
Abstract
Background:
Despite advances in therapy of Hodgkin's lymphoma (HL), a proportion of patients will not respond or relapse. The authors had previously identified CD25, IL-2Rα, as a target for systemic radioimmunotherapy of HL since most normal cells do not express CD25, but it is expressed by a minority of Hodgkin/Reed-Sternberg (HRS) cells and most Tregs rosetting around HRS cells.
Study Design and Treatment:
This was a single institution, nonrandomized, open-label phase I/II trial of radiolabeled 90Y-daclizumab, an anti-CD25 monoclonal antibody, BEAM (carmustine, etoposide, cytarabine, and melphalan) conditioning treatment followed by autologous hematopoietic stem cell transplant (ASCT). Four patients with refractory and relapsed HL were treated in this trial with 3 patients receiving a single dose of 564.6–574.6 MBq 90Y-daclizumab and the fourth patient receiving two doses of 580.9–566.1 MBq 90Y-daclizumab followed by high-dose chemotherapy and ASCT.
Results:
All 4 evaluable patients treated with 90Y-daclizumab obtained complete responses (CRs) that are ongoing 4.5–7 years following their stem cell transplant.
The spectrum and severity of adverse events were mild and more importantly none of the patients, including several with multiple therapies before this treatment, developed the myelodysplastic syndrome.
Discussion:
Targeting by daclizumab was not directed primarily at tumor cells, but rather the nonmalignant CD25-expressing T cells adjacent to the HRS cells and 90Y-daclizumab provided strong enough β emissions to kill CD25-negative tumor cells at a distance by a crossfire effect. Furthermore, the strong β irradiation killed normal cells in the tumor microenvironment.
Conclusions:
90Y-daclizumab (anti-CD25), high-dose BEAM chemotherapy and ASCT was well tolerated and yielded sustained complete remissions in all 4 patients with recurrent HL patients who completed their treatment.
Significance:
Despite advances, a proportion of patients with HL will not have a CR to their initial treatment, and some with CRs will relapse. They demonstrated that the addition of 90Y-daclizumab into the preconditioning regimen for refractory and relapsed HL patients with high-dose BEAM chemotherapy and ASCT provided sustained CRs in the 4 patients studied. Two of these patients were highly refractory to multiple prior treatments with bulky disease at entry into this study, including 1 patient who never entered a remission and had failed 6 different therapeutic regimens. Despite the small number of patients treated in this study, the sustained clinical benefit in these patients indicates a highly effective treatment. The daclizumab was directed primarily not at HRS cells themselves but toward nonmalignant T cells rosetting around malignant cells. 90Y provided strong β emissions that killed antigen nonexpressing tumor cells at a distance by a crossfire effect. Furthermore, the strong β radiation killed normal cells in the tumor microenvironment that nurtured the malignant cells in the lymphomatous mass. The present study supports expanded analysis of 90Y-daclizumab as part of the regimen of ASCT in patients with refractory and relapsed HL.
Introduction
There were ∼8500 new cases of Hodgkin's lymphoma (HL) in 2018 and 1050 patients died of their disease according to SEER database, based on November 2017 SEER data submission (posted to the SEER website, April 2018). 1 Although treatment with modern combination chemotherapy regimens is associated with about an 80% complete remission rate, 10%–15% of patients will not respond to treatment or will relapse. 2 –7 High-dose chemotherapy with autologous hematopoietic stem cell support (ASCT) has become the treatment of choice. Brentuximab vedotin has been approved for the treatment of relapsed HL. 8 –10 Furthermore, antiprogrammed death (PD)-1 agents have shown outstanding results in classical HL. 11 However, despite this aggressive treatment, a meaningful fraction of patients will not respond, and a proportion of patients will develop recurrent disease.
To date, more than 30 different monoclonal antibody preparations directed toward antigens expressed by malignant Hodgkin/Reed-Sternberg (HRS) cells have been studied. 8 These include monoclonal antibodies linked to drugs and targeting CD30 or CD25 expressed on HRS cells. Brentuximab vedotin, an anti-CD30 antibody drug conjugate, has induced a significant number of responses in refractory HL. 9,10 Although other antibody immunotoxins have demonstrated some clinical efficacy they have yielded few complete responses (CRs). 12,13 An alternative strategy has been to arm monoclonal antibodies with radionuclides. Radioimmunotherapy (RIT) using 131I-anti-CD30 and 90Y-anti-ferritin antibodies have provided partial responses (PRs) and CRs in HL. 14 –17 Deficiencies in these approaches reflect the small number of CD30-expressing HRS cells in the tumor and the lack of tumor specificity of ferritin-targeted antibodies.
We have identified CD25, the IL-2Rα subunit (IL-2Rα), as an alternative more favorable target for systemic RIT of HL. 3,18 –24 The scientific rationale is that with the exception of Tregs, CD25 is not expressed by many normal cells but is expressed on both a minority of HRS cells and pivotally on Treg cells rosetting around the HRS cells. 25 –28 90Y, an energetic β particle emitter that travels a mean of ∼3 mm in soft tissue, acts through crossfire throughout the tumor masses, providing a strategy for killing tumor cells at a distance of several cell diameters, including CD25negative HRS cells, provided that CD25+T cells in their vicinity express the target antigen. 25 –29 Previously the authors reported a trial in which they treated 46 patients with recurrent or refractory HL with 90Y-daclizumab every 6–10 weeks for up to 7 doses depending on hematological recovery. 3 Among the 46 evaluable patients, there were 14 CRs and 9 PRs, 14 patients with stable disease (SD), and only 9 patients whose best response was progressive disease. Responses were observed both in patients whose HRS cells expressed CD25 and in those whose neoplastic cells were CD25 negative provided that associated rosetting cells expressed CD25. 3 Toxicities in this advanced disease population were transient bone marrow suppression and the myelodysplastic syndrome (MDS) in 6 patients who had not been evaluated with bone marrow karyotype analysis before therapy.
