
Abstract
Background:
There are paradoxical results regarding whether carbonic anhydrase IX (CAIX) is a prognostic biomarker for patients with clear cell renal cell carcinoma (ccRCC). The objective of this study was to evaluate prognostic significance of CAIX in nonmetastatic ccRCC patients of different stages.
Materials and Methods:
This is a retrospective study on 1263 patients with nonmetastatic ccRCC from January 2005 to June 2018. Patients were stratified into eight subgroups (pT1a, pT1b, pT2a, pT2b, pT3a, pT3b, pT3c, and pT4) according to the 2016 TNM classification system. Immunohistochemical staining of membranous CAIX was quantified. Cancer-specific survival (CSS) rates in patients with high (>85%) and low (<85%) CAIX expressions were compared by Kaplan–Meier curves with log-rank test.
Results:
There were 220 tumors (17.42%) with low CAIX expression and 1043 tumors (82.58%) with high CAIX expression. The cumulative CSS rates were statistically significant between all patients with low and high CAIX expression (p-value <0.001). In pT2a, pT2b, and pT3a subgroups, the patients with low CAIX expression exhibited markedly decreased cumulative CSS rates compared to patients with high CAIX expression (p-value <0.05). Univariable and multivariable Cox regression analysis showed that CAIX expression was an independent predictor of prognosis in patients with pT2a, pT2b, and pT3a ccRCC (p-value <0.05), rather than in all nonmetastatic patients.
Conclusion:
CAIX expression is of independent prognostic value for ccRCC patients in pT2a, pT2b, and pT3a stages. CAIX expression combined with tumor stage would further improve risk stratification of nonmetastatic ccRCC patients and provide directions for therapies.
Introduction
Renal cell carcinoma (RCC) originates from renal epithelium and corresponds to 3% of all cancers and more than 90% of kidney cancers. 1 It has various histological subtypes and the primary subtype is clear cell renal cell carcinoma (ccRCC), which is accounted for up to 85% of all RCC cases. 2 Surgical management is preferred by patients with localized ccRCC. Nonetheless, relapse is eventually observed in approximately a half of patients receiving radical nephrectomy. 3 In addition to conventional prognostic parameters such as tumor node metastasis (TNM) stage and grade, 4 novel histological biomarkers of prognostic value are in demand and could be potentially beneficial for risk stratification, outcome prediction, and tailored therapies.
Carbonic anhydrase IX (CAIX), namely MN protein or G250, is a tumor hypoxia-related enzyme and has been found to be highly overexpressed in a wide range of malignancies, such as breast cancer, 5 head and neck cancer, 6 pancreatic cancer, 7 and lung cancer, 8 while scarcely observed in normal tissues. 9 CAIX functions as a key player in acidifying the tumor microenvironment by controlling extracellular pH, thereby virtually contributing to cancer progression and resulting in therapeutic resistance. 10,11 Immunohistological staining shows that CAIX is overexpressed in more than 90% of ccRCC, but is absent in adjacent normal renal tissue. 9,12 Moreover, there is evidence that supports the diagnostic value of CAIX for RCC. 13
It is controversial whether CAIX expression could provide accurate information concerning ccRCC prognosis. Some studies have pointed out that CAIX expression is a prognostic indicator and low CAIX expression indicates poor prognosis and low response to interleukin therapy in ccRCC patients. 12,14 –17 However, other studies hold an opposite viewpoint that CAIX is not related to ccRCC prognosis. 18,19 In light of these contradictory and inconsistent findings, the authors carefully analyzed these studies and found that the majority of patient data came from single medical center and the enrolled patients are varied in TNM stages. 12,18 Moreover, Takacova et al. provide evidence that CAIX expression is correlated with tumor stage in RCC patients. 20 Therefore, they hypothesized that the prognostic effect of CAIX in RCC might be associated with tumor stages. Therefore, in this study, the authors collected patients from four medical centers and analyzed the prognostic correlations between CAIX expression and nonmetastatic ccRCC in different TNM stages, respectively. This study did not focus on patients with metastatic ccRCC due to their well-recognized poor prognosis and short survival periods. 21 Finally, 1263 patients met the inclusion requirements and were retrospectively analyzed. Purpose of this article is to evaluate whether CAIX expression correlates with postoperative cancer-specific survival (CSS) in nonmetastatic ccRCC of different TNM stages.
