
Abstract
Thorium-227 (227Th) is a long-lived (T1/2 = 18.7 d) α-emitter that has emerged as candidate for radioimmunotherapy. Imaging of patients treated with thorium-227 conjugates is challenging due to the low activity administered and to photon emissions with low yields. In addition, the radioactive daughter radium-223 (223Ra) have photon emissions in the same energy range as 227Th. The long half-life of 223Ra (T1/2 = 11.4 d) and the possibility of redistribution motivates efforts to separate 227Th and 223Ra. The aim of this study was to investigate the feasibility of imaging of patients treated with 227Th-labeled-monoclonal antibody (mAb) and to determine acquisition and image processing parameters to enable discrimination between 227Th and 223Ra. Imaging was performed with a GE Discovery 670 NM/CT γ-camera. Radionuclide separation with different energy windows (EW) and collimators was studied in images of vials with either 227Th or 223Ra. Phantom acquisitions with clinically relevant activities were performed to assess image quality and the usefulness of background subtraction and spatial filtering. Two patients treated with 227Th-labeled-mAb were imaged. Imaging of vials showed that 223Ra can be distinguished from 227Th using multiple energy windows. Medium- and high-energy collimators showed similar performance of sensitivity and spatial resolution, whereas the low-energy collimator had higher sensitivity but poor resolution due to collimator penetration. Visually, the image quality was improved with background subtraction and spatial filtering. The patient images exhibited the expected image quality and a possibility to separate 227Th and 223Ra. γ-Camera imaging of patients treated with 227Th-mAb is feasible and 223Ra can be distinguished from 227Th. Image quality is substantially improved using background subtraction and a spatial smoothing filter. Acquisition settings recommended for planar images are: high-energy general purpose or medium-energy general purpose collimator, 40 min acquisition time and energy windows: (1) 70–100 keV (227Th and 223Ra); (2) 215–260 keV (227Th); (3) 260–290 keV (223Ra); (4) 350–420 keV (223Ra).
Introduction
Radionuclide therapy has an important role to play in the treatment of both local and metastatic malignancies and new radiopharmaceuticals are being evaluated for new indications. Alpha emitters are, given their high linear energy transfer and short path length, a group of radionuclides that are theoretically attractive for radionuclide therapy. The introduction of 223RaCl2 (Xofigo©)—a salt solution containing the α-emitter radium-223 (223Ra)—in the treatment of prostatic cancer has been successful, and multiple clinical studies are currently ongoing.
Thorium-227 (227Th) is another α-emitter that recently attracted clinical interest in radioimmunotherapy. It has beneficial labeling properties, and its half-life (18.7 d
1
) is a good match to the uptake and clearance rate of humanized monoclonal antibodies (mAbs). Human phase I clinical trials targeting lymphoma, mesothelioma, and prostate cancer (see, e.g.,
γ-camera imaging of patients after administration of 227Th is further complicated by the fact that the decay of 227Th is equivalent to production of the radioactive daughter 223Ra which has a physical half-life (11.4 d2) that is sufficiently long to allow for anatomic redistribution and excretion before it decays. Radium-223 decays in six steps by α- and β-decay to 207Pb, with a maximum half-life of 36 min for the 211Pb → 211Bi transition (Table 1), resulting in multiple photon emissions with relatively low emission probability over a wide energy range (Table 2). The photon emission spectrum originating from the decay of 223Ra and its daughters overlaps with the spectrum from 227Th when measured with conventional γ-camera systems, due to the limited energy resolution of the NaI(Tl) detector. A γ-camera image relying on a single energy acceptance window will have contributions from both 227Th and 223Ra (including the short-lived daughters), and will not provide information on the distribution of the individual nuclides. Considering that 223Ra ions released in the decay of 227Th labeled to a mAb, will have a completely different biodistribution and pharmacokinetics, it is important to develop imaging methods that can distinguish between the individual nuclides.
Decay Data for 227Th and Its Daughters
Ra, radium-223; 227Th, thorium-227; NA, not applicable.
Principal Photon Emissions (Energy >75 keV, Probability >2%) of 227Th and Its Daughters
Compound emission of photons in the energy range 80–103 keV. The listed energy and probability is the weighted mean energy and summed probability, respectively.
