
Abstract
Aim:
The objective of this study was to estimate the absorbed doses to the normal organs and tumor lesions in metastatic castration-resistant prostate cancer (mCRPC) patients treated with indigenously developed 177Lu-PSMA-617 that could establish optimal treatment protocol with minimum risk to the dose-limiting organs. Furthermore, attempt was also made to compare radiation absorbed doses for normal organs and tumor lesions in subsequent cycles of 177Lu-PSMA-617 peptide receptor radioligand therapy (PRLT) in the same group of patients during the course of treatment.
Methods:
A total of 30 patients of proven mCRPC were enrolled for this prospective study. These patients received up to 5 cycles of treatment with 177Lu-PSMA-617 PRLT (1 cycle for 13 patients, 2 cycles for 9 patients, 3 cycles for 3 patients, and 5 cycles for 5 patients), at 11–12-week intervals between the two successive therapies. The patients underwent postadministration whole-body scintigraphy at five time points: 0.5 (prevoid), 2, 12, 24, and 72/96 h (postvoid). From time-activity curves generated by drawing regions of interests on the images, number of disintegrations was determined. Tumor masses were estimated from pretherapeutic 68Ga-PSMA-11 positron emission tomography-computed tomography images. Absorbed doses for organs and tumors were calculated using OLINDA 2.0 software.
Results:
The average activity of 177Lu-PSMA-617 (mean ± SD) administered per patient per cycle was 4.94 ± 0.45 GBq. The mean absorbed organ doses (mean ± SD) from first therapy cycle in Gy/GBq were as follows: kidneys 0.52 ± 0.16, spleen 0.17 ± 0.07, liver 0.08 ± 0.05, salivary glands 0.53 ± 0.30, lacrimal glands 1.45 ± 0.85, nasal mucosa membrane 0.46 ± 0.19, urinary bladder 0.23 ± 0.02, and bone marrow 0.04 ± 0.03. The mean effective dose for whole body from first therapy cycle was 0.05 ± 0.03 Sv/GBq. Among all the normal organs, lacrimal glands received the highest absorbed dose. The median dose for all lesions, bone lesions, lymph nodes, primary site, liver lesion, lung lesion, and soft tissue deposit from first therapy cycle was determined to be 4.17, 4.23, 3.96, 4.36, 10.27, 0.78, and 4.68 Gy/GBq respectively. Absorbed doses received by the normal organs in five consecutive cycles follow three different trends, (a) for kidneys, salivary glands, and nasal mucous membrane, absorbed doses increased from first therapy cycle to second therapy cycle and then slowly decreased in subsequently therapy cycles; (b) for spleen, liver, and lacrimal glands, absorbed doses decreased with the successive therapy cycles; and (c) in case of bone marrow, bladder, and whole body, mean absorbed dose almost remained constant in each therapy cycle. Absorbed doses to the lesions gradually decreased with increase of the number of therapy cycles.
Conclusions:
The organ and tumor absorbed doses of 177Lu-PSMA-617 in mCRPC patients were found to be comparable to the data reported in the literature. The highest absorbed organ dose was observed in lacrimal glands and being a dose limiting organ, a cumulative activity up to 32.5 GBq (878 mCi) of 177Lu-PSMA-617 in 4–5 therapy cycles appears safe and feasible to achieve full therapeutic window.
Introduction
Prostate cancer is the second most frequently diagnosed cancer (7.1% of the all sites) and fifth (3.8% of the total sites) leading cause of cancer-related deaths among males worldwide. 1 It is also second most common cancer in men in metropolitan cities of India, and is among the top 10 leading sites of cancers in population-based cancer registries of the rest of India. 2 Although in some cases prostate cancer is localized, a large number of patients have advanced metastatic disease for which no curative treatment is available. Such patients are subjected to hormonal therapy followed by chemotherapy. However, as conventional chemotherapy responses are often transient, many patients progress to metastatic castration-resistant prostate cancer (mCRPC).
It has been documented in the recent literature that radionuclide therapy using 177Lu- radiolabeled prostate-specific membrane antigen (PSMA) is a safe and effective modality for the treatment of patients suffering from end-stage progressive mCRPC. 3 –7 PSMA is a type II transmembrane protein expressed in prostate epithelial cells (having extracellular, transmembrane, and intracellular components), which are potential targets for targeted delivery of radiation dose to the tumor cells. This protein is overexpressed in prostate carcinoma and the degree of upregulation increases in higher grade cancers, metastatic disease, and hormone-refractory disease, 8,9 making this an ideal target for developing agents for targeted radionuclide therapy.
Targeting of PSMA overexpression in prostate cancer with 177Lu-labeled PSMA ligands has recently emerged as a promising option for treating the mCRPC patients. 10 Moreover, 177Lu, which is indigenously sourced from the research reactor, DHRUVA, has excellent therapeutic properties [T½ = 6.73 d, Eβ(max) = 0.497MeV, and Eγ = 113 keV (6.6%), 208 keV (11%)] for use in labeling with PSMA. Treatment with 177Lu-PSMA-617 is being carried out in the center for the treatment of mCRPC on a routine basis since the last 3 years. It is well documented in the contemporary literature that, apart from exhibiting intense uptake in prostate cancer tissue and metastases, radiolabeled PSMA exhibits high uptake in salivary glands and lacrimal glands, as well as moderate uptake in liver, intestine, and kidneys within a few hours of administration. 11,12
Dosimetry studies with 177Lu-labeled PSMA suggested that salivary glands, lacrimal glands, and kidneys represent the dose-limiting organ for 177Lu-PSMA therapy. 3,6,7,13 –19 The aim of this study was to perform image-based absorbed dose calculations for the normal organs, whole body, and the tumors lesions in mCRPC patients treated with 177Lu-PSMA-617. The results thus obtained will provide the insight toward deciding the optimal treatment protocol with minimum risk to the dose-limiting organs. In addition, attempt was made to compare radiation absorbed doses in normal organs and tumor lesions in subsequent therapy cycles using 177Lu-PSMA-617 in the same group of patients.
