
Abstract
Objective:
This study explored the application value of the maximum standard uptake value (SUVmax) of 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (18F-FDG PET/CT) in gastric cancer.
Materials and Methods:
Data of 164 patients with gastric cancer who had undergone18F-FDG PET/CT before a biopsy were collected, and the correlation of SUVmax with clinical stage, pathological differentiation degree, human epidermal growth factor receptor-2 (HER-2) status, and Ki-67 index of gastric cancer was analyzed.
Results:
The SUVmax of poorly differentiated adenocarcinoma was significantly higher than that of moderately differentiated adenocarcinoma and signet-ring cell carcinoma (p < 0.01), and SUVmax in the well-differentiated adenocarcinoma group was higher than that in the signet-ring cell carcinoma group (p < 0.01). The SUVmax in the HER-2 negative group was higher than that in the HER-2 positive group (p < 0.01). The SUVmax was higher in the Ki-67 high expression group than in the low expression group (p < 0.01), and there was a significant positive correlation between the two (p < 0.01).
Conclusion:
18F-FDG PET/CT SUVmax can, to some extent, predict the degree of differentiation, HER-2 status, and Ki-67 index of gastric cancer patients.
Introduction
The prevalence and mortality of gastric cancer rank third of all malignant tumors in China. 1 In recent years, the incidence of gastric cancer has reflected an obvious trend, affecting younger populations while showing a high mortality rate and poor prognosis. Surgery is the most effective treatment method for resectable gastric cancer. However, the early diagnosis rate of gastric cancer in China is low. Most of the diagnoses are in the middle and late stages, so these patients have no chance of undergoing surgery. Therefore, a comprehensive and effective treatment plan with accurate prognosis judgment needs to be devised for these patients. The formulation of such depends on the pathological stage, histological type, the status of pathological molecular marker Ki-67, and antihuman epidermal growth factor receptor-2 (HER-2) of gastric cancer. Although a pathological biopsy remains the gold standard for obtaining these parameters, its invasiveness limits the number of sampling sites. Moreover, it is impossible to obtain samples at multiple sites frequently for continuous evaluation. Therefore, the use of noninvasive diagnostic tools to predict oncological behavior is becoming more important in the field of gastric cancer.
18 F-fluorodeoxyglucose-positron emission tomography/computed tomography ( 18 F-FDG PET/CT) is a new imaging technology, which combines three-dimensional imaging with metabolic imaging, 2 and the most commonly used imaging agent for it is 18 F-FDG, which is a glucose analogue. The metabolic rate of glucose in cancer cells is higher, so the FDG uptake is higher and the standard uptake value (SUV) reflects this metabolic capacity. This technology is usually used to evaluate the biological invasiveness of malignant tumors. Present research results reveal that maximum standard uptake value (SUVmax) is correlated with clinical features and pathological molecular biological markers in lymphoma, breast cancer, lung cancer, and colorectal cancer. However, studies on its application in gastric cancer are rare. In this study, the correlation of SUVmax with the clinical characteristics and pathological and biological indicators of gastric cancer was analyzed to find noninvasive indicators for predicting the biological behavior of gastric cancer and to provide a basis for developing reasonable and effective treatment programs.
Materials and Methods
Subjects
Between January 2011 and December 2017, 164 patients who were diagnosed with gastric cancer by pathology and had undergone 18 F-FDG PET/CT before a biopsy were enrolled in this study. The Ethics Committee of the hospital approved this study and all patients provided signed informed consent.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) patients with gastric cancer diagnosed by pathology after a biopsy, (2) patients who had undergone 18 F-FDG PET/CT before a gastroscopic biopsy, and (3) patients with accurate and comprehensive pathological results and complete clinical data. The exclusion criteria were as follows: (1) patients with incomplete pathological results, (2) patients who underwent 18 F-FDG PET/CT after a gastroscopic biopsy, (3) patients with incomplete clinical data, and, (4) patients with secondary malignant disease, serious infection, or inflammation.
