
Abstract
Objective:
This study addressed whether preoperative chemotherapy (PECT) plus surgery prolongs overall survival (OS) compared with surgery plus postoperative chemotherapy (POCT) among gastric cancer (GC) patients in Northwest China.
Materials and Methods:
The authors included 157 GC patients confirmed histologically or by gastroscopic pathological examination treated at the General Hospital of Ningxia Medical University of China between 2012 and 2018. All patients were followed up by telephone in January 2019 within a 2-week period. The endpoint was death due to GC or its complications.
Results:
Thirty-eight patients received PECT, 41 patients received POCT, 40 patients received surgery alone, and 38 patients received chemotherapy alone. Surgery was performed with R0 resection and subsequent extended lymph node dissection. Chemotherapy was performed with the S-1, oxaliplatin capecitabine regimen. Patients who received PECT had longer OS than those with POCT treatment (hazard ratio = 2.409, p = 0.037). The 5-year OS rate was 32.7% higher in the PECT group than in the POCT group.
Conclusions:
PECT was associated with better OS in GC patients and should be considered by clinicians in GC treatment, although prospective studies are needed for confirmation.
Introduction
Gastric cancer (GC) is the third leading cause of cancer death worldwide, with an estimated 783,000 deaths in 2018. 1 Over half of the GC deaths worldwide occur in East Asia. 1 In Japan, the 5-year survival of patients with GC was 50.5% in 2000, and it increased to 60.3% in 2014. 2 In China, the 5-year survival rate of GC, which was about 30.2% in 2000 increased by 5.7% in 2014. 2 Although it is promising to see that the overall survival (OS) rate has been enhanced due to early detection techniques and progress in therapeutics, GC is still a heavy health burden. This burden inspires researchers and clinicians to discover more effective therapeutic strategies worldwide, especially in China. 2 –4
Preoperative chemotherapy (PECT), which was first applied to advanced breast cancer in London in the 1970s, can downsize locally advanced (inoperable) disease, and improve resectability. 5 PECT has been employed in the treatment of locally advanced GC, especially in Europe, since the early 1990s. 6 In 2006, Cunningham et al. randomly assigned 503 stomach cancer patients in the United Kingdom to either PECT plus surgery or surgery alone to compare the efficacy of each treatment. 7 They found that patients who received PECT had a higher 5-year survival rate (13%) than patients treated with surgery alone, which meant PECT could prolong the survival of GC patients in some extent. In 2010, Qu et al. selected 76 Chinese GC patients and found that the 2-year survival rates in the PECT group and the postoperative chemotherapy (POCT) group were 59.0% and 28.2%, respectively, which suggested that PECT was superior to POCT for GC patients. 8 However, some other reports have shown that PECT can improve the R0 resection rate and reduce tumor staging, but it has no obvious advantage in terms of the long-term survival rate. 9 –11 Therefore, more investigations in different GC populations, especially in high-incidence GC areas, are still warranted.
This study aimed to evaluate the survival benefit for GC patients treated with PECT compared with GC patients treated with POCT, surgery alone, and chemotherapy alone to optimize the treatment strategy on the basis of collected data. All patients were selected from the Ningxia region, a high-incidence area for GC in Northwest China. 12
Materials and Methods
Patients
A total of 170 patients with GC confirmed histologically or by gastroscopic pathological examination treated at the General Hospital of Ningxia Medical University of China between 2012 and 2018 were retrospectively enrolled in this study. All data were obtained from the patients' medical records at the General Hospital of Ningxia Medical University.
A total of 53 datum, including sex, age, cigarette smoking, alcohol drinking, family history, Borrmann's type, clinical stage, tumor localization, surgical procedures, pathological diagnosis, and other relevant information pertaining to patients with primary gastric carcinoma, were collected for further analyses.
GC patients were eligible for this study if they (1) had histologically proven stage IB-IVA GC (as defined by the American Joint Committee on Cancer, 8th edition), (2) had primary GC, (3) had been treated according to the National Comprehensive Cancer Network (NCCN) guidelines, and (4) had no synchronous or metachronous cancer. Patients with gastroesophageal junction carcinoma were excluded if they were treated with PECT and esophagectomy according to the guidelines for esophageal cancer. The data of 157 GC patients were retrospectively examined after excluding 13 patients who did not meet these criteria.
