
Abstract
Objective:
To explore more refined classification methods of congenital middle ear cholesteatoma (CMEC) based on two existing staging systems.
Subjects and Methods:
This study involved a retrospective data review of 57 patients (61 ears involved) with CMEC requiring the surgical treatment. Patients were classified into different stages according to Nelson, Potsic, and Modified Nelson staging system. Preoperative data and intraoperative findings were recorded.
Results:
The mean age at operation was 15 ± 15.04 years with a median of 10 years. The main clinical manifestation was hearing loss (72.13%). CMEC mass was mainly located in the posterior portion of the tympanic cavity (65.57%). No patient was classified into Potsic stage II. The erosion of incus happened in all cases. Patients with Nelson type 2 and type 3 had erosions to the structures out of middle ear, such as dura mater, lateral semicircle canal, and facial canal. Postoperative follow-up time was more than 24 months. Recurrence occurred in four patients (6.56%), all of them in Nelson type 2, who had received canal wall down mastoidectomy (three cases) and canal wall up mastoidectomy (one case).
Conclusions:
Nelson staging system was more suitable for advanced CMEC patients than Potsic staging system. The rare case of Potsic stage II restricted the application of Potsic staging system. Moreover, since both of two staging systems do not distinguish the type of involved ossicles, the authors recommended to subdivide Nelson type 2 into type 2a and type 2b based on the erosion of the ossicular chain, as well as subdivide Nelson type 3 into type 3a and 3b based on the erosion of structures out of middle ear, which was named as Modified Nelson staging system.
Introduction
In 1683, Du Verney et al. 1 first discovered cholesteatoma-like substances between the brain and cerebellum, and they supposed that these substances were congenital. Such cholesteatoma-like substances were also discovered by other researchers. In 1838, Muller 2 named these cholesteatoma-like substances as congenital cholesteatoma (CC). In 1885, Politzer 3 found that cholesteatoma was located in the tympanic membrane (TM) of the middle ear cavity, which may be the first description of congenital middle ear cholesteatoma (CMEC).
CMEC was first clearly reported by Derlacki and Clemis, 4 and the diagnostic criteria were modified by Levenson et al., 5 defining CMEC as white pearly mass located behind the intact TM in the absence of prior surgical procedures or perforation, while the history of acute otitis media was not excluded. The anterosuperior quadrant of the middle-ear cleft is known to be the most frequently involved sites in over 80% of CMEC. 6 However, some researchers have reported CMEC presenting in the posterosuperior quadrant. 7
The theories concerning the origin of CMEC mainly include the middle ear mucosa metaplasia theory, the ectoderm transitional theory, the amniotic fluid inhalation theory, and the epidermis samples tissue theory. 8 It has been reported that the incidence of CMEC is 0.12%. 9,10 In the past 10 years, the incidence of CMEC has significantly increased, accounting for 2%–5% of all cholesteatomas. 11 Therefore, effective strategies are needed for the diagnosis and treatment of CMEC.
Accurately classifying CMEC can help diagnose and improve the prognosis. In 2002, two staging systems of CMEC were proposed by Nelson et al. and Potsic et al., respectively. 12,13 Potsic staging system is based on the quadrants involved and is often used to evaluate the degree of hearing loss, choose the surgical procedures, and predict the recurrence rate of CMEC. 14 However, some researchers found that Potsic stage I CMEC may have a greater tendency to progress to Potsic stage III CMEC by skipping Potsic stage II, 15 therefore lowering the value of Potsic stage II. If Potsic stage II was excluded, the remaining three stages would be the same as the Nelson staging system. This current study aimed to provide suggestions of a new classification for CMEC.
Subjects and Methods
Inclusion and exclusion criteria
This study involved a retrospective data review of 57 patients with CMEC (exclusive external auditory canal cholesteatoma), who were operated by the same experienced doctor from May 2011 to August 2016 in Beijing Friendship Hospital. These patients (four bilateral cases) were diagnosed as CMEC, according to the criteria of Levenson et al. 5 : a white mass medial to a normal TM; normal pars tensa and flaccida; no prior history of otorrhea or perforation TM; and prior history of otitis media is not a cause for exclusion. Meanwhile, the patients who underwent tympanostomy tube placement were included in the study if they were diagnosed with CMEC during operation. Patients with a history of surgery involving the middle ear were excluded from the study.