18 F-FDG PET/CT and image analysis
The detection instrument used was the Discovery STEPET/CT instrument of GE. Raw materials, 18 H2O, and FDG synthetic kits were purchased from Jiangsu Huayi Technology Co., Ltd. (China) and 18 F ion was produced by GE MiniTrace cyclotron. Then 18 F-FDG was produced by the GEtracerlabFXF-N automatic synthesis module. The radiochemical purity was >95%. The patients fasted for 6 h before the 18 F-FDG PET/CT examination, and their blood sugar was controlled at <70 mg/dL. They were injected intravenously with 3.7 MBq/kg of 18 F-FDG, according to their body weight, and drank 600–800 mL of water after 20 min of rest. Patients were asked to urinate just before images were acquired, while the images were acquired. Two or more experienced PET/CT diagnostic physicians read the images independently. Visual and semiquantitative analysis methods were used for image analysis and interpretation. Visual observation: radioactive uptake of the lesions was defined as higher than, equal to, and lower than the normal homologous tissues around the lesions, with a total of three levels. Semiquantitative analysis: for high metabolic lesions in the gastric tumors (with FDG uptake of the normal gastric wall as the background), the maximum SUV (SUVmax) was calculated automatically by the Xeleris workstation. For metabolic lesions with an equal metabolic rate, ROI was delineated based on the lesions revealed by CT after gastric filling, and the SUVmax was calculated automatically by the Xeleris workstation.
The detection of Ki-67 and HER-2 expression in lesions and the determination of HER-2 by fluorescence in situ hybridization (FISH)
All the 164 biopsy specimens of gastric cancer were fixed with a neutral formaldehyde fixative and embedded with paraffin. The detection of Ki-67 and HER-2 expression in lesions and the determination of HER-2 by FISH then took place.
Statistical methods
Data were statistically analyzed using statistical software SPSS22.0. Measurement data were expressed as mean ± standard deviation (x ± SD), and count data were expressed as a percentage (%). Normality was tested using a W-test, and the homogeneity of variance was tested using an F-test. The variables were compared between the two groups using a t-test, and non-normally distributed mean or normally distributed mean with the heterogeneity of multiple samples were evaluated using a nonparametric test. Count data were evaluated using a χ 2 test. The correlation between SUVmax and Ki-67 expression was analyzed using Spearman's correlation analysis. The receiver operating characteristic (ROC) curve was used to select the best SUVmax value of the different diagnostic groups and to determine the sensitivity and specificity. p < 0.05 was considered statistically significant.
Results
General information
A total of 164 patients were included in this study. Among these patients, 103 patients were male and 61 patients were female. The age of these patients ranged from 25 to 86 years, and the median age was 60 years. The patients were divided into stages I, II, III, and IV, according to the eighth edition of the American Joint Committee on Cancer's (AJCC) gastric cancer pathological staging system, published by the International Union Against Cancer. There were 66 patients at stages I–II and 98 patients at stages III–IV. The patients were divided into three groups, according to the degree of pathological differentiation: the moderately and highly differentiated group (n = 81), the poorly differentiated group (n = 48), and the signet-ring cell carcinoma group (n = 35). The patients were also divided into two groups according to the status of HER-2: the HER-2 positive group (n = 22) and the HER-2 negative group (n = 142). The Ki-67 index was determined by using immunohistochemistry, the average value being 50.3%. Thus, the patients were divided into two groups: the Ki-67 high expression group (>50.3%) (n = 78) and the Ki-67 low expression group (<50.3%) (n = 86).
The correlation between SUVmax and the clinical stage of gastric cancer
The SUVmax was 4.99 ± 2.01 in patients with stages I–II gastric cancer and 4.80 ± 1.98 in patients with stages III–IV gastric cancer. The difference between these two groups was not statistically significant (p > 0.05).