Patients and Methods
Patients
From January 2005 to June 2018, a total of 1263 patients who received surgical removal for nonmetastatic pT1–pT4 ccRCC based on 2016 TNM classification criteria 22 were included in this study. Of them, 794 underwent radical nephrectomies and 469 underwent partial nephrectomies. The 1263 patients were treated in four hospitals, including Yantai Yuhuangding Hospital, Yantai Hospital Affilicated to Binzhou Medical Univerity, the First Hospital Affiliated to Sun Yat-sen University, and Dongying People's Hospital. Demographic and clinical characteristics of patients were collected from the hospital databases. Central pathology re-review was carried out by two experienced uropathologists. TNM stages were determined based on the final pathological report according to the 2016 TNM classification system. 23 Final clinical status of the enrolled patients was retrieved from medical records or through telephone communications with patients or their close relatives. Informed consent was obtained from each patient or relatives. This study was approved by the Institutional Ethics Committee of the Affiliated Yantai Yuhuangding Hospital of Qingdao University.
Immunohistochemical analysis
Immunohistochemical staining and quantification of CAIX were conducted in a tissue microarray (TMA) format. 14 The set of kidney tumor TMA, which was composed of four blocks, contained one 0.6 mm diameter tissue core of kidney cancer from each patient. The presence or absence of cancer tissue was verified by visual observation of hematoxylin and eosin-stained TMA slides. Freshly cut TMA sections were stained on 1 d. The slides were incubated overnight with anti-CAIX monoclonal antibody clone M75 (1:1000; Abcam, Cambridge, USA). Immunohistochemical staining of CAIX was performed according to instructions of manufacturer. Only membranous staining pattern suggested positive CAIX staining. The score of CAIX expression in each spot was evaluated by combining staining intensity (0–3 points) and the percentage of stained cancer cells. The overall score of CAIX expression was calculated from the average from three spots of one specimen. Staining percent >85% was defined as high CAIX expression and staining percentage ≤85% was considered low CAIX tumor expression according to the criteria suggested by Bui et al. 12
Statistical analysis
The authors evaluated CAIX expression against clinical variables, including gender, symptoms at presentation, primary tumor stage, TNM stages, nuclear grade, and necrosis using Pearson's chi-square test. CSS was estimated and compared by using Kaplan–Meier curves together with log-rank test. Associations of CAIX expression and clinical features with survival were first evaluated in univariable Cox regression analysis. If p-value <0.05 in univariable Cox regression analysis, the variables were then included in multivariable Cox regression analysis. p-Value <0.05 suggested statistical significance, and all p-values were two sided. All statistical analyses were performed with IBM SPSS 18.0.
Results
Demographic and clinical characteristics of the 1263 participants are shown in Table 1. Of them, 783 (62.00%) were male and 480 (38.00%) were female. The median age was 65.51 (range 22–84) years, with the median tumor size of 6.70 (range 1.50–16.73) cm. The median follow-up was 63.5 months. During follow-up, 179 (14.17%) patients died, of which 129 specifically died of RCC postoperatively.
Comparison of Clinical Features of Patients with High Carbonic Anhydrase IX Expression and Low Carbonic Anhydrase IX Expression
This includes ccRCC that invades beyond Gerota's fascia, excluding lymph nodes and distant metastasis.
CAIX, carbonic anhydrase IX; TNM, tumor node metastasis.
According to the criteria for CAIX staining in immunohistochemical analysis, a total 220 tumors (17.42%) were evaluated as low CAIX expression and 1043 tumors (82.58%) were defined as high CAIX expression (Fig. 1). When analyzing the association of CAIX expression with clinicopathological features, the authors found that CAIX expression was significantly associated with TNM stages (p-value = 0.044), primary tumor stage (p-value = 0.030), nuclear grade (p-value <0.001), and tumor necrosis (p-value = 0.006). Compared to high CAIX expression, low CAIX expression was more likely to be observed in tumors at advanced stage, at higher TNM stages, at nuclear grade, and with necrosis. For instance, tumor necrosis was found in 19.09% of tumors with low CAIX expression and 12.18% of tumors with high CAIX expression, with significant differences between the two percentages (p-value = 0.006).
