
Abstract
Background:
Colorectal peritoneal carcinomatosis (CRPC) is a primary cause of death in colorectal cancer (CRC) patients. In the past, computed tomography (CT) has been the primary method used to evaluate the distribution of CRPC. This study uses 18F-FDG positron emission tomography/computed tomography (PET/CT) to investigate the distribution characteristics of CRPC.
Materials and Methods:
The distribution characteristics of 46 patients with CRC who were treated in the authors' hospital were retrospectively analyzed using the peritoneal cancer index (PCI).
Results:
The 46 patients in the study showed CRPC involvement in 203 of the 598 abdominal and pelvic regions studied (33.9%, 203/598). The regional proportions of CRPC involvement, from high to low, were as follows: region 6 (13.8%), region 0 (10.3%), region 1 (9.9%), region 5 (8.9%), region 7 (8.4%), region 3 (8.4%), region 2 (7.4%), region 4 (7.4%), region 11 (6.9%), region 8 (6.4%), region 12 (5.4%), region 9 (3.4%), and region 10 (3.4%). Thirty-three patients had a PCI of <20, and 13 patients had a PCI of ≥20. Those 13 were among the 17 (37% 17/46) who had CRPC involvement in all three regions. According to the location of the primary CRC focus, the 46 patients were divided into three groups: right hemicolon, left hemicolon, and rectum. The frequency of CRPC was greater in the rectum group than in the left hemicolon group, and the SUVmax of CRPC was greater in the right hemicolon group than in the left hemicolon group; these differences were statistically significant (p < 0.05).
Conclusions:
The distribution of CRPC has certain characteristics in the abdominal and pelvic cavities. The PET-PCI scores can provide a basis for the diagnosis and clinical treatment strategies in patients with CRC.
Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide and has the second highest cancer-related mortality. The pathological classification of CRC is primarily divided into mass type, ulcer type, and infiltrating type. At the time of initial diagnosis of CRC, 20%–30% of patients had tumor metastasis and had lost the opportunity for radical surgery, and 8% of these patients had peritoneal carcinomatosis (PC). In the 70%–80% of patients who received radical surgery, the incidence of metachronous PC reached 10% during the follow-up period. PC metastasis had the third highest recurrence frequency, behind that of the liver and lungs, and is the second leading cause of death in patients initially diagnosed with CRC. 1,2 In 2018, the Staging System of the American Joint Committee on Cancer refined the CRC grading system for distant metastasis and added the Mlc phase, meaning that peritoneal metastasis belongs to the IVC phase (AnyT, AnyN, and M1c). 3
In the past, colorectal peritoneal carcinomatosis (CRPC) was considered as end-stage CRC, with a survival time of fewer than 6 months, and patients received only supportive or palliative chemotherapy. In recent years, however, CRC patients with peritoneal metastasis are receiving the treatment mode of cytoreductive surgery (CRS) in combination with hyperthermic intraperitoneal chemotherapy (HIPEC). This treatment has a greater survival benefit, with an average overall survival of 46 months, and the possibility of a cure. 4 The first choice for evaluation of CRPC is noninvasive imaging, and the results will determine the clinical stages, the formulation of a treatment plan, and the evaluation of outcomes and prognosis.
At present, the Sugarbaker peritoneal cancer index (PCI), is the most commonly used grading system for CRPC load standardization and has been introduced from surgery to imaging study. The positron emission tomography/peritoneal cancer index (PET-PCI) can reflect histopathological features and appears useful for predicting recurrence in patients with PC. Previous imaging studies correlated to PCI focused on the ability of qualitative diagnosis 5 –8 However, few studies have investigated the distribution of PC through imaging, and these primarily relied on computed tomography (CT). 9 –11 Positron emission tomography/computed tomography (PET/CT) shows great advantages in clinical applications, and it was used to analyze the distribution characteristics and clinical significance of CRPC in the present study. The hypothesis of this study is that CRPC is formed by the spread of CRC tumor cells into the pelvic cavity and right abdomen, and this can provide a basis for clinical follow-up treatment and prognosis.
Materials and Methods
Study subject
The CRPC patients selected for this study were examined by PET/CT in the Center of Nuclear Medicine of the Affiliated Hospital of Nantong University between June 1, 2016 and August 30, 2018, and their data were retrospectively studied. This study was conducted in accordance with the declaration of Helsinki and approved by the Ethics Committee of Affiliated Hospital of Nantong University. Since the study did not entail direct patient involvement, it did not need informed consent from the patients.
Inclusion and exclusion criteria
Study patients had the following inclusion criteria: (1) a diagnosis of CRPC, (2) greater than 18 years old, (3) a PET/CT scan performed 6 months after surgery and 3 months after radiotherapy or chemotherapy, and (4) a blood tumor index that was completed 1 week before and after the PET/CT scan. Patients were excluded for the following reasons: (1) severe infection; (2) severe heart, liver, and kidney dysfunction; and (3) incomplete clinical data.