Compound emission of photons in the energy range 94–98 keV.
Ra, radium-223; 227Th, thorium-227.
This work has been performed in the context of a phase I clinical trial (NCT02581878), in which patients receive a mAb targeting CD22 labeled to 227Th (BAY1862864) for treatment of non-Hodgkin's lymphoma. Considering the very low activity administered to the patients, that is, 1.5 MBq 227Th for patients in the first cohort, the aim of this work was to investigate the feasibility of acquiring γ-camera images with meaningful image quality, with special emphasis on distinguishing 227Th from 223Ra. Phantom measurements were performed to establish suitable energy windows (EW), the optimal choice of collimator, and image processing parameters, including correction for background radiation. The suggested protocol was also applied for imaging of patients recruited at their center.
Materials and Methods
Data acquisition
All acquisitions were performed using a hybrid SPECT/CT-system (GE Discovery NM/CT 670) with detectors composed of NaI(Tl) crystal with 5/8” (1.59 cm) thickness, and ELEGP (extended low-energy general purpose), MEGP (medium-energy general purpose), or HEGP (high-energy general purpose) collimators. The acquisitions were performed in list-mode, with a file format that was available through a nondisclosure agreement with GE Healthcare. In-house developed software was used to bin event-by-event data into energy spectra and into images with arbitrary energy-window settings.
Source measurements in air
To study the measured energy spectra from 227Th and 223Ra, and to establish suitable energy windows for further analysis, measurements were made with source vials “in air,” that is, without scattering material in the vicinity of the source and between the source and γ-camera head. The vials, one with 4.9 MBq 227Th and another vial with 3.0 MBq of 223Ra, were placed at 10 cm distance from the anterior detector head. A planar static image (acquisition time 5 min, HEGP collimator) with both vials in the field-of-view (FOV) was acquired ∼4 h after the chemical separation of 227Th. At this time, the relative activity of 223Ra in the 227Th vial due to in-growth was less than ∼1%. Regions-of-interests (ROIs) drawn around each source was used to generate energy spectra from the list-mode data. Energy window settings for further analyses were then selected on the basis of the acquired spectra and corresponding images. The system sensitivities for the energy windows were calculated, which included attenuation and scatter in the vial.
Jaszczak phantom acquisitions
A Jaszczak phantom with two 16-mL spheres was prepared with the intent to mimic a clinically realistic scenario. One sphere was filled with 0.012 MBq 227Th and the other sphere with 0.012 MBq 223Ra. The background volume of 6.8 L was filled with 0.51 MBq 227Th solution, which also had a small amount of 223Ra content due to decay of 227Th between the time of purification and the time of phantom preparation. The resulting sphere-to-background activity concentration ratio was 10:1. The total activity in the phantom was 0.52 MBq 227Th and 0.05 MBq 223Ra, at the time of its preparation. Imaging, performed the day after phantom preparation, was performed with the γ-camera equipped with ELEGP, MEGP, and HEGP collimators. The acquisition time was 40 min, which was judged to be feasible for a patient.
Image processing
Radiation from cosmic and natural terrestrial sources gives rise to a background signal in γ-camera images. This background contribution is normally negligible, but presumably not in the current context due to low activity and emission probability of 227Th and 223Ra. The impact of background correction on image quality was therefore assessed. A background measurement was performed with an acquisition duration of 10 h, and the background-corrected image
where I
m denotes the acquired phantom or patient image, I
bkg is the acquired background image, both with index (
The poor count statistics expected in patient images results in excessive image noise, which is further amplified by the background subtraction. To study possible benefits of spatial smoothing with regard to image quality, the background-corrected images were filtered by convolution with a two-dimensional Gaussian kernel. The appropriate full width at half maximum (FWHM) of the Gaussian was defined by subjective, visual image quality assessment.
Due to the low activity administered to the patients, the overall image quality is expected to be poor. A CT localizer image (also named for example “scout” or “topogram,” depending on the camera manufacturer) provides, in addition to attenuation information that could be useful for quantitative purposes (not pursued in this work), a valuable anatomical frame of reference. Spatial coregistration of the images was facilitated by placing a 241Am marker on the couch during acquisition of the localizer and (part of) the γ-camera image acquisition. An additional energy window at 50–70 keV was included to image the photon emission at 59.5 keV from 241Am. The co-registration was performed by translation in the cranio-caudal direction. To further enhance the CT localizer as an anatomical reference for the γ-camera images, the localizer was processed using an edge-enhancing Sobel filter.