Materials and Methods
Patients
Between September, 2017, and July, 2019, a total of 30 patients were enrolled for this prospective study. The patients underwent up to 5 cycles of therapy with 177Lu-PSMA-617 (1 cycle for 13 patients, 2 cycles for 9 patients, 3 cycles for 3 patients, and 5 cycles for 5 patients) at 11–12-week intervals between the two successive therapies. The baseline demographics of all the patients enrolled for this study are shown in Table 1.
Baseline Demographic Characteristics of Patients (N = 30)
TRUS, transrectal ultrasound; TURP, transurethral resection of the prostate; EDTMP, ethylenediamine tetramethylene phosphonic acid; GFR, glomerular filtration rate; PSA, prostate-specific antigen.
All the patients had proven mCRPC and undergone positron emission tomography-computed tomography (PET-CT) scanning with 68Ga-PSMA-11 before the enrollment for this study to ensure expression of PSMA on the cancerous lesions. Detailed inclusion and exclusion criteria of patients enrolled for this study and the schema of this study are given in Figures 1 and 2, respectively.

Flow diagram of patient's inclusion and exclusion criteria.
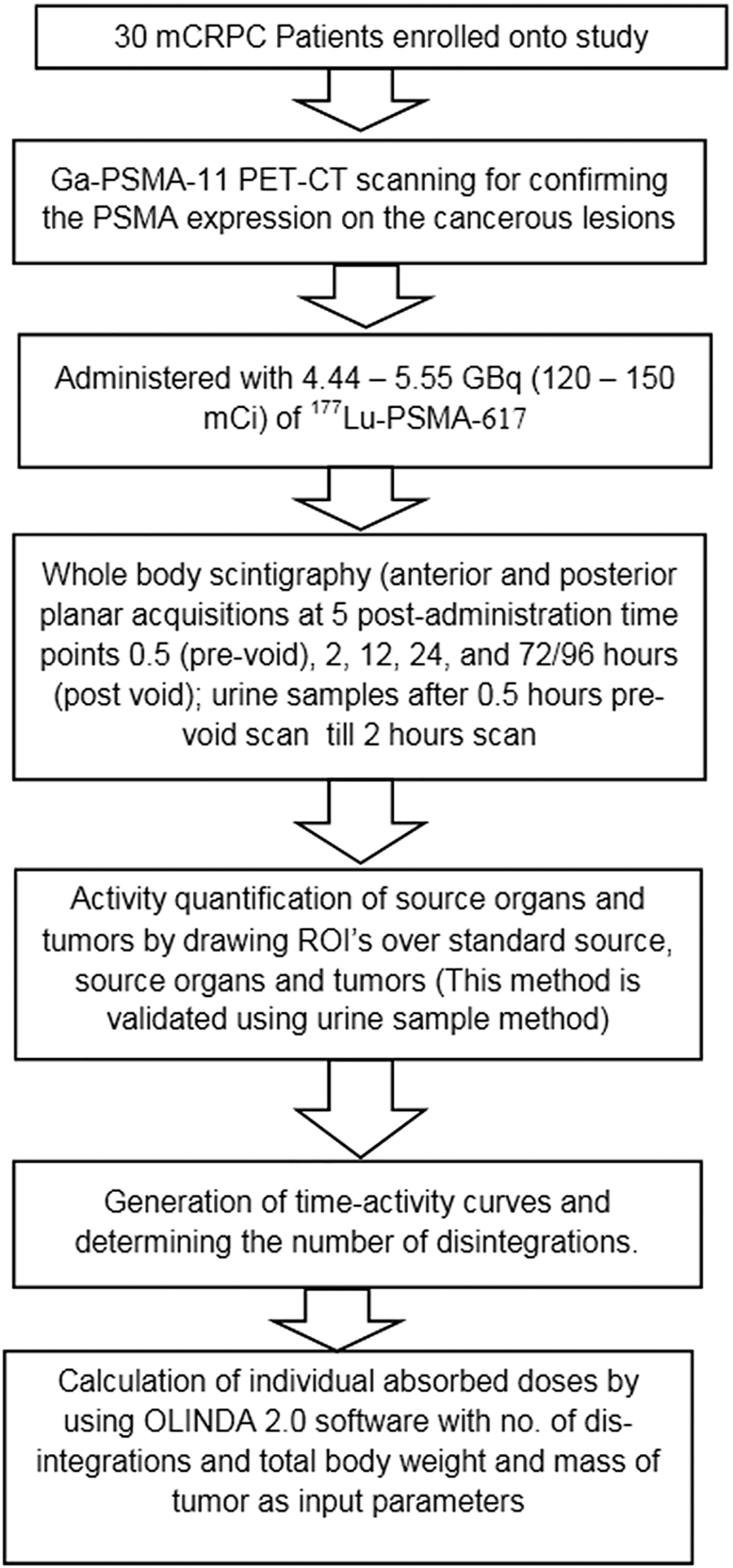
Schema of this study.
The study protocol was approved by Institutional Scientific and Medical Ethics Committees and was conducted in accordance with the declaration of Helsinki and good clinical practice. Prior informed written consents were obtained from all the enrolled patients before administering 177Lu-PSMA-617 therapy. The product was approved by the regulatory body of Department of Atomic Energy India, the Radiopharmaceutical Committee, for routine patient use.