Classification of CMEC patients
Two staging systems, including Nelson staging system and Potsic staging system, were used to classify the 57 CMEC patients. Nelson staging system 12 and Potsic staging system 13 are described in Figure 1. The reported recurrence rate was 0%, 34%, and 56% of type 1, type 2, and type 3 using Nelson staging system, while it was 14%, 33%, 41%, and 67% of stage I, stage II, stage III, and stage IV using Potsic staging system.
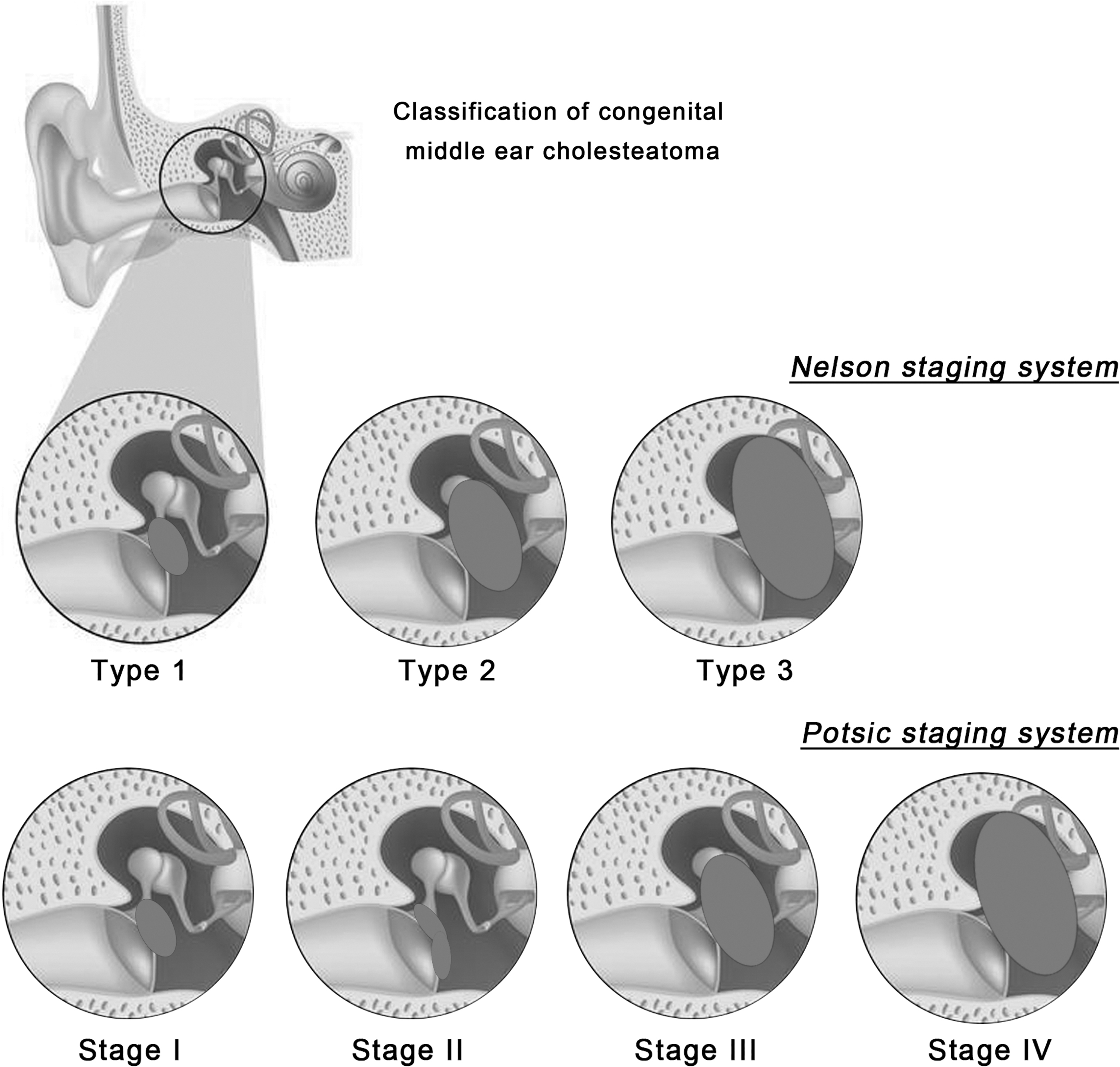
Classification of CMEC using Nelson staging system and Potsic staging system. CMEC, congenital middle ear cholesteatoma.