Patient acquisitions
All patients—having given their written informed consent to participate in the above-referenced clinical trial—recruited at their site, have been imaged on multiple occasions following study protocol. Included in this work is image data from two patients in different activity cohorts. Patient 1 received 1.5 MBq of 227Th-mAb and imaged in static mode with a single FOV, covering ∼40 cm in the cranio-caudal direction, centered over the abdomen. Patient 2 received 6.1 MBq of 227Th-mAb and was imaged in whole-body step-and-shoot mode, with two FOVs, including the thorax and abdomen, covering 77 cm in the cranio-caudal direction. Imaging was performed up to 42 d postinjection when the next cycle of treatment was administered.
Results
Energy window settings
The acquired energy spectra for 227Th and 223Ra vials with the HEGP collimator are shown in Figure 1. The spectra show that the main peaks within the 227Th spectrum can be seen at energies around 80 and 240 keV, which is in line with the decay data (Table 2). The broad peak around 240 keV is a combined signal from emitted photons with energies of 236 and 256 keV. The main peaks in the acquired spectrum for 223Ra and its daughters can be seen at ∼85, 155, 270, 350, and 400 keV. The spectral sensitivity (cps/MBq/keV) is higher for 223Ra than for 227Th in all parts of the energy spectrum apart from around the principal 227Th peak at 236 keV. It can be noted that there is no energy window setting that completely could isolate 227Th from 223Ra, and that there is no contribution from 227Th above ∼350 keV. On the basis of the acquired spectra and reasoning above, the following EW were selected for further investigation: EW1: 70–100 keV; EW2: 135–165 keV; EW3: 215–260 keV; EW4: 260–290 keV; EW5: 350–420 keV; EW6: 70–300 keV; EW7: Sum of EW1, EW3, EW4, and EW5.

Acquired energy spectra at the γ-camera from point sources of 227Th (blue) and 223Ra with its daughters (red), in units of cps/MBq/keV. The sensitivity is higher for 223Ra than for 227Th in all parts of the energy spectrum apart from the principal 227Th peak at 236 keV. The maximum energy of the 227Th spectrum is ∼350 keV, whereas the 223Ra spectrum is nonzero even at the camera hardware limit around 500 keV. Energy window 1–5 are shown in the diagram. 223Ra, radium-223; 227Th, thorium-227.
The system sensitivities (cps/MBq) for EW1–EW5 are summarized in Table 3. EW1 provides a relatively high count rate from both nuclides, and especially from 223Ra. It will likely not be useful for radionuclide separation in a clinical image, where the 227Th activity is much larger than the 223Ra activity. In addition, the image quality could be negatively affected by scattered photons. EW2+EW4 and EW3 are centered on the principal peaks from 223Ra and 227Th, respectively, and are thus likely to provide some information regarding the spatial distribution of the individual nuclides, although with an unwanted contribution from 223Ra in EW3 and analogously from 227Th in EW2 and EW4, mostly due to the poor energy resolution of the γ-camera. An additional high-energy window, EW5, was also included for further investigation. In EW5, there is only signal from 223Ra and no contribution from 227Th. However, insufficient photon collimation and low count statistics may limit the usefulness of this energy window in a clinically realistic context. As the count statistics is expected to be poor in a clinical measurement, two additional energy windows were included with the purpose of maximizing the acquired counts for a given acquisition time, (1) a broad energy window EW6 and (2) a summed window (EW1, EW3, EW4, and EW5).
System Sensitivity for Five Energy Windows
The γ-camera was equipped with a HEGP collimator.
Ra, radium-223; 227Th, thorium-227; EW, energy windows; HEGP, high-energy general purpose.
Figure 2 shows images of the two vials with 227Th (bottom right) and 223Ra (top left), respectively, corresponding to the four suggested energy windows, and qualitatively illustrates the possibility to distinguish 227Th from 223Ra under ideal conditions. Although 227Th dominates in the EW3 the 223Ra vial is clearly visible. The 227Th vial is also visible in the other energy windows, but only barely in EW5.