Preparation of 177Lu-PSMA-617 patient dose
177Lu was produced indigenously in the DHRUVA reactor of Bhabha Atomic Research Centre by thermal neutron bombardment [176Lu(n,γ)177Lu] on enriched (in 176Lu) Lu2O3 target following the protocol reported elsewhere 20 and received in the form of 177LuCl3 from Board of Radiation and Isotope Technology. All other chemicals used were procured from reputed local manufacturers and were of analytical reagent (AR) grade.
For the formulation of patient dose of 177Lu-PSMA-617, a solution of PSMA-617 was prepared by dissolving 1 mg of DOTA-PSMA-617 (procured from ABX, Germany) in 1 mL of ultrapure water and mixed with ammonium acetate buffer (pH 4.5). The resulting solution was incubated with 22.2 GBq (600 mCi) of 177LuCl3 at 95°C for 30 min. The metal-ligand molar ratio used for preparation of 177Lu-labeled PSMA-617 was always maintained 1:2.5 for all the batches. The radiochemical purity of 177Lu-PSMA-617, thus prepared, was assessed by using Whatman 3 MM chromatography paper (UK) using acetonitrile and water (1:1, v/v) as the solvent system. All radioactive counting, associated with the preparation and quality control of 177Lu-PSMA-617, was performed using a well-type NaI(Tl) scintillation detector, obtained from Electronic Corporation of India Limited, keeping the baseline and window at 150 and 100 keV, respectively, to utilize the 208 keV gamma photon emission of 177Lu.
Sterility of the radioactive preparation was ensured by passing the product through 0.22-μm filter before its administration in patients. Endotoxin limit was quantified by following the standard procedure using Gel Clot BET assay method before release of the batch for patient use.
177Lu-PSMA-617 therapy protocol
According to the institutional recommendations, all patients were treated as inpatients at radionuclide therapy ward and discharged after 24 h of administration of therapy dose. The patients were administered 100 mL of normal saline containing dexamethasone (8 mg) and ondansetron (8 mg) through intravenous pathway, subsequent to which 4.44–5.55 GBq (120–150 mCi) of 177Lu-PSMA-617 in 100 mL of normal saline was slowly infused over a period of 30 min. Infusion of another 1000 mL of normal saline was continued for 3–4 h after the completion of administration of 177Lu-PSMA-617 therapy dose.
177Lu-PSMA-617 imaging and quantification
The γ-camera used for scintigraphy studies employed a state-of-the-art dual head γ-camera (Symbia E Dual Head system, Siemens Medical Solution, Germany). The matrix size of 256 × 1024 pixels and a symmetrical window of 20% around the two major γ-ray energies of 177Lu (113 and 208 KeV) were used for all acquisitions. Analyses of the acquired images was performed by using software Syngo MI application version-VA60A/VA46A on Siemens workstation.
All patients enrolled in this study underwent whole-body γ-scintigraphy (anterior and posterior planar acquisitions) at five postadministration time points: 0.5 (prevoid), 2, 12, 24, and 72/96 h (postvoid). Since these patients were discharged from therapy ward after 24 h of dose administration, for 72/96 h imaging, they were instructed to report again in the department on the specific date and time. All imaging were performed at a scan speed of 30 cm/min using the dual-head gamma camera equipped with 1.0 cm thick NaI (Tl) crystals and high-energy collimators. In addition, a glass Petri dish containing known activity (18.5–120 MBq and 0.5–3.25 mCi) of 177Lu was used as the reference standard and placed in the field of view during each whole-body γ-scintigraphy, primarily to account any variation in the distance between the patient and the detector. For activity quantification and attenuation correction, the conjugate view method 21 was used and no scatter correction was applied. All five scans were compared and regions of interest (ROIs) were drawn anterior and posterior (Fig. 3) over the standard source, whole body, kidney, liver, spleen, lacrimal glands, salivary glands, nasal mucosa, and tumors. ROIs were drawn initially on images recorded at 12 h postadministration (anterior and posterior) and manually relocated on other images acquired at the other postadministration time points, keeping pixels (acceptable difference within ±10%), size, and shape unchanged except, for overlying or underlying organs, based on visual analysis of planar images. For overlying or underlying organs, small ROIs were drawn over the part of the organ without overlap, and the counts were extrapolated to include the entire organ, assuming similar counts per pixel. For organ/tumor background correction, separate ROIs were generated in the thigh and head region. From each ROI, counts were obtained and geometric mean was calculated. To quantify the radioactivity in the ROIs, transmission factor was calculated for each patient following the equation mentioned below:
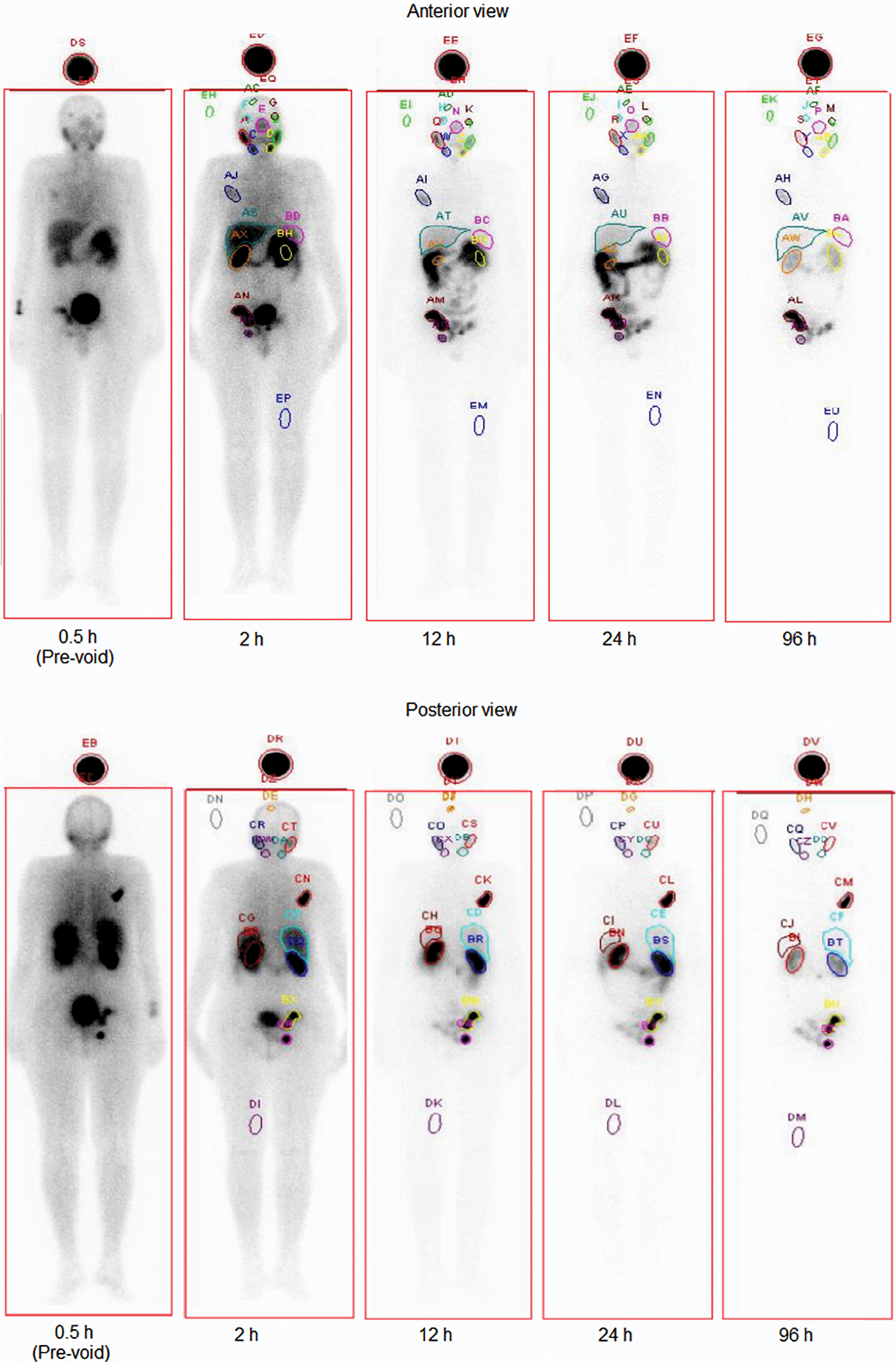
Whole-body (Anterior and Posterior view) scintigraphic images of a patient of mCRPC, recorded at 0.5 (prevoid), 2, 12, 24, and 96 h postinjection of 177Lu-PSMA-617; ROIs were drawn at various organs/metastatic lesions for determining activity. mCRPC, metastatic castration-resistant prostate cancer; ROI, regions of interest. Color images are available online.
where T is the transmission factor, AC is the calculated activity based on the initial (0.5 h) whole-body scan (before excretion of the radioactivity from the body), and A0 is the actual or administered activity. Again,
where AR is the activity of reference imaging source, CWB is the geometric mean of background-subtracted whole-body counts obtained from patient's ROIs of the initial scan (0.5 h), and CR is the geometric mean of background-subtracted counts obtained from reference source ROIs during the initial scan (0.5 h). From reference source activity, reference source counts, and transmission factor and counts in respective organ/tumor, the amount of radioactivity retained in the patient's respective organ/tumor was calculated. This method of calculating the radioactivity inside the body was validated by collecting the urine samples between start of infusion (prevoid scan) and 2 h postvoid scan of all the patients who underwent 177Lu-PSMA-617 therapy for the first time. All urine bottles were measured for urine volume. Samples of 1 mL were taken from each urine bottle and subsequently diluted with water to a total volume of 5 mL before measuring the sample in HPGe detector (P-type Coaxial Detector GCD-50 190, BSI). From these samples, the total amount of activity excreted during 2 h (before 2 h postvoid-scintigraphy) was calculated and compared with the decrease in activity calculated by using transmission factor and imaging data of 0.5 h prevoid and 2 h postvoid scans.
From the retained activity statistics, time-activity curves were generated and extrapolated from last measured value to terminal point where it almost touches x-axis (time axis). The cumulative activity was estimated by determining the area under the time-activity curves using Origin (R) software (Microcal Lab Corporation, Northampton, MA). For effective half-life determination, time-activity curves were fitted to biexponential functions using this software. The number of disintegrations (i.e., residence time) in normal organ/tumor was derived by dividing cumulative activity in the normal organ/tumor by the administered activity and validated by calculating the number of disintegrations using exponential modeling (EXM) module of OLINDA/EXM 1.0 software 22 in 40 organs. From the number of disintegrations in the organ/tumor, absorbed doses were estimated by using OLINDA 2.0 software. 23 For urinary bladder, the number of disintegrations was derived using the voiding bladder model built in OLINDA 2.0 software by assuming voiding interval of 2 h. Tumor masses used for absorbed doses estimation were obtained from the corresponding computed tomography (CT) data of the patients. For the estimation of absorbed dose in tumor, sphere model available in OLINDA 2.0 software was used. The masses for kidneys, liver, spleen, urinary bladder, bone marrow, salivary glands, and whole body were modified in the OLINDA 2.0 software using mass correction factor, which is the ratio of weight of the patient and ICRP 89 adult male phantom mass. Due to anatomy of the lacrimal gland and only anterior ROIs, the absorbed dose per unit administered activity was calculated using calibration factor obtained from imaging reference source.
