
Abstract
Objective:
To prevent postoperative relapse after HOLRBT, we compared postoperative adjuvant therapies.
Methods:
One hundred fifty patients with non-muscle invasive bladder cancer (NMIBC) were meanly divided into three groups: A, B, and C. Group A patients only took sunitinib, group B patients underwent TGC perfusion chemotherapy, and group C patients took sunitinib and underwent TGC chemotherapy.
Results:
It was discovered that TGC perfusion chemotherapy combined with taking sunitinib can significantly reduce the relapse rate. Most of the tumor relapse period was assembled at 9 months after the operation. No-tumor relapse survival rate and no-fluorescence in situ hybridization positive survival rate in Group C were significantly higher than those of Group A and Group B.
Conclusion:
Therefore, the combined application of taking sunitinib drug and going through TGC perfusion chemotherapy after secondary HOLRBT will evidently improve the prognosis of patients with a glorious applicated prospect.
Introduction
Bladder cancer is one of the most common malignant tumors that threaten human health in the urinary system, whose morbidity and mortality are rising gradually every year. The American Cancer Association workers have made a precise prediction that the quantity of new bladder cancer cases and death patients in 2018 are 81,190 and 17,240, respectively. 1 In recent years, an upward trend has also been seen in the incidence and mortality of bladder cancer in China. 2 Non-muscle invasive bladder cancer (NMIBC) accounts for 70% of patients with newly diagnosed bladder cancer. 3 NMIBC has such following characteristics as a high incidence, multiple occurring sites, and prone to occult lesions, such as carcinoma in situ (cis). It is easy to relapse after operations and is inclined to drug resistance after perfusion chemotherapy. 4
Currently, the commonly utilized NMIBC surgical method is transurethral resection of bladder tumors (TURBT). Its recurrence rate at 1 year after surgery is 20%–60%, whereas the 5-year recurrence rate is 31%–75%. Both Holmium laser resection of bladder tumors (HOLRBT) and transurethral resection of bladder tumors (TURBT) are the most common surgery for NMIBC. TURBT is widely implemented in clinical practice, with a certain probability of bleeding and bladder perforation. However, there are some advantages in hemostasis, reducing surgical trauma and postoperative obturator nerve reflex as well as bladder perforation, by HOLRBT working under continuous wave mode. 5
Sunitinib is a novel, multitargeted, tumor-treating oral drug that selectively targets certain protein receptors, inhibiting cancer growth and blocking blood and nutrients required for tumor proliferation. It is extensively used in solid tumors, such as renal carcinoma, gastrointestinal stromal tumor, lung cancer, liver cancer, etc. Eto, Masatoshi et al. 6 reported the role of sunitinib in the development of drug-resistant bladder cancer. Paclitaxel, combined with cisplatin and gemcitabine (TGC), is often used for antitumor chemotherapy postoperatively, with satisfying results in bladder cancer. However, there are currently few targeted drugs for bladder cancer, and seldom reports about traditional and chemotherapeutic drugs are related to single or combined targeted drugs. For this article, the efficacy of sunitinib and TGC chemotherapy alone or combined for relapsed NMIBC is carefully evaluated to seek the optimal clinical regimen for bladder cancer that could alter the prognosis.
Methods
Overall, 150 NMIBC cases were collected from March 2016 to March 2017 in our hospital. After the tumor stages and grades were evaluated, all patients were distributed into three groups with the double-blind, randomly digital table method: A, B, and C. All patients underwent HOLRBT twice. Group A patients took oral sunitinib, a targeted drug therapy, Group B patients postoperatively received TGC perfusion chemotherapy, and Group C patients received both sunitinib and TCG perfusion chemotherapy, combined double treatment. Computed Tomography (CT) was used to re-examine relapse and complications, and then, we conducted a 2-year follow-up and prognostic analysis.
Inclusion criteria: (1) patients with first diagnosis and surgical treatment; (2) NMIBC patients were confirmed by preoperative CT and cystoscopy or postoperative pathological slices; (3) patients with no preoperative acute hepatitis, autoimmune disease, and immunosuppressive treatment history; (4) patients with no other chronic inflammatory diseases, such as chronic pneumonia preoperatively; (5) patients with no other malignant tumors preoperatively; (6) patients with no radiotherapy and chemotherapy before surgery; and (7) patients with complete medical records and voluntary signature on the informed consent form. Exclusion criteria: (1) patients with kidney disease and positive urine protein; (2) patients with other urinary tumors except bladder cancer; (3) patients with unexplained gross hematuria (electrophoresis); (4) patients inflicted with severe urinary infections; (5) patients with primary diseases, such as liver, kidney, brain, and hematopoietic system; and (6) patients who underwent organ transplantation and blood transfusion.
