
Abstract
Purpose:
Painful metastatic bone involvement is common in advanced stages of many cancers. Between available radionuclides for bone pain palliation, no consensus has been reached on lutetium ethylenediaminetetramethylene phosphonate (177Lu-EDTMP) administration in this milieu. The aim of this study is to evaluate the treatment efficacy, safety profile, and toxicities of 177Lu-EDTMP in patients with metastatic bone involvement, according to the published literature.
Methods:
A comprehensive literature search of PubMed/MEDLINE, Scopus, and Google Scholar databases was carried out to retrieve pertinent articles published until January 2019, concerning the clinical efficacy and safety of 177Lu-EDTMP for bone pain palliative purposes.
Results:
Eight studies (172 patients) were included. This analysis revealed statistically significant effect of 177Lu-EDTMP therapy on the visual analog score (4.84% (95% CI: 3.88–5.81; p < 0.001), bone palliative pain response (84%, 95% CI: 75%–90%; p < 0.001), and Karnofsky performance status (21%, 95% CI: 18%–24%; p < 0.001) overall (as well as in the high-dose and low-dose subgroups). Complete palliative pain response to treatment was observed in 32% (95% CI: 16%–53%) of patients receiving 177Lu-EDTMP. Anemia was found to be the most common hematologic toxicity imposed by this therapeutic approach (grade I/II anemia in 24% (95% CI: 14%–38%; p < 0.001) and grade III/IV anemia in 19% (95% CI: 12%–28%; p < 0.001)).
Conclusions:
177Lu-EDTMP seems to have comparable efficacy and safety profile as that of the frequently administered radiopharmaceuticals for bone palliation. Therefore, this agent can be a good option for bone pain palliative purposes, in case of limited access to other bone palliative radiopharmaceuticals.
Introduction
Skeletal metastases are considered a major cause of morbidity and mortality in 65%–75% of patients with advanced stages of breast and prostate cancer, as well as in 15%–30% cases of lung, colon, stomach, bladder, uterus, rectum, thyroid, and kidney malignancies, deteriorating quality of life in all these groups of patients. 1,2
Alleviation of painful bone metastasis as a major concern, commonly endured by patients with advanced metastatic bone involvement, remains a major therapeutic challenge and is found to be essential so as to improve patients' quality of life. Therefore, many therapeutic options, aiming to improve quality of life of patients with metastatic bone involvement through pain reduction and prevention of further complications and morbidities, have been the focus of research interest. 1,2
Currently available palliative strategies include the administration of conventional analgesics, bisphosphonates, chemotherapy, external beam radiotherapy, and radionuclide therapy, showing variable degrees of success for bone pain palliation. Among them, radionuclide bone pain palliation is of particular interest due to its low level of adverse reactions, while imposing systemic effects. 3 –5
Various bone-seeking radiopharmaceuticals with decades of experience are available for bone pain palliation. β−-emitting radionuclides, to be named, samarium-153 (153Sm) lexidronam (153Sm-EDTMP), phosphorus-32 ( 32 P) sodium orthophosphate, rhenium-186-hydroxyethylidene diphosphonate (186Re-HEDP), rhenium-188-hydroxyethylidene diphosphonate (188Re-HEDP), and strontium-89 chloride (89SrCl2) have revealed various promising results in the field of metastatic bone pain palliation (3). In addition, particular attention has been placed on the α-emitting agent, radium-223 (223Ra), showing satisfactory outcome and survival benefits (for 2.8 months) in patients with metastatic castration-resistant prostate cancer. 6
Lutetium ethylenediaminetetramethylene phosphonate (177Lu-EDTMP) is another radiopharmaceutical suggested for systemic radionuclide therapy in patients with metastatic bone involvement, mostly investigated in patients with breast or prostate cancers, but not yet approved by the Food and Drug Administration (FDA). With favorable β and γ characteristics, 177Lu-EDTMP seems to be an interesting radiotracer among bone-seeking radiopharmaceuticals. Favorable synthesis process, which is affordable by the use of medium-efflux reactors, as well as the long physical half-life (6.73 d) of 177Lu, which may result in the improvement of treatment efficiency and facilitation of the radiopharmaceutical transportation conditions, altogether propose 177Lu-EDTMP as a good candidate for bone palliation purposes. 7
Considering the abovementioned suitable features of 177Lu-EDTMP and the fact that this agent has not been mentioned in the latest guideline published by the European Association of Nuclear Medicine (EANM) on radionuclide therapy of bone metastases with β−-emitters, 8 possibly due to scarcity of the data regarding the efficacy and safety of 177Lu-EDTMP, the authors aimed to perform a systematic review and meta-analysis of all available records to assess the efficacy and safety of 177Lu-EDTMP in metastatic bone pain palliation.