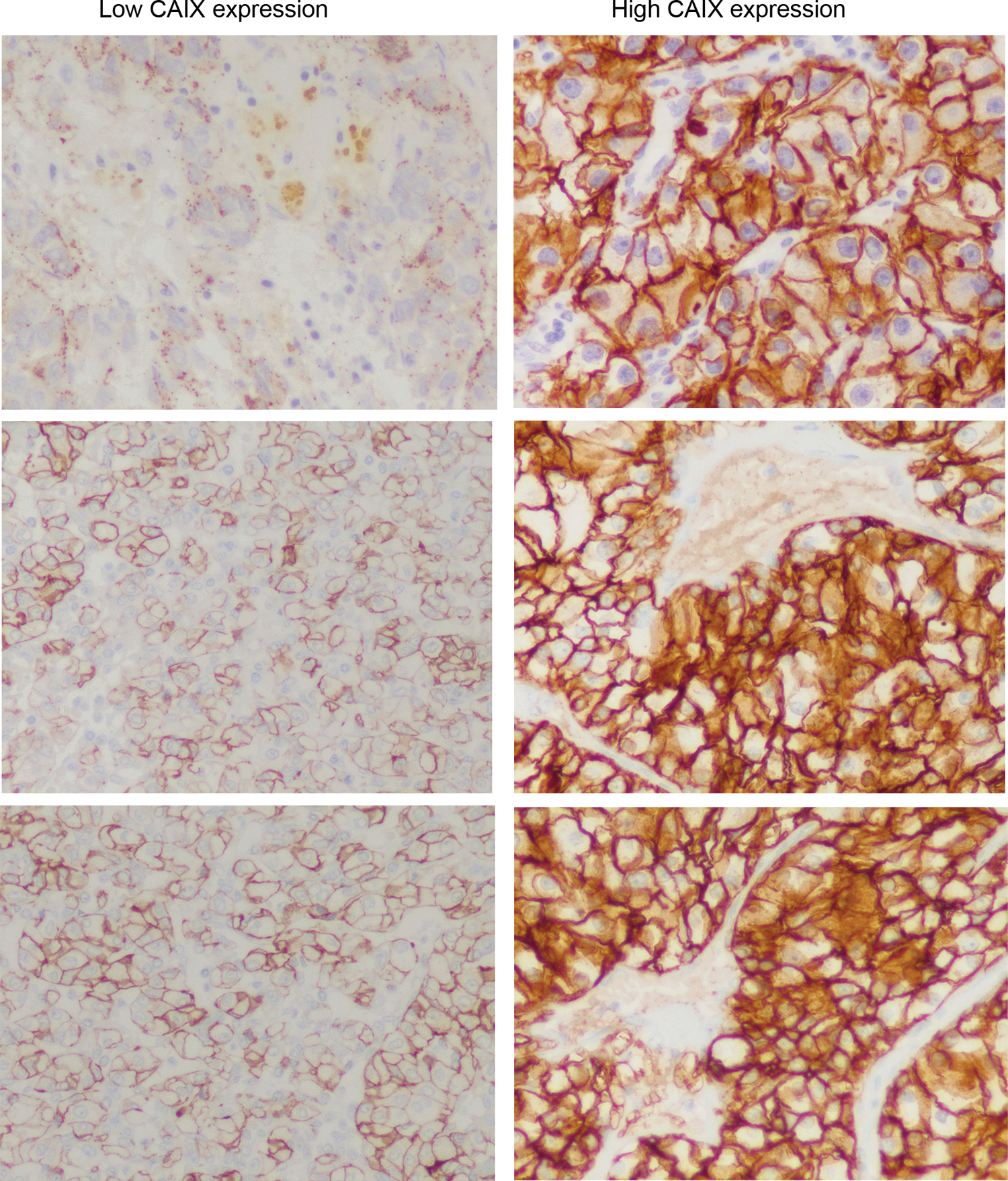
Representative images of immunohistochemical staining of low (left panel) and high (right panel) CAIX expression ( × 400 magnification). Low and high expression suggest ≤85% positive staining and >85% positive staining, respectively. CAIX, carbonic anhydrase IX.
