
Abstract
Background:
Esophageal cancer (EC) is an aggressive neoplasm of the gastrointestinal tract that is usually treated with a combination of chemotherapy, radiotherapy (RT), and/or surgery, according to disease status. Despite the availability of multimodal therapeutic strategies, local recurrence is frequently observed. Immunotherapy is a promising therapeutic approach that is currently highly investigated in association to standard therapies, including RT, with the aim to improve patients' outcomes.
Materials and Methods:
A PubMed search was performed with the following keywords in all fields: “esophageal cancer” and “radiotherapy” and “radiation” and “immunotherapy” and “PD-1” and “PD L1.” For an overview of ongoing trials, an additional search on
Conclusions:
Published results encourage the use of personalized therapeutic approaches for EC patients in the future; results from ongoing studies will help to identify the optimal strategies for patient selection and treatment response evaluation.
Background
Esophageal cancer (EC) is an aggressive neoplasm with poor prognosis. It ranks seventh in terms of incidence (572,000 new cases) and sixth in mortality (509,000 deaths) worldwide. 1
EC incidence is higher in some areas of Asia and Sub-Saharan Africa, as well as in several high-income countries (e.g., the United States, Australia, France, and the United Kingdom).
Between the two most common histologic subtypes, in recent years there has been a gradual decrease in esophageal squamous cell carcinoma (ESCC), probably due to the reduction in smoking habits, and an increasing of esophageal adenocarcinoma (EAC) histotype linked to obesity and gastroesophageal reflux disease, especially in the United States and Europe countries. Nevertheless, ESCC still represents the most common histotype with 78% of cases. 1 –3
According to the latest ESMO guidelines, surgery is the treatment of choice in limited disease, including stage cT1–T2c N0 M0. However, for those patients unable or unwilling to undergo surgery, combined chemo-radiotherapy (CRT) can be used. Conversely, in locally advanced disease (cT3–T4 or cN1-3M0), surgery alone is not the standard treatment. In operable patients it has been demonstrated that CRT (or chemotherapy alone) as neoadjuvant treatment increases R0 resection and survival rates. 4
Despite current multimodal therapeutic approaches, local recurrence of EC is frequently observed.
The promising results achieved by immunotherapy in the treatment of different aggressive neoplasms, such as nonsmall cell lung cancer (NSCLC) and metastatic melanoma, have encouraged the research and application of this novel approach also in advanced and refractory EC. In this scenario, interesting results from multimodal therapeutic strategies that include immunotherapy with radiotherapy (RT)/CRT are expected. 5 –7 Nevertheless, challenges in understanding the role and the resistance mechanisms of immunotherapy agents in EC still remain; further results from appropriate prospective studies are needed to assess the synergistic effect of immunotherapy and RT delivered with standard or novel fractionation regimens.
The authors provide an overview of current knowledge and future perspectives about the potential efficacy of combining immunotherapy with RT to improve the prognosis of EC patients.
Search Strategy
The search strategy to analyze the role and application of immunotherapy with or without RT in EC patients, including gastric carcinoma (GC) and esophagogastric junction carcinoma (EGJC), was specifically focused on original article.
For this purpose, a PubMed search was performed entering the following keywords in all fields: “esophageal cancer” and “radiotherapy” and “radiation” and “immunotherapy” and “PD-1” and “PD-L1.”
Articles edited in English from 2002 until 16th March 2020 were initially included. Exclusion criteria were as follows: sample size <40, objective not in the inclusion criteria, abstract, review, case report, and case series. Only for the “Abscopal effect” section, in absence of original articles, did the authors use case reports to discuss the topic.
For an overview of ongoing trials, the authors performed an additional search on
Results about their search strategy are reported in Figure 1.