Informed consent was obtained in all cases, and this study was approved by the Ethics Committee of Ningxia Medical University of China.
Treatment
Patients could be treated with no chemotherapy, PECT, or POCT. Likewise, patients could undergo or forego surgery. Thirty-eight patients received PECT and surgery, 38 patients received chemotherapy alone, 40 patients received only surgery, and 41 patients received surgery and POCT. The authors compared survival outcomes based on the different therapies.
Chemotherapy
Patients were treated with any combination of chemotherapy (administered orally, intravenously, or intraperitoneally). Chemotherapy regimens were classified into two types: (1) S-1, oxaliplatin (SOX) regimen: For SOX therapy, S-1 80 mg/m2 was administered from days 1 to 14 and oxaliplatin 130 mg/m2 was administered on day 1. (2) oxaliplatin, capecitabine (XELOX) regimen: For XELOX therapy, patients received oxaliplatin 130 mg/m2 on day 1 and capecitabine 1000 mg/m2 twice daily from days 1 through 14.
Surgery
Surgical treatment consisted of proximal subtotal gastrectomy, total gastrectomy and subsequent extended lymph node dissection (D2 resection), radical resection of cardiac carcinoma, and palliative subtotal gastrectomy. The operations were in accordance with the NCCN guidelines.
Follow-up
The initial event of this study was admission to the hospital for treatment. The endpoint of this study was cause of death due to GC or complications while in or after discharge from the hospital. Patients who were lost to follow-up or alive at the end of follow-up were censored. OS was calculated from the time of first treatment to the date of death or the last follow-up. All selected patients were followed up by telephone in January 2019 within a 2-week period. The purpose of the phone calls was to collect survival information. Additional phone calls or messages were made to patients who could not initially be contacted. Nine patients were lost to follow-up, so there were follow-up data from 148 patients: 40 patients who were alive and 108 patients who died from GC. The causes of missing information included discontinued phone service, number change, and no response.
Statistical analyses
All analyses were performed using SPSS 24.0 software (IBM Corporation, Armonk, NY). The distribution of baseline characteristics was compared with Pearson's Chi-square (χ 2 ) test or Fisher's exact test. Patient survival was first estimated with the Kaplan–Meier method. To identify independent prognostic factors of GC, a multivariate Cox proportional hazards model was then conducted on the basis of meaningful and clinically relevant factors extracted from univariate analysis. The most appropriate statistic for evaluating primary endpoints (time-to-event outcomes) was the hazard ratio (HR). p < 0.05 was considered statistically significant. All tests were two sided.
Results
Patients' characteristics
From 2012 to 2018, a total of 170 GC patients were treated at their hospital. After assessment of eligibility, 157 patients remained. The included patients' demographic information and clinicopathological characteristics are shown in Table 1. There was no significant difference in the demographic or clinical characteristics among the four groups over the period studied.
Basic Information and Clinicopathological Characteristics of Gastric Cancer Patients Enrolled During 2012–2018 (N = 157)
cN stage, clinical N stage; cT stage, clinical T stage; CT, chemotherapy; PECT, preoperative chemotherapy; POCT, postoperative chemotherapy.