As shown in Figure 2, the cumulative CSS rates were statistically significant between different tumor stages (pT1–pT4 stages, χ 2 = 444.82, p-value <0.001). Moreover, difference in the cumulative CSS rates achieved statistical significance between all patients with low and high CAIX expression (N = 220 and N = 1043, χ 2 = 24.695, p-value <0.001; Fig. 3). For the patients with low CAIX expression, the cumulative CSS rates at postoperative 1, 3, 5, 8, and 10 years were 95.22%, 87.35%, 76.06%, 66.34%, and 50.46%, respectively. For the patients with tumors containing high CAIX expression, the cumulative CSS rates at postoperative 1, 3, 5, 8, and 10 years were 98.39%, 94.48%, 87.61%, 80.99%, and 76.18%, respectively.

Kaplan–Meier curves for CSS according to eight-stage subgroups in nonmetastatic ccRCC patients. CSS, cancer-specific survival; ccRCC, clear cell renal cell carcinoma.
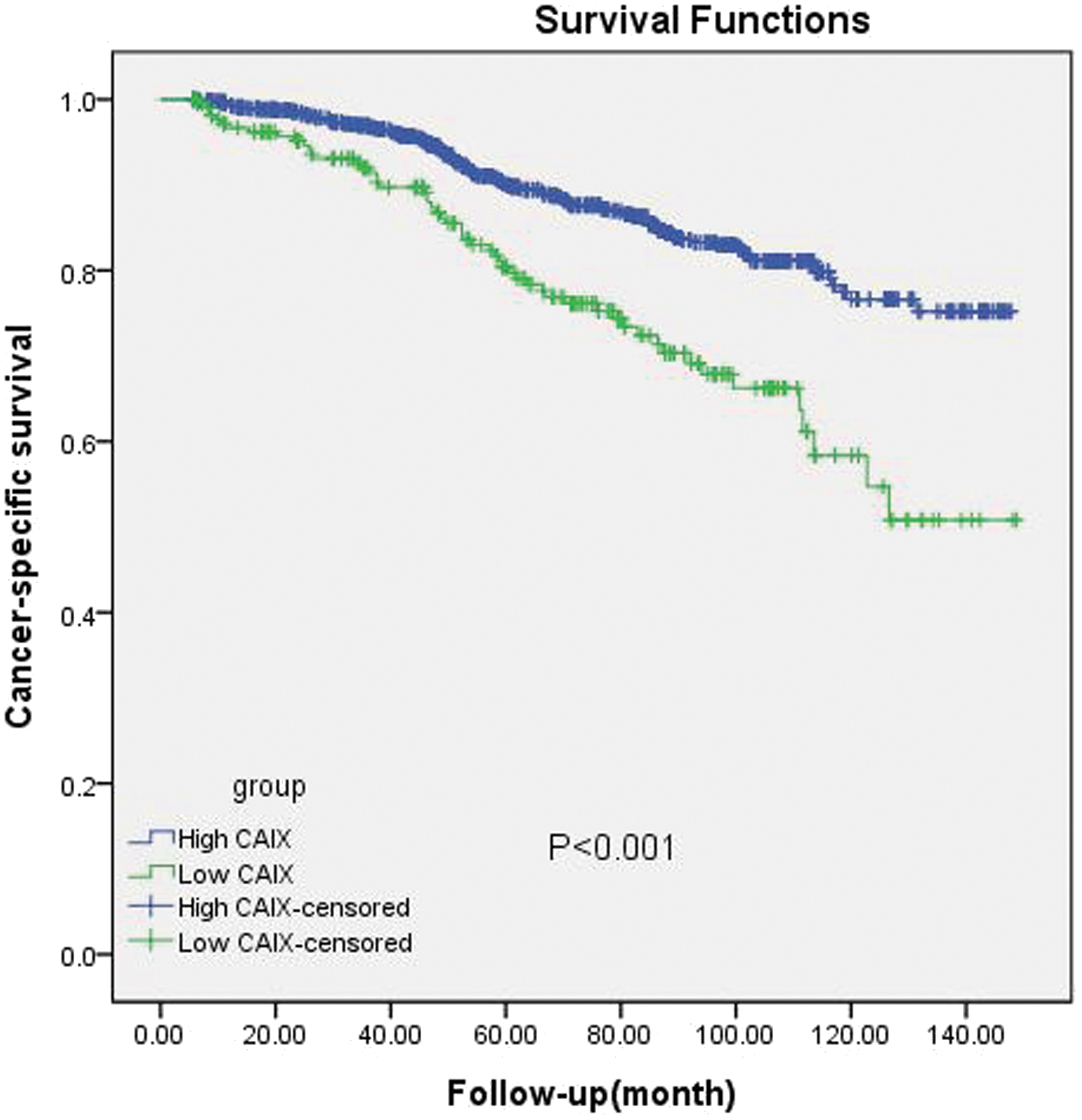
Kaplan–Meier curves for CSS in nonmetastatic ccRCC patients stratified by CAIX expression.