The correlation between SUVmax and the different degrees of differentiation
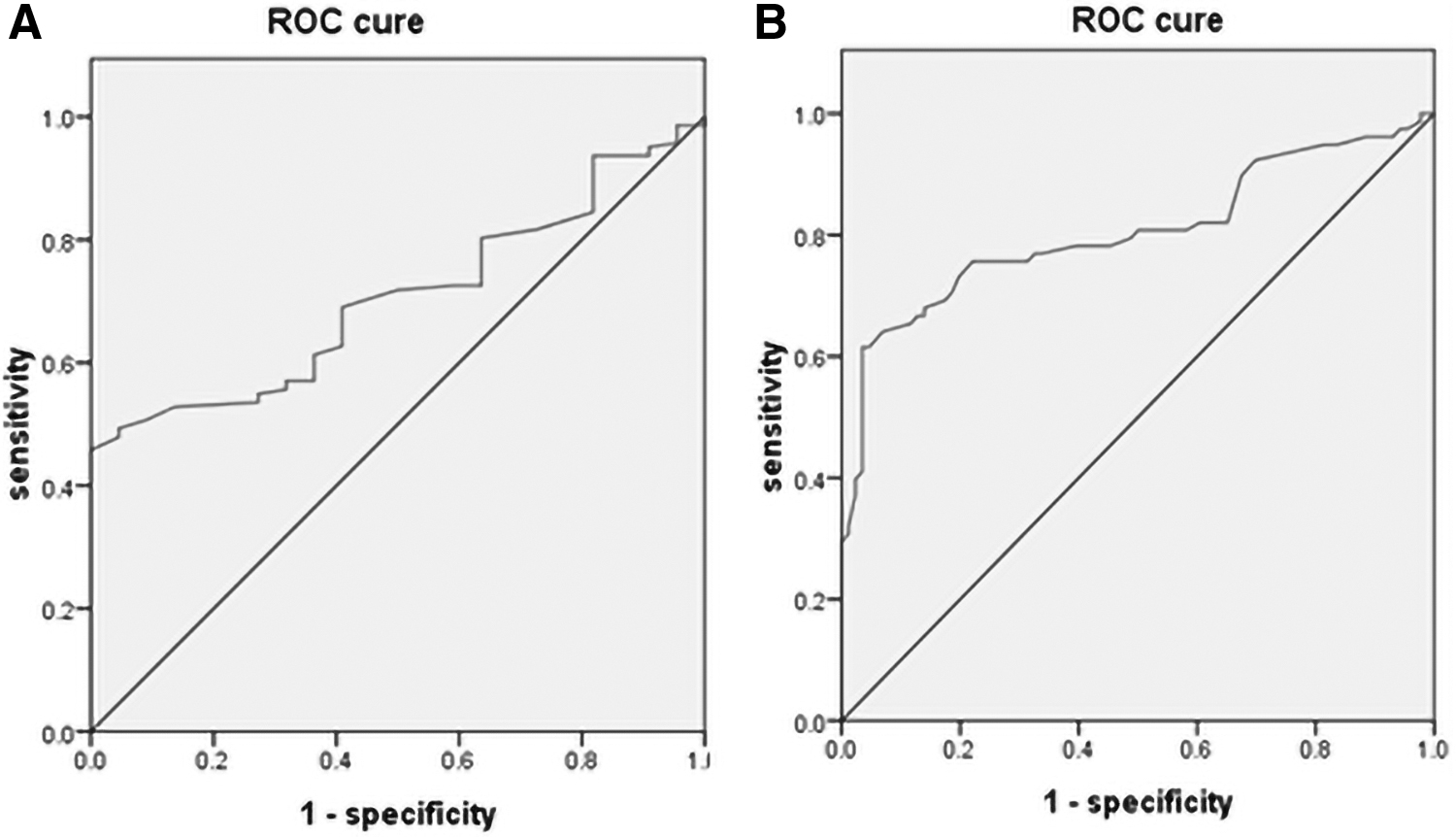
The SUVmax was 4.42 ± 1.58 in the moderately and highly differentiated adenocarcinoma group, 7.06 ± 1.22 in the poorly differentiated adenocarcinoma group, and 2.93 ± 0.83 in the signet-ring cell carcinoma group. The SUVmax of poorly differentiated adenocarcinoma was significantly higher than that of moderately and highly differentiated adenocarcinoma and signet-ring cell carcinoma (both p < 0.01), and the SUVmax of poorly differentiated adenocarcinoma was significantly higher than that of signet-ring cell carcinoma (p < 0.01, Fig. 1). The best critical value of SUVmax for predicting poorly differentiated and moderately and highly differentiated adenocarcinomas by ROC curve was 5.74 (Fig. 2A), and the area under the curve (AUC) was 0.907. When SUVmax was >5.74, the sensitivity of diagnosis of poorly differentiated adenocarcinoma was 89.6%, and the specificity was 77.8%. The best critical value of SUVmax for predicting highly differentiated