Diagnostic criteria of PC
CRPC determining standards: (1) pathological diagnosis of peritoneal lesions that was confirmed by surgical procedures or aspiration biopsies; (2) identification of tumor cells through the cytological testing of ascites; (3) an imaging examination (with two consistent findings) suggesting that the peritoneal lesions were reduced or disappeared after treatment, accompanied by a decrease in serum tumor markers; and (4) an imaging examination (two consistent findings) suggesting that the peritoneal lesions were progressive (an increase in morphology, diameter, and SUVmax) during the follow-up period, accompanied by a progressive elevation of serum tumor indices.
18F-FDG PET/CT imaging
The radioactive drug 18F-FDG was provided by Nanjing Jiangyuan Andiko Positron Research Development Co., Ltd. The requirement of FDG PET imaging was ≥95% for the purity. Before the imaging, patients fasted for 4–6 h, and their blood glucose levels (<11.1 mmol/L or <200 mg/dL) were monitored before the 18F-FDG injection. In addition, blood sugar regulation was performed for diabetic patients, with the blood sugar level higher than the normal reference value. After quietly resting for 5–10 min, the patients adopted a supine position and received a dose of 0.10–0.12 mCi/kg (3.70 × 4.44 MBq/kg), according to their body weight, through forearm vein access. The patients received a whole-body PET/CT scan after remaining supine for 45–60 min, urinating, and then drinking 500–1000 mL of water. A polycrystal Discovery™ PET/CT 710 device (GE Medical Systems, Milwaukee, WI) was used. This was equipped with a 64-row, 128-layer high-end spiral volume CT.
The MSCT scan was first carried out, with a scan voltage of 120 kV and a current of 180 mA (this is the median value of 160–200 mA of the current fixed in milliamps). The pitch was 1.375:1.000; the spiral time was 0.8 s per cycle; the bed speed was 22.5 mm/s; and the matrix was 512 × 512. The scan range was from the cranium to the middle segment of the femur. The PET images were collected in 3D mode. The thickness of the fixed scanning layer was 3.75 mm, and the matrix was 128 × 128. According to the height of the patient, six to eight beds were set up, with 2–3 min for each bed and 5 min for the head scan bed. Ordered subset expectation maximization was used or reconstructed, and the data were transferred to the AW workstation. The PET/CT image fusion and postprocessing were performed using Advance VolumeShare 5 (AW 4.6). CT, PET, and PET/CT fusion images were obtained from the cross-sections, coronal sections, and sagittal sections, respectively.
Image analysis
At present, the most commonly used PC grading system is the PCI grading system proposed by Harmon and Sugarbaker. 12 This system divides the abdominal cavity into 13 regions, which include 9 abdominal and pelvic regions (region 0: central, region 1: right upper, region 2: epigastrium, region 3: left upper, region 4: left flank, region 5: left lower, region 6: pelvis, region 7: right lower, and region 8: right flank) and four small intestine regions (region 9: upper jejunum, region 10: lower jejunum, region 11: upper ileum, and region 12: lower ileum) (Fig. 1). The diameter (lesion size [LS]) of the largest PC lesion among the 13 regions was separately measured for the comprehensive scores. Lesion size scores (LSS) were determined as follows: LSS-0 means no PC lesion; LSS-1 means that the diameter of the PC lesion is <0.5 cm; LSS-2 means the diameter of the PC lesion is between 0.5 and 5.0 cm; and LSS-3 means the diameter of the PC lesion is >5.0 cm (Fig. 1).

Anatomical structures involved in the 13 abdominopelvic regions of the PCI. The abdomen and the pelvis are divided into 13 regions. The LS of the largest sizes of the largest implants is scored (0 through 3) in each abdominopelvic region. They can be summated as a numerical score, which ranges from 0 to 39. LS, lesion size; PCI, peritoneal cancer index.
The comprehensive PCI scores of the study patients ranged from 0 to 39. If the boundary of a fused lesion could be distinguished, this was recorded as two or more lesions; if the boundary could not be distinguished, this was recorded as one lesion. Primary tumors and/or tumors with local recurrence that could be resected were not included. If tumors were fused with adjacent organs and could not be distinguished, this would score as LSS-3. The measurement of the LS is combined from the PET and CT images to determine the target lesion, using the CT image that showed the boundary. Otherwise, the LS was measured from the PET image (the left and right diameter or anteroposterior diameter were included to avoid the influence of respiratory movement).