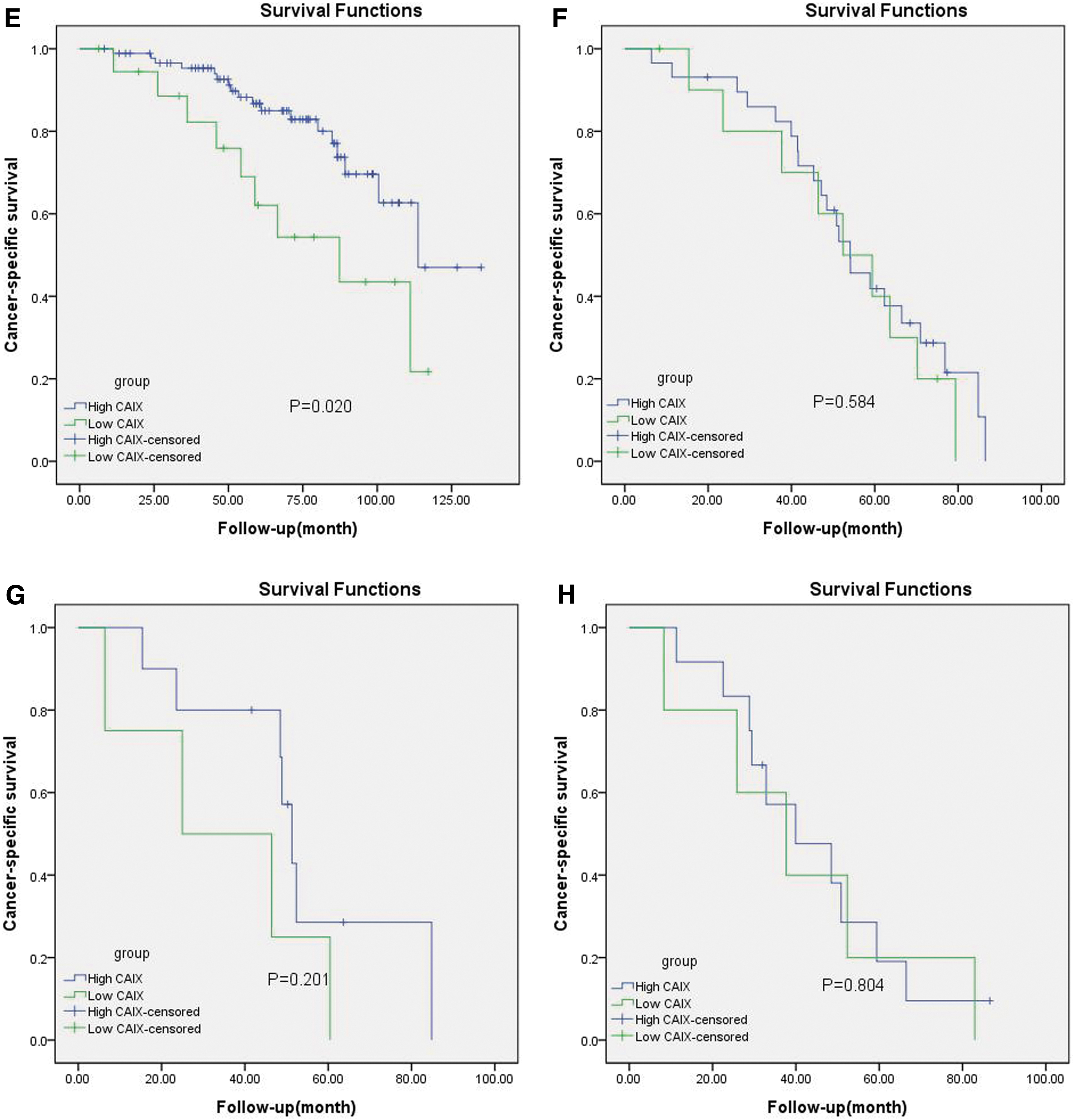
All patients were stratified into eight subgroups (pT1a, pT1b, pT2a, pT2b, pT3a, pT3b, pT3c, and pT4) according to TNM stage. In each subgroup, the cumulative CSS rates were compared between the patients with low and high CAIX expression (Fig. 4A–H). Kaplan–Meier curves showed that the cumulative CSS rates were significantly different between the patients with low and high CAIX expression in pT2a (79.65% vs. 91.27%, p-value = 0.046; Fig. 4C), pT2b (78.65% vs. 89.24%, p-value = 0.024; Fig. 4D), and pT3a (54.30% vs. 80.51%, p-value = 0.020; Fig. 4E) subgroups. However, differences in the cumulative CSS rates were not significant in pT1a (p-value = 0.668; Fig. 4A), pT1b (p-value = 0.209; Fig. 4B), pT3b (p-value = 0.584; Fig. 4F), pT3c (p-value = 0.201; Fig. 4G), and pT4 (p-value = 0.804; Fig. 4H) subgroups.

Kaplan–Meier curves for CSS according to CAIX expression in pT1a
There were a total of 391 patients in pT2a, pT2b, and pT3a stage. Consequently, the authors performed univariable and multivariable Cox regression analysis in the 391 patients to identify prognostic factors from clinicopathological variables and CAIX expression. Univariately, CAIX expression (p-value = 0.015), age at surgery (p-value <0.001), nuclear grade (p-value <0.001), TNM stage (p-value <0.001), and necrosis (p-value = 0.031) were all found to be significantly associated with CSS in pT2a, pT2b, and pT3a subgroups (Table 2). Furthermore, CAIX expression (p-value = 0.028), nuclear grade (p-value <0.001), TNM stage (p-value <0.001), and necrosis (p-value = 0.046) were identified to be independent prognostic factors in the patients with pT2a, pT2b, and pT3a ccRCC by multivariable Cox regression analysis (Table 2). According to results of univariable and multivariable Cox analysis, CAIX expression is of independent prognostic value for ccRCC patients in pT2a, pT2b, and pT3a stages. CAIX expression would further improve risk stratification of nonmetastatic ccRCC patients.
Univariable and Multivariable Cox Regression Model Analysis of Cancer-Specific Survival in Patients with pT2a, pT2b, and pT3a Clear Cell Renal Cell Carcinoma
CI, confidence interval.
Discussion