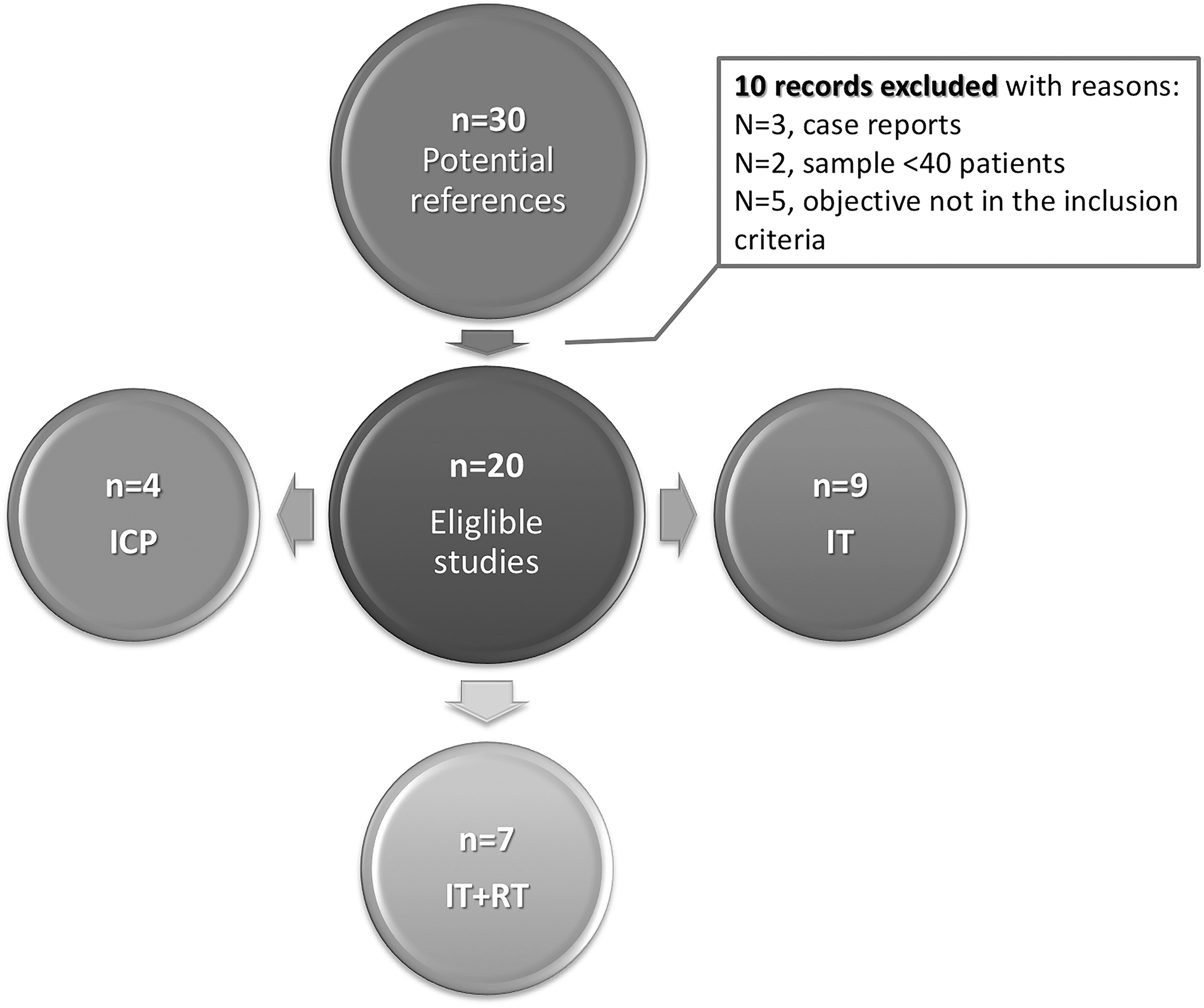
Original article selection workflow. Search strategy: esophageal cancer AND immunotherapy AND radiotherapy; esophageal cancer AND radiation AND PD-L1; esophageal cancer AND (PD-L1 or PD-1) AND radiotherapy. ICP, immune checkpoint; IT, immunotherapy; RT, radiotherapy; PD-1, programmed death-1.
Supplementary articles, additional references, or review articles were eventually considered to discuss general aspects.