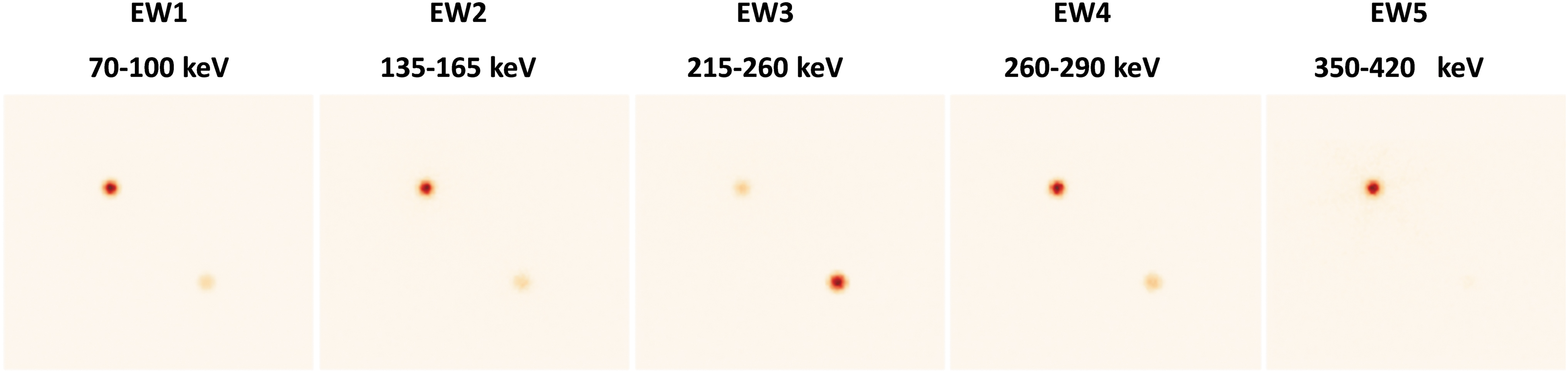
A vial containing 4.9 MBq of 227Th (lower-right corner of the FOV) and another vial with 3.0 MBq of 223Ra (upper-left corner of the FOV) were imaged. The images were acquired 4 h after the chemical separation of 227Th. EW [keV] denotes the energy window in which the image was acquired. 227Th, thorium-227; EW, energy windows; FOV, field-of-view.
Jaszczak phantom measurements
The images presented in Figure 3A show that background subtraction in combination with smoothing will subjectively improve the image quality. The acquired background image (second image from the left) is nonuniform with a pattern consistent with the spatial configuration of the photomultiplier tubes. This nonuniform pattern might arise from photons not passing through the collimator, but from the back of the detector heads, thus passing the photomultiplier tubes. The background-corrected anterior image (third image from the left) highlights the high contribution from the background radiation in relation to the number of detected events that actually contributes to the image. The ratio of number of detected counts from the phantom and the background is ∼0.3 in the acquisition presented in Figure 3A.

Figure 3B shows that EW1 (70–100 keV) is useful for imaging of both 227Th and 223Ra for all collimators. Energy window 2, centered over a 223Ra peak contains a significant portion of scatter from 227Th. Energy windows 3–5 are useful for separation of 227Th and 223Ra for the MEGP and HEGP collimators. However, for the ELEGP collimator, penetration degrades the image quality making it impossible to separate 227Th and 223Ra.
Figure 3B also shows the difference in image quality between the background-corrected and smoothed image (Gaussian with FWHM 2 cm) acquired in the broad EW6, corresponding to 70–300 keV, and EW7 (the image calculated as the sum of the background-corrected and smoothed images acquired from the four energy windows EW1, EW3, EW4, and EW5).