In contrast, Nelson type 2 patients were subdivided into type 2a (erosion of incus alone, incus with malleus, or incus with superstructure of stapes) and type 2b (erosion of the whole ossicular chain), and Nelson type 3 patients were subdivided into type 3a (without eroding structures out of middle ear) and type 3b (eroding structures out of middle ear), which were named as Modified Nelson staging system (Table 1).
Details of Nelson, Potsic, and Modified Nelson Staging System
Diagnosis of CMEC
All patients underwent temporal bone high resolution computed tomography (CT) to confirm the presence of the mass before surgery, and the final diagnosis was confirmed by postoperative pathology examination. All patients were followed up for at least 24 months after surgery.
Pure-tone hearing threshold examination
Pure-tone thresholds were measured in ill ears at frequencies of 0.5, 1, 2, and 4 kHz. Both air-conduction thresholds and bone-conduction thresholds were examined. The threshold at each frequency was calculated as an average of the ill ear thresholds.
Hematoxylin–eosin staining
The mass tissue sections were fixed in 10% formalin, embedded in paraffin, and cut into 4-μm thick slides. Then the specimens were dewaxed thrice with xylene for 5–10 min. After the alcohol dehydration, the specimens were stained with hematoxylin solution for about 4 min and treated with 1% hydrochloric acid alcohol and 0.5% ammonia water until the nucleus turned blue and then stained with eosin for 1 min. After being rinsed by alcohol, the specimens were again treated with xylene thrice. The specimens were observed under a microscope and photographed.
Data collection
During the data collection, two experienced doctors, including one senior doctor, worked together and helped check the validity of the collected data. Preoperative characteristics included the age at operation, gender, lateral, presenting symptoms at the time of initial diagnosis, and otoscopic findings. Intraoperative findings included the distribution of mass, ossicular chain status, surgery approaches, and recurrence rate.
Results
The clinical characteristics of CMEC
A total of 57 patients (61 ears) who were diagnosed with CMEC and underwent surgical treatment by the same experienced surgeon between May 2011 and August 2016 were evaluated. The mean age at operation was 15 ± 15.04 years (range from 2 to 60 years with a median of 10 years). In line with published literature, there was a higher prevalence in males (70.18%) than in females, whose ratio was nearly 3 to 1. According to their data, the incidence of CMEC was 15.28% among patients of cholesteatoma from May 2011 to August 2016. Only 4 of 61 ears (6.56%) were found incidentally without symptoms, which all happened to children. In symptomatic ears, hearing loss (46 ears, 75.41%) was the most common complaint, followed by the prolonged middle ear effusion (13 ears, 21.31%) and tinnitus (10 ears, 16.39%) (Table 2). Otoscopic findings showed that 39 ears (63.93%) had a normal TM, 15 ears (24.59%) had an intramembranous whitish mass, which were mainly located in the posterior quadrant of the tympanum or multiple quadrants of the tympanum, and 7 ears (11.48%) had the retraction of TM. None of the 61 ears had the TM perforation. CMEC patients were classified using Nelson staging system, Potsic staging system, and Modified Nelson staging system (Table 3). Interestingly, no patient was found in Potsic stage II. The typical CT images of Nelson type 2/Potsic stage III are shown in Figure 2A (right ear) and Figure 2B (left ear). The hearing loss status before surgery is shown in Table 4, which was measured using pure-tone hearing threshold examination.