Basics and Application of Immunotherapy for EC Patients
Immunomodulation mechanisms and immune-checkpoint expression
Tumor recurrence has been correlated to anomalies in the delicate equilibrium between tumor and host immune surveillance. 6,8,9
The host immune system is able to distinguish between normal and neoplastic cells and plays a regulatory role in the tumor progression. 8 –10
Nevertheless, tumor cells can escape from the host immune control using multiple defensive mechanisms, which include the inactivation of cellular systems involved in the major histocompatibility complex (MHC)-I pathway and the activation of CD4 regulatory T lymphocytes characterized by immunosuppressive activity. 9,11 Furthermore, tumor cells can inactivate the dendritic cells (DC) that are generally involved in the maturation of cytotoxic T lymphocytes in normal tissues—also including esophagus—through the phagocytosis of apoptotic tumor cells and the presentation of tumor-associated antigens. Also pro-angiogenetic factors in tumor microenvironment have been shown to alter DC activity, and immunogenic response, as well as hypoxia in tumor microenvironment, can promote tumor progression by suppressing natural killer cells. 6,9,11
Tumor cells are also capable to reduce the efficacy of the “active antitumor immune surveillance” through the activation of the programmed death-1 (PD-1) receptor—a checkpoint inhibitor located on the surface of cytotoxic T cell—and the expression of PD-ligands (PD-L1 and 2). In some tumors, also the inhibitor receptor cytotoxic T lymphocyte antigen 4 (CTLA-4), which reduces the stimulation of CD4 T helper and CD8 T lymphocytes, resulted to be upregulated. 10,12,13
To enhance the antitumor immune surveillance and antagonize the aforementioned mechanisms of tumor immune escape, novel immunotherapeutic strategies have been proposed also in EC.
Even if EC has been conventionally considered as a poor target for immunotherapy, due to the variable rates of tumor mutational burden and T lymphocyte infiltration, immune checkpoints (PD-1, PD-L1) have confirmed to be expressed in immune-escaping EC cells. 6,12,13 Therefore active immunotherapy with specific antibodies started to be investigated, and clinical results of new drugs targeted to these immune checkpoint are of great interest in translational research. 6,12 –14
PD-1 is a negative costimulatory receptor expressed mainly on activated T cells, 10 which downregulates excessive immune responses by binding to its ligands, PD-L1 and PD-L2.
PD-L1 is constitutively expressed in various tissues and on an expanding list of several tumor types, including EC. 11,15 PD-1 blockade is postulated to work during the T cell effector phase to restore the immune function of exhausted T cells following extended or high levels of antigen exposure, as occurring in advanced cancer. 8 Moreover, even the tumor-infiltrating lymphocytes play an important role in regulating signaling pathway in the immune response and it is highly variable in different types of tumors.
The study of immune checkpoint in patients with EC has been evaluated to identify new strategies for personalized medicine.
Above all, the PD-L1 expression on tumor cells and tumor-infiltrating cells has been evaluated in relation to prognosis. A retrospective study conducted on 428 patients with EC demonstrated that about 80% resulted as PD-L1 positive. Patients were divided in two groups according to treatment received: definitive treatment versus palliative care. In definitive treatment cohort, PD-L1 positivity was significantly related with a worse disease-free survival (DFS) and overall survival (OS). No significant association was found in the palliative treatment cohort. 16
Similar results have also been achieved by Hynes et al. in their study where PD-L1 positivity was found to be associated with significantly lower survival in specimens of patients who underwent esophagectomies for EAC. 17
More recently, Rong et al., 18 using tissue microarray and immunohistochemistry, studied PD-L1 expression on tumor cells and tumor-infiltrating cell in 378 advanced (T2–T4a) ESCC. No patient recruited had undergone neoadjuvant chemotherapy that could have changed PD-L1 exposure. On tumor cells, PD-L1 expression was positive in 29.9% of patients and higher in poor differentiating ESCC, whereas on tumor-infiltrating immune cells, PD-L1 expression was 40.2% and significantly associated with N stage (p < 0.05). They also evaluated the correlation between PD-L1 expression and prognosis: PD-L1 positive expression on tumor cell resulted in a significantly shorter DFS (p = 0.008). In addition, the median OS was 60 months in PD-L1 negative patients compared to 36 months in PD-L1 positive ones. 18
Although PD-L1 overexpression in EC is estimated to be considerably lower than in other cancers, the evidence that PD-L1 expression may be related to prognosis has paved the way for the introduction of new target therapies. 19
Clinical trials about immunotherapy in GC, EGJC, and EC
Over the years, studies on the effectiveness of immunotherapy with or without standard therapy have led immune-checkpoint inhibitors to the approval by the Food and Drug Administration (FDA) already in several tumors and in different line therapies, such as in NSCLC or head and neck squamous cell carcinoma. 20
Due to the lack of randomized clinical trials in patients with EC, to date scientific evidence is currently based on clinical studies in patients with GC or EGJC. 21 Pembrolizumab is a high-affinity, humanized monoclonal antibody against PD-1 that blocks interaction between PD-1 and its ligands, which has been licensed by the U.S. FDA in third-line or more advanced PD-L1 positive (>1%) GC.
