
Abstract
Background:
This study investigated the association of circulating tumor cells (CTCs) change during chemoradiation with the treatment response and survival profiles in advanced nonsmall-cell lung cancer (NSCLC) patients.
Materials and Methods:
Fifty-eight advanced NSCLC patients who underwent concurrent chemoradiation were enrolled; their peripheral blood samples were collected before chemoradiation, and at 1 month postchemoradiation, the CTCs were assayed using a CTC-Biopsy system. Moreover, CTCs were classified as CTCs positive and CTCs negative according to CTCs' count, and change of CTCs was calculated. In addition, response of chemoradiation was evaluated at 1 month postchemoradiation, then progression-free survival (PFS) and overall survival (OS) were assessed.
Results:
Prechemoradiation CTCs positive were associated with increased TNM stage, but not other clinicopathologic characteristics. After chemoradiation, the CTCs' number [1.0 (0.0–3.0) vs. 4.0 (2.0–10.0)] and the percentage of CTC-positive cases (37.9% vs. 77.6%) were both decreased compared to those before chemoradiation. Regarding treatment response, prechemoradiation CTCs positive were associated with lower partial response; postchemoradiation CTCs positive were associated with reduced disease control rate, while CTCs' change during chemoradiation was not associated with treatment response. Kaplan–Meier curves showed that postchemoradiation CTCs positive and increased CTCs' number during chemoradiation were associated with reduced PFS, then multivariate Cox's regression analysis disclosed that they independently predicted decreased PFS. However, no correlation of CTCs' status or CTCs' change with OS was observed.
Conclusions:
Prechemoradiation CTCs relate to increased TNM stage and worse prognosis in chemoradiation-treated advanced NSCLC patients.
Introduction
Lung cancer, with 80%–85% being nonsmall-cell lung cancer (NSCLC), remains the main cause of cancer-related death worldwide. 1,2 More than one-third of all newly diagnosed lung cancer cases occur in China, making it a large social and economic burden. 3 For NSCLC patients diagnosed at early stage, surgery is commonly used to remove the tumor, while most NSCLC patients are diagnosed with advanced-stage disease owing to inadequate screening and late onset of clinical symptoms.
Then, for the advanced-stage disease, patients with gene mutations (such as mutation in the epidermal growth factor receptor [EGFR] gene) can benefit from targeted therapy (such as tyrosine kinase inhibitors [TKIs] of EGFR), whereas patients unavailable for target therapy have to receive chemotherapy alone or in combination with radiation therapy, by which the efficacy is still far from satisfactory. 4,5
Circulating tumor cells (CTCs) are the tumor cells that originate from either primary tumor or its metastasis circulating in the peripheral blood. 6 Detection, monitoring, and molecular investigation of CTCs offer a meaningful and noninvasive way to customize individual treatment plans and have a better surveillance for tumor progression. 3,7
As to NSCLC, a few investigations disclose the correlation of CTCs with prognosis in advanced NSCLC patients. 8 –10 For instance, one study shows that high baseline CTCs' level is associated with fewer treatment response and shorter survival profiles in TKI or chemotherapy-treated advanced NSCLC patients. 8 Also, a study displays that baseline CTCs' level is correlated with unfavorable progression-free survival (PFS) and overall survival (OS) in TKI-treated advanced NSCLC patients. 10 Another study displays that higher posttreatment CTCs' level correlates with worse treatment response in chemotherapy-treated advanced NSCLC patients. 9
However, the indications from these previous studies are restricted to the patients treated with targeted therapy or chemotherapy alone, and they merely focus on the reflection of prognosis by pretreatment or posttreatment CTC measurement in advanced NSCLC patients, but limited evidence uncovers the role of CTCs' change during chemoradiation in advanced NSCLC patients. To address this, the authors paid attention to the longitude change of CTCs in chemoradiation-treated advanced NSCLC patients, and aimed to investigate the association of CTCs' change during chemoradiation with the treatment response and survival profiles in advanced NSCLC patients.