adenocarcinomas and signet-ring cell carcinoma by ROC curve was 4.25 (Fig. 2B), and the AUC was 0.775. When SUVmax was >4.25, the sensitivity of diagnosis of signet-ring cell carcinoma was 53.1%, and the specificity was 88.6%.
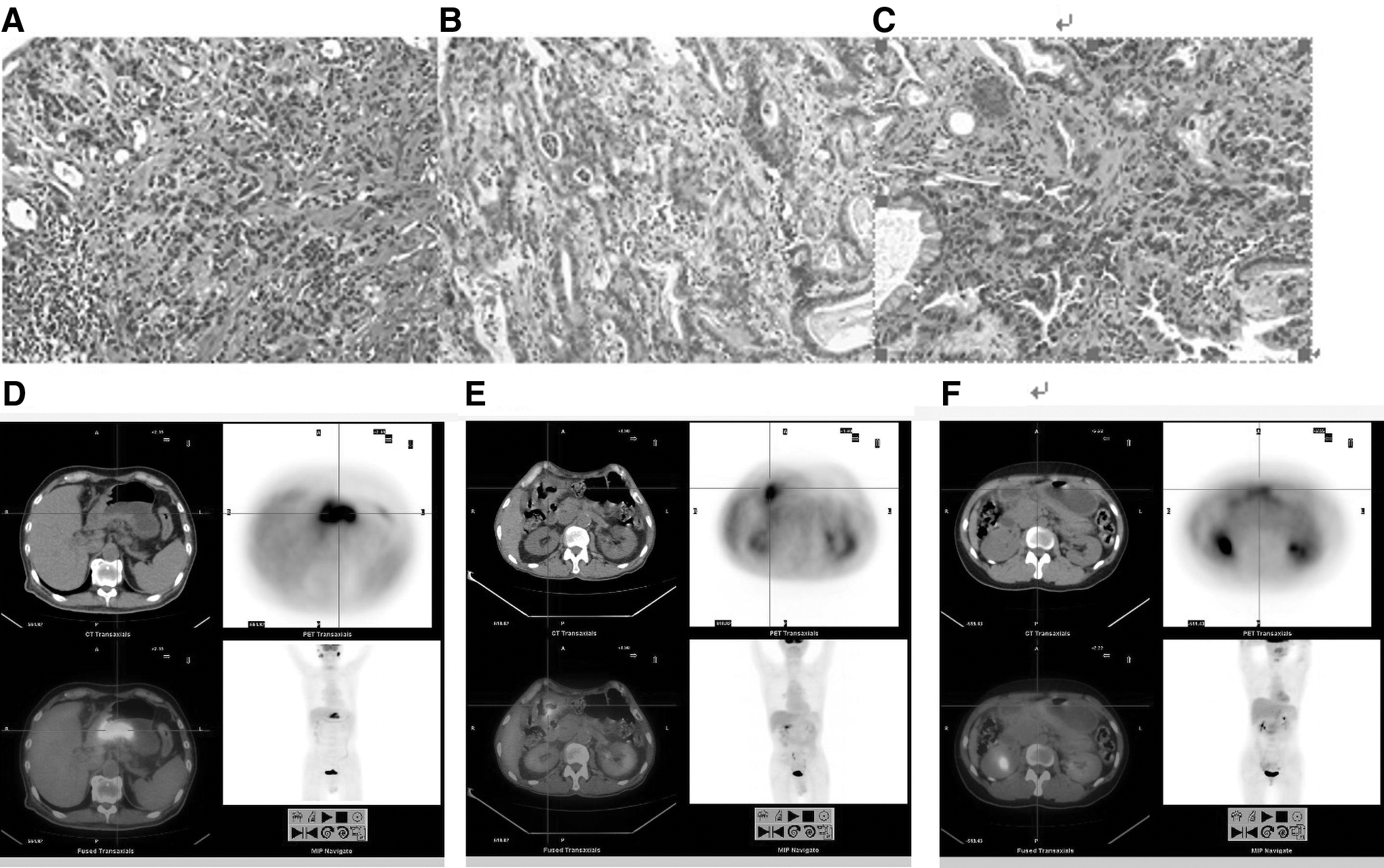
The correlation between the different pathological types of gastric cancer and SUVmax.

The correlation between SUVmax and the different degrees of differentiation.
The correlation between SUVmax and the HER-2 expression of gastric cancer
The SUVmax was 3.65 ± 1.17 in the HER-2 positive group and 5.07 ± 2.07 in HER-2 the negative group; the SUVmax was higher in the HER-2 negative group than in the HER-2 positive group (p < 0.01, Fig. 3). The best critical value of SUVmax for predicting the HER-2 status by ROC curve was 5.25 (Fig. 4A), and the AUC was 0.704. When SUVmax was >5.25, the sensitivity of the diagnosis of HER-2 negative was 49.3%, and the specificity was 95.5%.
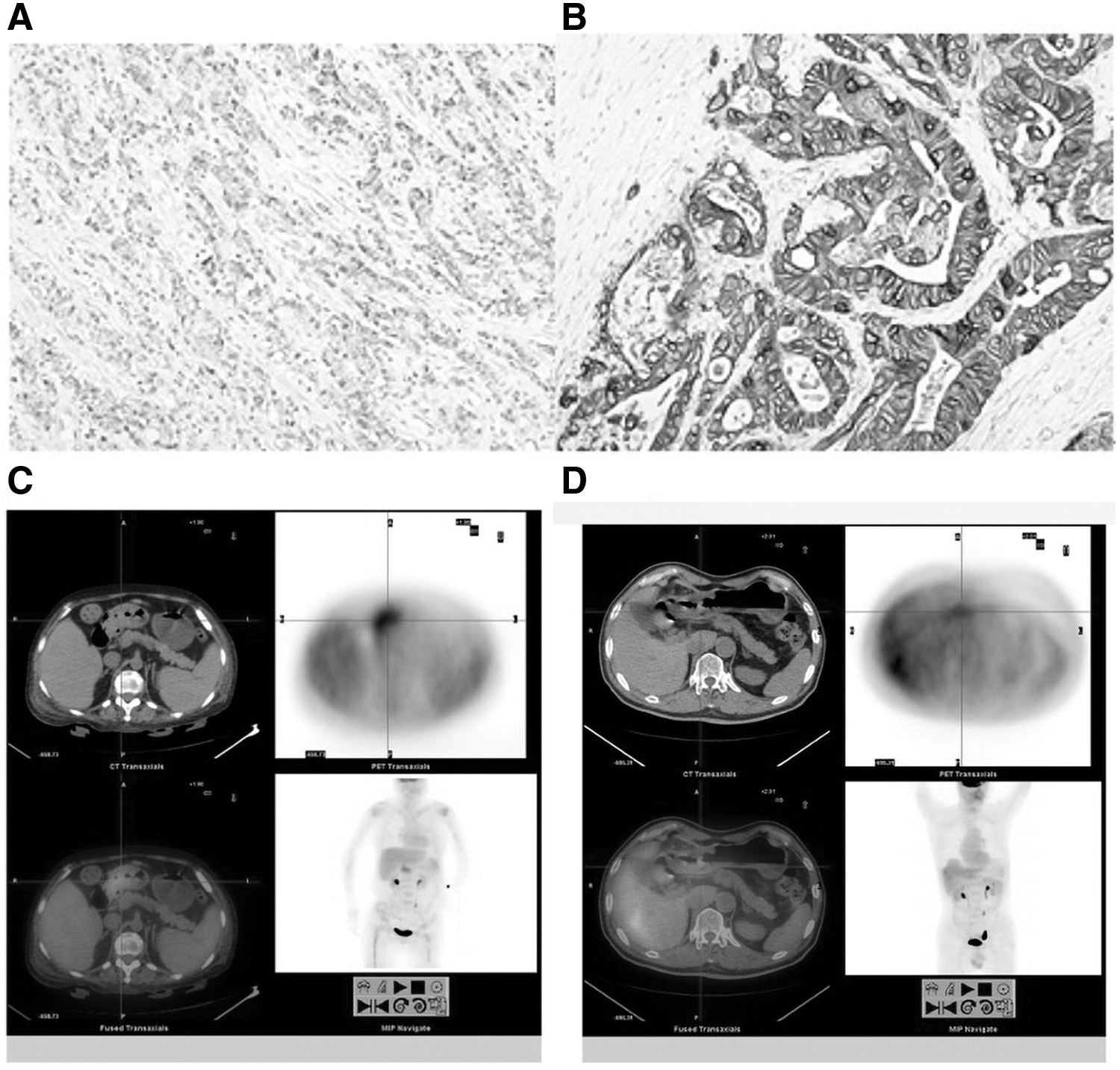
The correlation between the HER-2 status and SUVmax in gastric cancer immunohistochemistry.