Image analyses and data measurements were performed by two diagnostic physicians (each with more than 3 years of PET/CT experience). Using region of interest technology, the standardized uptake value (SUV) was automatically calculated in g/mL by computer. The indices, which included the distribution and shape of the PC loaded in each region, were obtained by visual inspection and semiquantitative analysis. The number, size, SUVmax, and PCI scores of each CRC patient were quantitatively analyzed. The quantitative value was measured by two doctors, and the mean value was obtained; a senior doctor resolved measurements, where the two doctors did not agree. Using the measurements from each case, the maximum value of the PC and SUVmax in all the regions of each patient was taken as the maximum value of PC and SUVmax of this patient. A higher PCI score means wider CRPC distribution, and the authors chose a PCI of 20 as a cutoff for this study.
Statistical methods
An Excel form was used to record and sort the data, and applied SPSS 19.0 statistical software was used to carry out the data processing. The measurement data were presented as mean ± standard deviation. The enumeration data were expressed in percentages. For multiple comparisons, each value was compared by one-way ANOVA following a Dunnetts test when each datum conformed to normal distribution; when a value did not conform to normal distribution, the data were compared using nonparametric tests. A chi-square test was used for counting data. The statistical results were analyzed by bilateral α = 0.05, and a value of p < 0.05 was considered statistically significant.
Results
General data
During the study period, 293 patients with CRC were examined at the hospital's PET/CT Center. Forty-nine of these patients (16.7%, 49/293) developed CRPC. Three patients were excluded because of metachronic gastric cancer, ovarian cancer, or abdominal infection, so the data of 46 patients were analyzed (Fig. 2). Five patients had two PET/CT examinations, and images from the first were used; 41 patients received only one PET/CT scan. The PC diagnoses of 12 patients were confirmed by surgery; diagnoses of five patients were confirmed by peritoneal aspiration biopsy; and diagnoses of 29 patients were confirmed by imaging examinations after treatment. Of those patients, the scope and volume of the PC had decreased in 7 (Fig. 3) and increased in 22 (Table 1 and Fig. 4).
This flow diagram shows information about inclusion and exclusion criteria leading to the selection of the study group of 46 patients with peritoneal carcinomatosis.
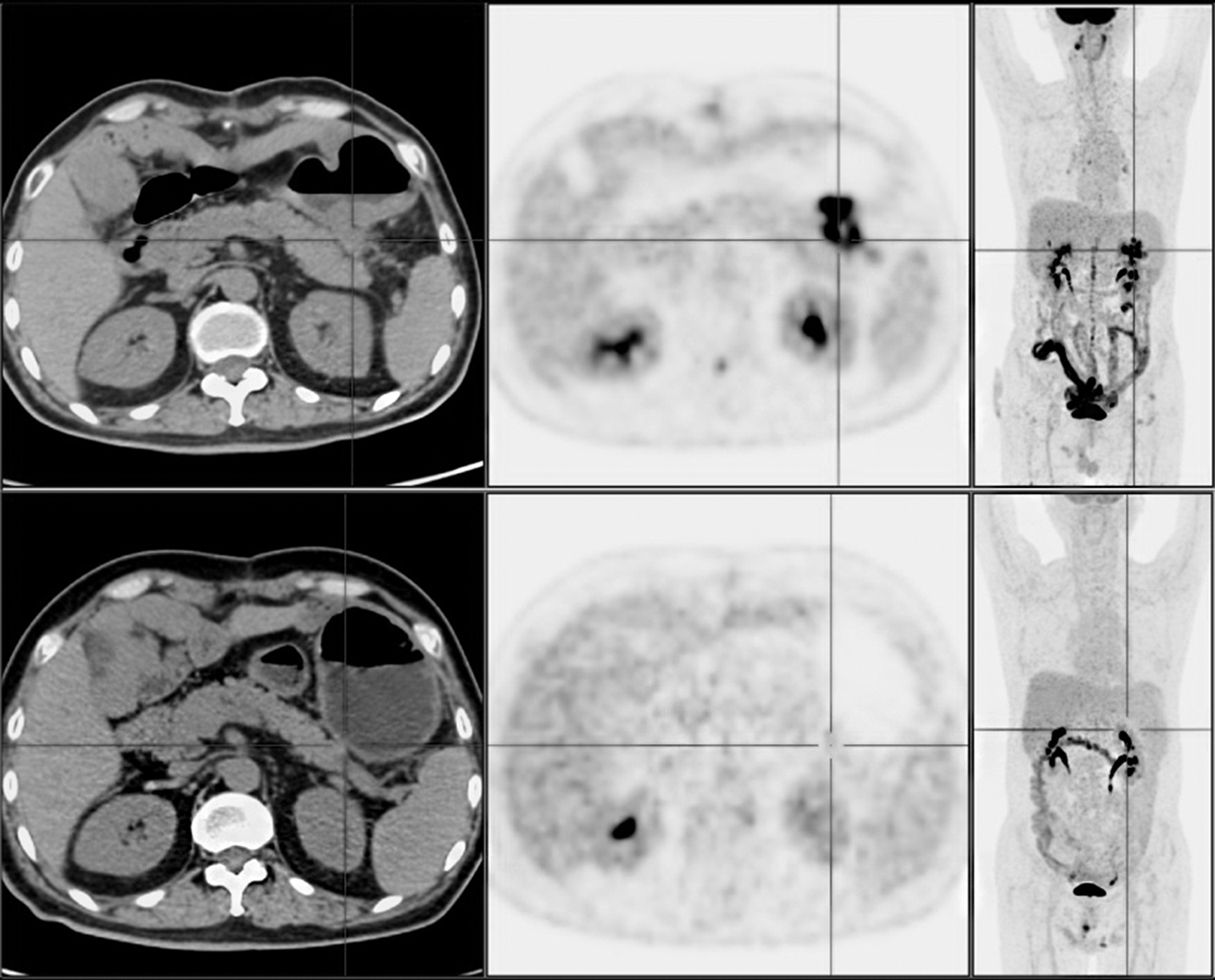
A 56-year-old male patient with poorly differentiated adenocarcinoma in the left hemicolon (splenic flexure of the colon). Colon cancer surgery was performed on May 17, 2017. The 18F-FDG PET/CT scan (the first row of images: axial plain CT scan image, same layer axial PET image, and 3D-MIP PET image, successively from left to right) was reviewed on September 5, 2017. The results revealed a plaque-like high-FDG uptake soft tissue density CRPC (cross, LS-2) in the left upper (region 3), and the SUVmax