Ethical approval: Our study was approved by the Ethics Committee of Liaocheng People's Hospital. The tumor stages of all patients were based on the 7th Edition of TNM stages method in 2009 launched by the Union of International Cancer Control (UICC). Superficial bladder cancer and NMIBC include three stages, Tis, Ta, and T1; whereas muscle invasive bladder cancer (MIBC) includes above T2 stages. The pathological grade of bladder cancer was determined according to 2016 classification criteria by the World Health Organization (WHO): (1) low-grade malignant urothelial papilloma, (2) low-grade urothelial papillary carcinoma, and (3) high-grade urothelial papillary cancer.
HOLRBT two times: The patients kept the lithotomy position, and epidural anesthesia was administered to them. The operator placed the cystoscopical operation scope through the urethra into the bladder, rinsing with 0.9% sodium chloride solution, to determine the tumor position. Then, the holmium laser fiber was placed through the cystoscope operating hole into the bladder, with the parameter setting as follows: laser energy 1.0–2.0 J, frequency 15–20 Hz, and power 20–40 W. Then, the krypton laser fiber was moved close to the tumor. At a 1-cm border distant from the tumor, the lesion was cut by a push-type mode through the muscle layer, lifting the tumor tissue together functioning by water flow.
In addition to removing the tumor tissue, it was also quite essential to remove the normal mucosal tissue within 2 cm around the tumor. At the end of the operation, the resected tissue was flushed out with an irrigator and the F22 three-chamber balloon catheter was placed for anti-infective drug infusion by it. The catheter was obtained 3–6 d after surgery. The secondary HOLRBT was performed 4 weeks after the first one; all visible tumors, primary electric scar, and edema area were fully excised, deeply removing them till the bladder serosal layer. Groups A, B, and C patients were administered targeted drugs or perfusion chemotherapy was performed according to the instructions after secondary HOLRBT. Cystoscopy, urinary fluorescence in situ hybridization (FISH), blood biochemistry, and blood routine examination were performed every 3 months, maintaining for 2 years. If a suspicious lesion was found, it would be confirmed through pathological biopsy.
Observed indicators include: Hospitalized evaluation indicators: operation time, hospitalization time, number of postoperative bladder irrigation, catheter indwelling time Adverse drug reactions: urinary tract irritation, myelosuppression, renal dysfunction, gastrointestinal reactions Relapse: All patients were followed up for 2 years, whose frequency was every 3 months. It was necessary to re-examine CT, blood and urine regular test, liver and kidney function, B-ultrasound, and urinary FISH. Postoperative no-tumor relapse survival rate was compared among three groups, and immunofluorescence hybridization in situ (FISH) was for the no-positive relapse survival rate.
Statistical analysis
SPSS 17. 0 software was used for normal statistical analysis. Counting data were expressed as cases and percent, whereas the χ 2 test was used to compare between three groups. Kaplan–Meier survival analysis was utilized to assess patient survival rate, and the log-rank test was performed for data; p < 0.05 indicated statistically significant differences.
Results
General data
General data pertained to all research subjects, including gender, age, smoking, tumor size, number, stages, grades, etc. There was no distinct discrepancy in clinically pathological features between three groups of patients (p > 0.05, Table 1).
Clinical Basic Pathological Features of Three Groups of Patients (n,%)
Hospitalization indicators
The surgery proceeded successfully, no serious complications occurred during the operation, there was no serious bleeding and no blood transfusion, and tumors were completely removed with the naked eye. The initial HOLRBT operation time was 15–50 min, on average 30 min; the bleeding volume was 10–70 mL, on average 26 mL; and the hospitalization time was 3–7 d, on average 4.5 d. The postoperative pathological report showed that tumors belong to transitional cell carcinoma, including 71 cases in grade I, 53 cases in grade II, and 26 cases in grade III. During secondary HOLRBT, there were 28.6% residual tumors. Seventy-eight cases were dealt with by conducting a routine bladder flush after operation, whereas the catheter was indwelled for 7–9 d after operation every time. No obvious urine extravasation was found after the operation. Throughout HOLRBT twice, CT was compared with the initial admission CT. The results are shown in Figure 1.

Typical CT for bladder cancer after HOLRBT twice.