The introduction of this monoclonal antibody into clinical practice has been supported by clinical studies that have evaluated its safety and tolerability, as well as the prognosis of the treated patients. Interesting results were reported by Fuchs et al. 22 in 2018, from the large phase II Clinical KEYNOTE-059 Trial. The study enrolled 259 recurrent or metastatic GC or EGJC patients with progression disease after two or more prior chemotherapy regimens, demonstrating that pembrolizumab elicited durable objective responses in 30 patients (11.6%) and complete response (CR) in 6 patients (2.3%). Moreover, 95 patients (42.4%) experienced reduction in measurable tumor size. Only 46 patients (17.8%) experienced a grade 3–5 treatment related adverse events (AEs). The objective response rate (ORR) was higher in patients with PD-L1-positive versus PD-L1-negative tumors (15.5% vs. 6.4%, respectively), as well as longer response duration in patients with PD-L1-positive tumors was observed (16.3 vs. 6.9 months). 22
Based on these encouraging results, other clinical trials started evaluating the potential role of pembrolizumab also in EC, particularly as third line of therapy in advanced stage.
The anti-programmed death-1 pembrolizumab was evaluated also in the phase II KEYNOTE-180 study which enrolled 121 patients with advanced metastatic EC that progressed after two or more lines of therapy. An ORR of 9.9% in all patients was observed. The 6-month progression-free survival (PFS) rate was 16%, and the median OS was 5.9 months, with a 6-month OS rate of 49% and a 12-month OS rate of 28%, suggesting encouraging survival outcome. 23
Following the phase II KEYNOTE-180 trial, the KEYNOTE-181 study evaluated pembrolizumab versus chemotherapy as second-line treatment in patients with advanced EC. The 628 patients were randomly assigned to receive pembrolizumab at 200 mg every 3 weeks for up to 2 years or investigator's choice of paclitaxel, docetaxel, or irinotecan. Available preliminary results showed that although pembrolizumab was of significant benefit in patients with a PD-L1 combined positive score (CPS) ≥10; it did not improve OS or PFS in the overall intent-to-treat population. A trend was observed favoring pembrolizumab in patients with ESCC: median OS was 9.3 months with pembrolizumab versus 6.7 months with chemotherapy (p = 0.0074). 24
Further analysis exploring the role of Pembrolizumab in earlier lines of therapy exists for GC and EGJC in KEYNOTE-061 and KEYNOTE-062 studies.
In KEYNOTE-061 phase III study, pembrolizumab was compared with paclitaxel in patients with advanced GC or EGJC that progressed on first-line chemotherapy with platinum and fluoropyrimidine. In 395 patients, who had a PD-L1 CPS ≥1, Pembrolizumab did not show to significantly improve OS compared with paclitaxel. However, pembrolizumab demonstrated a better safety profile than paclitaxel. 25
As first-line approach pembrolizumab was tested in the randomized, phase III KEYNOTE-062 still ongoing trial. Preliminary results demonstrated that primary end point was achieved, showing that for patients with PD-L1 positive, HER2-negative, advanced GC, or EGJC, initial therapy with pembrolizumab resulted in no inferior OS compared with standard chemotherapy. In addition, pembrolizumab showed clinically meaningful improvement in OS among patients with tumors that had high levels of PD-L1 expression: at 2 years, 39% of patients who received pembrolizumab alone were alive, compared with 22% of people who received standard chemotherapy. Conversely, when used in combination, pembrolizumab and standard chemotherapy did not improve survival compared to chemotherapy alone. 26 The randomized placebo-controlled Phase III KEYNOTE-590 (NCT03189719) focuses this setting, studying the safety and efficacy of Pembrolizumab in combination with chemotherapy as first-line treatment specifically in advanced EC. 27 However, results from this active but not recruiting trial are not available yet.
Another humanized monoclonal antibody to PD-1 is Nivolumab. As for pembrolizumab, nivolumab was first tested in GC.