was 22.3. The patient's PCI score was 2. Cyfra21-1 was 2.8 ng/mL in the same period. The other serum tumor markers were negative. After four courses of chemotherapy, the 18F-FDG PET/CT scan (the second row of images) was reviewed on June 9, 2018. The results did not show CRPC, and the serum tumor markers were negative. CRPC, colorectal peritoneal carcinomatosis; LS, lesion size; PCI, peritoneal cancer index; PET/CT, positron emission tomography/computed tomography; SUV, standardized uptake value.

A 46-year-old female patient with moderately differentiated adenocarcinoma in the right hemicolon (ileocecal region) underwent an 18F-FDG PET/CT scan (the first row of images: axial plain CT scan and PET fusion image, same layer axial PET image and 3D-MIP PET image, successively from left to right) after surgery, and the results revealed a high-FDG uptake of CRPC (cross, LS-2) on the right side of the uterus in the pelvis (region 6). The same layer plain CT scan failed to be displayed. SUVmax was 4.1. The PCI score of this patient was 2, and the Cyfra21-1 was 2.5 ng/mL in the same period. All other serum tumor markers were negative. No treatment was performed, and the serum tumor index increased after 1 year (Cyfra21-1 was 2.5 ng/mL, CEA was 294.0 ng/mL, and Ca199 was 772.0 U/mL). At this time, the 18F-FDG PET/CT scan was reviewed (the second row of images), and the results revealed that the CRPC lesion on the right side of the uterus was significantly enlarged. The uptake of FDG increased, and the SUVmax was 13.8. A circular calcified uterine myoma appeared on the left side of the uterus after anhydrous ethanol injection. CEA, carcinoembryonic antigen; CRPC, colorectal peritoneal carcinomatosis; LS, lesion size; PCI, peritoneal cancer index; PET/CT, positron emission tomography/computed tomography; SUV, standardized uptake value.
Demographic Characteristics of Patients
CEA, carcinoembryonic antigen; PC, peritoneal carcinomatosis; PCI, peritoneal cancer index; PET/CT, positron emission tomography/computed tomography.
Distribution characteristics of patients
According to the PCI scoring system, there were 598 regions represented among the 46 patients with CRPC (46 subjects × 13 regions/subject), and PC occurred in 203 regions. There were 21 PC distribution modes in the 46 CRPC patients, and region 6 was involved in 60.9% of patients (28/46) (Table 2). The regional proportion of CRPC involvement, from high to low, was as follows: region 6 (13.8%), region 0 (10.3%), region 1 (9.9%), region 5 (8.9%), region 7 (8.4%), region 3 (8.4%), region 2 (7.4%), region 4 (7.4%), region 11 (6.9%), region 8 (6.4%), region 12 (5.4%), region 9 (3.4%), and region 10 (3.4%). The 46 patients had regional involvement as follows: region 6 (60.9%), region 0 (45.7%), region 1 (43.5%), region 5 (39.1%), region 7 (37.0%), region 3 (37.0%), region 2 (32.6%), region 4 (32.6%), region 11 (30.4%), region 8 (28.3%), region 12 (23.9%), region 9 (15.2%), and region 10 (15.2%). The 46 patients with CRC were divided into 3 groups, according to the location of their primary lesions: right hemicolon group, left hemicolon group, and rectum group.
