem cells as the authors have known that most CSC markers are positive for both normal and CSC cells.
Based on above information, the authors have therefore designed this study to evaluate the clinicopathological and prognostic significance of CD166, CD44, and Lgr5 expression in patients with ESCC.
Materials and Methods
Paraffin tissue blocks
A total of 65 paraffin blocks of ESSCs and 16 paraffin blocks of control esophageal tissues were collected from the biobank in Department of Pathology, the Second Affiliated Hospital of Zhengzhou University. The mean age at treatment was 58.6 years (ranging from 32 to 76 years). The male female ratio was 42:23. No patient received radiotherapy, chemotherapy, and/or immunotherapy before curative surgery was performed. Regular follow-up was conducted in all 45 ESCC patients and overall survival (OS) was recorded. The median follow-up time was 48 months. Representative sections were cut at 4 μm and stained with hematoxylin-eosin (H&E) for routine histological diagnosis. Basic information of ESSC histological and clinical findings is summarized in Table 1. Written informed consent has been obtained, studies have been performed according to the Declaration of Helsinki, and the procedures had been approved by the local Medical Research Ethics Committee of the Second Affiliated Hospital of Zhengzhou University.
Basic Information of Esophageal Squamous Cell Carcinoma Patients
Upp, upper part of esophagus; M, middle part of esophagus; L, lower part of esophagus; ESCC, esophageal squamous cell carcinoma.
Immunochemistry
Representative sections from both ESCC and control tissues were deparaffinized in xylene, rehydrated in graded ethanol, and incubated in 0.3% H2O2 solution in methanol for 15 min to block endogenous peroxidases. Antigen retrieval was achieved of boiling sections for 15 min in 0.01 M citrate buffer, pH 6.0. Nonspecific binding was blocked by incubating sections in phosphate-buffered saline (PBS) containing 4% normal bovine serum and 0.25% Triton-X 100. The slides were rinsed three times with PBS with 0.25% Triton-X 100 (PBS-T) for 3 min each time and incubated with mouse anti-CD166 (Thermo Fisher, Carlsbad, CA), rabbit anti-CD44 (Abcam, Cambridge, United Kingdom), and rabbit anti-Lgr5 antibodies (MBL International, Woburn, MA) overnight at 4°C. After washing with PBS-T for 3 times, the slides were developed with commercial VECTASTAIN Elite ABC Kits (Vector Laboratories, Burlingame, CA) according to the manufacturer's instructions and the authors' published methods. 2,3,29,46,47 3-Amino-9-ethylcarbazole (AEC; Vector Laboratories) was used as chromogen, and slides were slightly counterstained with Mayer's hematoxylin. Then, the stained slides were observed and evaluated under light microscope.
The negative control slides for immunohistochemistry (IHCs) were performed routinely: (1) primary antibodies were substituted with the isotype-matched control antibodies; and (2) secondary antibody was substituted with PBS-T.
Morphological evaluation
The semiquantified density grading of CSCs was used according to the method described in their previous publication. 29 In brief, scoring for CD166-, CD44-, and Lgr5-positive ESCC cells was conducted in at least five well-orientated fields with abundant positive cell distribution from each slide under 400 × high-power magnification. In the ESCC or control sections, the densities of epithelial cells positive for CD166, CD44, and Lgr5 were graded on a scale of 0–3: grade 0 indicated an absence of cells; grade 1 indicated a 1%–5% presence of cells; grade 2 indicated a 6%–25% presence of cells; and grade 3 indicated a presence of 26%–100% cells. 29
Statistical analysis
All statistics were compiled using the software package SPSS, version 21.0. The grading score data of CSC markers in the control and ESCC were evaluated by nonparametric rank correlation test, and the two-category data were analyzed by the chi-squared and Fisher's exact tests. Moreover, Spearman's correlation coefficient was used to analyze the relationships among expressions of these three factors in ESCC tumor tissues. The grading score data of stem cell markers in the ESCC against OS curves were plotted using of Kaplan–Meier method and analyzed using a log-rank test. Multivariate analysis of prognostic factors for OS was performed using the Cox regression model. p < 0.05 was considered as statistically significant.
Result
Tumoral expression of CD166, CD44, and Lgr5 in ESCC tissue
IHC images revealed that CD166-immunoreactivity (IR) was completely absent in control esophageal epithelial cells (Fig. 1A), however it was observed in 87.69% (57/65) ESCC cases. CD166-IR in ESCC tissues was located in the cell membrane or cytoplasm of ESCC cells (Fig. 1B). Semiquantitative results showed that density score of CD166-IR cells in ESCC tissues was significantly higher than that in the controls (p < 0.01, Table 2).