ATTRACTION-2 was the first pivotal phase III, placebo-controlled, randomized, and licensing trial that reported nivolumab in third- or subsequent-line therapy. This study recruited 493 randomized patients, not selected according to PD-L1 status, that receive nivolumab or placebo (2:1). Nivolumab resulted in statistically superior OS, PFS, and ORR (11.2%) compared with placebo. Twelve-month OS rates were 26.6% versus 10.9%. After this large study, nivolumab has obtained a license in advanced GC in Japan. 28
Subsequently, in ATTRACTION-4 (phase II/III trial) study, nivolumab was evaluated as first therapeutic line in combination either with oxaliplatin (SOX) or with capecitabine plus oxaliplatin (CapeOX) for unresectable advanced or recurrent GC/EGJC. This study demonstrated a manageable safety profile and clinical relevant antitumor activity of combined nivolumab-chemotherapy treatment. An objective response (CR or PR) was observed in approximately two-thirds of patients regardless of the chemotherapy regimen administered with nivolumab and it was independent of tumor PD-L1 status. A clinically relevant PFS for the overall population was found (9.7 months). 29
Nivolumab was evaluated also in patients with treatment-refractory EC in an open label, multicenter phase 2 trial. The study was conducted on 64 patients, unselected for tumor PD-L1 positivity. An ORR of 17% in all patients was observed, and 42% achieved disease control, which suggests the ability of Nivolumab to reduce tumor burden. The median OS was 10.8 months. Nivolumab showed also a manageable safety profile. 30
In this context, a multicenter, randomized, open-label phase 3 trial, ATTRACTION-3, deserves particular mention. Four hundred nineteen patients with unresectable advanced or recurrent ESCC (regardless of PD-L1 expression) were enrolled. Patients were randomly assigned (1:1) to either nivolumab or investigator's choice of chemotherapy (paclitaxel or docetaxel). At note, OS was significantly improved in the nivolumab group compared with the chemotherapy group (10.5 vs. 8 months, respectively). The safety profile was also acceptable compared to the control group. 31
All the above-mentioned studies are summarized in Table 1.
Main Study References About Clinical Application of Immunotherapy in Gastric Carcinoma, Esophagogastric Junction, and Esophageal Cancers
Preliminary result (abstract 4010).
EAC, esophageal adenocarcinoma; ESCC, esophageal squamous cell carcinoma; EGJ, esophagogastric junction; EGJC, esophagogastric junction carcinoma; GC, gastric carcinoma; PFS, progression free survival; OS, overall survival; ORR, objective response rate; AE, adverse event; CPS, combined positive score.
However, it is known that, after an initial response to immunotherapy, unfortunately disease relapse can occur. This is probably due to the acquired resistance to immunotherapy agents related to epigenetic variations in immune surveillance pathways, anomalies in tumor antigen presentation (due to variations in MHC I expression), and alterations in tumor microenvironment. For example, alterations of microbiome have been shown to correlate with immunotherapy resistance, although mechanisms of cross reactivity between patient-specific microbiome and tumor antigens are still unclear. 12
For this reason, personalized therapeutic strategies and further multimodal immunotherapy approaches have to be studied to overcome the resistance mechanisms.
Immunotherapy Combined with RT: A Synergic Approach
RT in esophageal carcinoma: use and disadvantages
RT is a fundamental part of standard treatment for EC. Recommended RT doses in the neoadjuvant setting are in the range of 41.4–50.4 Gy; when RT is performed as definitive approach, total radiation dose is generally 50–50.4 Gy. 10
The introduction of intensity-modulated radiotherapy (IMRT) and volumetric modulated arc therapy could allow to reduce the overall treatment time increasing radiation doses up to 60 Gy in fractions of 1.8–2.0 Gy. Nevertheless, currently there is no sufficient evidence that RT doses higher than 50.4 Gy can be useful to improve outcome in patients with EC, without increasing morbidity and mortality. In metastatic disease, palliative single-dose brachytherapy may be a preferred option, even after external RT, improving long-term relief of dysphagia. 12
However, it should be considered that chest radiation could present some complications. The most important one is related to postactinic pneumonia characterized by cough, fever, and dyspnea, with or without radiological signs, in an acute phase and by fibrosis in a chronic phase. At the same time, dysphagia, odynophagia, anorexia, and retrosternal pain may occur following RT.