Patient acquisitions
Figure 4 displays the filtered and background-corrected images fused with the CT localizer for patient 1 (1.5 MBq), acquired at 1 d (upper row), and 28 d (lower row) postinjection, for energy windows EW3 (215–260 keV), EW5 (350–420 keV), and EW7 (EW1+EW3+EW4+EW5). The images to the left show mainly the 227Th-distribution, with some undesired spill-in contribution from 223Ra. The images in the center column, corresponding to EW5, show the distribution of 223Ra essentially without contamination from 227Th. It is shown that 223Ra can be separated from 227Th early after injection. Activity of 227Th follows mainly the blood-rich organs, like the heart and liver, but also as uptake in B cells maturing in the spleen (better seen in the posterior images). Most of the 223Ra activity is excreted through the intestine, but uptake is also visible in the skeleton at later time points. At 28 d postinjection, the only clear uptake is in the liver. EW7 might indicate the presence of 223Ra in the intestine, but EW5 is too noisy to conclude this.
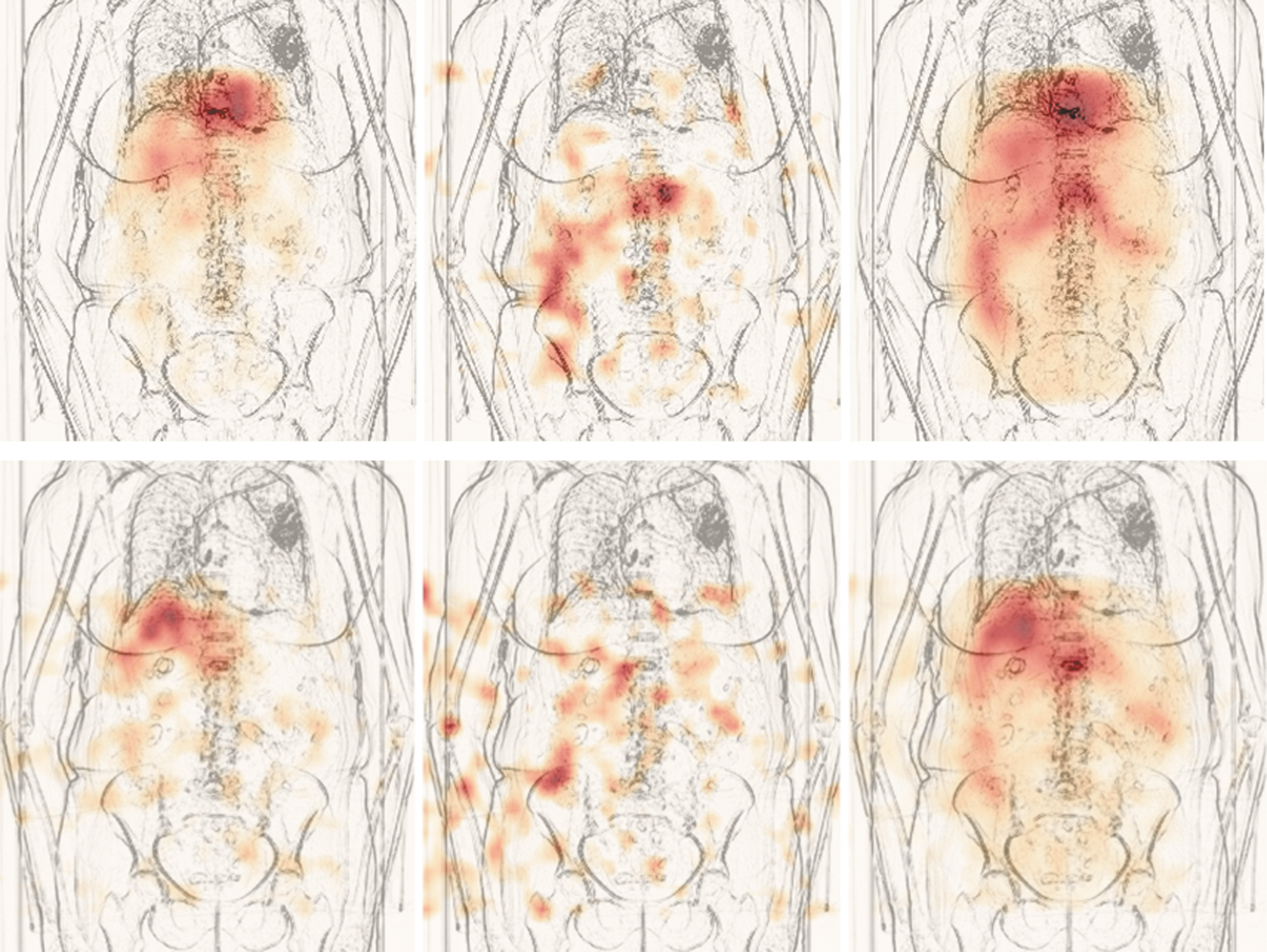
Anterior filtered background-corrected images fused with a CT-localizer. The different columns represent the different energy windows (from left to right) EW3 (215–260 keV), EW5 (350–420 keV), and EW7 (sum of energy windows 1, 3, 4, and 5). Upper row shows images for patient 1, acquired 24 h postinjection of 1.5 MBq 227Th-mAb targeting CD22. EW7 visualizes activity in the liver, heart, intestines, and to a lesser extent spleen (better seen in posterior images). By comparing EW3 and EW5 with EW7, it is realized that the signal from the liver, heart, and spleen originates from 227Th, whereas the signal from the intestines is due to 223Ra. Lower row shows the same images for patient 1 acquired 28 d postinjection. By comparing EW3 and EW5 with EW7, it is realized that the signal from the liver and spleen (seen in posterior images) originates from 227Th. EW5 might indicate some activity in the intestines, but the signal is too noisy to conclude this. 227Th, thorium-227; EW, energy windows; mAb, monoclonal antibody.