Adverse drug reactions
Common Terminology Criteria Adverse Events grade on adverse drug reactions is shown in Table 2. There were 4 cases of urinary tract stimulus syndrome, 2 cases of myelosuppression, 1 case of renal function damage, 2 cases of gastrointestinal reactions, and 2 cases of hand
Common Terminology Criteria Adverse Events Grade on Adverse Drug Reactions, Cases (n)
Relapse
In Group A, there were 13 relapse patients, with a 26% relapse rate. In Group B, there were 12 relapse patients, with a 24% relapse rate. In Group C, there were 3 relapse patients, with a 6% relapse rate. The relapse rate among three groups was statistically significant (A vs. C, B vs. C, p < 0.05, Fig. 2), and there was no significant difference between Group A and Group B (p > 0.05). The tumor relapse periods among three groups mostly occurred at least 9 months after the operation, whose difference was statistically evident (p < 0.05, Fig. 3). There was no statistically evident discrepancy in relapse location between groups (p > 0.05, Fig. 4).
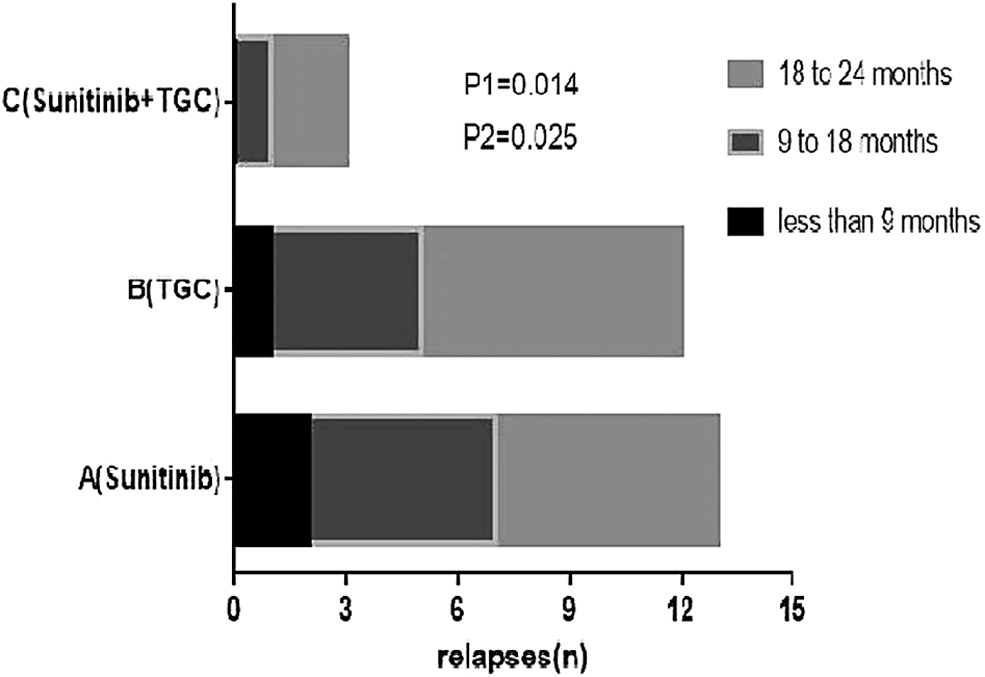
Tumor relapses within 2 years after treatment in three groups of patients. P1: Group A versus Group C; P2: Group B versus Group C.

Comparison of tumor relapses in three groups of patients at different periods. p < 0.05.