Given that recurrent disease remains the single most common cause of treatment failure after ASCT in patients with relapsed HL and given the 50% response rate achieved with 90Y-daclizumab, they sought to improve the long-term disease-free survival achieved by ASCT by incorporating 90Y-daclizumab into the transplant preconditioning regimen. In the present study, patients with refractory or relapsed HL who had not undergone previous autologous stem cell transplant (ASCT) were treated in the Phase I dose-escalation trial with the initial cohort receiving a single administration of 90Y-labeled daclizumab 566–570 MBq followed by a 4-day myeloablative regimen with carmustine, etoposide, cytarabine, and melphalan (BEAM) and ASCT. Subsequent cohorts were to receive additional treatments with 90Y-daclizumab before BEAM-ASCT; however, the study was ended prematurely as the radiopharmacy production facility for the radiolabeled antibody was no longer available. In this study, they report the results of the four patients treated on the study, all of whom remain in CR without evidence of treatment-related MDS after at least 4.5 years of follow-up.
Materials and Methods
Eligibility and qualifying testing
This was a single institution, nonrandomized, open-label phase I/II trial. From September 2012 to September 2014 patients with refractory and relapsed (classical nodular Hodgkin's lymphoma nodular sclerosis subtype were excluded) HL who had not undergone a previous ASCT were treated in phase I dose escalation of 90Y-daclizumab followed by the standard preparative (carmustine, etoposide, cytarabine [Ara-C], and melphalan [BEAM]) chemotherapy regimen and then ASCT (Table 1). To be eligible for this protocol, adult patients were required to have radiographically measurable disease, adequate biochemical (renal, hepatic), hematologic function (pulmonary, cardiac), absence of infections (HepB, HepA, HIV), and ECOG performance status ≤1.
Patient Characteristics Prior to Therapy
Withdrew from protocol
Removed from protocol due to noncompliance with treatment plan after initial Yttrium daclizumab treatment
ABVD, doxorubicin, bleomycin, vinblastine, dacarbazine; ICE, Ifosfamide, carboplatin, etoposide; BV, brentuximab vedotin; GV, gemcitabine, vinorelbine; IGEV, Ifosfamide, gemcitabine, vinorelbine; EPOCH-RC, etoposide, prednisone, vincristine, doxorubicin, cyclophosphamide, Revlimid, alemtuzumab; EPOCH, etoposide, prednisone, vincristine, Adriamycin, cyclophosphamide; GemOx, Gemcitabine, Oxaliplatin; HD Dex, high-dose dexamethasone; CCNU, Lomustine; CDDP, Cisplatin; VP-16: Etoposide
Furthermore, the patients must have had at least one of the following: (1) initial relapse <12 months after achieving a CR with primary chemotherapy for HL; (2) stage III/IV disease at diagnosis; (3) chemotherapy-resistant disease, or (4) did not achieve a CR with cytoreductive chemotherapy before a planned transplant. Pretreatment evaluation included standard biochemical panels, complete blood count, confirmation of HL pathologic diagnosis by NIH Pathology Department, and that more than 10% of cells in the tumor sample were immunohistochemically positive for CD25, the target of daclizumab. The HRS cells could be negative for CD25 provided the Tregs rosetting around these cells were positive. In addition to qualify for the study, patients needed adequate respiratory function in formal pulmonary function testing and an absence of cardiac pathology on echocardiograph and EKG.
Pretreatment staging procedures included bone marrow (biopsy and aspirate) to assess for bone marrow involvement, computed tomography (CT) scan of neck, chest, abdomen, and pelvis, and FDG positron emission tomography (PET)/CT scan to assess extent of disease, and when appropriate, magnetic resonance imaging of the brain to confirm absence of central nervous system involvement that would disqualify the patient for the trial. Six patients qualified and were consented for the protocol with 4 receiving their full treatment. Patient 4 was removed from the study for protocol-defined criteria for failure to mobilize an adequate number of CD34+ stem cells and never received any therapeutic treatment. Patient 5 received initial 90Y-daclizumab treatment without significant difficulties but withdrew his consent for treatment and was removed from the protocol before BEAM-ASCT (see Supplementary Data).
Treatment, dose escalation, and dose-limiting toxicity
Approximately 1 month before the start of therapy, all patients had CD34+ stem cell mobilization using high-dose G-CSF (granulocyte colony-stimulating factor; 10–16 μg/kg/d × 5 or 6 d) with plerixafor (Mozobil) mobilization (240 μg/kg within 6 h) before the stem cell pheresis to obtain 4 × 106 CD34+ cells/kg that were stored for later hematopoietic reconstitution. The radioimmunotherapy dose escalation plan used the standard 3 + 3 phase I design with the initial patient cohort receiving a single administration of 90Y-daclizumab 555 MBq. Subsequent cohorts were planned to receive the same amount of 90Y-daclizumab followed 42 d later with the second 90Y-daclizumab treatment and in the absence of dose-limiting toxicity (DLT) at progressively higher doses of the second treatment of 90Y-daclizumab 555, 1110, 1665, 2220, 2775, and 3330 MBq.
The therapeutic 90Y-daclizumab was administered with unconjugated daclizumab to bring the total combined mass of antibody to 5 mg. In addition, for 3 d after their 90Y-daclizumab infusion all patients received repeat infusions of trisodium calcium diethylenetriaminepentaacetate (Ca-DTPA) to chelate and promote excretion of any free 90Y. Ten days (2.7 half-lives) after their last 90Y-daclizumab treatment, all patients began their 4-d myeloablative regime with BEAM regimen. Treatment with Keratinocyte Growth Factor (KGF/Palifermin) was initiated 3 d before the start of BEAM chemotherapy for mucositis prophylaxis.