Materials and Methods
Patients
From July 2016 to June 2019, a total of 58 advanced NSCLC patients who underwent concurrent chemoradiation in Changzhou Tumor Hospital Affiliated to Soochow University were consecutively recruited if they met the following criteria: (1) diagnosed as NSCLC; (2) older than 18 years of age; (3) TNM stage IIIB–IV (The eighth edition of the American Joint Committee on Cancer staging system); (4) Eastern Cooperative Oncology Group (ECOG) score 0–2; (5) unable to receive resection evaluated by the Thoracic Malignancy Multi-disciplinary Clinic; and (6) schedule to receive concurrent chemoradiation. Patients had history of other malignancies, had severe infection, severe liver/kidney dysfunction, severe cardiovascular disease, or numerous metastasis were excluded.
This study was approved by the Institutional Review Board of Changzhou Tumor Hospital Affiliated to Soochow University. All patients or their family members provided written informed consents.
Data collection
After enrollment, patients' clinical characteristics were recorded, which included the information of age, gender, smoke status, ECOG score, histological type, TNM stage, carcinoembryonic antigen (CEA) level, carbohydrate antigen 125 (CA125) level, cytokeratin 19 (CYFRA21-1) level, and neuron-specific enolase (NSE) level.
Treatment
All patients received concurrent chemoradiation. The radiotherapy was delivered to the primary tumor and nodal metastatic sites or oligometastatic site with the basis of size criteria as follows: 5250–6000 cGy in 15–20 fractions of external beam Intensity Modulated Radiation Therapy (300–350 cGy per fraction, 5 fraction per week) with Varian Clinac IX Linear Accelerator (Varian Medical Systems, American). The chemotherapy was carried out as one of the following regimens according to National Comprehensive Cancer Network clinical practice guidelines in Oncology: Non-Small Cell Lung Cancer (Version 4. 2016): (1) cisplatin 50 mg/m2 on days 1, 8, 29, and 36; etoposide 50 mg/m2 days 1–5, 29–33 and (2) paclitaxel 45–50 mg/m2 weekly and carboplatin area under the curve (AUC 2).
CTCs assessment
Peripheral blood samples (5 mL) of patients were collected in ethylenediamine tetraacetic acid tubes at 24 h prechemoradiation and 1 month postchemoradiation, respectively. The collected blood samples were processed immediately to assess the CTCs using a CTC-Biopsy system (Wuhan YZY Medical Science & Technology Co., Ltd., China). CTCs were gathered based on isolation by size of epithelial tumor cells technology and separated with the use of Romanowsky staining, which were performed according to the method from a previous report. 11 Then, the stained cells were observed at 100 × /200 × original magnification for cell counting, further observed at 630 × /1000 × original magnification with oil immersion for detailed cytomorphologic analysis. 11
The CTCs were identified by the presence of at least four of the following criteria: (1) irregular nuclear borders; (2) nuclear-cytoplasmic ratio >0.8; (3) nucleus larger than 18 μm; (4) hyperchromatic and uneven nucleus; (5) thickened and wrinkled nuclear membrane; and (6) nuclear deviation, large nucleoli, or abnormal nuclear division. CTCs positive were defined as the count of CTCs in 5 mL peripheral blood sample ≥2. 12 CTCs' change was calculated by subtracting CTCs postchemoradiation from CTCs prechemoradiation, and the negative value was defined as CTCs' up, the positive and unchanged value was defined as CTCs' down/unchanged.
Follow-up and outcomes assessment
All patients received serial radiographic surveillance with either positron emission tomography-computed tomography (CT) or intravenous contrast CT scans 1 month postchemoradiation, every 3 months in the first 2 years, then every 4–6 months. The response of chemoradiation were evaluated at 1 month postchemoradiation according to the response evaluation criteria in solid tumors (Version 1.1), 13 which included (1) complete response (CR), disappearance of all target lesions; (2) partial response (PR), at least a 30% decrease in the sum of diameters of target lesions, taking as reference the baseline sum diameters; (3) progressive disease (PD), at least a 20% increase in the sum of diameters of target lesions, taking as reference the smallest sum on study; and (4) stable disease (SD), neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD.
Meanwhile, objective response rate (ORR) was defined as the percentage of patients with CR or PR, and disease control rate (DCR) was defined as the percentage of patients with CR, PR, or SD. The disease status and survival status of patients were recorded regularly by visit or telephone. PFS was calculated from the date of initiation of chemoradiation to the date of progression or death, and for the patients not known to have progression or died at the last follow-up, they were censored on the date of the last examination. OS was calculated from the date of initiation of chemoradiation to the date of death, and for the patients not known to have died at the last follow-up, they were censored on the date of last known to be alive.