Results
Administration of 177Lu-PSMA-617 was well tolerated by the patients as neither any immediate adverse effect was recorded during injection nor any treatment-related deaths were recorded till the completion of the study. In addition to intense uptake observed in the cancerous lesions and metastatic sites, the planar images showed high uptake in the salivary glands, lacrimal glands, and kidneys, along with moderate uptake in liver, spleen, nasal mucous membrane, and proximal intestine. The calculated mean ± SD (median) tumor to kidney absorbed dose ratios were found to be 16.64 ± 26.94 (6.83) for all lesions, 13.58 ± 19.54 (6.53) for bone lesions, 45.28 ± 56.68 (14.08) for lymph nodes, 6.29 ± 4.68 (5.44) for primary tumor site, 8.55 ± 11.50 (2.86) for lung lesions, and 24.59 ± 16.54 (21.02) for liver lesions.
Method of calculating the radioactivity inside the body by using transmission factor was correlated with the method of calculating the radioactivity inside the body by using urine samples (r = 0.95, p = < 0.0001) (Fig. 4). For calculating the number of disintegrations in the organ/tumor, strong correlation was found between OLINDA/EXM software method and ORIGIN software method (r = 0.98, p = < 0.0001) (Fig. 5).
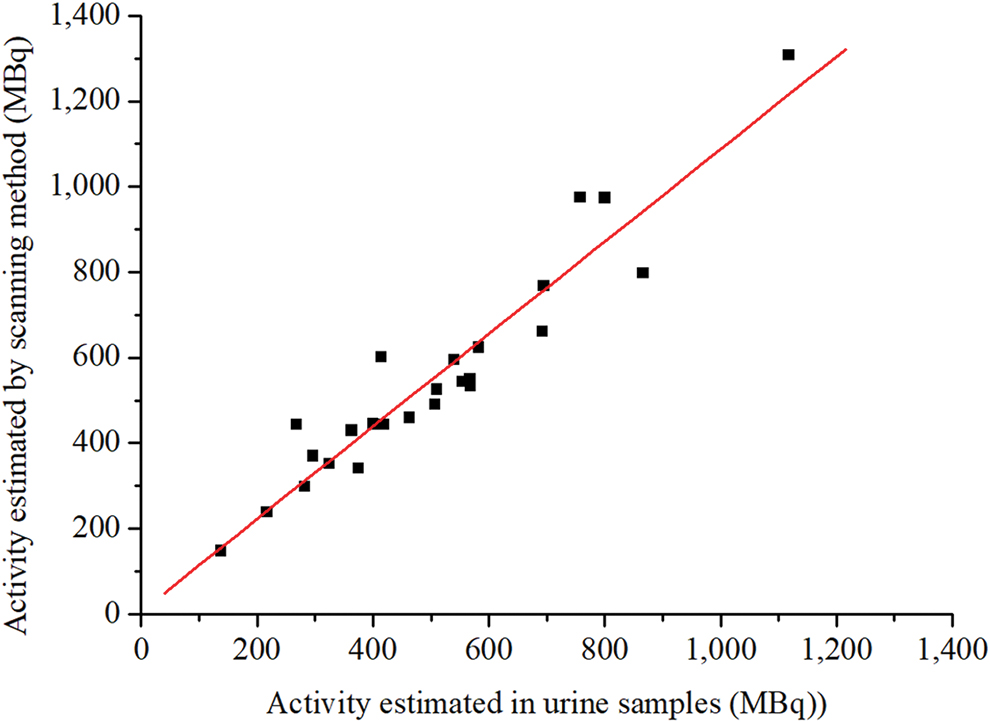
Correlation between activity quantification estimated by using (a) scanning method and (b) urine sampling method. The red line represents the linear regression line. Both methods strongly correlated with Pearson's rho of 0.95. Color images are available online.