One day after completion of their myeloablative treatment, all patients received their ASCT infusion (2–4 × 106 CD34+ cells/kg of actual weight) and 3 d later began G-CSF that was given until neutrophil recovery ≥1000/μL for 3 consecutive days. All patients received standard post stem cell transplant supportive care, including prophylactic antibacterial and antiviral antibiotics until recovery of their other hematopoietic functions.
Dose-Limiting Toxicities were defined as ≥grade 3 (CTCAE v4.0) nonhematologic toxicity related to 90Y-daclizumab with the exception of fatigue lasting for more than 5 d and occurring before the start of the BEAM chemotherapy.
This study was approved by the Institutional Review Board of the National Cancer Institute. This trial is registered as NCT01468311. All patients gave written informed consent for participating in the protocol. This study was performed under the conditions of the Helsinki accords (see Supplementary Data).
90Y-and 111In-labeled daclizumab
Daclizumab (Hoffmann-La Roche, Nutley, NJ) was conjugated with 2-p-isothiocyanatobenzyl-transcyclohexyldiethylenetrimine pentaacetic acid (CHX-A) and was radiolabeled with 90Y for therapy and with 111In for imaging as similar to previously described. 3,29
111In-labeled daclizumab imaging
Simultaneous with administration of therapeutic 90Y, 111In-labeled daclizumab was administered to identify biodistribution and tumor targeting. The patients received 185–188.7 MBq of 111In daclizumab with 0.4 mg of CHX-A-conjugated daclizumab mixed together with 566.1–580.9 MBq of 90Y-daclizumab on 0.4–0.6 mg of CHX-A daclizumab; these antibodies were mixed and 4–4.2 mg of cold daclizumab was added to bring the mass to 5 mg. Purity of all radiolabeled antibodies determined by instant thin-layer chromatography ranged from 99% to 100% and median immunoreactivity for 111In daclizumab was 88% and for 90Y daclizumab was 86% using an HPLC assay. The antibodies were administered intravenously as a 1.8–2 h infusion.
Patients also received a 250 mg/m2 infusion of diethylenetriaminepentaacetic acid (DTPA) to bind any free 90Y. No acute toxicity was noted related to antibody infusion. All patients, including those whose Reed-Sternberg cells did not express CD25, had positive localization of 111In-daclizumab at disease sites. On the basis of this and a previous study, the estimated tissue radiation dose per 555 MBq of 90Y-daclizumab was 173 cGy to bone marrow, 263 cGy to liver, 1062 cGy to spleen, and 33 cGy to the whole body. The estimated tumor dose with 555 MBq ranged from 210 to 365 cGy. 3
Immune responses to daclizumab
The method used to define immune responses to treatment was described previously. 3
Assessment of extent of disease
All patients underwent baseline contrast-enhanced CT and PET scan within × 28 d of the start of treatment and at regular intervals following their ASCT. Index lesions were selected for response evaluation criteria in solid tumors assessment of their pretreatment FDG PET/CT and were reassessed in the subsequent restaging scans. In brief, PET/CT images were acquired after a 60-min uptake period and no patient was hyperglycemic. Images were read clinically and then re-read together with prior FDG images as well as with antibody immunoscintigraphy.
All patients underwent single-proton emission computed tomography CT imaging from neck to proximal thigh at 2 h postadministration of 111In-daclizumab and at 96–144 h. Images were interpreted by an experienced nuclear medicine physician and compared with baseline and subsequent PET/CT scans.
Results
This was a single-institution, nonrandomized, open-label phase I/II trial. Six patients were evaluated and 4 patients with refractory and relapsed HL were treated with radiolabeled 90Y-daclizumab anti-CD25 monoclonal antibody incorporated into the preconditioning regimen before BEAM conditioning therapy with an ASCT (Table 1).
Treated patients
As seen (Table 2), the patients were heavily pretreated with a median 3 prior chemotherapy regimens and all had progressive multisite disease at the time they began the protocol treatment regimen as summarized below in Table 2. Patients 1 through 3 were treated with a single 564.6–574.6 MBq infusion and patient 6 received two 580.9 and 566.1 MBq infusions of 90Y-daclizumab 15 mCi before BEAM. Using immunohistochemical analysis in only one biopsy (in 4 patients) did >10% of the HL neoplastic cells express CD25 (Fig. 1B), whereas the associated rosetting cells expressed CD25 in all 4 cases examined (Fig. 1A–D).