Methods
Search strategy and study selection
A search algorithm based on various writing styles of the term “177Lu-EDTMP” was applied for the comprehensive literature search of PubMed/MEDLINE, Scopus, and Google Scholar databases, so as to retrieve pertinent published articles concerning the efficacy and safety of 177Lu-EDTMP in patients with metastatic bone involvement. References of relevant articles were hand searched as well. The search was carried out from inception to January 2019 with no language restriction.
All studies were considered eligible provided that all the following criteria were fulfilled: (a) clinical studies performed on patients diagnosed with cancer (excluding case reports), (b) 177Lu-EDTMP used for bone palliation, and (c) toxicity profile and bone palliation efficacy assessed in the study. Two researchers (E.A. and G.D.) independently evaluated titles and abstracts of the retrieved articles, applied the inclusion criteria mentioned earlier, and eventually appraised the full-text version of the recruited articles to establish their eligibility to be included in the meta-analysis. Discrepancies between the reviewers were resolved through discussions and consensus.
Data extraction and quality assessment
Two independent reviewers (E.A. and S.H.) extracted the following study details from the full-text articles: first author, year of publication, study design, patient characteristics (sex and type of malignancy), interventions (sample size, dose, and frequency), and results (patient-rated visual analog score [VAS]), serving as the basis for pain documentation (the scale according to which pain was rated as zero when the patient experienced no pain and 10 represented intolerable pain), 9 the Karnofsky performance score (KPS), 10 used to assess the quality of life, and hematologic toxicity, evaluated by assessment of hemoglobin levels and platelet and leukocyte counts, and graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 3.0. or 4.0. The authors of eligible investigations were contacted if there was suspicion of duplicate datasets. Only studies providing such data were finally included in the meta-analysis.
The available studies investigating the use of 177Lu-EDTMP for the palliation of metastatic bone pain were quite heterogeneous; therefore, formal quality assessment of the eligible trials was not undertaken, but the inclusion criteria were set so as to circumvent the inclusion of small trials (less than 10 patients), or trials without a well-defined endpoint (objective pain or measure of analgesic consumption or quality-of-life scale).
Statistical analysis
Random-effects model was applied to pool VASs, the frequencies of overall palliative pain response to treatment, the frequencies of complete palliative pain response to treatment, KPSs, the frequencies of anemia, thrombocytopenia, and leukopenia, and calculate their 95% CI. In addition, the same method was used to compare the effect of 177Lu-EDTMP and 153Sm-EDTMP on VAS, with the intent to establish the extent of the pain palliation effect of these radiopharmaceuticals. The I2 statistic was used to assess the heterogeneity among studies, representing the percentage of total variation contributed by a between-study variation, ranging from 0% to 100%. 11 Funnel plots and Egger's regression intercept were used to evaluate the publication bias. 12 All statistical analyses were carried out by using Comprehensive Meta-analysis (version 2; Biostat, Inc.) software. The final results were depicted as forest plots.
Results
From 250 records retrieved through either bibliographic or hand searching, eight studies (172 patients) were finally included in this study (Fig. 1). 7,13 –19 The majority of cases were diagnosed with either breast or prostate cancer and treated with a single dose of 177Lu-EDTMP (ranging from 692 to 5550 MBq). No additional studies were recruited after screening the references. Basic study characteristics and safety aspects of the eight included studies are depicted in Tables 1 and 2.