Survival analysis
In this retrospective study, the survival status of all GC patients was compared by both univariate and multivariate analysis (Tables 2 and 3). The median follow-up time for the entire cohort was 12.0 months (0.4–74.2 months). The 1-, 3-, and 5-year OS rates in the PECT group were 68.8%, 55.1%, and 51.0%, respectively, which were significantly higher than the corresponding OS rates in the POCT group (60.0%, 30.5%, and 18.3%, respectively), the surgery group (50.0%, 11.8%, and 15.0%, respectively), and the chemotherapy group (60.5%, 11.8%, and 0%, respectively) (Table 4). PECT (Fig. 1A–D, all p < 0.05), age younger than 55 years (Fig. 1E, p = 0.049), tumor site in the middle (Fig. 1F, p = 0.003), Stage I and II (Fig. 1G, p = 0.001), and radical surgery (Fig. 1H, p = 0.012) were shown to be significant predictors of good survival in GC patients. The Kaplan–Meier curves are provided in Figure 1. Then, to analyze the survival efficacy of the different treatments, they compared the outcomes of patients undergoing PECT, POCT, chemotherapy, and surgery and significant differences were noted. It was shown that there existed statistical differences in the survival of patients undergoing PECT compared with those undergoing other treatments (PECT vs. POCT: p = 0.048, PECT vs. surgery: p < 0.001, PECT vs. chemotherapy: p = 0.008; Fig. 1B–D). The statistical differences were also found in age, tumor site, N stage, clinical stage, and type of resection (Table 2, all p < 0.05). The results of the Cox regression analysis, in which the type of treatment, cigarette smoking, lymph node metastasis, and tumor site were included to identify prognostic factors are shown in Table 3. The type of treatment (HR = 2.409, 95% confidence interval [CI] = 1.056–5.494, p = 0.037), cigarette smoking (HR = 2.067, 95% CI = 1.022–4.180, p = 0.043), and lymph node metastasis (HR = 4.946, 95% CI = 1.438–17.012, p = 0.011) all showed to be significant, independent prognostic factors for OS in GC patients.
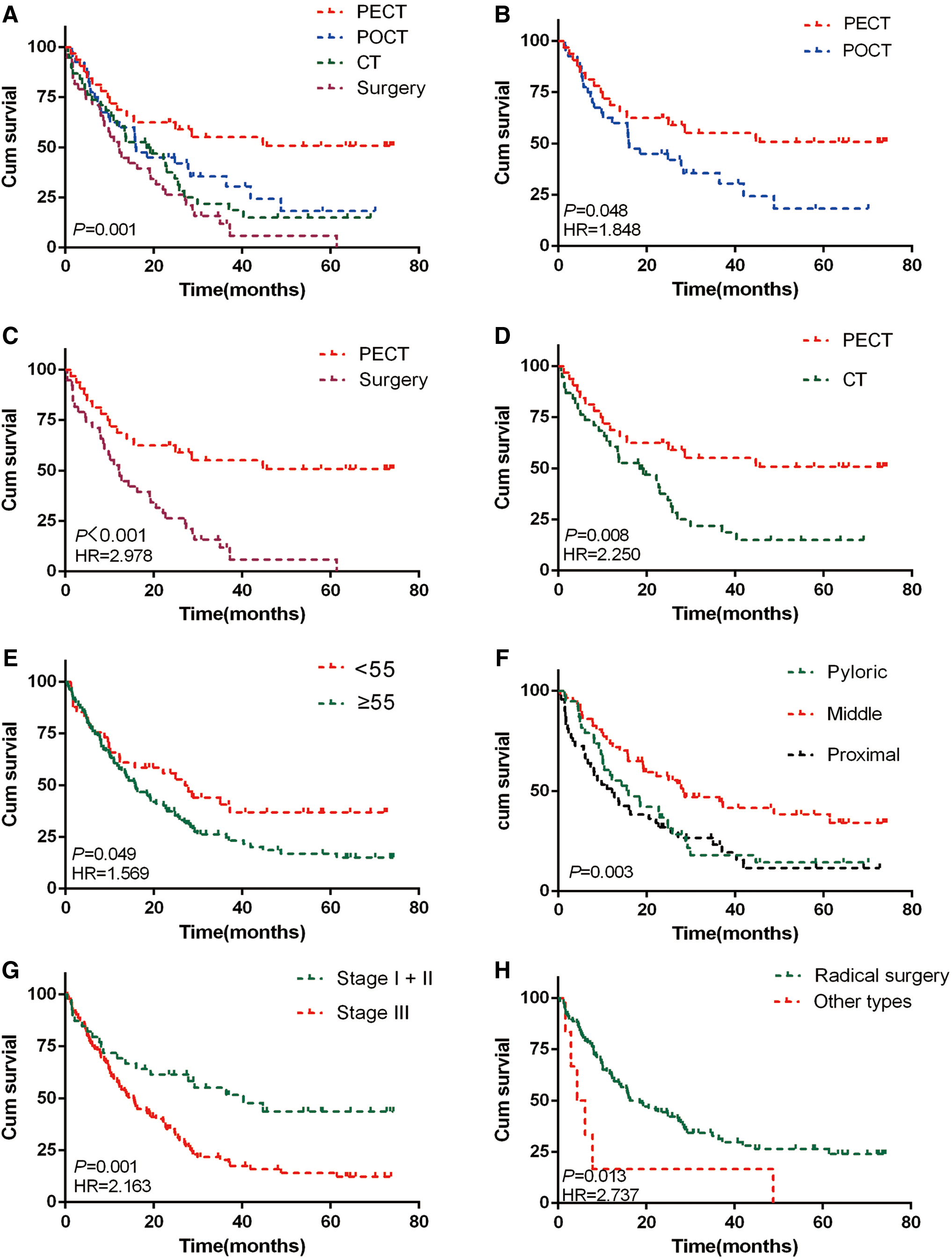
Survival curves of four treatments and clinically related factors in gastric cancer patients.
Univariate Analysis of Overall Survival of Gastric Cancer Patients
Multivariate Analysis of Gastric Cancer Patients
The Overall Survival of Four Treatments of Gastric Cancer Patients
OS, overall survival.
Discussion