The corresponding images for patient 2 (6.1 MBq) postinjection are displayed in Figure 5. Thorium-227 can be seen in liver, heart, and spleen at the first time point and 223Ra in the intestine. Twenty-eight days postinjection, activity is still well visualized in liver, spleen, but also in the skeleton, where the spleen and skeleton are better visualized in the posterior images. Radium-223 excretion through the intestine is still seen in the EW5 image.

Anterior filtered background-corrected images fused with a CT-localizer. The different columns represent the different energy windows (from left to right) EW3 (215–260 keV), EW5 (350–420 keV), and EW7 (sum of energy window 1, 3, 4, and 5). Upper row shows images for patient 2, acquired 24 h postinjection of 6.1 MBq 227Th-mAb targeting CD22. EW7 visualizes uptake in the liver, heart, intestines, and to a lesser extent also in the spleen (better seen in the posterior images). By comparing EW3 and EW5 with EW7, it is realized that the signal from the liver, heart, and spleen originates from 227Th, whereas the signal from the intestines is due to 223Ra. Lower row is for the same patient acquired 28 d after administration. Energy window 7 visualizes uptake in the spleen, liver, intestines, and skeleton. By comparing EW3 and EW5 with EW7, it is realized that the signal from the liver, skeleton, and spleen originates from 227Th, whereas activity in intestines is due to 223Ra. 223Ra, radium-223; 227Th, thorium-227; EW, energy windows; mAb, monoclonal antibody.
Figure 6 shows the actual energy spectra within two ROIs with high accumulation of either 227Th or 223Ra, and one ROI with little activity. It is clearly shown that there is a spill-in of EW3 in EW4 and vice versa, but that EW5 is almost free from contribution of 227Th. The last ROI shows how important the background subtraction is, as the cps in a pixel is the area under curve and without background subtraction would be hugely overestimated.