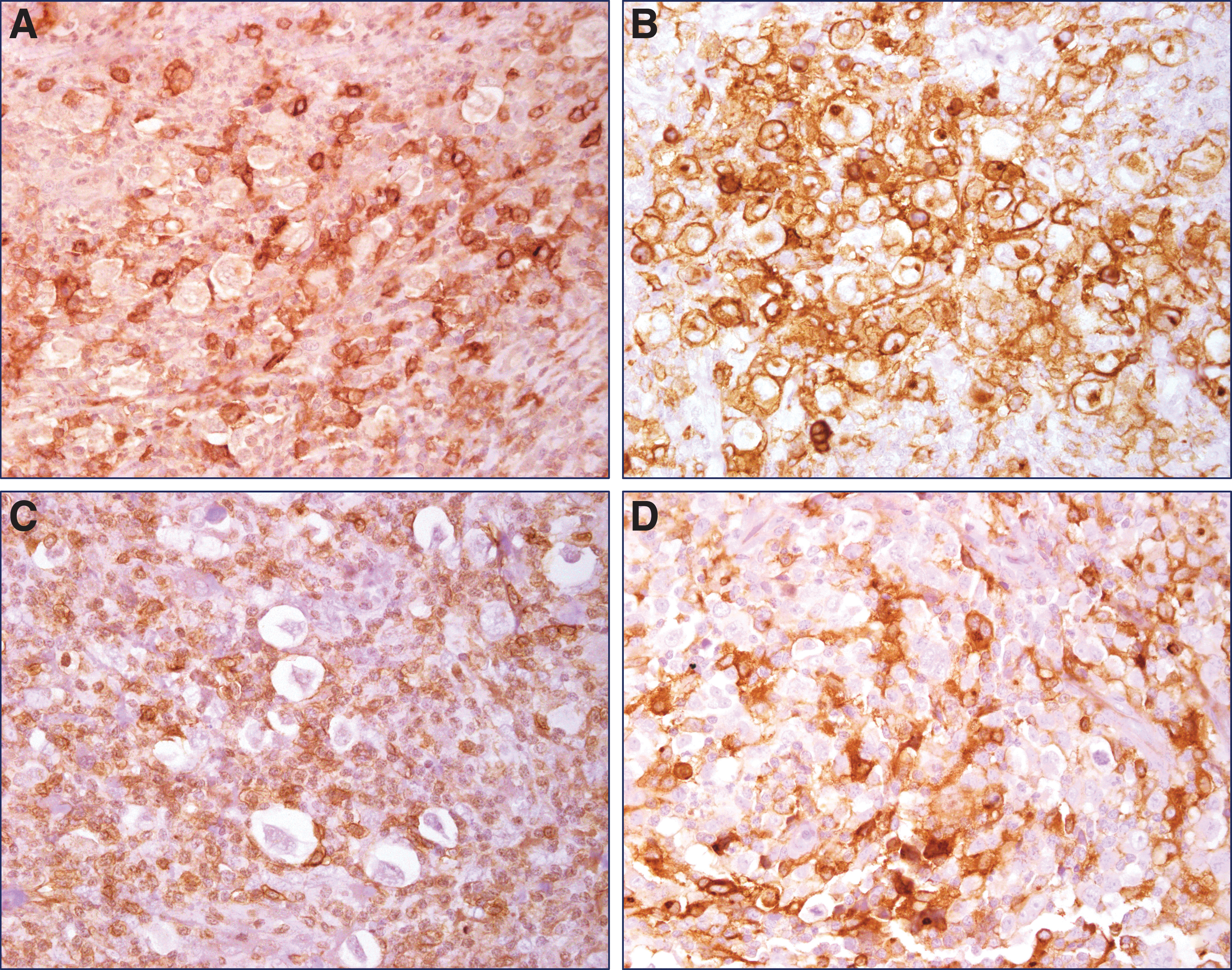
All cases were rich in HRS cells often forming large clusters associated with CD25 positive T cells and macrophages. Only in
Patient Clinical Features and 90Y-Daclizumab Treatment
Removed from protocol for noncompliance with treatment plan.
CT, computed tomography; ABVD, doxorubicin, bleomycin, vinblastine, dacarbazine; XRT, radiation therapy; CR, complete response; ICE, ifosfamide, carboplatin, etoposide; PR, partial response; GV, gemcitabine, vinorelbine; EPOCH-RC, etoposide, prednisone, vincristine, doxorubicin, cyclophosphamide, Revlimid, alemtuzumab; SD, stable disease; EPOCH, etoposide, prednisone, vincristine, adriamycin, cyclophosphamide; IGEV, ifosfamide, gemcitabine, vinorelbine; GemOx, gemcitabine, oxaliplatin; HD Dex, high dose dexamethasone; CCNU, lomustine; CDDP, cisplatin; VP-16, etoposide, GemOx (Gemcitabine, Oxaliplatin); HD Dex: high-dose dexamethasone; PD, progressive disease; LN, lymph node.
Three patients received a single dose of 564.6–574.6 MBq 90Y-daclizumab (day 15), followed by high-dose beam chemotherapy (beginning day 6) with ASCI performed on day 0. One patient received 2 doses of 90Y-daclizumab 6 d apart (days 56 and 15), followed by high-dose chemotherapy (beginning day 6) ASCT day 0.
Patients 1, 2, 3, and 6 completed their protocol prescribed treatment without experiencing DLT or severe or unexpected adverse events (AEs). As seen in Table 3, the spectrum and severity of AEs were generally mild, the vast majority grade 1 or 2 and consistent with the safety profile of most patients with HL undergoing ASCT. All but one patient had bone or back pain related to their high-dose G-CSF stem cell mobilization. Patients 2 and 4 had grade 2 pain related to research biopsies of tumor-involved lymph nodes post-90Y-daclizumab infusion. All patients had grade 1 pain related to sites of disease and interestingly 3 of the patients had slight flare of pain after their 90Y-daclizumab infusions. All the patients had the common BEAM-related nausea, vomiting, and other gastrointestinal AEs. Three of the patients had cutaneous reactions to the plerixafor or KGF.
Adverse Events
AE, adverse event; CP, chest pain.
Patient 6 had two less common, more serious but not unexpected, grade 3 AEs. The first event was catheter-related (strep mitis) bacteremia that occurred during her period of neutropenia after her BEAM treatment. The patient's central venous catheter was removed, she began empiric antibiotic treatment and her bacteremia cleared quickly. She completed a 2-week course of appropriate antibiotics without sequelae or complications. This patient was also noted to have irregular periods after completing her protocol requiring 1 year of Depo-Provera birth control, and developed amenorrhea and increasingly frequent “hot flashes” at the 18-monthposttransplant evaluation. Hormonal analysis at this time showed elevated luteinizing hormone (LH), follicle-stimulating hormone (FSH), and low serum estradiol levels. The patient remained amenorrheic and continued to have intermittent hot flashes through her year 2 follow-up visit and repeat hormonal analysis showed the same pattern that was consistent with premature ovarian failure (POF). The patient was started on replacement calcium, vitamin D, and daily Levonorgestrel/Ethinyl Estradiol and had serial analysis of LH, FSH, and serum estradiol levels. At her 4-year follow-up visit the patient reported return of intermittent menses in the previous 2 months. Repeat hormonal analyses showed a dramatic decrease in her LH, FSH levels, and very elevated serum estradiol level (>100 pg/mL) indicating return of ovarian function. At her 4.5-year follow-up visit, the patient reported continued improvement toward more regular menses and laboratories again indicated return of ovarian function. There were no instances of serious infection or febrile neutropenia that occurred during the 90Y daclizumab treatments or associated with the myeloablative BEAM chemotherapy.