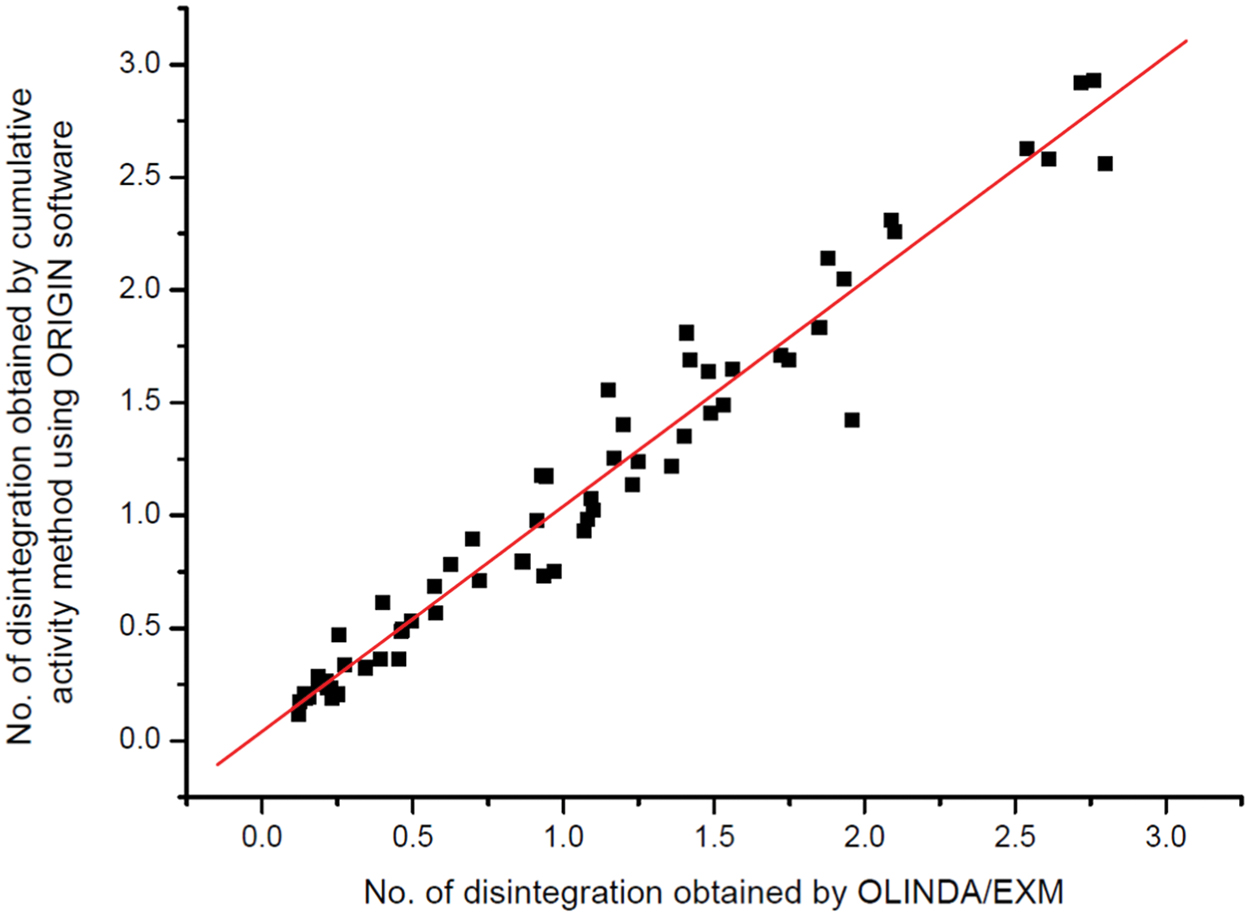
Correlation between number of disintegration calculated by OLINDA/EXM software and cumulative activity method using ORIGIN software. The red line represents the linear regression line. Both methods strongly correlated with Pearson's rho 0.98. Color images are available online.
The activity (mean ± SD) of 177Lu-PSMA-617 administered per patient per cycle was 4.94 ± 0.45 GBq (133.51 ± 12.16 mCi). The maximum cumulative activity administered was 25.51 ± 1.40 GBq (689.46 ± 37.84 mCi) for five patients who underwent five cycles of treatment.
Normal-organ dosimetry
The values (mean, SD and range) for the corresponding absorbed doses per unit administered activity (Gy/GBq) for overall and different treatment cycles are presented in Table 2 and found that among all the normal organs, lacrimal glands received the highest dose, followed by salivary glands. Five patients had completed five treatment cycles and a comparison of absorbed doses in different treatment cycles was attempted for such patients (Table 3). It is evident from the data that the absorbed doses received by the different organs in five consecutive cycles follow three different trends, (a) for kidneys, salivary glands, and nasal mucous membrane, absorbed doses increased from first therapy cycle to second therapy cycle, and then slowly decreased in subsequently therapy cycles; (b) for spleen, liver, and lacrimal glands, absorbed doses decreased with the successive therapy cycles; and (c) in case of bone marrow, bladder, and whole body, the mean absorbed dose almost remained constant in each therapy cycle.
Absorbed Doses for Normal Organs in Gy/GBq
Comparison of Absorbed Doses for Normal Organs in Gy/GBq in Five Patients Who Completed Five Treatment Cycles
Tumor lesion dosimetry
The absorbed doses in the tumors showed large variation based upon the tracer uptake in the individual lesions, with a median absorbed dose of 3.22 Gy/GBq (range 0.05–46.22 Gy/GBq). The maximum dose of 46.22 Gy/GBq (225.74 Gy) was received by one skeletal lesion during first cycle of therapy. The values (n, mean, SD, median, and range) for the corresponding absorbed doses per unit administered activity are shown in Table 4. Five patients had completed five treatment cycles and a comparison of absorbed doses in different treatment cycles was done for these patients (Table 5). It is evident from the table that absorbed doses in tumorous lesions decreased with the increase in the number of treatment cycles. A similar trend was also observed in bone lesion subgroup. However, no reliable comparison could be made for lymph nodes, primary sites, and liver lesions due to low sample size.
Absorbed Dose for Tumor Lesions in Gy/GBq
NA, No data available for these lesions in the particular treatment cycle.
Comparison of Absorbed Doses for Tumor Lesions in Gy/GBq in Five Patients Who Had Completed Five Treatment Cycles
NA, No data available for these lesions in particular treatment cycle.
Response of 177Lu-PSMA-617 therapy
After the first cycle of 177Lu-PSMA-617 therapy, 9 patients expired due to their progressive disease. Of the 21 patients, where prostate-specific antigen (PSA) data are available, 16 (76%) showed reduction in PSA levels (Fig. 6) and their analysis of PSA levels before and after first therapy cycle is presented in Table 1. Figure 7 shows the response of 177Lu-PSMA-617 therapy in one of the study patients, which was evaluated by comparing the 68Ga-PSMA-11 PET-CT recorded before each therapy cycle, and from this figure, it is evident that there is drastic reduction (99%) in liver lesion volume after four treatment cycles.

Waterfall plot presenting PSA response in mCRPC patients after first therapy with 177Lu-PSMA-617. Last value of progression of PSA >100% was cropped to simplify the plot. PSA, prostate-specific antigen. Color images are available online.