Statistical analysis
Statistical analyses were performed using SPSS 22.0 software (IBM, USA). Figures were plotted using GraphPad Prism 7.01 software (GraphPad Software, USA). Comparison between prechemoradiation CTCs and postchemoradiation CTCs was determined by Wilcoxon signed-rank test or McNemar's test. Comparison between CTC-negative patients and CTC-positive patients was determined by χ 2 test. Comparison between CTCs' down/unchanged patients and CTCs' up patients was determined by χ 2 test or Fisher's exact test.
PFS and OS were illustrated using Kaplan–Meier curves, and the differences in PFS and OS between the two groups were determined by log-rank test. Comparison of prechemoradiation CTCs with metastasis status in the patients with TNM stage IV by Kruskal-Wallis H test or χ 2 test. Factors independently predicting PFS and OS were analyzed by backward stepwise multivariate Cox's proportional hazard regression model. p-Value <0.05 was considered significant.
Results
Characteristics of NSCLC patients
Fifty-eight NSCLC patients [including 10 (17.2%) females and 48 (82.8%) males] with mean age of 63.0 ± 12.0 years were enrolled (Table 1). There were 10 (17.2%), 36 (62.1%), and 12 (20.7%) patients who showed ECOG score of 0, 1, and 2, respectively. Regarding the histological type, 35 (60.3%) patients were identified as squamous cell carcinoma and 23 (39.7%) patients were identified as adenocarcinoma. As to TNM stage, 30 (51.7%) patients were with TNM stage IIIB and 28 (48.3%) patients were with TNM stage IV. Besides, detailed information of tumor biomarkers such as CEA, CA125, CYFRA21-1, and NSE was exhibited in Table 1.
Patients' Characteristics
ADC, adenocarcinoma; CA125, carbohydrate antigen 125; CEA, carcinoembryonic antigen; CYFRA21-1, cytokeratin 19; ECOG, Eastern Cooperative Oncology Group; NSCLC, nonsmall-cell lung cancer; NSE, neuron-specific enolase; SCC, squamous cell carcinoma.
Association of prechemoradiation CTCs with clinicopathologic characteristics
According to the prechemoradiation CTCs' level, 45 patients were categorized as CTC-positive patients and 13 patients were categorized as CTC-negative patients (Table 2). CTCs positive were associated with increased TNM stage in NSCLC patients (p = 0.007), whereas no correlation of CTCs' status with age (p = 0.421), gender (p = 0.301), smoking (p = 0.457), ECOG score (p = 0.189), histological type (p = 0.457), CEA (p = 0.988), CA125 (p = 0.167), CYFRA21-1 (p = 0.701), or NSE (p = 0.490) was found in NSCLC patients.
Correlation of Prechemoradiation Circulating Tumor Cells with Clinicopathologic Characteristics
Comparison was determined by χ 2 test.
CTCs, circulating tumor cells.
Comparison between postchemoradiation CTCs and prechemoradiation CTCs
The number of postchemoradiation CTCs was decreased compared to the number of prechemoradiation CTCs [1.0 (0.0–3.0) vs. 4.0 (2.0–10.0), p = 0.004] (Table 3), meanwhile, the percentage of postchemoradiation CTC-positive cases was reduced compared with percentage of prechemoradiation CTC-positive cases (p < 0.001).
Comparison Between Prechemoradiation Circulating Tumor Cells and Postchemoradiation Circulating Tumor Cells
Comparison was determined by Wilcoxon signed-rank test or McNemar's test.
IQR, interquartile range.
Association of CTCs' status with treatment response to chemoradiation
Prechemoradiation CTCs positive were associated with lower PR (p = 0.039), while no correlation of prechemoradiation CTCs' status with CR (p = 0.439), SD (p = 0.326), PD (p = 0.320), ORR (p = 0.073), or DCR (p = 0.320) was discovered in NSCLC patients (Table 4). Moreover, postchemoradiation CTCs positive were associated with increased PD (p = 0.025) and reduced DCR (p = 0.025), while no correlation of postchemoradiation CTCs' status with CR (p = 1.000), PR (p = 0.837), SD (p = 0.141), or ORR (p = 0.940) was found in NSCLC patients. In addition, the CTCs' change during chemoradiation was not associated with treatment response in advanced NSCLC patients (all p > 0.05).