Immune response to daclizumab
None of the patients had baseline human anti-human antibodies (HAHA) to daclizumab nor did they develop them after treatments.
Hematopoietic recovery and hospital discharge
Given their significant prior treatment history and the nature of the protocol treatment, significant, at least transient, trilineage cytopenias were expected. All patients had brief periods of absolute neutropenia following their BEAM chemotherapy. Hemoglobin (Hgb) was also affected with grade 3 anemia (Hgb <8 g) occurring in 3 of these 4 patients (nadirs 7.4, 7.2, 9.4, and 6.9 g) with the two lowest nadirs occurring in patient 2 and 5 who were already anemic at the start of treatment. Platelet counts nadired at 10,000/μL or lower in the week after the subcutaneous infusion. However, as shown in Table 4 below, there was no evidence that 90Y daclizumab had any significant negative impact on hematopoietic recovery with 11 (range 10–12) d being the median time to recovery of absolute neutrophil count to >500/μL and 10 (range 8–11) d being the median time to recovery to untransfused platelet count >20, 000/μL for the 4 patients who completed their planned protocol treatment and had their SCT. The patient's rapid recovery from their treatment is reflected in the timing of their discharge from hospital being essentially 2 weeks after receiving their SC infusion.
Hematopoietic Recovery and Hospital Discharge
ANC, absolute neutrophil count.
Response to treatment
The pattern of response assessment by CT scans and PET scans showed a similar pattern for the 4 patients who are evaluable for response (Figs. 2 –4). All had sizable or bulky lesions that began to shrink promptly in their regular posttreatment restaging CT scans. As seen in Table 5, all 4 patients had very significant shrinkage in the index lesions (61%–87% decreases) in the 12–24 months after treatment that plateaued, leaving small residual masses at the site of their larger metastatic lesions. The first post-ASCT treatment FDG PET scan showed dramatic resolution of many sites of disease, although a few sites still had increased FDG that eventually resolved. “No active lesions” PET scans occurred between 30 and 48 months after treatment.
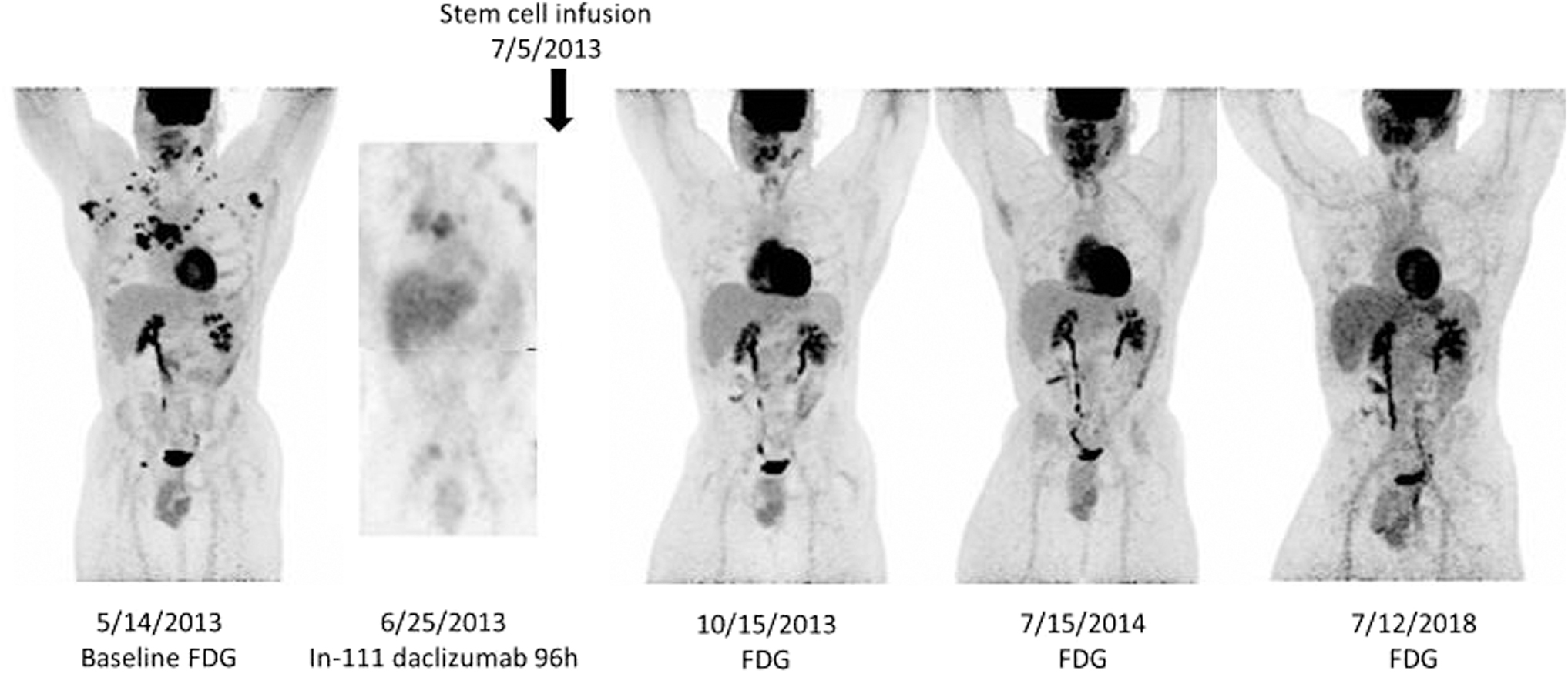