Distribution of Colorectal Peritoneal Carcinomatosis
Prop. (%) = (the total number of PCs in the reg./the total number of all PCs) × 100%.
Dis. Comb. Num., distribution combination number; CRC, colorectal cancer; Num., number; PC, peritoneal carcinomatosis; Prop., proportion; Reg., region.
The right hemicolon group had 13 patients with lesions in 55 regions; the left hemicolon group had 20 patients with lesions in 91 regions; and the rectum group had 13 patients with lesions in 57 regions. The quantity of PC and SUVmax in each group is presented in Table 3 and Figures 3–6. The PCI scores were determined for each patient, and two groups were formed according to the PCI score: a PCI <20 group (33 patients) and a PCI ≥20 group (13 patients). The distribution of CRC patients and the distribution of CRPC were compared between these two groups (Table 4 and Figs. 5 and 6).
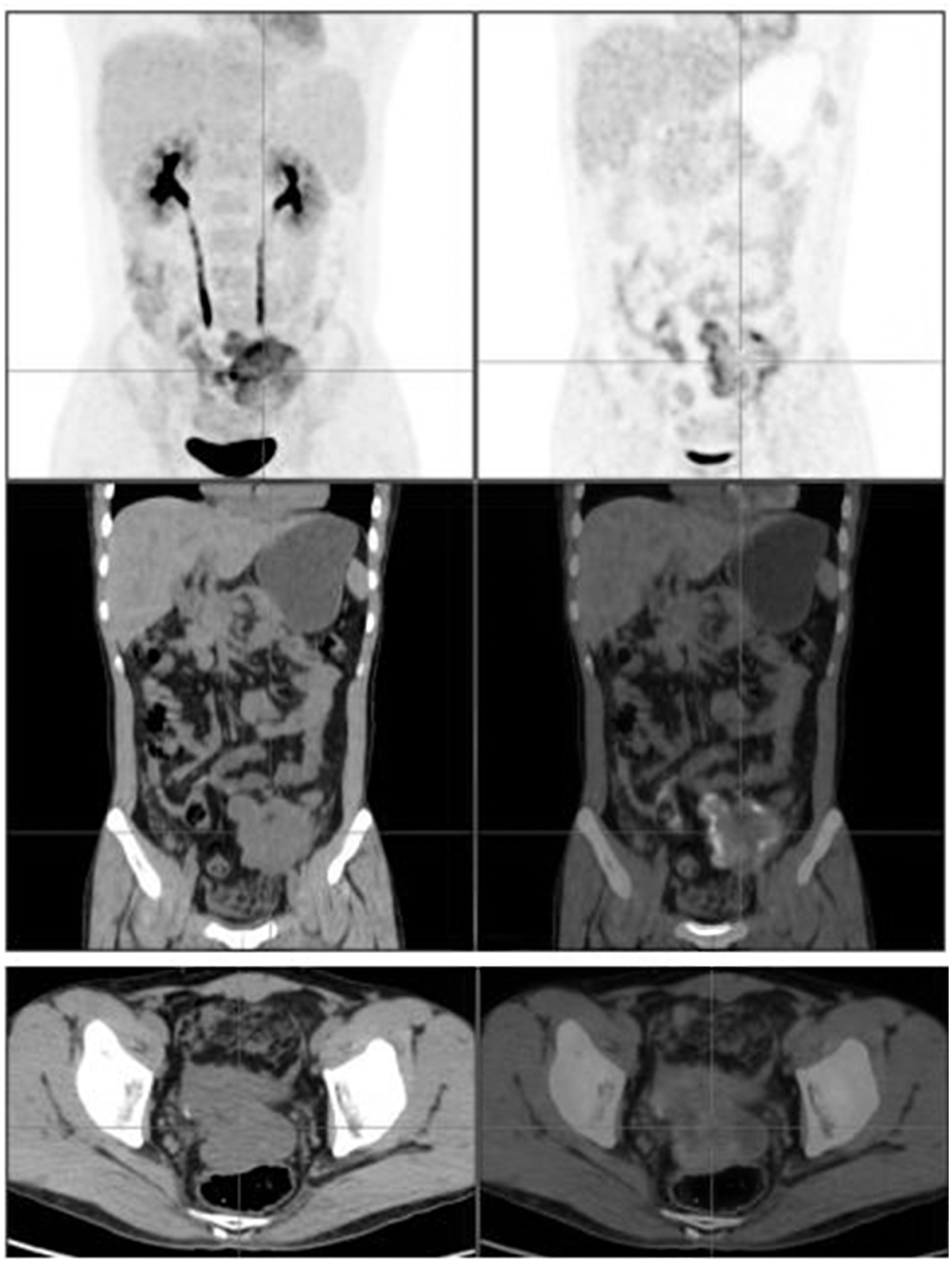
A 37-year-old male patient with a left hemicolon (sigmoid colon) adenocarcinoma concomitant mucinous adenocarcinoma. The CRPC was distributed in the central (region 0, LS-2), right upper (region 1, LS-2), left lower (region 5, LS-2), pelvis (region 6, LS-3), right lower (region 7, LS-2), and upper ileum (region 11, LS-2). The patient's PCI score was 13, the SUVmax of the CRC (3D-MIP PET image, coronal image cross) was 10.1, and the SUVmax of the CRPC (axial position image cross) was 4.3. CEA was 30.3 ng/mL, and the other serum tumor markers were negative. The pelvic effusion is also shown. CEA, carcinoembryonic antigen; CRC, colorectal cancer; CRPC, colorectal peritoneal carcinomatosis; LS, lesion size; PCI, peritoneal cancer index; SUV, standardized uptake value.