Correlation of Circulating Tumor Cells Status with Treatment Response
Comparison was determined by chi-square test or Fisher's exact test.
Association of CTCs' status with PFS
The prechemoradiation CTCs positive showed a trend to be correlated with shorter PFS in NSCLC patients, with no significant difference (p = 0.053) (Fig. 1A). Moreover, postchemoradiation CTCs positive (p = 0.016) (Fig. 1B) and CTCs' up after treatment (p = 0.034) (Fig. 1C) were associated with reduced PFS in NSCLC patients.
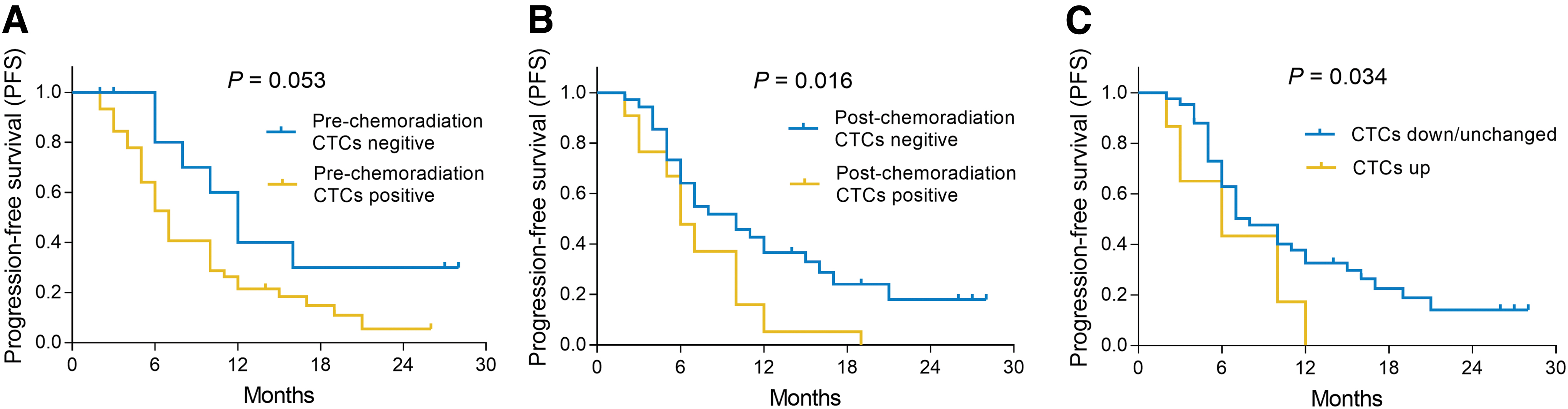
Correlation of CTCs with PFS in NSCLC patients. Correlation of prechemoradiation CTCs' status
Association of CTCs' status with OS
No correlation was discovered between prechemoradiation CTCs' status (p = 0.584) (Fig. 2A), postchemoradiation CTCs' status (p = 0.131) (Fig. 2B), or CTCs' change and OS (p = 0.292) (Fig. 2C) was observed in NSCLC patients. In this study, there were 30 NSCLC patients at TNM stage IIIB and 28 NSCLC patients at TNM stage IV. The authors assessed the correlation of prechemoradiation CTCs with PFS and OS in patients with TNM stage IIIB as well as patients with TNM stage IV, and they discovered no correlation of prechemoradiation CTCs with PFS (p = 0.122) (Supplementary Fig. S1A) and OS (p = 0.796) (Supplementary Fig. S1B) in patients with TNM stage IIIB; Also, prechemoradiation CTCs were also not associated with PFS (p = 0.624) (Supplementary Fig. S1C) and OS (p = 0.762) (Supplementary Fig. S1D) in patients with TNM stage IV.