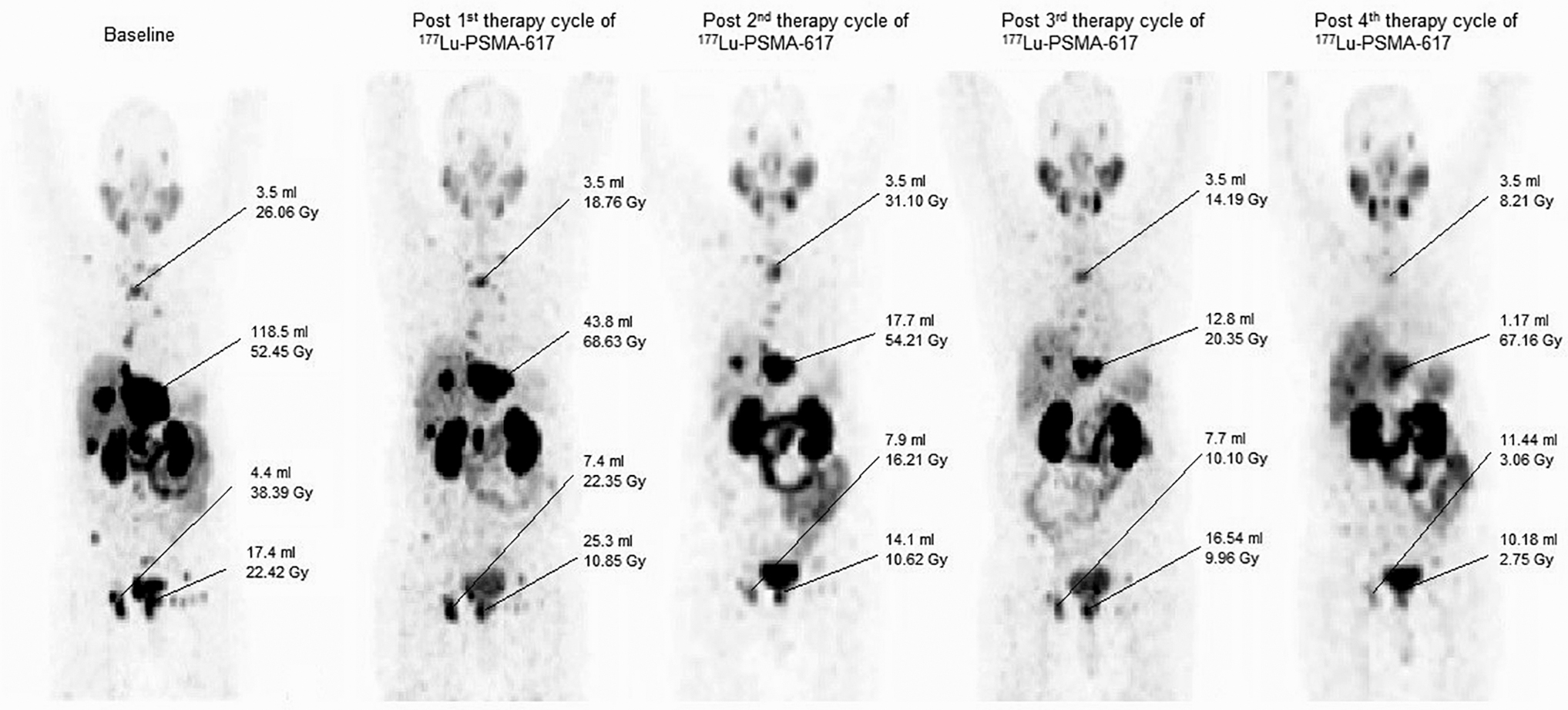
68Ga-PSMA-11 PET-CT images of a patient undergoing successive therapy with 177Lu-PSMA-617 showing gradual decrease of tumor volume in the liver with increase in number of therapy cycles.
Discussion
In the recent years, radionuclide therapy with 177Lu-PSMA-617 has emerged as an important therapeutic modality for the treatment of mCRPC patients, and several reports have been documented describing the clinical efficacy of this agent. 4 –6,10 It is reported that radiolabeled PSMA-617 also exhibits uptake in various normal tissues. 12 This study also revealed the similar findings, which is high uptake in the salivary glands, lacrimal glands, and kidneys, along with moderate uptake in liver, spleen, nasal mucous membrane, and proximal intestine. The radiolabeled agent also exhibited high tumor-to-kidney uptake for all investigated metastases (median 6.83), which is comparable with the median value of 5.8 previously reported by Delker et al. 14
In this study, the authors have documented the radiation dosimetry data of 177Lu-PSMA-617 in normal organs and tumor lesions generated from 30 patients and a total of 65 therapy cycles. The absorbed doses for 177Lu-PSMA-617 in tumor lesions, whole body, and healthy organs were estimated using quantitative planar images. It has been reported in the contemporary literature that the 177Lu activity in the intestine overlapped significantly with the kidneys in most of the planar image dosimetry in 177Lu-DOTATATE/177Lu-PSMA therapy, and this would probably lead to overestimation of absorbed dose to the kidneys. Similarly, overlying or underlying organs may lead to the overestimation of absorbed doses received by the tumors or other organs. 14,16,17,24,25 In this study, they adopted pixel-based approach, wherein small ROIs were drawn over the organ/tumor to avoid the contribution from overlying or underlying organs, and later, the counts under ROI were escalated to actual pixel size of the organ, assuming uniform activity distribution in the entire organ. The kidney-absorbed doses of 0.49 ± 0.17 Gy/GBq (mean ± SD) observed in this study are well comparable to the values between 0.39 and 0.99 Gy/GBq reported in the literature. 4,7,13 –19 Kidney being one of the critical organs, the authors' data predict that a cumulative activity of 47 GBq (1270 mCi) of 177Lu-PSMA-617 is safe, keeping in mind that 23 Gy is the dose considered safe for kidneys based on the data from external beam radiotherapy. 26 In this study, maximum cumulated activity administered was 25.83 GBq (698 mCi) in 5 treatment cycles and no case of nephrotoxicity was observed.