This study directly compared the survival benefit of PECT with other treatments in GC patients and demonstrated that patients who received PECT plus gastrectomy had a higher 5-year OS rate than those who received surgery plus POCT (55.1% vs. 30.5%), surgery only (55.1% vs. 15.0%), or chemotherapy alone (55.1% vs. 0%). The results from this study are consistent with those of two previous investigations from Fazio et al. 13 and Kano et al., 14 who showed that the survival rates of GC patients undergoing PECT were higher compared with patients undergoing POCT (44.1% vs. 29.4% and 80.0% vs. 58.7%, respectively).
The survival improvement observed with PECT might be related to tumor regression. Spoerl et al. 15 assessed the tumor response to PECT and confirmed that pathological regression identified on PECT is an important prognostic marker for survival in stomach cancer. In that study, TRG1a (defined as no residual cancer found on histological examination of the specimen) was achieved in 8.8% of patients treated with PECT, and TRG1b (subtotal regression, <10% residual tumor) was achieved in 27.3% of patients treated with PECT. These patients had a more favorable prognosis (3-year survival rates: 82.8% and 71.3%, respectively) when regression was accompanied by a decrease in maximum infiltrative depth, referred to as tumor shrinkage. More importantly, in the remaining 63.9% of patients whose tumors did not recede, the survival rates were lower, although still above 37.9%. Therefore, patients who had a complete or partial response had significantly better OS than nonresponding patients or the immediate surgery group. 16 –19
The reasons for tumor shrinkage after PECT are manifold. First, PECT is generally better tolerated than POCT. Therefore, patients are most likely to receive sufficient treatment dosage and have the highest probability of receiving multimodal treatment if the treatment starts before surgery. This is also true for primarily resectable cancer. 20 Second, tumor resection can induce the production of tumor cell growth-stimulating factors, which make tumor cells grow rapidly and be less responsive to antichemotherapy agents. 21 Accordingly, noncurative reduction of the tumor increases proliferation of the residual tumor. This can be prevented by administering PECT instead of POCT. 22 Last, many patients with advanced cancer may theoretically undergo complete tumor resection, and PECT may allow for safer surgical intervention. 23 However, if the tumor spread is extensive and/or the general condition of the patient is poor, the risk of preoperative mortality may outweigh any potential benefits. Furthermore, postsurgical complications usually result in the delay of postoperative therapy, which negatively impacts treatment outcomes.