Deng et al. in a recent interim report of a prospective phase III, randomized controlled study evaluating postoperative RT in pathological T2-3N0M0 thoracic ESCC underlined that adjuvant RT could improve DFS and decreased local region recurrence rate. 32 However, evidence is not sufficient, and recurrence remains frequent. Recent data indicate local-regional recurrence rates of 35.7%–41.8%, which account for the major failure pattern rather than systemic metastases. 33 –35
Immune-mediated RT-induced mechanisms
Radiation produces multiple biological effects, which are involved in tumor cell damage and death. These mechanisms include DNA damages that tumor cells are not able to repair and the induction of “immunogenic tumor cell death,” which is an immune-mediated radiation-induced mechanism that produces antitumor specific immune cells. 5,8,9 In other terms, local irradiation of tumor sites produces several immunomodulation effects that counteract tumor progression by inducing a tumor-specific immune response. 5,36,37 Indeed, neoplastic cells dying due to radiation effects can expose tumor-specific surface antigens, which activate DC. 13 DC are also activated by additional radiation-induced molecular mechanisms, such as the extracellular release of calreticulin, high mobility group box B1 proteins, damage-associated molecular patterns, and shock proteins HSP. 8,37,38 Subsequently, DC are able to activate tumor-specific cytotoxic T lymphocytes, which can induce the “immunogenic tumor cell death.”
As reported above, besides the activation of DC and cytotoxic T lymphocytes against tumor cells, RT can induce immune-stimulatory and pro-inflammatory factors, such as tumor necrosis factor α and interleukins (ILs) involved in antitumor immunity. 8,9,37
Another mechanism at the basis of the synergism between immunotherapy and RT is the suppression of immune checkpoint inhibitors. 36 Indeed, it has been suggested that RT has the potential to enhance the effects of immunotherapy agents by upregulating PD-L1 expression in the tumor microenvironment. 7,12,13,39
Some studies evaluated the effects of neoadjuvant therapy on tumor microenvironment and the expression of some checkpoints in patients with EC, demonstrating that multiple key immune-inhibitory ligands, receptors, and metabolic enzymes were highly upregulated in tumors postchemoradiation compared to baseline samples. 40
In a retrospective study, Lim et al. 41 assessed the PD-L1 expression changes in a group of patients with locally advanced ESCC treated with neoadjuvant CRT compared to the control group treated with neoadjuvant chemotherapy alone. They found significant differences in PD-L1 expression after neoadjuvant treatment between CRT and chemotherapy groups (p < 0.001). In particular, PD-L1 significantly increased after neoadjuvant CRT (p = 0.007) and significantly decreased after neoadjuvant chemotherapy (p = 0.048). 41
About this topic, Zhang et al. showed promising results also in the adjuvant RT. The authors found an increasing expression of PD-L1 during the irradiation of EC cell lines with the standard fractionation regimen (2 Gy per fraction). 42 In addition, in patients treated with adjuvant RT, the prognosis was significantly improved. 16
Already in 2016, Chen et al. 43 highlighted, through in vitro experiments, how PD-L1 level was increased by RT in the plasma membrane and in the cytoplasm of EC cells compared to nonradio-treated cells. The authors stated that irradiation increased the ability of tumor cells to suppress nonspecific stimulation (anti-CD3/CD28 antibody)-mediated T cell proliferation, and anti-PD-L1 attenuated the ability of irradiated tumor cell-mediated T cell suppression. Then, the PD-L1 inhibition combined with irradiation resulted in increased tumor cytolysis compared with anti-PD-L1 monotherapy or irradiation alone when tumor cells cocultured with sorting CD8+ cells from patients. 43
For all these reasons, preliminary clinical results were achieved by testing adoptive cytokine-induced killer cell and DC in association with RT. In particular, Yan et al. 44 compared the above-mentioned association with RT alone in a randomized trial in elderly EC patients. Authors reported higher time-to-progression rate and treatment efficacy in the study group compared to control group, with improved patients' quality of life and satisfactory treatment tolerance. 6,44
Similarly, Wang et al. 45 showed that levels of interferon-γ, IL-2, and IL-12 were significantly increased after receiving RT plus immunotherapy with DC loaded with heat shock-induced apoptotic tumor cells, indicating that DC immunotherapy could enhance in vivo antitumor immunity and trigger Th1 immune response in tumor patients. Supporting these results, changes of cytokine levels were not found in patients only receiving RT. 45
Despite these promising results, both these studies presented some limitations. First of all, sample size was too small to observe relationships between increase of T cell subgroups and survival. In addition, patients were highly selected (e.g., at the early stage [I–II] in the Wang et al. 45 study), follow-up time was relatively short, and data about recurrence were not collected. Additional multicenter trials are necessary to allow the wide use of DC vaccine against EC.