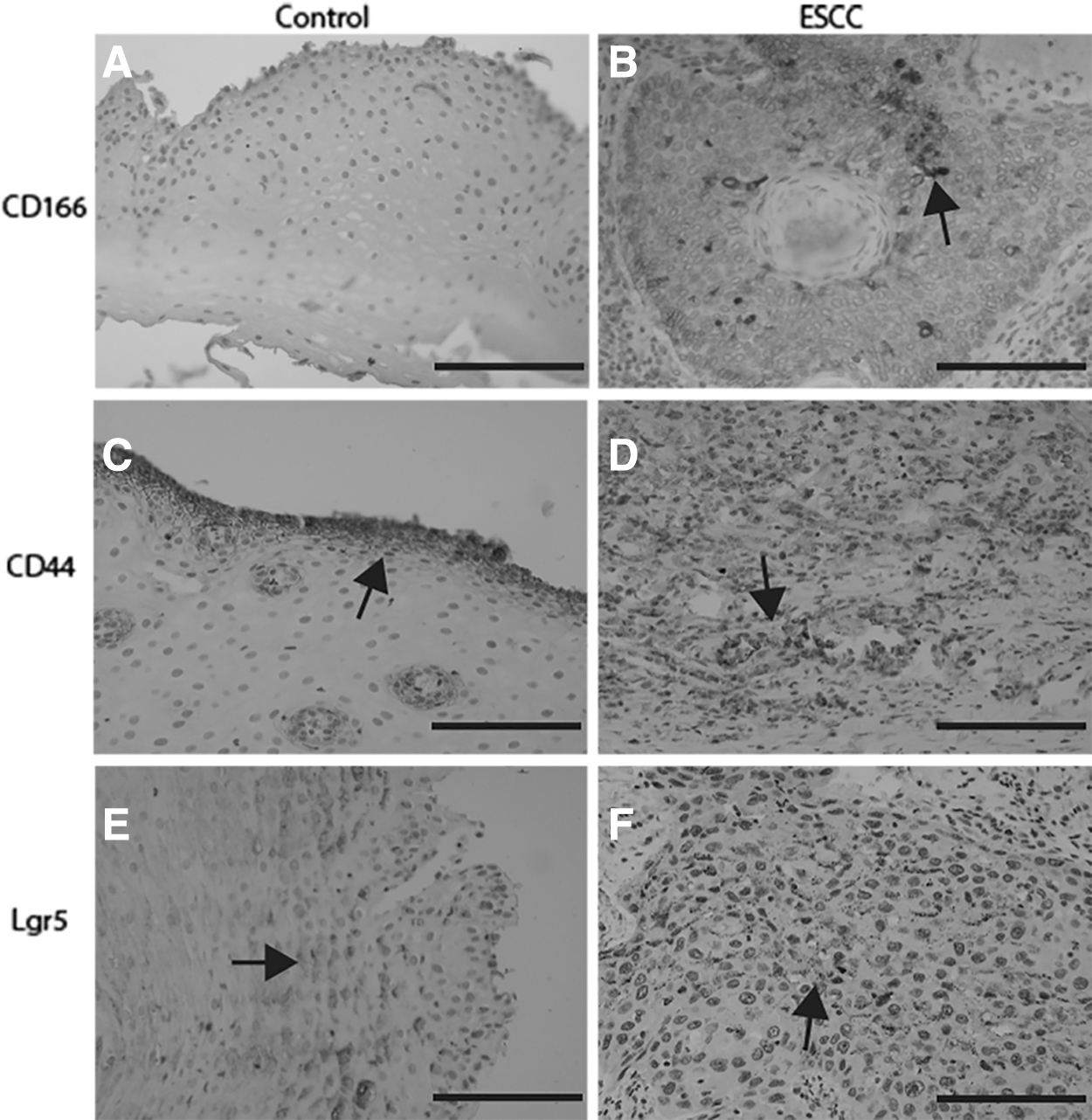
The tumoral expression of commonly used cancer stem cell markers in ESCC tissues. Immunohistochemical results showed that the expression of CD166 was totally absent in normal control epithelium
Epithelial Expression Rate of CD166, CD44, and Lgr5 in Esophageal Squamous Cell Carcinoma Tissues
CD44-IR in control esophageal sections was solely expressed in the cell membrane (Fig. 1C). However, it was observed in both the cytoplasm and membrane of cancer cells in ESCC sections (Fig. 1D). The positive rates of CD44 in ESCC sections were similar to that in control sections (p > 0.05, Table 2).
Lgr5-IR was diffusely expressed in the cytoplasm and cell membrane in both control esophageal squamous cells (Fig. 1E) and ESCC cells (Fig. F). The positive rate was not different between the control and the ESCC groups (p > 0.05, Table 2).