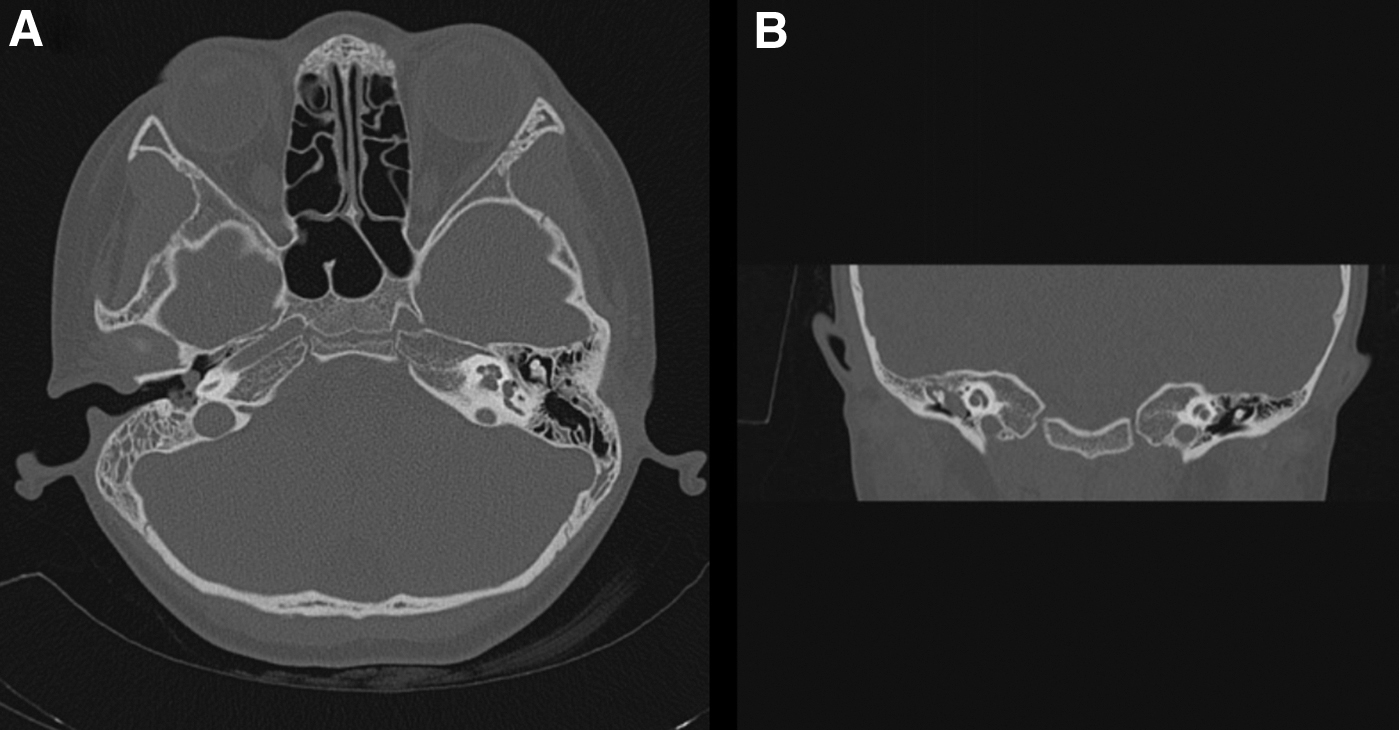
Typical CT images of Nelson type 2 CMEC.
Demographic Features and Clinical Symptoms of CMEC Patients (57 Patients with 61 Involved Ears)
CMEC, congenital middle ear cholesteatoma.
The Distribution of CMEC Patients According to Nelson, Potsic, and Modified Nelson Staging Systems
Pure-Tone Hearing Threshold Results of CMEC Patients with Nelson Type 2 and Type 3 Before Surgery
The erosion of structures in middle ear and out of middle ear
According to Nelson staging system, the location of CMEC was analyzed. The result indicated that CMEC was localized to the posterior portion of the tympanic cavity in Nelson type 1 (3 ears). In Nelson type 2 (44 ears) and type 3 (14 ears), the posterior portion of the tympanic cavity was also the major location of CMEC (65.91% and 57.14%, respectively) (Fig. 3). In total, there were 40 ears localized to the posterior portion of the tympanic cavity among 61 ears (65.57%).

The mass distribution at the different portions of the tympanic cavity according to Nelson staging system.