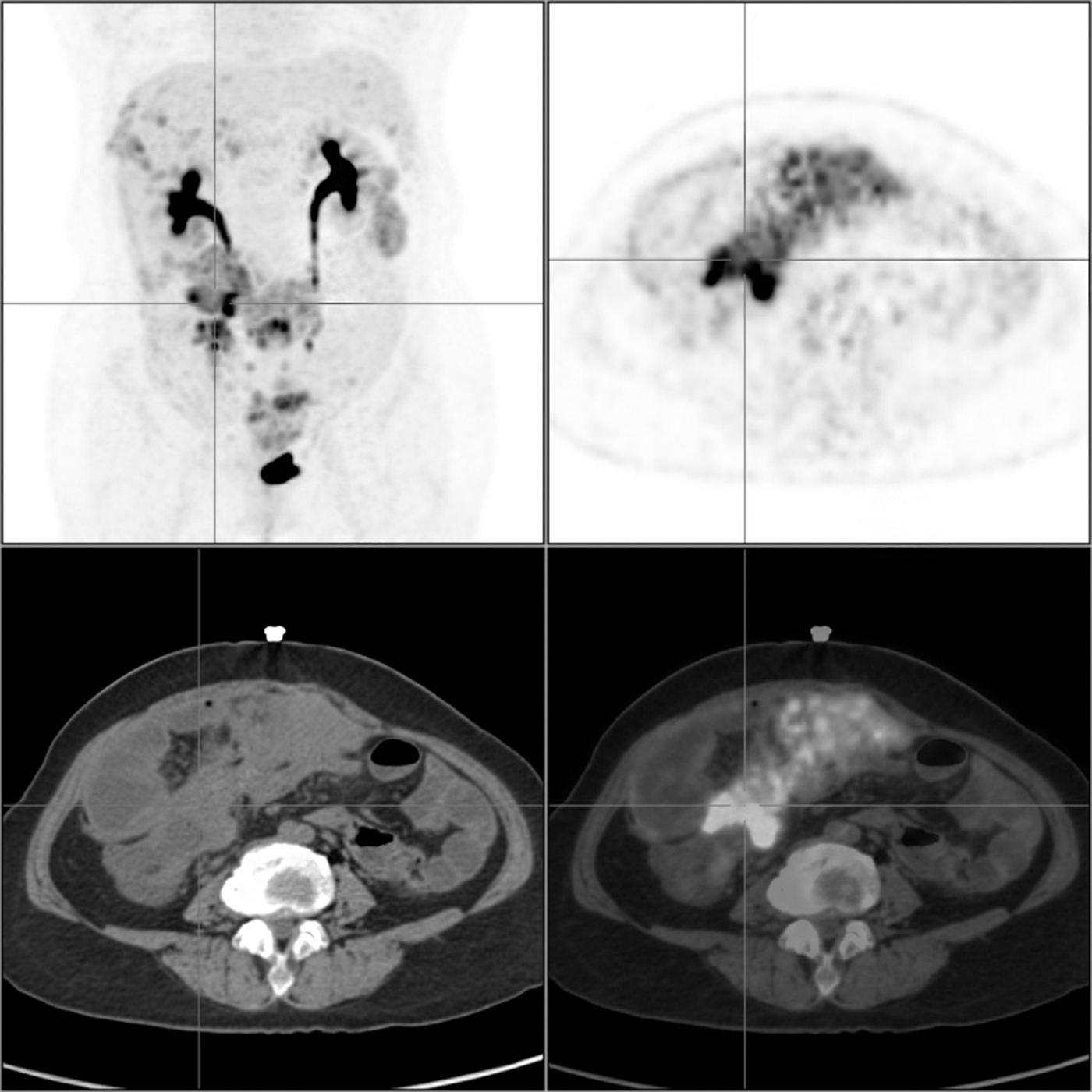
A 54-year-old female patient with poorly differentiated rectal cancer after surgery. The CRPC was distributed in the central (region 0, LS-3), right upper (region 1, LS-2), epigastrium (region 2, LS-2), left upper (region 3, LS-2), left flank (region 4, LS-3), left lower (region 5, LS-2), pelvis (region 6, LS-2), right lower (region 7, LS-2), right flank (region 8, LS-2), upper ileum (region 11, LS-2), and lower ileum (region 12, LS-3). The patient's PCI score was 25, and the SUVmax of the CRPC (axial position image cross) was 19.8. However, the serum tumor indices were not examined in their hospital. CRPC, colorectal peritoneal carcinomatosis; LS, lesion size; PCI, peritoneal cancer index; SUV, standardized uptake value.