FDG study (not shown) with evidence of hypermetabolic lesions consistent with lymphoma in nodal sites above the diaphragm including right, left cervical (SUVmax12.9), right and left axillary (SUVmax 17), mediastinal (SUVmax 22.5), right inguinal, lung (SUVmax 19.8) and sternum (SUVmax 15.2). Post-treatment 111In-daclizumab maximum intensity projection image from SPECT study obtained on 6/25/2013, 4 days after injection of ∼185 MBq of 111In-daclizumab that was co-infused with 564.6 MBq of 90Y-daclizumab uptake in bilateral cervical, bilateral axillary, mediastinum, lung, and right inguinal, corresponding to sites seen on baseline FDG, although somewhat less obvious given the lower resolutions of SPECT. Post 90Y-daclizumab and post autologous stem cell transplant treatment a follow-up FDG scan obtained October 15, 2013 shows that resolution of uptake in all the lesions with exception of some residual uptake in left cervical region (SUVmax 7.99) that was either residual disease or inflammatory. FDG PET CT of July 15, 2014 shows residual left cervical uptake that was slightly less than the October 15, 2013 scan that given the lack of increase in size or uptake was probably nonmalignant, also nonspecific low level bilateral hilar uptake was also noted. The last scan of December 12, 2018 did not show any abnormal hypermetabolic sites suspicious for lymphoma. Note that nonspecific FDG uptake is noted in the thyroid in all post treatment FDG scans, probably reflecting inflammatory/autoimmune disease. SUV, standardized uptake value.
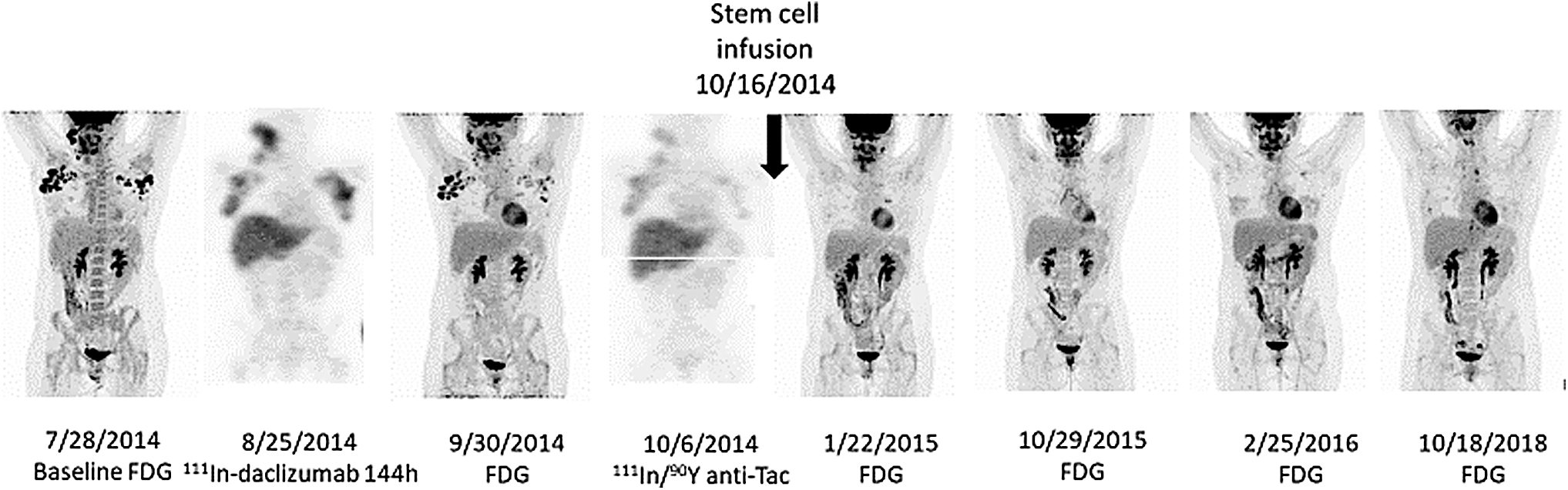
Patient (number 6) Baseline FDG PET CT on July 28, 2014 shows hypermetabolic lesions consistent with lymphoma in right cervical (SUVmax 24.1), right axillary (SUVmax 21.3), and left axillary (SUVmax 20.6). 111In-daclizumab co-administered with 580.9 MBq of 90Y-daclizumab on August 25, 2014, shows uptake in right cervical and bilateral axillary nodules. The 9/30/2014 post initial treatment FDG shows decreased but persistent abnormal uptake in right cervical (SUVmax 7.3) and right axillary (SUVmax 18.0) and left axillary nodes (SUVmax 6.6). A repeat administration of 111In-daclizumab co-administered with 566.1 MBq of 90Y-daclizumab on October 6, 2014 shows persistent uptake in right cervical and bilateral axillary nodes that while decreased from previous was still present. A FDG on January 22, 2015 post second treatment with 90Y-daclizumab and BEAM plus transplant shows resolution of right cervical node, nonspecific uptake in left cervical node, bilateral axillary nodes and left hilar node. Follow-up FDG on October 29, 2015 shows uptake in right cervical that was suspicious for lymphoma and nonspecific minimal bilateral axillary uptake. The February 25, 2016 FDG scan shows persistent right cervical uptake and nonspecific axillary nodal uptake. FDG on October 18, 2018 shows nonspecific right cervical and right axillary node uptake with no evidence of FDG avid lymphoma. BEAM, carmustine, etoposide, cytarabine and melphalan.