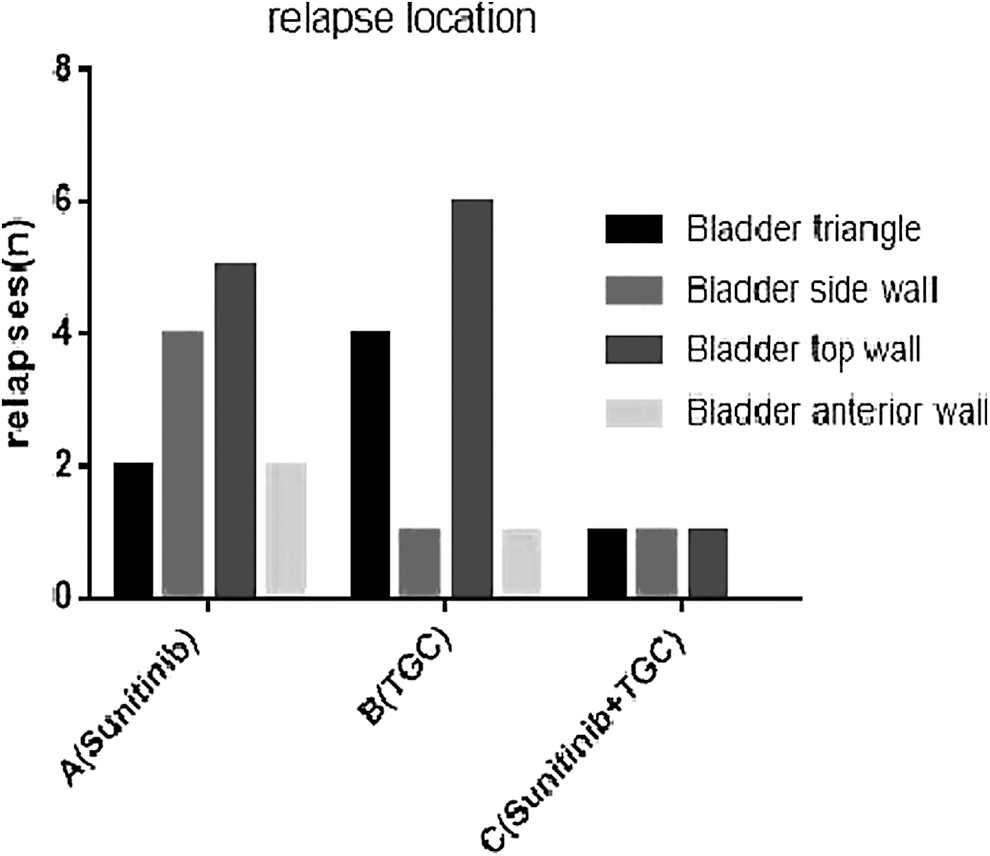
Tumor relapse location in three groups of patients. p > 0.05.
No-tumor relapse survival rate and no-FISH-positive survival rate
No-tumor relapse survival rate (A vs. C, B vs. C, log rank test χ 2 AC = 6.532, χ 2 BC = 8.665, p < 0.05, Fig. 5) and no-FISH-positive survival rate (A vs. C, B vs. C, log rank test χ 2 AC = 7.013, χ 2 BC = 9.183, p < 0.05, Fig. 6) in Group C were significantly higher than those of Group A and Group B.
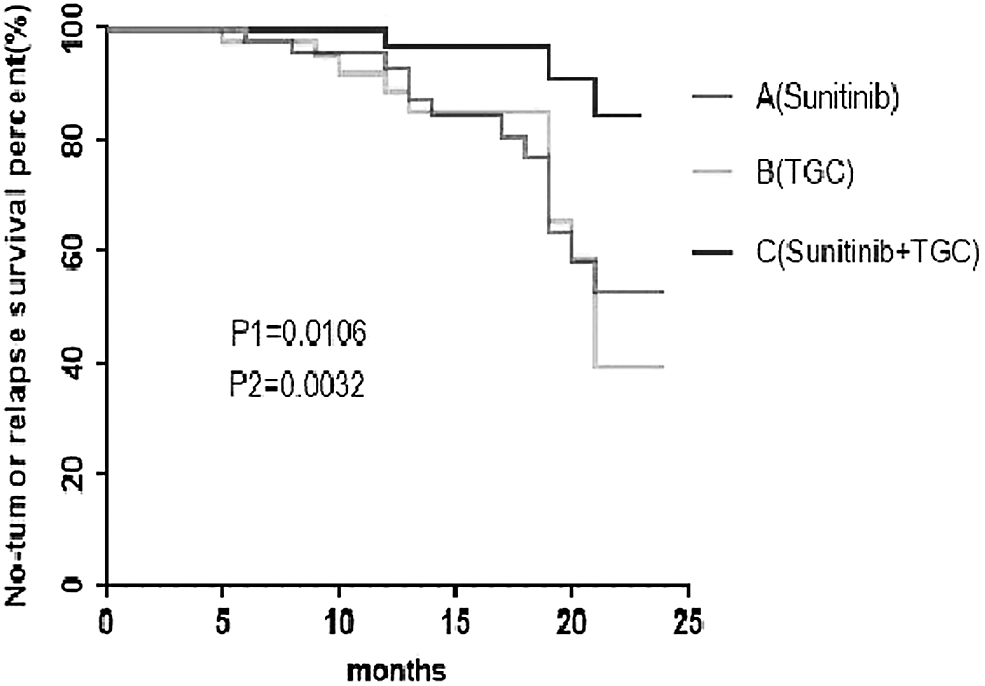
No-tumor relapse survival rate in three groups of patients. P1: Group A versus Group C; P2: Group B versus Group C.