Comparison of Size of Peritoneal Carcinomatosis and SUVmax in Three Groups (According to Regional Statistics)
The overall comparison uses single-factor analysis of variance, the test level is a = 0.05, the pairwise comparison between groups uses t or approximate t-test, and the corrected test level is a′ = 0.016 7.
p < 0.05 or # p < 0.016 7, with statistical significance.
SUV, standardized uptake value; PC, peritoneal carcinomatosis.
Distribution of Colorectal Peritoneal Carcinomatosis Patients (According to Patients' Statistics, Peritoneal Cancer Index = 20 Group Comparison)
p < 0.05 and the results are statistically significant.
CRC, colorectal cancer; CRPC, colorectal peritoneal carcinomatosis; PCI, peritoneal cancer index.
CRPC with metastasis
In the present study, 32 patients had lymph node metastasis; 15 patients had liver metastasis; 14 patients had lung metastasis; 15 patients had bone and soft tissue metastasis; 4 patients had adrenal metastasis; 2 patients had pleura metastasis; 1 patient had renal metastasis; and 2 patients had ovarian metastasis. Abdominal and pelvic effusion occurred in 10 patients (21.7%, 10/46). Among these patients, the ascites of six were punctured and drained to identify the exfoliated tumor cells. The remaining 36 patients (78.3%, 36/46) had no apparent pelvic effusion.
Discussion
The results show that the 46 study patients with CRPC had involvement in 598 abdominal and pelvic regions; of these, PC was found in 203 regions (33.9%, 203/598). The regions that had the highest level of CRPC involvement are ranked above in the Results section, and region 6 had involvement in the highest percentage of patients (60.9% 28/46) in the 21 PC distribution modes. As also described in the Results section, the patients were divided into three groups according to the location of the primary lesion: right hemicolon group, left hemicolon group, and rectum group. The average size of the CRPC was greater in the rectum group than in the left hemicolon group; the SUVmax of the CRPC was greater in the right hemicolon group than in the left hemicolon group, and the differences were statistically significant (p < 0.05).
Since there are no obvious clinical symptoms in the early stages of metastasis in CRPC patients, early diagnosis and treatment are difficult. 13,14 Among the CRC patients who underwent radical surgery, up to 50% of recurrences were in the peritoneum. 15 Furthermore, 20%–25% of recurrent CRPC has no distant metastasis, and this is limited to the peritoneum. 16 In recent years, there have been a large number of studies on peritoneal metastasis and clinical practice. 17 –20 There is a consensus that peritoneal metastasis is a complex process involving multiple stages, factors, and molecular mechanisms.
Intra-abdominal dissemination of CRPC included direct spread, implantation metastasis, operational procedures, or trauma. 21 PC cell metastasis can be caused by the mechanical forces of abdominal pressure, gravity, gastrointestinal peristalsis, respiratory movement, and diaphragm movement. Under the action of these forces, ascites flow through multiple potential cavities into the peritoneum. Since the flow rate is slow, tumor cells can easily be deposited, retained, and planted. The action of gravity causes the ascites to accumulate at the lowest part of the pelvic cavity, while the subphrenic negative-pressure suction allows them to rise to the right subphrenic area and right posterior gap of the liver along the right paracolon sulcus. However, the spread does not occur as frequently in the left subphrenic area because it is blocked by the sickle ligament.
The ascitic fluid that slowly rises along the shallow left paracolon sulcus is eventually blocked by the phrenicocolic ligament. On the right side of the lower abdomen, the ascites flow from the ileocecal area to the pelvic cavity; on the left side of the lower abdomen, the flow is from the mesenteric area of the sigmoid colon to the pelvic cavity. 22 Therefore, the tumor cells are most likely to plant in the following sites: pelvic floor depression (>50%), ileocecal junction, mesentery of the small intestine (>40%), bilateral paracolic sulci (18%), liver and kidney recesses, and the right subphrenic area. The greater omentum is rich in lymphoid tissue and can be easily involved because of ascitic absorption.