Spearman correlation coefficient analysis revealed that correlations were not found among the expression levels of CD166, CD44, and Lgr5 in ESCC tissues (p > 0.05, Table 3).
Correlation of CD166, CD44, and Lgr5 Expression Levels in Esophageal Squamous Cell Carcinoma Tissues
Clinicopathological significance of tumoral expression level of CD166, CD44, and Lgr5 in patients with ESCC
The expression score of CD166-IR in tumor cells was not correlated with age, gender, degree of differentiation, invasion depth, and growth site in patients with ESCC (all p > 0.05, Table 4). However, it was significantly correlated with lymph node metastasis and TNM stages (p < 0.05, Table 4). In addition, the expression of CD44 in ESCC tissues was inversely correlated with TNM stages (p < 0.05, Table 5). But, the expression scores of Lgr5 did not correlate with clinicopathological variables in patients with ESCC (p > 0.05, Table 6).
Correlation Between Clinicopathological Parameters and Tumoral Expression of CD166 in Patients with Esophageal Squamous Cell Carcinoma
Upp, upper part of esophagus; M, middle part of esophagus; L, low part of esophagus.
Correlation Between Clinicopathological Parameters and Tumoral Expression of CD44 in Patients with Esophageal Squamous Cell Carcinoma
Upp, upper part of esophagus; M, middle part of esophagus; L, low part of esophagus.
Correlation Between Clinicopathological Parameters and Tumoral Expression of Lgr5 in Patients with Esophageal Squamous Cell Carcinoma
Upp, upper part of esophagus; M, middle part of esophagus; L, low part of esophagus.
Survival analysis
OS data were available for 45 patients with ESCC. According to the mean values of density scores, the tumoral expression of CD166-IR, CD44-IR, and Lgr5-IR in ESCC patients were divided into low (score 0 & 1) and high (score 2 & 3) groups. Kaplan–Meier survival analysis showed that OS after surgery was significantly reduced in patients with a high expression level of CD166 than those with a low expression level of CD166 (p = 0.0003, Fig. 2A). Whereas, the expression levels of CD44 and Lgr5 in ESCC were not associated with OS (p = 0.5392 and p = 0.1448, respectively, Fig. 2B, C). To investigate whether CD166 expression was an independent prognostic factor for OS, and to assess the clinical significance of various parameters that might influence OS in patients with ESCC, univariate and multivariate analyses were performed. Data of univariate Cox proportional analysis showed that CD166 expression was a significant risk factor that affected the OS in patients with ESCC with a hazard ratio of 5.646 and a p-value of 0.001 (Table 7). In addition, multivariate survival analysis based on the Cox proportional hazards regression model identified that increased tumoral expression of CD166 was a significant prognostic factor, with a hazard ratio of 7.334 and a p-value of 0.000 (Table 7).

Survival curves of ESCC patients according to the tumoral expression levels of CD166, CD44, and Lgr5. Kaplan–Meier analysis revealed that the tumoral expression level of CD166 predicated the overall survival rate after surgery in patients with ESCC, patients with higher expression of CD166 appeared to have a shorter survival rate after surgery
Univariate and Multivariable Analyses of Overall Survival in Patients with Esophageal Squamous Cell Carcinoma
HR, hazard; CI, confidence interval.
Discussion
In this study, the authors investigated the clinicopathological and prognostic significance of tumoral expression of CSC markers CD44, CD166, and Lgr5 in patients with ESCC. The authors' results suggest that despite the tumoral expression of these three CSC markers in ESCCs as expected, only the tumoral expression level of CD166 was correlated with advanced features and prognosis.
IHC with specific antibodies is an ideal technique to visualize the localization of proteins in cells and tissues. 2,3,6,48,49 Using this technique, they examined that expression of CD166, CD44, and Lgr5 in ESCC specimens. The results showed that CD166 is expressed 87.69% of ESCC tissues and entirely absent in control esophageal tissues. Their findings are consistent with other studies that detected a higher level of CD166 in ESCC tissues compared to expression in control esophageal tissues. 45,50 CD44 is one of the early used CSC markers. The authors were able to show that although high positive rates of CD44 were observed in both the control and ESCC groups, the difference of CD44-positive cells was not significant between the control and ESCC. Since they use IHC as a main technique in determining and semiquantifying CD44 expression in the ESCC, the difference of CD44 intensity between the control and ESCC must be considered. Indeed, 36 of 65 ESCC specimens were with a strong intensity (score 2 or 3, Table 5) that was higher than that in the controls, which is similar to a previous study that reported a higher proportion of strong CD44 intensity in ESCC specimens. 23 Previously, two studies have examined the expression of Lgr5 in human Barrett's esophagus and esophageal adenocarcinomas. 28,35 Their main findings were that the expression of Lgr5 was increased from Barrett's esophagus to esophageal adenocarcinoma. However, they did not find the expression of Lgr5 in ESCC specimens, 35 and a recent study has reported a completely contrast finding, in which a significant increased expression of Lgr5 was shown in ESCC tissues. 36 In this study, the authors have found that Lgr5 is nonstatistically expressed in both control and ESCC sections. Discrepancies between the current findings and other groups may be due to the use of different techniques and patient cohorts.