In this study, lacrimal glands received the highest absorbed dose of 1.23 ± 0.70 Gy/GBq (mean ± SD), which is comparable with the value of 1.49 Gy/GBq, reported by Hohberg et al. 17 using imaging standard for calibration. Considering the anatomic shape and position of the lacrimal gland, the authors also used imaging standard for calibration in this study. It is reported that the absorbed dose to lacrimal gland varies over a wide range starting from 0.36 ± 0.18 Gy/GBq to 3.8 ± 1.4 Gy/GBq. The value of 0.36 ± 0.18 Gy/GBq was reported by Violet et al., 16 which was calculated using voxel-based technique. However, the authors found the calculated value is 10 times lower than the value determined using MIRD. On the other hand, the higher value of 3.8 ± 1.4 Gy/GBq, reported by Okamoto et al., 15 was calculated using 177Lu-PSMA Imaging & Therapy (177Lu-PSMA I&T), and considering the mean mass for lacrimal gland as 0.8 g. Mass of the organ is one of the critical aspects that determines the absorbed dose to the organ. However, for lacrimal glands, no data related to its mass are available for reference man. For this study, mass of the lacrimal glands is taken as 1.6 gm, as given by Bukhari et al. for Indian population. 27 Considering the safe dose of 40 Gy to the lacrimal gland, 28 this study predicts that a cumulative activity of 32.5 GBq (878 mCi) of 177Lu-PSMA-617 is safe to be administered in mCRPC patients.
Another critical organ that received high absorbed dose is the salivary glands. In this study, the absorbed dose to salivary glands was found to be 0.53 ± 0.25 Gy/GBq, which is comparable with the data reported in the literature. 13,15 –17 However, few other dosimetric studies reported the absorbed dose to the salivary glands is in the range of 1.17–1.4 Gy/GBq. It is pertinent to mention that in those groups of studies, the mass of salivary glands was taken much less than 85 gm, as given by ICRP 89 for reference man. 29 In this study, with maximum dose of 21.15 Gy to the salivary glands in 5 therapy cycles, no incidence of xerostomia was observed. This study also predicts that a cumulative activity of 60 GBq (1.62 Ci) 177Lu-PSMA-617 could safely be administered in patients, considering 32 Gy is the safe dose for the salivary glands based on external beam radiotherapy data. 26
The absorbed doses for tumor lesions, lacrimal glands, salivary glands, kidney, liver, spleen, urinary bladder, and red marrow, and effective dose to the whole body in this study were found to be comparable with the doses reported in the literature; the comparison of this study results and data available in literature are presented in Table 6. A comparison of the doses received by various organs in five consecutive therapy cycles on the same patients was attempted during this study, and this revealed that for kidney, salivary glands, and nasal mucous membrane, the absorbed dose was increased from first therapy cycle to second therapy cycle, and then slowly decreased in subsequently therapy cycles. However, for spleen, liver, and lacrimal glands, absorbed doses decreased with the successive therapy cycles, whereas in case of bone marrow, bladder, and whole body, the mean absorbed dose almost remained constant in each therapy cycle. Kratochwil et al. 7 compared 4 patients' data with two cycles of treatment and reported that there was no relevant difference in the kidney and red marrow dose between the first and second treatment cycle. Okamoto et al. 15 did comparison of four different cycles and found that absorbed doses were relatively constant among the four cycles.
Comparison of Absorbed Doses (Gy/GBq) for Normal Organs and Tumor Lesions Obtained in This Study and Available Literature Data
No data available.
Parotid gland.
Submandibular gland.
Left kidney.
Right kidney.
Bone lesions.
Tumor metastasis in Nodes.
Calibration standard model thyroid.
The results reported in this study for tumor dosimetry compare well with the data published in the literature. 4,13 –16 It was observed that tumor absorbed dose decreased with the increase of the number of therapy cycles, which is akin to that reported by Scarpa et al. 13
A few limitations of the study need to be mentioned here: due to the aggressiveness of the disease, a number of patients expired during the course of treatment, so the number of patients completing five therapy cycles were less. Also, due to the nonavailability of the SPECT-CT and integrated ROI and dose calculations tools, only 2D dosimetry results were produced; however, care was taken to avoid the overestimation of organ/tumor doses due to overlapping organs/tumors.
Conclusion
The dosimetry studies performed with 177Lu-PSMA-617 in 30 patients involving 65 177Lu-PSMA-617 PRLT administrations revealed that this indigenous radiopharmaceutical can be safely administered for the treatment of mCRPC patients. The agent delivered significantly higher dose to the tumors compared to other critical organs. The agent also exhibited high tumor-to-kidney ratio. The organ, whole body, and tumor absorbed doses obtained during this course of work were comparable to the data reported in the literature for the same ligand as well as 177Lu-PSMA I&T. Lacrimal glands followed by salivary glands received the highest absorbed doses among the normal organs. Extrapolating the safe dose data from external beam therapy, a cumulative activity up to 32.5 GBq (878 mCi) of 177Lu-PSMA-617 can be safely administered in patients in 4–5 therapy cycles to achieve the full therapeutic window with limited radiation-induced side effects to normal organs and this may probably increase the chances of a better outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was recieved for this article.