Ongoing trail of combined RT and immunotherapy: new drugs and future prospective
The effectiveness of combination CRT with immunotherapy has been already proven in NSCLC, for the treatment of surgically unresectable stage III patients. The PACIFIC trial validated the efficacy of durvalumab (anti PD-L1) as second line, allowing it final approvation by the FDA on February 2018. 46
The scientific evidences on other solid tumors and the above-mentioned immunogenic mechanisms have led to the development of new clinical trials that explore the combination of CRT with immunotherapy also in patients with advanced EC to open the scenario to new personalized therapeutic strategies.
Pembrolizumab has been studied in association with RT in EC in some active trials. Most of them have recently completed recruitment without any evidence yet. However, among these trials, a pilot study evaluates treatment tolerability combining two fractions of brachytherapy followed by pembrolizumab for the treatment of metastatic EC. Secondary outcome measures are estimating both local and systemic antitumor effects, as well as OS and PFS (NCT02642809).
OS and event-free survival are also the first end point in the ongoing KEYNOTE-975 phase III trial that aims to assess if definitive CRT + pembrolizumab is better than definitive CRT + placebo. These results are going to be related with PD-L1 status in the enrolled patients.
Currently, the ongoing NCT03416244, a multicenter open-label phase II trial (RAMONA), is evaluating Nivolumab in monotherapy or in combination with Ipilimumab (CTLA-4 antibody). This study enrolled confirmed advanced stage nonresectable ESCC patients beyond frontline therapy (chemotherapy ± RT or palliative systemic chemotherapy), including stage IV, stage III nonresponder to CRT, any relapsed patients after CRT or surgery, and any patient ineligible or intolerant to standard therapies or refuses other treatment. The first end point is to assess the OS, as well as the efficacy and safety, considering several prognosis parameters.
The addition of CRT in the two previously described study arms is the goal of NCT03437200 trial, evaluated in inoperable patients with early or locally advanced EC.
The INEC (phase I/II) trial (NCT03544736) is a three parallel cohort clinical trial which aims to analyze safety and feasibility of PD-1 inhibition with Nivolumab given concomitantly with standard RT regimens. The three cohort study includes: advanced/inoperable EC, eligible for palliative RT of the primary tumor (Cohort A), inoperable EC without metastases, eligible for definitive CRT (Cohort B), and operable EC, eligible for neoadjuvant CRT (Cohort C).
Among the active trials about this topic that have completed the enrollment, CheckMate-577 phase III study randomized 760 patients to receive Nivolumab or Placebo treatment. All patients included had completed preoperative CRT followed by surgery, with negative margins after complete resection. The goal is to establish DFS and OS.
Toripalimab is another anti-PD-1 antibody drug undergoing further multiple clinical trial evaluation. It is evaluated in ongoing NCT04005170, a phase II trial, as first-line combined with definitive CRT in unresectable locally advanced ESCC. The protocol provides that all patients will receive IMRT scheme: 50.4 Gy in 28 fractions over 5–6 weeks, concurrently with five cycles of paclitaxel/cisplatin on days 1, 8, 15, 22, 29 and two cycles of toripalimab on days 1, 22 followed by a maintenance phase with toripalimab every 3 weeks for up to 1 year. Tumor response will be evaluated 3 months after treatment completion, based on computed tomography (CT) or positron emission tomography PET/CT scans and endoscopy with biopsies.
At the same time, NCT04006041 trial is ongoing to evaluate the toripalimab combined with neoadjuvant CRT in patients with resectable thoracic ESCC (T1-4aN1-3M0 or T3-4aN0M0). All patients will receive IMRT concurrently with four cycles of paclitaxel/cisplatin on days 1, 8, 15, 22 and two cycles of toripalimab on days 1, 22. Esophagectomy is performed 6–8 weeks after treatment completion and estimating the pathologic complete response rate.
Other ongoing clinical trials are also evaluating Durvalumab, including ARION study (NCT03777813) that randomizes 120 patients, in 12 centers in France, to assess this anti-PD-L1 inhibitor efficacy in combination with CRT (FOLFOX and IMRT) and then as maintenance therapy for treating patients with localized unresectable EC.
The main ongoing trials discussed are reported in Table 2.
Ongoing Clinical Trials Involving Immune Checkpoint Inhibitors With or Without Radiotherapy
Frontline therapy is defined as chemotherapy (±radiotherapy) (e.g., CROSS, FLOT, or similar protocols) OR any palliative systemic chemotherapy.