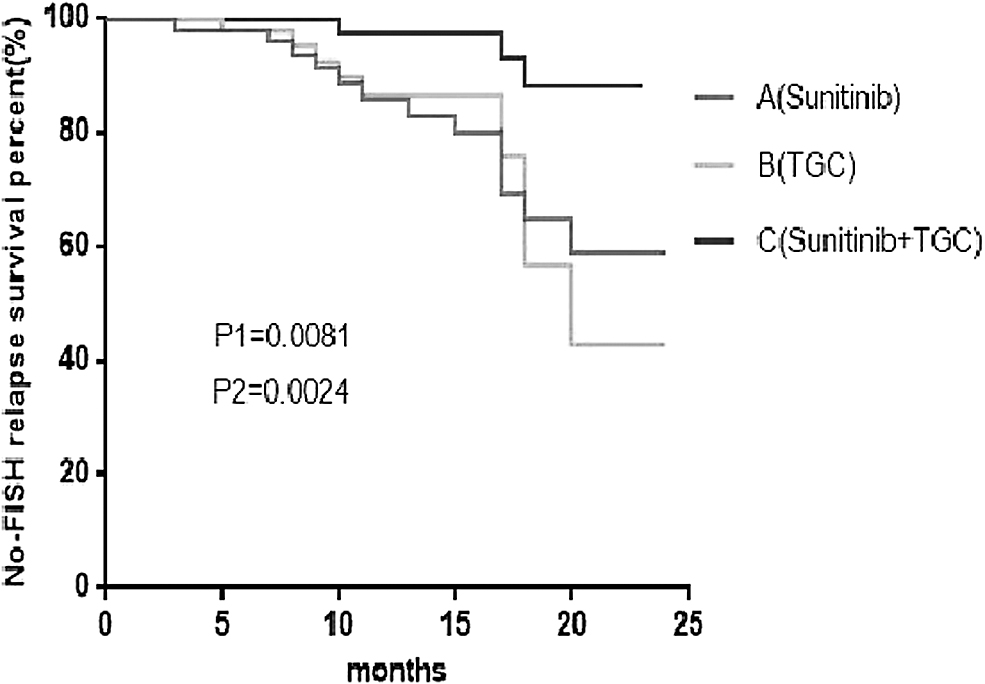
No-FISH relapse survival rate in three groups of patients. P1: Group A versus Group C; P2: Group B versus Group C.
Discussion
According to the invasion depth, NMIBC includes three clinical stages, Ta, T1, and CIS (carcinoma in situ), and myometrial invasive bladder cancer (muscle invasive bladder cancer, MIBC). 7,8 Seventy percent of bladder cancer is NMIBC, 9 whereas 30% is MIBC. 10 At present, TURBT is more commonly used in clinical practice, but it resulted in the relapse rate of patients being as high as 70% during the 5 years, and the percentage of patients with superficial bladder cancer progressing to invasive bladder cancer was as high as 50%–80%. 11 Recently, holmium laser technology is widely carried out as a new means of urinary tumors, taking on glorious clinical application prospects. In 1994, Johnson 12 reported initially that 15 patients with superficial bladder transitional cell carcinoma were treated with holmium laser. No complications occurred after surgery, and no catheter was required after operation. HOLRBT has multiple advantages such as less bleeding, clear surgical vision, short operation time, no obturator nerve reflection, short postoperative hospital stay and catheterization time, and less hospitalization costs.
Holmium laser will destroy cancer cells with vaporization, and it will simultaneously reduce the probability of cancer cells planting. Therefore, the relapse rate after HOLRBT is lower than that of TURBT. The lamina propria of the bladder is very thin in the neck and triangle, and the muscles are very close to the lamina propria. Both aspects may promote tumor relapses. 13 In this study, because of the limited bladder cancer cases, there were no relapse locations found in the three groups, whose difference was not statistically significant (p > 0.05). In this study, HOLRBT twice was applied with a combination of postoperative chemotherapy and targeted drug therapy, to further reduce postoperative relapses of bladder cancer.