The erosion of ossicles was commonly seen in CMEC, especially for the erosion of incus. In this study, the erosion of incus was found in all the patients in Nelson type 2 and type 3 (Table 5). Meanwhile, the erosion of whole ossicular chain (malleus + incus + stapes) was more commonly seen in Nelson type 3 patients than in type 2 patients (28.57% vs. 11.36%).
Erosion of Ossicular Chain in CMEC Patients with Nelson Type 2 and Type 3
I, incus; M, malleus; SS, the superstructure of stapes.
For the erosion of structures out of middle ear, the authors found that the Nelson type 3 CMEC was more intended to erode to lateral semicircle canal (42.86% vs. 0%), external auditory canal (21.43% vs. 0%), attic (50.00% vs. 2.27%), dura mater (35.71% vs. 2.27%), and facial canal (21.43% vs. 6.82%) than Nelson type 2 CMEC (Table 6).
Erosion of Structures Out of Middle Ear in CMEC Patients with Nelson Type 2 and Type 3
EAC, external auditory canal; LSCC, lateral semicircle canal.
Operative approaches and the recurrence rate
All patients were performed with the one-stage surgery. The postoperative pathologic images showed squamous epithelium and keratin (Fig. 4A) and the keratin migration into interstitial cells with giant cell response (Fig. 4B), suggesting the typical characteristics of CMEC. Interestingly, there were 4 cases that were found to be CMEC during the cochlear implant (CI), including two cases in Nelson type 1 and 2 cases in Nelson type 2 (Table 7). At the end of the study, 4 ears in Nelson type 2 recurred, making the recurrence rate of 9.09% in the total 61 ears. Among the four recurrent ears, three cases had been treated with the canal wall down mastoidectomy (CWDM) and one case had been treated with the canal wall up mastoidectomy (CWUM).
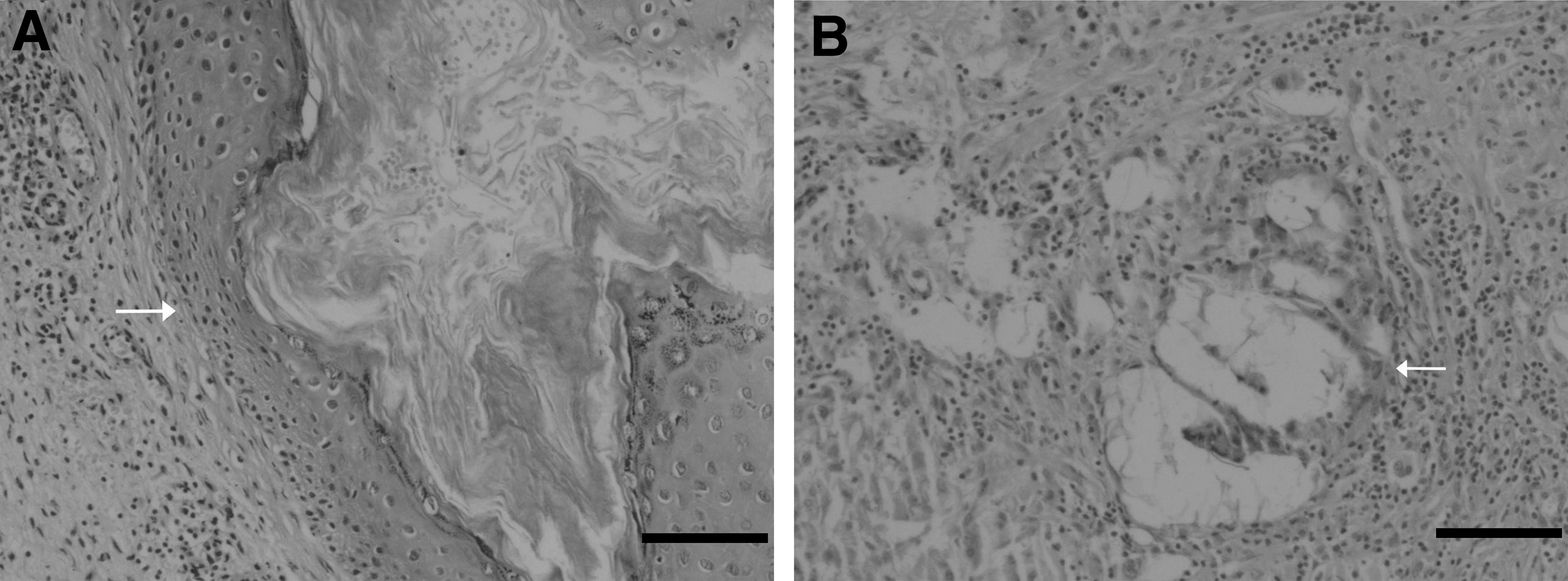
Typical HE staining images (10 × 10) postoperation. Scale bar = 10 μm.