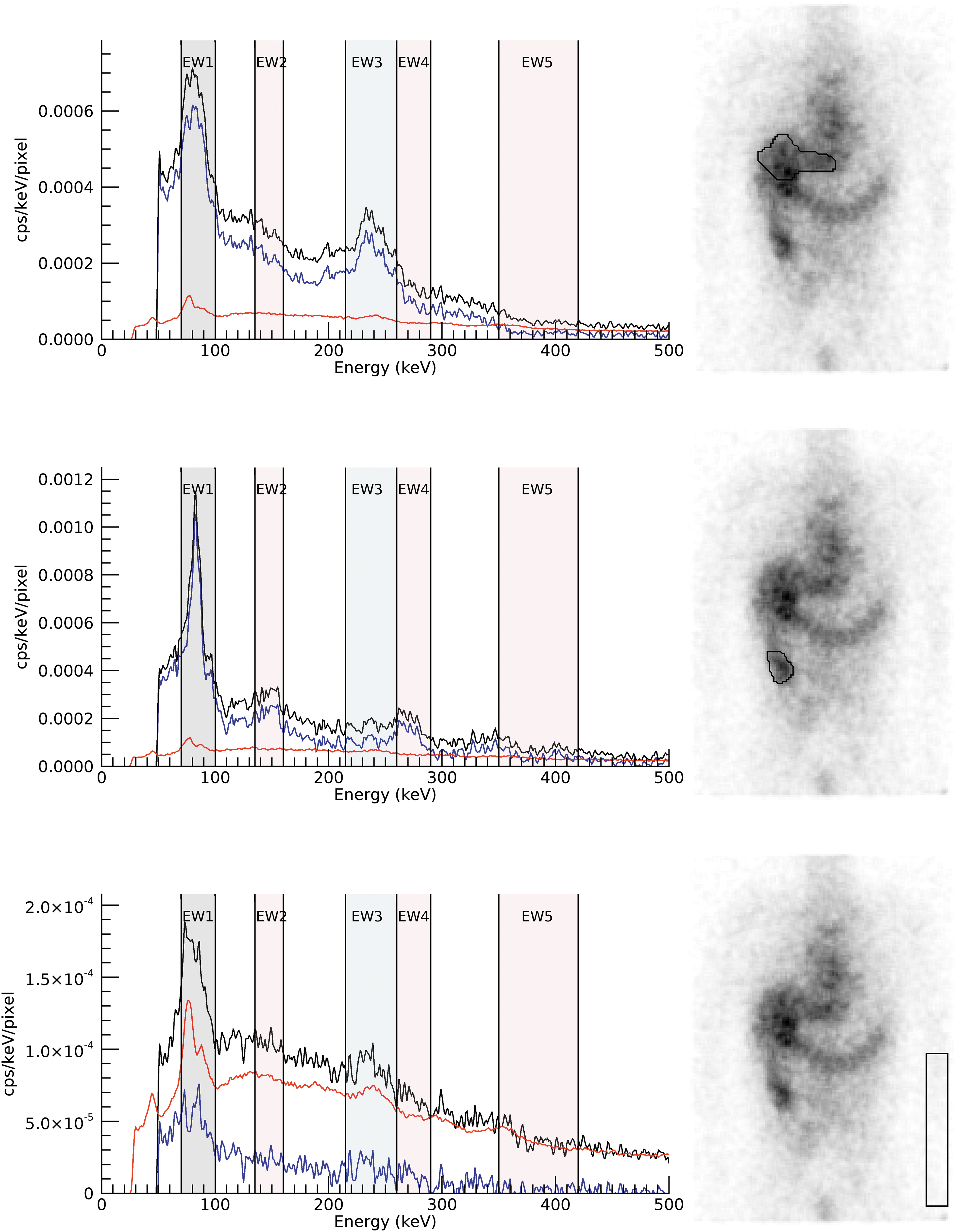
Unfiltered energy spectra within the ROI shown to the right. The patient image corresponds to EW7 (sum of energy window 1, 3, 4, and 5). The black curves show the acquired data. The red curve is from a 20-h-long background acquisition and the blue curve is the background-subtracted energy spectra. The upper ROI contains a part of the liver where there is predominantly 227Th present. The middle row show an ROI over a hotspot in the intestine, which is known as the main excretion path of 223Ra. The lower row show spectra from an ROI with low activity, likely only some 227Th circulating in blood in the arm. This highlights the effect of the background subtraction, where otherwise the natural background would dominate in the energy windows. 223Ra, radium-223; 227Th, thorium-227; EW, energy windows; ROI, region-of-interest.
Discussion
Acquisition settings for separate 227Th/223Ra γ-camera imaging of patients injected with targeted thorium-227 conjugates have been investigated. Energy window settings and collimator performance have been investigated through analysis of emission data and phantom acquisitions. The suggested settings have been tested for two patients having received treatment with CD22-targeting 227Th-mAb.
Of the identified and investigated energy windows, the 135–165 keV window is suboptimal due to the large portion of scatter from 227Th. The sum of energy windows EW1, EW3, EW4, and EW5 qualitatively appears to improve the image quality slightly compared with the broad energy window (70–300 keV).