Bacille Calmette-Guérin vaccine (BCG), an immunoadjuvant, works toward upregulating cellular immunity and humoral immunity. The urological diagnosis and treatment specification indicate that BCG is the most effective bladder perfusion immunotherapy for bladder noninvasive tumors. Shelley et al. 14 systematically evaluated BCG perfusion therapy to prevent recurrence of NMIBC after TURBT. It was shown that TURBT combined with BCG intravesical perfusion was effective in preventing tumor recurrence compared with TURBT alone.
A meta-analysis by Sylvester et al. 15 was done for BCG intravesical perfusion, preventing progression of NMIBC after TURBT, which showed that TURBT combined with BCG intravesical perfusion was effective in preventing disease compared with TURBT alone. Although BCG displays good effects in the treatment of superficial bladder cancer, long-term perfusion of BCG has significant side-effects, and about 30% of patients will relapse and progress. However, due to purity and safety, it is relatively rare to be used clinically. After bladder infusion treatment, it can often lead to complications such as cystitis, hematuria, fever, granuloma, pneumonia, sepsis, arthritis, joint pain, ureteral obstruction, bladder contracture, etc. Therefore, it has been abandoned in the actual clinical work of our department, replaced by postoperative adjuvant chemotherapy and oral targeted drug therapy.
Chemotherapy for bladder cancer began in the 1960s and 1970s. Most of the early chemotherapy was single-agent chemotherapy, but the effectiveness of single-agent chemotherapy was not very well, with short clinical remission time and patient survival time. Since the 1980s, a combination chemotherapy regimen has been utilized to treat progressive bladder cancer. The current chemotherapy regimen is a cisplatin-based GC regimen (gemcitabine + cisplatin). There are no uniform standards for other second-line regimens, for example, paclitaxel, ifosfamide, oxaliplatin, and pirarubicin. In the past 20 years, a lot of evidence showed that cisplatin-based neoadjuvant chemotherapy has achieved good effects. A multicenter randomized study of the European Organization for Research and Treatment of Cancer (EORTC) has compared cystectomy alone with cystectomy and postoperative adjuvant chemotherapy. The results suggested a 5% increase in survival benefit and a 16% reduction in the risk of death. 16
The main adverse reactions of chemotherapy with GC regimen were myelosuppression and digestive tract reactions, mostly mild to moderate, with no treatment-related deaths. In recent years, EORTC members believe that taxanes may be a first-line treatment for local progression and metastatic bladder cancer. The researchers evaluated the safety and efficacy of paclitaxel combined with cisplatin gemcitabine (TGC). The overall and complete response rates of the program were significantly improved, but there was no difference in overall survival between the two regimens. 17 Most patients are partially relieved after chemotherapy, which is just alleviated syndrome and does not mean prolonged survival. Traditional perfusion chemotherapy often does not take into consideration the multidrug resistance of the tumor, as well as empirical medication, which leads to chemotherapy failure. In this study, we tried the TGC regimen in NMIBC treatment, which can avoid the occurrence of drug resistance to the greatest extent and enhance the effect of chemotherapy.
Sunitinib is a novel molecularly targeted drug that selectively targets multiple receptor tyrosine kinase inhibitors, which function by combining anti-angiogenesis of suspending blood supply to tumor cells with the antitumor mechanism of direct attack on tumor cells. Gallagher et al. 18 evaluated the value of sunitinib as a second-line treatment alone for advanced bladder cancer. Now, there are a few reports about sunitinib in NMIBC. This study found that sunitinib-targeted therapy combined with TGC chemotherapy after HOLRBT twice, compared with sunitinib or TGC infusion chemotherapy alone, can evidently reduce the relapse rate. No-tumor relapse after surgery and No-FISH-positive survival rate in Group C were significantly higher than that of Group A and Group B. Therefore, HOLRBT is a safe and effective approach for NMIBC. If combined with sunitinib-targeted therapy and TGC perfusion chemotherapy after HOLRBT twice, it will evidently reduce tumor relapses and promote the No-tumor survival rate.
Footnotes
Author Contributions
Conceived and designed the experiments: Songjiang Li and Kai Zhao. Collected the patients' information: Yueli Jin. Analyzed the data: Zheng Ma. Wrote the article: Songjiang Li.
Acknowledgments
The authors are grateful for the support of the pathological department for tissue identification and the image department for providing CT photos.
Disclosure Statement
The authors have declared that there is no conflict of interest.
Ethical Approval Statement
The Chinese Food and Drug Administration has granted the hospital concerned the National Drug Clinical Trial Institute qualification, Number 0249. This study was approved by the Hospital Research Ethics Committee. All patients provided written informed consent before enrollment in the study.
Funding Information
No funding was received for this article.