With respect to the relationship between these three CSC markers and clinicopathological parameters of patients with ESCC, they indicated that the tumoral expression level of CD166 was significantly associated with lymph node metastasis and TNM staging, which confirm previous findings that increased expression of CD166 was associated with advanced disease stage, enhanced tumor invasiveness, and nodal metastasis in patients with ESCC. 45 They also found that the expression of CD44 was inversely associated with TNM stage in patients with ESCC. Their current results are consistent with the results from a previous study, 22 but contrast to the report by Hara et al. 25 They have found that c-Met/CD44v6 were associated with tumor progression or chemoresistance, and negatively impact patient prognosis in ESCC. 25 One of the reasons may be different antibodies and positive cell density grading methods used in different studies. However, such a correlation between the tumoral expression level of Lgr5 and clinicopathological variables were not found in patients with ESCC. In addition, Spearman's correlation coefficient analysis revealed that correlations were not found among the expression levels of CD166, CD44, and Lgr5 in ESCC tissues. This finding may suggest that each putative CSC only label a small proportion of CSCs, instead of all CSCs.
A Kaplan–Meier survival analysis revealed that the tumoral expression level of CD166 has a predicating significance of survival rate after surgery in patients with ESCC. ESCC patients with a higher expression level of CD166 tend to have a shorter OS time than those with lower expression level. The tumoral expression levels of CD44 and Lgr5 did not show such predication. The authors' results seem to be in contrast to a recent report, in which the authors found that ESCC patients with a high expression of Lgr5 are associated with a poor prognoses. 36 One of the possible reasons for conflicting results could be that they examined the expression level of Lgr5 by quantitative PCR that measured the total Lgr5 in whole tissues at mRNA level, whereas the authors used IHC with a specific antibody that evaluated only the expression of Lgr5 only in ESCC cells. Using different cell surface markers combining with IHC is the most common histological technique to identify CSCs in human cancers. However, each marker could only label a small proportion of CSCs. This might result in a conflicting conclusion.
Finally, data from univariate Cox proportional analysis suggested that density of tumoral CD166 expression was a significant risk factor for the OS in patients with ESC). Multivariate survival analysis based on the Cox proportional hazards regression model revealed that only increased tumoral expression of CD166 intensity remains an independent prognostic factor, but not CD44 and Lgr5. CD166 is an immunoglobulin superfamily cell adhesion molecule involved in tumor cell-tumor cell adhesion, tumor cell-endothelial cell adhesion, or tumor cell-matrix adhesion and plays a crucial role in the formation or metastasis of primary tumors. 44,45 Weichert et al. 44 described that CD166 correlates with shortened patient survival and confirmed in other types of solid cancers. 37,42 Currently, there are few studies to evaluate the prognostic impact of CD166 in patents with ESCC. Tachezy et al. 50 reported a positive correlation between predominantly membranous CD166 expression and shortened survival in a group of 410 cases of ESCC. In addition, Verma et al. 45 also found that CD166 expression is increased in dysplastic tissues as well as in ESCC tissues, which is associated with aggressive tumor behavior. Taken together, those findings might suggest that CD166 could be a potential predicator for tumor progression and prognosis in patients with ESCC.
It has been postulated that direct targeting of CSCs might be a better treatment efficacy of cancer.
51
More recently, Satar et al. have demonstrated that capacity of proliferation and chemoresistance are higher in nonsmall cell lung cancer cell line with the triple-positive (EpCAM+/CD166+/CD44+) compared to that with triple-negative (EpCAM−/CD166−/CD44−) subpopulation.
52
Furthermore, the therapeutic effect of targeting CD166 in solid cancers has been discussed. Wang et al. have shown that
In conclusion, the authors' current results revealed that the tumoral expression of CD166 in ESCC tissues is a useful putative CSC biomarker for assessing the tumor progression, prognosis, and may be used as a molecular target for the treatments for ESCC.
Footnotes
Acknowledgment
The authors greatly appreciate the help from colleagues at the Department of Pathology of the hospital for data analysis.
Disclosure Statement
There are no existing financial conflicts.
Funding Information
This work is supported by the Innovation Scientists and Technicians Troop Construction Projects of Henan Province (CXTD20150009) and the Nature and Science Foundation of Henan Province (Program No. 182300410326), China.