Operative Approaches and the Recurrence Rate of CMEC Patients at Different Nelson Types
CI, cochlear implant; CWDM, canal wall down mastoidectomy; CWUM, canal wall up mastoidectomy.
Discussion
Although CMEC is a rare disease, the incidence has been significantly increased in the past 10 years. Some researchers thought that the higher incidence of CMEC was related to the improvement of diagnostic equipment and patient awareness, while the timely and effective diagnosis and treatment reduced the number of patients with TM perforation and acquired cholesteatoma. 16 CMEC is commonly seen in children, especially in those around 5 years old. 12 However, adult patients are more aware of symptoms caused by CMEC, so the mean age of the included patients was relatively higher in this study (15.2 years, ranging from 2 to 60 years). The authors supposed that although CMEC was congenital, its symptoms may be shown in adulthood, although the controversy exists. The growth of CMEC in children is more aggressive than that in adults, and the growth of CMEC is slow. When the middle ear is stimulated by chronic inflammation and with the dysfunction of the eustachian tube, the growth of cholesteatoma in children will be more invasive than adults. 17 In their data, the incidence of CMEC was 16.35% among 373 patients with cholesteatoma (both congenital and acquired) from May 2011 to August 2016, which was consistent with the other studies. 18
Potsic staging systems are more popularly used to classify CMEC patients to evaluate the severity of the disease. However, no Potsic stage II patient was found in their data, which may be due to the advanced stages of the included patients. In other author's studies, there were just fewer patients found in Potsic stage II, so they predicted that Potsic stage I patients may have a greater tendency to progress to Potsic stage III by skipping Potsic stage II. 15 Therefore, the authors considered that Nelson staging system was more suitable for advanced CMEC patients than Potsic stage system. In their data, the most common symptom of CMEC was hearing loss (72.13%), which was mostly caused by erosion of the ossicular chain.
All the patients with Nelson type 2 and type 3 had incus erosions, and 55.1% had erosions of the superstructure of stapes, which was consistent with the previous reports. 19 –21 As reported, the integral and functional ossicular chain plays critical roles in hearing and postoperative reconstruction of hearing. Previous studies have indicated that the injury of stapes is closely related to the hearing loss and the recurrence rate. 17,22 However, both of the two staging systems (Potsic and Nelson staging systems) do not distinguish the type of involved ossicles, which might be the shortcomings of the two staging systems. 17
By observing the injury of the ossicles in different stages and considering the importance of the stapes in hearing protection, the authors subdivided Nelson type 2 into type 2a (erosion of incus alone or incus with malleus) and type 2b (erosion of the whole ossicular chain or incus with superstructure of stapes). The authors believed that this subdivision may have good predictive value for the recovery of postoperative hearing and residual in CMEC patients, and these data were under investigations in their future studies. Meanwhile, the authors found that for some Nelson type three patients had erosions of structures out of middle ear, such as lateral semicircle canal, the wall of external auditory canal, attic, dura mater, facial canal, and eustachian tube. Therefore, the authors subdivided Nelson type 3 into type 3a (without eroding structures out of middle ear) and type 3b (eroding structures out of middle ear), which may help assess the prognosis of CMEC patients and deserve further investigations.
In recent years, with people's understanding of middle ear cholesteatoma and the continuous improvement of their diagnosis and treatment requirements, CMEC staging classification standards have emerged. In 2020, Sun et al. 23 reported novel surgery classification approaches to middle ear cholesteatoma, aiming to standardize the use of microscopy and endoscopy. In 2015, the European Ophthalmology and Neuro-Otology Society jointly revised the global consensus document on the definition, classification, and staging of middle ear cholesteatoma, 24 which involved the staging of CMEC. Yang et al. 25 used JOS system to observe the clinical characteristics of cholesteatoma in children. Although the JOS staging method involves intracranial and extracranial complications, it does not discuss in depth the possible impact of the destruction of specific anatomy in the middle ear on disease treatment and prognosis. Therefore, the authors recommend subdividing Nelson type 2 and type 3, which may be helpful to reflect the lesion development with progress, especially in the ossicular chain and complications (intracranial and extracranial).