Esquivel et al. 11 suggested that CRPC involvement occurs most often in the pelvic cavity (75%), right abdomen (71%), left abdomen (67%), distal ileum (69%), and middle abdomen (65%). In the present study, when CRC occurs in the peritoneum, its pattern is complex and varied, resulting in 21 PC distribution patterns in the 46 CRPC patients. According to the findings, the PC of CRC is primarily involved in the lower abdominal region (region 6, 60.9%), umbilical region (region 0, 45.7%), right hypochondriac region (region 1, 43.5%), left inguinal region (region 5, 39.1%), and right inguinal region (region 7, 37.0%). The results of the present study may be correlated to the flow path of the peritoneal fluid in the abdominal cavity, which allows the CRPC to easily stay and grow in the pelvic cavity and right abdomen.
The choice of a PC therapy strategy is correlated to the degree of PC dissemination. The Sugarbaker PCI has been recognized as the most appropriate intraoperative grading system, and it is used as the standard for the selection of treatment options as well as to avoid unnecessary surgery. The load of abdominal and pelvic CRPC is important for predicting the effectiveness of CRS in combination with HIPEC. The results of a multicenter study revealed that the 5-year survival rate of patients with a PCI <20 was 27%–50%, which is higher than the 10% of patients with a PCI ≥20 who received a complete resection; a PCI ≥20 is considered to be a contraindication to CRS. 23 –26 Therefore, this study analyzes the patients according to whether they had scores above or below a PCI of 20.
A comprehensive assessment should be carried out before CRPC surgery that includes distribution and size of lesions, and their relationship with the surrounding tissues and organs. In clinical practice, a comprehensive assessment of PCI brings the greatest benefit to CRC patients. The PET-PCI scores can provide a basis for the diagnosis and clinical treatment strategies in patients with CRC.
The PCI score is the basis for deciding whether CRS treatment is suitable for a patient. From this scoring, the authors have learned that a higher PCI score means a higher CRPC distribution involving more regions. In the present study, there were 13 CRC patients in the PCI ≥20 group who had total CRPC involvement in 154 regions. By comparison, the 33 CRC patients in the PCI <20 group had a total CRPC involvement in only 49 regions.
Involvement of the left subphrenic area (left hypochondrial region) in CRPC has been regarded as late-stage PC with a poor prognosis. Peritoneal fluid is slow to reach this area, compared with the more accessible pelvic floor depression, right inferior abdominal region, left inferior abdominal area, and right paracolon sulcus.
Some scholars have also emphasized that the occurrence of CRPC in the left upper region predicts a low survival rate. 10 Seventeen patients (37%) had involvement in the left superior abdominal region (left upper, region 3) in the present study. Seventeen patients involved in the left upper were analyzed; 76.5% (13/17) of the patients were basically involved in the rest of the area. The remaining regions of these patients were basically affected, with PCI ≥20.
There are limitations in the present study. First, this study is a single-center clinical study with a small sample size and would benefit by being repeated as a multicenter study with a larger sample size. Second, the CRPC in the present study failed to obtain a pathological diagnosis due to the short duration of CRS treatment for CRPC in a large-scale medical institution with a referral destination. Finally, due to the limitation in the CRPC imaging ability, lesions with small CRPC, especially those smaller than 2 mm, could only be identified by visual inspection during the operation. Hence, the imaging PCI score may be smaller than the intraoperative PCI score. 6,7 However, it was speculated in the present study that the CRPC size does not determine its distribution due to the flow path of the ascitic fluid. The authors will continue to collect more data about CRPC patients at a later stage to conduct in-depth studies on additional questions: Does the distribution of CRPC determine survival? Is CRPC not easily detectable in the early stages? Are common pelvic wall invasion and lymph node metastasis in rectal cancer patients related to CRPC?
Conclusions
Due to the influence of many factors, the CRPC formed by the spread of CRC tumor cells is primarily distributed in the pelvic cavity and right abdomen. With greater CRPC involvement, the distribution range becomes wider. In determining treatment options, PET-PCI scores provide a basis for clinical follow-up treatment and prognosis. Clinicians can screen patients to see if they are suitable candidates for CRS, a surgical method for peritoneal metastasis that, when combined with HIPEC, has been shown to increase the overall survival rate of patients. The use of 18F-FDG PET/CT in examinations can go beyond evaluating the condition in the abdominal and pelvic cavities to also synchronously evaluating the distant metastases outside the abdominal and pelvic cavities; therefore the clinical use of 18F-FDG PET/CT and its clinical application value is greater than the use of CT or magnetic resonance imaging.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding or sponsorship was received for this study or publication of this article: The National Key Research and Development Program of China (No. 2017YFC0114300), The National Natural Science Foundation of China (81771885), Nantong Science and Technology Plan Project (MS12018084), Nantong Youth Medical Talent Research Fund Project (WQ2016087).