The correlation between SUVmax with the HER-2 status and the Ki-67 expression level.
The correlation between SUVmax and the Ki-67 expression of gastric cancer
The SUVmax was 6.00 ± 2.04 in the Ki-67 high expression group and 3.85 ± 1.37 in the Ki-67 low expression group; the SUVmax was higher in the Ki-67 high expression group than in the Ki-67 low expression group (p < 0.01, Fig. 5). In these 164 patients, the total SUVmax was 4.88 ± 2.03, the value-added index of Ki-67 was 0.50 ± 0.15, and there was a significant positive correlation between these two groups (r = 0.70, p < 0.001). The best critical value of SUVmax for predicting Ki-67 status by ROC curve was 6.05 (Fig. 4B), and the AUC was 0.805. When SUVmax was >6.05, the sensitivity of diagnosis of Ki-67 high expression was 61.5%, and the specificity was 96.5%.

The correlation between the Ki-67 status and SUVmax in gastric cancer immunohistochemistry.
Discussion
The results of this study revealed that the difference in SUVmax between patients with stage I–II and stage III–IV gastric cancer was not statistically significant. The SUVmax of poorly differentiated adenocarcinoma was significantly higher than that of moderately and highly differentiated adenocarcinoma and signet-ring cell carcinoma. The best critical value of SUVmax for predicting poorly differentiated and moderately and highly differentiated adenocarcinomas by ROC curve was 5.74. The SUVmax in the highly differentiated adenocarcinoma group was higher than that in the signet-ring cell carcinoma group. The best critical value of SUVmax for predicting moderately and highly differentiated adenocarcinomas and signet-ring cell carcinoma by ROC curve was 4.25. The SUVmax in the HER-2 negative group was higher than that in the HER-2 positive group. The best critical value of SUVmax for predicting the HER-2 status by ROC curve was 5.25. The SUVmax was higher in the Ki-67 high expression group than in the Ki-67 low expression group. In these 164 patients, SUVmax was significantly positively correlated with the Ki-67 value-added index. The best critical value of SUVmax for predicting Ki-67 status by ROC curve was 6.05.