Patient (number 3) Baseline FDG PET CT study on June 17, 2013 shows abnormal hypermetabolic lesion in right axilla (SUVmax 14.3), mediastinum (SUVmax 12.5), right supradiaphragmatic (SUVmax 11.2), retroperitoneal (SUVmax 12.2), splenic (SUVmax 7.4) and left proximal femur (SUVmax 8.0). Uptake in the left submandibular area is nonspecific (SUVmax 4.83). 111In-daclizumab co-administered with 574.6 MBq of 90Y-daclizumab shows uptake in the right axilla, mediastinum, retroperitoneum, splenic focus, and left proximal femur. Lesion in the liver was not identified, cervical region is out of the fie ld of view. Follow-up FDG scan on November 12, 2013. ∼3.5 months later, shows increased abnormal uptake in left cervical region and resolution of axillary, mediastinal, supradiaphragmatic, retroperitoneal lesions and probable resolution of left proximal femoral lesion. FDG scan of August 14, 2014 shows unchanged persistent left cervical node, very mild nonspecific uptake in axillary and inguinal nodes, bilateral hilar nodes. clara ra called RUL nodule on this and prior. Follow-up FDG scan of August 13, 2015 shows persistent uptake in the left cervical node and minimal nonspecific unchanged uptake in bilateral hila. FDG of July 28, 2016 shows persistent left cervical node uptake and some mild non-specific uptake in bilateral axillary nodes hila. FDG of July 19, 2018 shows nonspecific bilateral axillary and hilar uptake with no sites of abnormal uptake suggestive of lymphoma.
Summary of Radiographic Findings
All the patients had a somewhat evanescent or random pattern of transiently increased standardized uptake value at known sites of disease after apparent normalization of these previously involved areas that made it impossible to assess the patient as a CR. However, given the highly refractory nature of their HL at the start of protocol treatment and the absence of regrowth of previous sites of disease or new lesions and consistently diminishing sites in restaging PET scan has led us to assess all 4 patients as CRs now ranging 4.5 to nearly 8 years post autoSCT.
Discussion
The standard treatment for relapsed and primary refractory HL is salvage chemotherapy, followed by high-dose chemotherapy and autologous stem cell transplantation, which has shown a 5-year progression—survival of ∼50%–60%. 30 –34 A series of diverse clinical prognostic factors such as those used in the present study have been useful in predicting prognosis in refractory and relapsed HL patients. Freedom from ASCT failure in the presence of 0, 1, 2, or 3 factors have ranged between 45%–93%, 27%–59%, and 10%–18%, respectively. 35 –37 All of these patients had at least one factor.
A large number of monoclonal antibodies have been approved for the therapy of cancer. 23 The CD30 antibody/drug conjugate brentuximab vedotin and the PD-1 directed antibodies nivolumab and pembrolizumab are highly efficacious in treating relapsed and/or refractory HL. 9 –11,38 In a pivotal phase II study of brentuximab vedotin for patients with relapsed or refractory HL, objective responses were induced in 75% of patients with complete remissions in 34% of patients. 38 The median progression-free survival of all patients was 5.6 months and the median duration of response for those in CR was 20.5 months. The most common treatment-related AEs were peripheral sensory neuropathy, nausea, fatigue, neutropenia, and diarrhea. On March 20, 2018, brentuximab vedotin in combination with chemotherapy was granted FDA approval to be used in adult patients with previously untreated stage III or IV classical HL.
Preclinical studies suggested that HRS cells exploit the PD-1 pathway to evade immune detection. In classic HL alteration in chromosome 9p24.1 increased the abundance of PD-1, ligands, PD-L1, and PD-L2 and promote their induction through Janus kinase (JAK)-signal transducer and activator of transcription (STAT) signaling. 39 PD-1 blockade with nivolumab in relapsed or refractory HL of 23 studied patients after relapse following autologous stem cell transplantation and/or following receipt of brentuximab vedotin was associated with an objective response in 27 patients (87%), including 17% with a CR and 70% with a PR. 11 The remaining 3 patients (13%) had SD. The rate of progression-free survival at 24 weeks was 86%.
Although these studies change the landscape for classical HL management, in 2018 ∼ 1000 patients with HL died of their disease. 1 In particular, a significant proportion of patients with HL will not respond or will relapse. The arming of monoclonal antibodies by linking them to cellular toxins or radionuclides is to target these agents specifically to tumors. 3,9,10,12 –18,23,40 –50 One advantage of the use of a radiolabeled monoclonal antibody conjugate for therapy over unmodified monoclonal antibodies or monoclonal antibodies linked to toxins is that with the appropriate choice of radionuclide radiolabeled antibodies can kill cells at a distance of several cell diameters and thereby make targets of the antigen-negative tumor cells adjacent to antigen-expressing normal cells.
Various monoclonal antibodies with different antigenic targets have been employed to deliver targeted RIT. 3,14 –18,23,40 –50 In an effort to evaluate RIT as part of the salvage regimen pre-ASCT, there have been a number of trials of 90Y ibritumomab tiuxetan (Zevalin anti-CD20), followed by BEAM-conditioning regimen and autologous hematopoietic stem cell transplantation (ASCT) in relapsed and refractory high-risk B cell non-HL. In each of the studies, the combined use of RIT with BEAM plus autologous stem hematopoietic cell transplant was feasible with acceptable toxicity even in elderly and heavily pretreated patients. However, with the exception of one case that showed borderline efficacy, the addition of 90Y did not confer a further survival benefit when compared with rituximab added to BEAM and autologous hematopoietic stem cell transplant.