PECT may be conducted on the basis of different treatment modalities. Because there are fewer tumor cells in patients with early stage disease, the proliferation rate is high and doubling time is relatively short. In contrast, more advanced tumor cells with a low proliferation rate will have a prolonged doubling time and a decreased sensitivity to chemotherapeutic drugs. 24 Therefore, using a drug that does not target the cell cycle can reduce the tumor volume and improve the proliferation rate, thereby increasing the sensitivity to cell cycle-specific chemotherapeutic drugs. 25 Recently, many new drugs, including SOX and XELOX, have been administered as PECT. Xue et al. suggested that there was no significant difference in survival in patients receiving SOX and XELOX (5-year survival rates: 78% and 66%, respectively). According to Samaratunga et al., 26 the SOX regimen induced a relatively high number of pathologically complete responses without increasing morbidity and mortality. This study showed that, in patients receiving SOX or XELOX, the 5-year survival rate of patients receiving PECT was 32.7% higher compared with patients receiving POCT. Therefore, it is not surprising that the SOX regimen is considered to be one of the most effective chemotherapy treatments for GC, particularly in China and Japan 27 –30 (it is not available in most other countries). However, it is still controversial whether PECT based on SOX or XELOX is more advantageous than POCT.
In addition, curative resection with D2 lymphadenectomy is recommended for advanced GC, according to the Japanese, 31 Korean, 32 British, 32 German, 33 and Italian guidelines. 34 In this study, because of the large number of patients with advanced GC having lymph node metastases, D2 lymphadenectomies were performed in more than 90% of cases. Therefore, there was no difference in the extent of lymph node dissection between the PECT and POCT groups. However, the benefits of PECT on lymph node dissection were assessed by a group from the European Institute of Oncology in Milan. 35 Their study indicated that the median number of metastatic lymph nodes (1 vs. 5) and the median number of excised lymph nodes (20 vs. 26) were lower in patients who received PECT than in patients who received POCT. The investigation by Chao et al. 36 concluded that extensive lymph node dissection after preoperative therapy confers a strong survival benefit. PECT has also been confirmed to eliminate micrometastases and improve the success rate of surgery. 37 Therefore, it is reasonable to assume that patients receiving PECT have fewer metastatic lymph nodes. These benefits were reflected in their study (5-year OS rate of PECT vs. POCT: 55.1% vs. 30.5%).
However, this study has some limitations. It is a retrospective study, and only early outcomes were observed. That the OS of the PECT group was longer compared with the other treatment groups may not necessarily be because the mortality was higher in the other groups. The results also depend on the quality of data collection. Furthermore, there were only 38 patients in the PECT group, and the effect of PECT still needs to be verified in a larger study. Additionally, evaluation of PECT efficacy was hampered by patient withdrawal during the treatment process, mainly due to transfer to another hospital or no longer receiving the same therapy. Despite controlling for many important factors that can influence long-term survival and cancer recurrence, there are inevitably other confounding variables that were not studied. Nonetheless, this study highlights the important finding that PECT has survival advantages over other therapies in patients with stage IB to III GC.
Conclusion
In summary, these data from a high GC incidence area of China showed that PECT with D2 gastrectomy had a better outcome than the surgery-first approach for patients with cStage IB to III GC. Therefore, PECT should be considered by clinicians in GC treatment, and SOX regimen should be considered preferentially for the preoperative treatment, although more prospective studies are needed for confirmation.
Footnotes
Acknowledgments
The authors thank Wiley for the linguistic assistance during the preparation of this article. They thank all of the participants of this study.
Authors' Contributions
Guarantor of integrity of the entire study: W.Y. and Z.C. Study concepts and design: Q.Z., Qinghua Z., J.C., W.W., D.Z., X.Z., J.W., and W.Y. Literature research: Qinghua Z., H.Y., and Y.Y. Clinical studies: N/A. Experimental studies/data analysis: N/A. Statistical analysis: Q.Z. and J.C. Article preparation: Q.Z., W.Y., and Z.C. Article editing: Q.Z., W.Y., and Z.C.
Disclosure Statement
No competing financial interests exist.
Funding Information
W.Y. was supported by grants from National Natural Science Foundation of China [Grant Nos. NSFC 81760525, 81160249, and 81860426].