Correlation of CTCs with OS in NSCLC patients. Correlation of prechemoradiation CTCs' status
Among 28 NSCLC patients at TNM stage IV, there were 13 cases with osseous metastasis, 7 cases with brain metastasis, 5 cases with liver metastasis, 3 cases with others. No difference was found in number of CTCs (p = 0.381) and CTCs' status (p = 0.478) among different sites of metastasis in the patients with TNM stage IV (Supplementary Table S1). Meanwhile, they compared the PFS and OS among different sites of metastasis in the patients with TNM stage IV, and it was found that there was difference in PFS (p = 0.021) (Supplementary Fig. S2A), but not different in OS (p = 0.126) (Supplementary Fig. S2B) among different sites of metastasis in the patients with TNM stage IV. Furthermore, there was also no correlation of PFS (p = 0.164) (Supplementary Fig. S3A) and OS (p = 0.349) (Supplementary Fig. S3B) between NSCLC patients with brain metastasis and patients without brain metastasis.
Analysis of factors affecting PFS and OS
Backward stepwise multivariate Cox's proportional hazard regression model analysis displayed that prechemoradiation CTCs positive (p = 0.008) (HR: 3.346, 95% CI: 1.379–8.121) were an independent predictive factor for unfavorable PFS, so did CTCs' change (up vs. down/unchanged) (p = 0.002) (HR: 3.130, 95% CI: 1.504–6.516) and NSE level (abnormal vs. normal) (p = 0.026) (HR: 2.199, 95% CI: 1.099–4.400) (Table 5). In addition, NSE level (abnormal vs. normal) (p = 0.022) (HR: 2.504, 95% CI: 1.144–5.483) was an independent factor predicting worse OS in NSCLC patients.
Independent Factors Predicting Progression-Free Survival and Overall Survival
Factors independently predicting PFS and OS were analyzed by backward stepwise multivariate Cox's proportional hazard regression model.
CI, confidence interval; HR, hazard ratio; NSE, neuron-specific enolase; OS, overall survival; PFS, progression-free survival.
Discussion
Knowledge of metastasis may help understand the biology of CTCs in NSCLC. 7,14,15 Metastasis is an extremely complex process that requires multiple steps, in which the tumor cells must undergo a crucial cellular process termed as epithelial mesenchymal transition (EMT). 7 EMT enables the tumor cells to be motile, and also allows the cells to penetrate into the lymph vessels and to circulate as a single or clusters of CTCs. 7,14,15 In this way, CTCs spread to distant organs and facilitate the formation of secondary sites of the tumor disease, moreover, CTCs could form the disseminating tumor cells, which are known as a settlement of CTCs in other organs that may stay in a quiescence state or lead to an detectable metastasis. 16 Thus, CTCs are regarded as potential metastasis-inducing cells.
In addition, previous data demonstrate that the CTC clusters present with high expression of adhesion markers (such as MPDZ and TNC genes), which endow the clusters an advantage of avoiding anoikis in the circulation; furthermore, various genetic alterations (such as EGFR, mesenchymal-epithelial transition factor, and B-Raf proto-oncogene [BRAF]) that correlate with resistance of chemotherapy are abundantly expressed on CTCs. 17 –19 Regarding these properties, monitoring CTCs may bring important indications for the progression of NSCLC.
In clinical practices, previous investigations have disclosed that CTCs provide important reflection for the clinicopathological features of lung cancer patients: one study shows the positive association of prechemoradiation CTCs' count with lymph node metastasis, distant metastasis, and elevated TNM stage in small-cell lung cancer (SCLC) patients. 20 Another study discloses that prechemotherapy CTCs positive are associated with lymph node metastases and larger primary tumors in early stage NSCLC patients. 21
However, the related evidence in advanced NSCLC patients is limited. In the authors' study, it was observed that the prechemoradiation CTCs positive were associated with increased TNM stage in advanced NSCLC patients, which might result from the following facts: higher CTCs' count indicated that more cancer cells could be displaced to distant site, which was a crucial step promoting the process of metastasis and leading to elevated TNM stage, thus prechemoradiation CTC-positive status was positively correlated with TNM stage in advanced NSCLC patients. 7,14
In view of the detection of CTCs' change during treatment in advanced NSCLC patients, it is reported in only two previous studies. One study displays that there is no change of CTCs' number among the time points of post-first cycle of chemotherapy, post-second cycle of chemotherapy, and post-third cycle of chemotherapy in advanced NSCLC patients. 9 Another shows that CTCs' number is increased in the majority of TKI-treated advanced NSCLC patients. 10 However, corresponding investigation in chemoradiation-treated advanced NSCLC patients is seldom reported. The authors' study compared the postchemoradiation CTCs' number and prechemoradiation CTCs' number, then found that the CTCs' number and percentage of CTC-positive cases both decreased after chemoradiation compared with those before chemoradiation. These results could be explained by the following theory. Chemotherapy in combination with radiation directly promoted apoptosis of CTCs; meanwhile, chemoradiation induced tumor necrosis, inhibited tumor progression, and further attenuated the production of CTCs, thus CTCs' number and percentage of CTC-positive cases were reduced after chemoradiation therapy in advanced NSCLC patients.