CAIX has emerged as a promising antitumor target due to its tumor-specific expression and active role in promoting survival and metastasis of tumor cells. 24 It has been demonstrated that CAIX is highly and homogeneously expressed in ccRCC rather than papillary and chromophobe RCC. 14 Because of dramatic expression differences, immunohistochemical detection of CAIX expression in RCC has been widely used in research and could facilitate certain difficult morphological classification of RCC. 12,14,25 In this study, the authors analyzed CAIX staining in tumors of 1263 patients with nonmetastatic ccRCC and found high CAIX expression in 1043 tumors (82.58%). Moreover, results of chi-square test exhibited that CAIX expression was significantly related to several clinical features, including primary tumor stage, TNM stage, nuclear grade, and tumor necrosis. The patients with advanced tumors with necrosis are more likely to have low CAIX expression compared to the patients with early-stage tumors without necrosis. These results implied that low CAIX expression is related to increased malignant degree and advanced TNM stage of nonmetastatic ccRCC. These findings are in agreement with a study by Takacova et al., which demonstrated that the positive expression of CAIX in RCC tumors at higher stage was decreased. 20 Moreover, a recent study reached a consistent conclusion that high CAIX expression is associated with low Fuhrman grade, low tumor stage, and absence of distant metastases within RCC patients. 14
It is established that survival of patients with tumors of different stages is different. 26 So far an agreement has not been achieved regarding the prognostic value of CAIX expression in ccRCC. 12,14 –19 This study found that patients with low CAIX expression had significantly shorter survival in comparison to patients with high CAIX expression, which was in congruence with previous studies showing that low CAIX expression is associated with unfavorable outcome and shorter survival. 15,16,18 Besides, CSS rates were significantly different between the patients in pT1–pT4 stages. A highlight of the authors' study was that, as far as the authors know, for the first time, CSS rates were further compared between patients with tumors containing high and low CAIX expression in different stage subgroups. Only in pT2a, pT2b, and pT3a subgroups, differences in CSS rates were markedly significant between patients with high and low CAIX expression. These observations further prove that CAIX expression correlates with TNM stage in nonmetastatic ccRCC.