In the current study, the mass was mainly located in the posterior portion of the tympanic cavity where incus and stapes are located. Some researchers found that anterior-superior portion of tympanic cavity was the most frequent location of CMEC, while some reports, including ours, show that the posterior-superior portion was also the common location of CMEC. 7 It is easy to determine the origin of an early CMEC, but it becomes more difficult for advanced CMEC. In the current study, all of the Nelson type 1 CMEC, which could be considered as the early CMEC, was located in the posterior region of the tympanic cavity. The authors propose that CMEC may be originated from the posterior region or intended to progress to the posterior region, although more evidence is still needed.
The focus of this study is to discuss the stage classification of CMEC. Since all the cases (61 cases) in this study were completed by the same doctor, it is possible to rule out the uneven postoperative effects caused by the operation of multiple surgeons. The treatment goals of CMEC are removing diseased regions, creating a safe and dry ear, preventing recurrence, and preserving or restoring hearing, which can only be achieved through surgery. 21 Exploring tympanoplasty, tympanoplasty with atticotomy, CWUM with tympanoplasty, and CWDM with tympanoplasty are commonly used surgical approaches. 26,27 As no single method is superior in all cases, the authors used personalized strategies according to the condition of patients, and all the patients underwent one-stage surgery, which was considered better than two-stage surgery. 21
In this study, the selection of surgical approaches depended on disease status and classification. CWDM tympanoplasty and CWUM tympanoplasty were mainly used in Nelson type 2 and type 3 patients. The choice of CWDM or CWUM was made according to many factors, including the location of the mass, the scope of the erosion, the degree of mastoid gasification, the age of the patient, and compliance. 28 However, the high recurrence of CWUM and CWDM was reported. For example, a recurrence of 42% for CWUM was reported by Dodson et al. 29 ; a recurrence of 13% for CWDM was reported by Marco-Algarra. 30 In their present data, the total recurrence was four cases (6.56%), which occurred in Nelson type 2 patients performing CWUM (one case) and CWDM (three cases). The recurrent CMEC is mostly located in the anterior tympanic fossa and around the entrance of the eustachian tube. The relative low recurrence in this study may be related to the same experienced surgeon who performed all the surgeries as previous studies showed that experienced surgeon is important for the prognosis of CMEC patients. 31
There are some limitations in this study. Due to the low incidence of CMEC, the number of sample cases in this study is low, affecting the statistical analysis of the data. Meanwhile, the data of postoperative pure-tone hearing threshold are also important to evaluate the surgical outcome on hearing improvements. In their future studies, the authors will continue to collect CMEC cases and improve the validity of the collected data.
Conclusion
Nelson staging system is suitable for classifying CMEC patients at advanced stages. The authors recommended subdividing Nelson type 2 and type 3, which may be helpful to assess the lesion development in the ossicular chain and extracranial complications. However, the authors did not confirm the clinical significance of these subdivisions. Next, the authors will expand the number of cases and collect more relevant data for further investigations.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Beijing Friendship Hospital (Approval number 2016L02228). The written informed consent was not obtained due to the retrospective review.
Consent for Publication
For the participation of this research, consent for publication was obtained from each patient or their parent or legal guardian in case of children. The name and identity of all patients were kept confidential.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors' Contributions
Y.Y.Z. put forward the concept of the study, designed the study, prepared the article, and contributed to the statistical analysis. S.S.G. put forward the concept of the study and designed the study. P.L. and J.L. contributed to the data acquisition. J.X. and G.P.W. contributed to the data analysis and the quality control of data. J.Y.G. analyzed the data and interpretation and edited the article. All authors read and approved the final article.
Footnotes
Disclosure Statement
There are no existing financial conflicts.
Funding Information
No funding was received for this article.