Moreover, CTCs assessment is a useful way for the surveillance in cancer patients' prognosis after treatment. 22 –25 For example, negative association of CTCs' level and treatment response has been revealed in several cancers, such as nasopharyngeal carcinoma, colorectal cancers, and breast cancer. 23 –25 With regard to lung cancer, one study shows that the prechemoradiation CTCs is negatively associated with PR in advanced NSCLC patients. 22 Furthermore, a study displays that elevated preradiation CTCs and persistence of postradiation CTCs both associate with higher recurrence risk outside the targeted treatment site in early stage NSCLC patients. 26 Another study displays that higher prechemoradiation CTCs' level is an independent predictive factor for worse OS in SCLC patients. 20
All these studies merely evaluate the correlation of pretreatment or posttreatment CTCs' level with prognosis of lung cancer patients, resulting in a paucity of evidence about the role of CTCs' change during treatment in advanced NSCLC patients. Meanwhile, related evidence in chemoradiation-treated advanced NSCLC patients is limited. Therefore, the authors' study explored the association of pretreatment CTCs, posttreatment CTCs, and CTCs' change during treatment with the treatment response and survival profiles in chemoradiation-treated advanced NSCLC patients. Also, they observed that in advanced NSCLC patients, prechemoradiation CTCs positive were associated with decreased PR, meanwhile, postchemoradiation CTCs positive were associated with elevated PD and reduced DCR in advanced NSCLC patients.
In addition, prechemoradiation CTCs positive, postchemoradiation CTCs positive, and CTCs' up after treatment were associated with shorter PFS. The possible reasons for these results might be as follows: (1) CTCs are able to access the distant organs and prechemoradiation CTCs positive may indicate that CTCs have undergone the EMT process and tend to colonize at distant organs, which facilitates the distant metastasis and indicates less possibility to achieve survive from the disease; thus prechemoradiation CTCs positive were associated with decreased PR and shorter PFS in advanced NSCLC patients who underwent chemoradiation therapy 27 –29 ; (2) postchemoradiation CTCs positive and CTCs' up after treatment indicate that considerable CTCs survive from the chemoradiation therapy and may further facilitate the formation of tumors at secondary sites, leading to aggravated progression, thus in their study, postchemoradiation CTCs positive correlated with increased PD, reduced DSE, and shorter disease-free survival in advanced NSCLC patients. 17 –19
There were still some limitations regarding this study design, which needed to be improved in future. First, the sample size of 58 was small, which might cause a relatively low statistical efficacy, hence larger number of patients was desirable for a further study. Second, this was a single-center study, which might have some selection bias, and thus further validation of the findings in a multicenter study is needed. Third, the postchemoradiation CTCs were only detected at 1 month after treatment, but not at a long-term period, whereas it would be difficult to constantly count CTCs during the follow-up. Fourth, this study focused just on NSCLC patients who underwent concurrent chemoradiation, while the role of CTCs in NSCLC patients receiving other treatments was not investigated. Thus, a further relevant study is needed.
Furthermore, additional detection of CTCs and the mechanism of CTCs underlying NSCLC were not explored. Hence, further relevant studies are needed. Meanwhile, this study was a retrospective study and there was no validation cohort. Further prospective study with a validation cohort is necessary.
Conclusion
In conclusion, longitudinal change of CTCs relates to disease severity and prognosis in chemoradiation-treated advanced NSCLC patients.
Availability of Data and Material
The dataset supporting the conclusions of this article is included within the article.
Footnotes
Authors' Contributions
Conception and design: X.L.; collection and assembly of data: J.L. and Y.L.; data analysis and interpretation: C.G. and L.Z.; article writing: All authors.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.