Prognostic factors may be varied for RCC patients of different tumor stages. 27 Since significantly different CSS rates between high and low CAIX expression were found in the nonmetastatic ccRCC patients of pT2a, pT2b, and pT3a stages, the authors selected to perform univariable and multivariable Cox regression analysis specifically in these patients and identified CAIX expression, nuclear grade, TNM stage, and necrosis to be independent predictors of prognosis. Previous studies have established that nuclear grade, TNM stage, and necrosis are important prognostic clinical features in RCC. 28,29 According to results of univariable and multivariable Cox analysis, CAIX expression did not have independent prognostic significance for overall nonmetastatic ccRCC patients, whereas CAIX expression is of independent prognostic value for ccRCC patients in pT2a, pT2b, and pT3a stages. CAIX expression would further improve risk stratification of nonmetastatic ccRCC patients. Quantification of CAIX expression in combination with tumor staging could help clinicians more accurately predict prognosis for nonmetastatic ccRCC patients and determine the subgroups of patients who demand closer follow-up and more aggressive therapeutic strategies.
It is still controversial whether CAIX expression is an indicator of prognosis in ccRCC in several published articles. 12,14 –19 Through carefully reviewing these studies, the authors found that most of these studies were conducted at a single center. Besides, the sample size of these studies is smaller than the authors'. The proportion of patients in each TNM stage was different in each study. This may be one of the reasons that lead to different conclusions. They collected a total of 1263 patients from four medical centers to obtain more accurate TNM staging composition. The results showed that low CAIX expression is a risk predictor only for pT2a, pT2b, and pT3a subgroups. This may be a better explanation for the inconsistent prognostic significance of CAIX expression in previous studies.
However, the molecular mechanisms behind the predictive value of CAIX expression in ccRCC remain elusive. CAIX expression is regulated by hypoxia-inducible factor in the acidic microenvironment of tumor cells, participating in regulating tumor growth, proliferation, metastasis, and resistance to anticancer therapies. 30,31 A recently published study reveals that hypoxia-induced CAIX is involved in affecting immune checkpoint blockade by regulating glycolytic metabolism of tumor cells and acidic microenvironment. 32 Cho et al. report that inhibiting CAIX could strengthen the efficacy of 3-bromopyruvate, a hexokinase II inhibitor, in a mouse model. 33 There is in vitro evidence that CAIX plays a role in controlling angiogenesis by modulating pulmonary microvascular endothelial cell pH. 34 In this study, the authors found that the proportion of tumor cell necrosis in low CAIX expression group was significantly higher (19.09% vs. 12.18%) than that in high CAIX expression group (p = 0.006). Therefore, they suspected that low expression of CAIX might be related to tumor ischemic necrosis, poor differentiation, and cell membrane destruction. However, the different performance of further studies is still necessary to unravel the molecular mechanisms of CAIX expression in ccRCC.
Conclusion
Taken together, this study suggests that CAIX expression is an independent prognostic factor in patients with nonmetastatic ccRCC in pT2a, pT2b, and pT3a stages, rather than in all nonmetastatic ccRCC patients. Integration of CAIX expression with TNM stage would lead to a more accurate prediction of prognosis and guide individualized treatment for nonmetastatic ccRCC patients. Furthermore, well- designed prospective studies with long-term follow-up are warranted to validate findings of this study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Yantai Science and technology project (No. 2019YD025), Shandong key research and development plan project (No. 2018GSF118118), and Natural Science Foundation of China (No. 81870525 and 81972376).