All collimators gave images with an acceptable quality for the low-energy window (EW1, 70–100 keV), but the penetration for the higher energy windows with the ELEGP collimator became prominent. Therefore, the ELEGP collimator could not be used to separate 227Th from 223Ra. The MEGP and HEGP collimators produced images with similar sensitivity. Since the images are noisy because of low count statistics and therefore have to be filtered, the spatial resolution in the final images are similar for the two collimators. The use of a HEGP collimator minimizes septum penetration, which is beneficial for activity quantification. A HEGP collimator was chosen for acquiring the patient images, since it would give the best conditions for a quantitative method that is currently under development.
The background correction for images following administration of 227Th-mAb improved the image quality, as judged by qualitative assessment, especially at the low activity cohorts where the signal-to-background ratio is lowest. The background images originating from natural background radiation are not uniform, which means that background correction cannot be performed through a subtraction with a scalar, but has to be performed on a pixel-by-pixel level. The uniformity is energy dependant and resembles the shape of the photomultiplier tubes, probably due to interactions in the γ-camera head behind the NaI-crystal. For continuous scanning acquisition, that is, scanning in whole-body mode, the background uniformity might be of less importance, but is of outmost importance for static and SPECT acquisitions.
The co-registration with the anatomical image (the CT localizer image) facilitates the visual interpretation of the biodistribution. The localizer acquisition will give an additional radiation dose to the patient, but the contribution is negligible compared with the total radiation dose that the patient will receive during his/her radionuclide treatment. One source of 241Am placed on the patient is enough for co-registration as the images only will need to be adjusted in one dimension (in the cranio-caudal direction).
The vial experiment showed that, when no surrounding activity is present, 223Ra can be separated from 227Th relatively well (using EW5), but that 223Ra will always spill down in the 227Th main energy window (EW3). When surrounding activity is present, as in the Jaszczak phantom experiment, the primary photons emitted from 223Ra and/or 227Th are drowned in scattered photons originating from surrounding activity. However, the patient images from 24 h after administration clearly show that it is possible to visually observe the major distribution of 227Th and 223Ra by studying both EW3 and EW5. This separation could be seen up to 28 d postinjection for the high-activity cohort. For patient images from the low-activity cohort (1.5 MBq) the signal from 223Ra was very low resulting in very noisy images with almost no counts and no means to adequately distinguish between 223Ra from 227Th. These noisy images are an effect of background subtraction. As an example, an acquisition without any source will produce an image that only includes the difference between the acquisition and the “noise-free” long acquisition. The total net counts in the entire background-corrected image would be very close to zero, but due to the statistical variation of the acquisition on a pixel level this will be seen as noise having both positive and negative values.
Although all experiments were performed on a SPECT/CT-system with 5/8” thick NaI crystals, the authors believe that the results are transferable also to systems with 3/8” crystals. There is likely some loss of efficiency at higher energies, especially for 223Ra in EW5, but this could be counterbalanced by the lower contribution from background radiation.
Conclusions
The phantom measurements show that it is possible to acquire images to visually observe the biodistribution of 227Th-mAb when 1.5 MBq or more is injected to a patient. By selecting the correct energy windows 223Ra could be distinguished from 227Th relatively well by using multiple energy windows. The patient measurements confirm this and show that 227Th could be distinguished from 223Ra for acquisitions up to at least 28 d postinjection depending on the administered activity.
Recommended energy window settings are (1) 70–100 keV (227Th and 223Ra); (2) 215–260 keV (227Th); (3) 260–290 keV (223Ra); and (4) 350–420 keV (223Ra). A sum of all windows is useful to improve the noise statistics, but cannot alone differentiate 227Th from 223Ra.
A long background acquisition coming from terrestrial and cosmic radiation is highly recommended to subtract the signal from the background and thus enhance the image quality.
Low-pass filtering is recommended to reduce image noise.
An energy window set on 50–70 keV for visualization of a 241Am point source used for coregistration of images is also recommended. Coregistration of an X-ray scout image and the γ-camera images will facilitate the interpretation of the qualitative biodistribution images.
Footnotes
Disclosure Statement
There are no existing financial conflicts.
Funding Information
No funding was provided for this research.