EC, esophageal cancer; CRT, chemo-radiotherapy; RT, radiotherapy; IMRT, intensity-modulated radiotherapy; EFS, event-free survival; DFS, disease-free survival; PD-1, programmed death-1.
Many other trials are ongoing to demonstrate how the combined effect of CRT with immunotherapy can represent a turning point in the treatment of EC.
However, it should be emphasized that immunotherapy is not without risk. Immune-related AEs of concern include dermatological, gastrointestinal, hepatic, endocrine, and other, less common, inflammatory events. The incidence of respiratory immune related adverse events (irAEs) in trials with anti-PD-1 agents equaled to up to 13%, with only 2% being grade ≥3 in trials of lung cancer, with interstitial pneumonitis as the most frequent irAE of the respiratory tract. 47,48 As previously described, also RT can be complicated by actinic pneumonia. Therefore, given the limited evidence regarding the side effects of radiation therapy combined with immunotherapy, it is important to consider lung involvement in further clinical studies to prevent this eventuality.
Only few data have been reported on toxicity related to immunotherapy combined with standard therapies in the past years. Of note, immunotherapy agents can produce autoimmune effects, which mainly affect the skin and the gastrointestinal tract. Van den Ende et al. have recently reported two cases of acute cutaneous toxicity during the administration of CT and Atezolizumab (a PD-L1-targeted antibody) for resectable EC. The cumulative toxicity risks after the administration of immunotherapy with CT and/or RT in EC patients are not well known due to the lack of long-term clinical data from adequate patient cohorts. 49
Abscopal effect
Among the immune-mediated RT-induced mechanisms, the abscopal effect deserves particular mention as an impressive example of existing correlation between antitumor immunity and RT.
Stimulating antitumor immunity, RT activates cytotoxic T lymphocytes that are able to induce a cytotoxic effect on neoplastic cells localized in sites distant from the irradiated area. This phenomenon has been observed in anecdotic clinical experiences as the disappearance of metastatic lesions, which were far from the irradiated tumor site. 8,37
There is now a growing consensus from many studies indicating that combining RT with immunotherapy provides an opportunity to boost abscopal response rates.
Over the years, the abscopal effect has been reported for several cancers. For example, it was described in a case report by Postow et al. about a patient affected by metastatic melanoma who had a systemic response to localized RT after disease progression during ipilimumab treatment. 50 Further supporting data stating that disease regression at distant sites is due to an enhanced systemic response combining RT and immunotherapy are derived from some preclinical studies about colon/colorectal carcinoma. 51,52
About this topic, even for the EC, there are only few scientific evidences. Zhao et al. reported an abscopal effect in a 65-year-old male patient affected by EC with multiple lymph node metastases who was treated with CT, Pembrolizumab, and Cyberknife. 53 RT was delivered to a retroperitoneal lymph node with a total dose of 42 Gy in six fractions. Two months after RT all lymph node metastases were undetectable at radiological reevaluation. 53
High radiation dose/fraction, such as those prescribed in stereotactic regimens, has been suggested to better support immunogenic mechanism, which induces the abscopal effect. 54
Because the available literature mostly consists of case reports and preliminary studies, more randomized clinical trials are needed to investigate abscopal effect value, reducing toxicity as much as possible.
Conclusions
The possibility of exploiting the synergistic effect between novel or well-established immunotherapy agents and RT or CRT could support future personalized therapeutic approaches for EC patients in the perspective of “precision oncology” strategies.
Although studies of a possible combination of immunotherapy with radiation therapy in EC are still in early phases, the initial results are promising particularly for disease control and toxicity outcomes.
However, it should be remembered that, compared to other solid tumors in which the immunomodulation mechanisms are better specified, many aspects remain to be clarified in EC. Ongoing studies will provide extensive data and will help to clarify existing challenges in establishing the optimal strategies for patient selection and treatment response evaluation.
Authors' Contributions
A.S. developed the idea and organized the work; C.F. performed the bibliographic research and organized the work; R.C. was the major contributor in writing the article; C.A. performed the bibliographic research; V.L. finalized the article; G.R. supervised the article. All authors have read and agreed to the published version of the article.
Footnotes
Disclosure Statement
There are no existing financial conflicts.
Funding Information
No funding was received for this article.