Gastric cancer is one of the most common malignant tumors worldwide, but most patients are in the advanced stages and experiencing complications with malignant proliferation by the time they are first diagnosed. Although surgery and chemotherapy can be effective in the treatment of gastric cancer, a previous study revealed that the median overall survival of patients with advanced gastric cancer was <12 months. 3 This is correlated to the low rate of early diagnosis, the lack of effective predictors of biological behavior, and the limited means of treatment for gastric cancer. At present, the selection of treatment depends on indexes such as clinical stage, pathological differentiation type, and HER-2 status. However, some indexes are not available for patients who cannot undergo a biopsy or who have too few biopsy specimens. Therefore, a noninvasive means of predicting the aforementioned indexes is urgently needed. SUV is the most commonly used semiquantitative index of 18 F-FDG PET/CT in the diagnosis and treatment of tumors, and SUVmax is the highest intake value in the region of interest in tumor lesions. At present, many studies have proved that SUVmax is associated with the prognosis, stage, and certain biological indexes of a number of tumors. 4 However, there are few studies on the correlation between SUVmax and the clinical features and biological indicators of gastric cancer in China.
Clinical stage is the most important index for devising treatments and making prognoses for cancer patients. Gastric cancers are divided into stages I–IV according to the size of the tumor, lymph node, and distant metastasis. At each stage, the treatment plans are different, and the 5-year survival rate can also differ widely. Previous studies have shown that SUVmax increases as the clinical stage of gastric cancer progresses from stage I to stage IV, there being a positive correlation between the two. 5,6 However, another study indicated that there was no correlation between SUVmax and the clinical stage of gastric cancer, 7 and this study also demonstrated that there was no difference in SUVmax between stage I–II and III–IV gastric cancer patients (p > 0.05). Therefore, it would appear that the value of SUVmax cannot be used to predict the clinical stage of gastric cancer.
Gastric cancers can be divided into four types in line with the degree of histological differentiation: highly differentiated, moderately differentiated, poorly differentiated, and undifferentiated (signet-ring cell carcinoma was undifferentiated). 8 Differentiation is closely correlated to the malignant degree of the gastric cancer. The malignant degree of poorly differentiated adenocarcinoma is higher than that of moderately and highly differentiated adenocarcinoma, whereas the malignant degree of signet-ring cell carcinoma is the highest. Differentiation needs to be fully considered in formulating treatment plans and making prognoses. Furthermore, SUVmax can reflect the malignant degree of tumors. At present, study results concerning whether there is any correlation between the two are not consistent. Chen et al. revealed that 7 the SUVmax of poorly differentiated adenocarcinoma was significantly higher than that of moderately and highly differentiated adenocarcinoma and signet-ring cell carcinoma, and the SUVmax in moderately and highly differentiated adenocarcinoma was higher than that in the signet-ring cell carcinoma. Kim et al. 9 also reported that the SUVmax of signet-ring cell carcinoma was lower than that of moderately and highly differentiated and poorly differentiated adenocarcinoma. It has also been shown in other research that the difference in SUVmax between groups of gastric cancer patients with different degrees of differentiation was not statistically significant. 10,11 The results of this study were that the SUVmax of poorly differentiated adenocarcinoma was significantly higher than that of moderately and highly differentiated adenocarcinoma, and signet-ring cell carcinoma (both p < 0.01), and SUVmax in moderately and highly differentiated adenocarcinoma group was higher than that in the signet-ring cell carcinoma group (p < 0.01). The reasons may be that the lower the degree of differentiation, the higher the malignant degree of the tumor, and the more active the proliferation is, the more active the glucose metabolism is and the higher the SUVmax, as it reflects the glucose metabolism. Signet-ring cell carcinoma has a relatively smaller number of cells, low density, and a scattered distribution; there is a lot of mucus in and outside the cells, and the expression of GLUT1 is very low.