The current study used daclizumab (humanized anti-Tac, anti-CD25) armed with the energetic β′-particle emitter 90Y. Daclizumab targets the 55kDa/IL-2R (CD25) subunit that is constitutively expressed on Treg cells, but not on other resting normal cells. 19,51 In contrast, CD25 is overexpressed on certain lymphoid malignancies, including select patients with anaplastic large cell lymphoma, adult T cell leukemia/lymphoma, chronic lymphocytic leukemia, cutaneous T cell lymphoma, Hairy cell leukemia, and in HL. 21,51 Unmodified murine anti-CD25 was evaluated in a trial involving patients with adult T-cell leukemia. Seven of 19 treated patients responded to the antibody. 19,51 In a subsequent trial 9 of 16 evaluable patients with ATL responded to 90Y-labeled murine anti-CD25 . 8,
Subsequently, 46 patients with relapsed or refractory HL received 370–555 MBq of 90Y-daclizumab every 6–10 weeks for up to 7 doses. 3 Among the 46 patients treated with multiple doses of 90Y-daclizumab 14 achieved a complete remission and 9 manifested a PR. In a separate study of unconjugated antibody using saturating amounts of daclizumab in 22 patients with Hodgkin's disease, there were no PRs or CRs. 3 Freedom from disease progression in the 90Y-daclizumab-treated patients ranged from 28 to 788 d with a median response duration of 151 d (range 28–720 d). Median CR duration was 328 d not counting the period in the PR. Thus, although 14 patients manifested a CR, the lack of cures indicated that monotherapy with this agent was not optimal.
Given the 50% response rate achieved with 90Y-daclizumab RIT in a heavily pretreated population, the authors sought to improve the long-term disease-free survival achievable with ASCT by incorporating escalating doses of 90Y-daclizumab into the preconditioning regimen that included high-dose chemotherapy with carmustine, etoposide, cytarabine, doxorubicin, and melphalan (BEAM). They hypothesized that this use of an autologous hematological stem cell transplant using cells harvested from the patient before the administration of 90Y-daclizumab should permit an escalation of 90Y-daclizumab doses because the hematological stem cell transplant should ameliorate the otherwise dose-limiting hematological toxicity of the radiolabeled anti-CD25 monoclonal antibody. Furthermore, they hoped that use of the nonirradiated stem cell transplant would reduce the incidence of the development of MDS.
The spectrum in severity of AEs were mild with 90Y-daclizumab plus ASCT in HL (Table 3). The only serious AE observed during the trial was transient POF, an expected complication of stem cell transplant that is more common in patients who have had multiple treatment regimens for their cancers, so it is not possible to determine the possible contribution of 99Y-daclizumab treatment to this AE. There were 6 MDS in the previous study of 46 patients. 3 These 6 occurred in the 30 patients who had not had a cytogenetic study of bone marrow specimens before initiation of systemic RIT, whereas none of the 16 patients after such analysis developed this disorder. Although the present study is too small to draw meaningful conclusions, the fact that only one or two doses of 90Y-daclizumab rather than up to seven, as in the previous study, as well as the fact that autologous stem hematopoietic cell transplant of unirradiated bone marrow was provided after the 90Y, may be factors in reducing this complication. Nevertheless, a subsequent clinical trial should require pretreatment cytogenetic studies of bone marrow specimens before initiation of systemic RIT.
In contrast to the fact that none of the 46 patients in the previous study, including the 14 patients that manifested a CR were cured of their HL by the administration of 90Y-daclizuamb alone, all 4 of the patients in the present study who received 90Y-daclizumab in high-dose BEAM therapy autologous hematopoietic stem cell transplant remain in CR 4.5 to almost 8 years following therapy. In previous studies 50%–60% of patients with refractory and relapsed HL receiving an autologous hematopoietic stem cell transplant alone achieved a sustained CR. 30 –34 In the present study, responses were observed both in the patient whose HRS cells expressed CD25 and the remainder whose neoplastic cells were CD25 negative; thus the daclizumab was directed primarily not at the tumor cells themselves but toward nonmalignant Treg cells rosetting around the HRS cells.
Yttrium-90 provided strong β′-emissions that killed antigen-nonexpressing tumor cells at a distance by a crossfire effect. Furthermore, the strong β′-irradiation killed normal cells in the tumor microenvironment that nurtured the malignant cells in the lymphomatous mass. In addition, the ionizing radiation increases the generation of tumor-associated antigen and neoantigens as well as increasing expression of MHC molecules and antigen presentation suggesting that it might be of value to combine RIT with murine checkpoint blockers. Therefore, the 90Y-daclizumab infusions may provide meaningful therapy for select HL patients. The encouraging results of the present study support future similar studies of 90Y anti-CD25 monoclonal antibody into the BEAM, ASCT preconditioning regimen.
Footnotes
Acknowledgments
The study was performed under the conditions of the Helsinki accords. All patients signed a written informed consent for participation in clinical studies. Clinical studies were approved by the Intramural Review Board of the National Cancer Institute.
Author Contributions
Concept and design: T.A.W., K.C.C., C.S., R.G., M.W.B., and J.A.C. Development of methodology: J.A.C., M.W.B., and T.A.W. Acquisition of data (managed patients' administration of 90Y-daclizumab): K.C.C., C.S., D.H.F., C.C.C., M.A.W., and T.A.F. Analyses and interpretation of data: T.A.W., K.C.C., M.D.M., J.A.C., and K.A.K. Writing review and or revision of article: T.A.W., K.C.C., M.D.M., M.W.B., and J.A.C. Administrative, technical, or material support (i.e., reporting or organizing data): E.M.C. and B.R.B. Study supervision: T.A.W. and K.C.C. Other (acquired photomicrograph images of histology slides, manufacturing and testing of IL-15): J.H.L., C.H.P., and S.P. All coauthors have reviewed and approved for publication of the article before submission.
Disclosure Statement
The authors declare no potential conflicts of interest.
Funding Information
This work was supported by the Intramural Research Program of the Center for Cancer Research, National Cancer Institute, NIH.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.