In recent years, the rapid development of molecular targeted therapy has offered a new therapeutic strategy for advanced gastric cancer. Among many molecular targets for gastric cancer, HER 2 is one of the most widely used targets with the most definite clinical significance. Trastuzumab is the first globally approved humanized monoclonal antibody targeting HER2 overexpression. For HER-2 positive patients, chemotherapy combined with trastuzumab has become the standard treatment. Previous studies have revealed that HER-2 was positive in 7.3%–20.2% of patients with gastric cancer, 12 –14 and the positive rate of HER-2 in Chinese gastric cancer patients was 12%–13%. 15,16 A previous retrospective study revealed that the positive expression of HER-2 was correlated to older age, males, intestinal type of histological Lauren classification, and the tumor being in the upper third of the stomach. However, whether it is correlated to SUVmax, which can reflect the tumor's metabolic capacity, has not been confirmed. Previous studies also showed that 17 –19 the positive expression rate of HER-2 in moderately and highly differentiated adenocarcinoma was higher than that in poorly differentiated adenocarcinoma and signet-ring cell carcinoma, whereas the difference in the positive rate of HER-2 expression between poorly differentiated adenocarcinoma and signet-ring cell carcinoma was not statistically significant. Chen et al. revealed that 7 there was no significant correlation between SUVmax and HER2 expression in gastric cancer. However, when signet-ring cell carcinoma was excluded, the SUVmax was significantly higher in the HER-2 negative group than in the HER-2 positive group. The results of this study indicated that the SUVmax was significantly higher in the HER-2 negative group than in the HER-2 positive group (p < 0.01). The inconsistency in the research results to date suggests that the mechanism remains unclear and needs further study.
Ki-67 is a nuclear antigen found in proliferating cells, expressed in the G1, S, G2, and M phases of the cell cycle. The expression level is highest in the M phase, but not expressed in the G0 phase. The Ki-67 index reflects the proportion of cells entering the proliferative cycle and, to some extent, the proliferative activity of tumor cells. A study concerning breast cancer reported that 20 SUVmax was moderately correlated with the Ki-67 expression but could not yet be used as a surrogate marker for tumor proliferation. The results of a study into ovarian cancer had similar results to those of breast cancer. 21 A meta-analysis involving 5600 patients with gastric cancer in 29 studies suggested that 22 a high expression of Ki-67 was significantly associated with Lauren's typing and tumor size but not correlated with lymph node metastasis, tumor stage, and tumor differentiation. However, there are few studies on whether there is a correlation between SUVmax and the Ki-67 index. Deng et al. found that 23 in gastric cancer, SUVmax was weakly correlated with the Ki-67 index. The results of this study revealed that SUVmax was significantly higher in the Ki-67 high expression group than in the Ki-67 low expression group (p < 0.01), and there was a significant positive correlation between these two groups (r = 0.70). In principle, both expressions can reflect the degree of proliferation of tumor cells, and a positive correlation can be seen.
This study has the following limitations. First, it is a case–control study, not a randomized controlled trial, and it is not blind. Therefore, there is still a certain risk of bias. Second, this study is a single-center clinical trial; the included sample size is small, and multicenter clinical trials with larger sample sizes are still needed. Finally, the correlation between PET/CT SUVmax, the status of HER-2, and the Ki-67 index in gastric cancer patients still require further study.
Conclusion
18 F-FDG PET/CT SUVmax can, to some extent, predict the degree of pathological type, HER-2 status, and Ki-67 index of gastric cancer patients, and so it can be used as a noninvasive predictor of the biological behavior of patients with gastric cancer, thereby, contributing to clinical diagnosis and treatment.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The study is funded by Provincial Natural Science Foundation of Gansu (17JR5RA037) and Science Foundation of Gansu Provincial Hospital (16GSSY2-7).