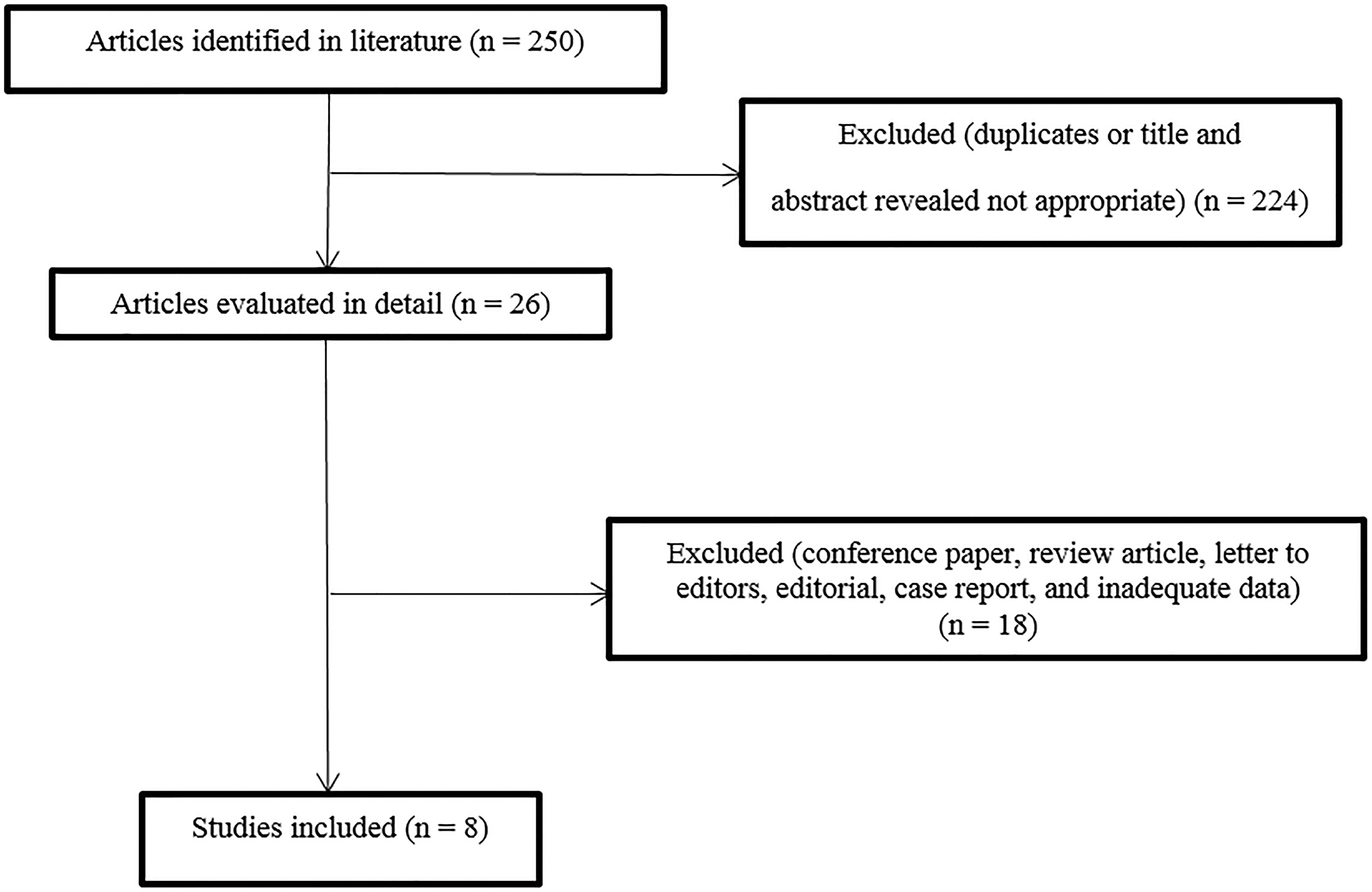
Flow diagram of studies incorporated in this meta-analysis.
Efficacy Estimates of Studies on 177Lu-EDTMP Included in This Meta-Analysis
Complete response (CR) defined as disappearance of all bone pain, freely mobile, and at least a 50% decreased use of pain medication; partial response (PR) defined as some improvement in bone pain.
CR defined as >70% decrease in VAS and PR defined as 40%–70% decrease in VAS, minimal response (MR) 20%–40% decrease in VAS.
CR defined as either pain score of 0 at 3 month or >75% decrease in analgesic score with change in pain score, PR defined as either change in pain score by >3 or 50%–75% decrease in analgesic score with change in pain score, and MR defined as either change in pain score by 1–3 or 25%–50% decrease in analgesic score with change in pain score.
Baseline and 12 weeks after therapy ECOG were 2.5 ± 1.3 and 1.6 ± 0.6, respectively. No difference is noted in the ECOG between 153Sm-EDTMP and 177Lu-EDTMP group.
CRPC, castration-resistant prostate cancer; ECOG, Eastern cooperative oncology group; HDG, high-dose group; LDG, low-dose group; CRR, complete response rate; PRR, partial response rate; MRR, minimal response rate; ORR, overall response rate; VAS, visual analog score; MTC, medullary thyroid carcinoma; NSCLC, non-small cell lung cancer; RCC, renal cell carcinoma; NET, neuroendocrine tumor.
Hematologic Toxicities Reported by Studies Included in This Meta-Analysis
HDG, high-dose group; LDG, low-dose group.
Among the eligible articles, six studies (10, 11, 13, 14, and 16) indicated significant pain palliation after reception of the 177Lu-EDTMP therapy 7,13,14,17 –19 and four reported a significant increase in performance status, assessed by KPS. 13,16,18,19 One study assessed the functional performance by Eastern Cooperative Oncology Group (ECOG), which showed considerable improvement after treatment with 177Lu-EDTMP (level of significance was not reported). 17 Two of the eligible studies divided their cases to two groups and allocated them two different doses of the radionuclide, while others used fixed doses of the radionuclide. 13,19 Four studies have been found to administer high dosages of 177Lu-EDTMP (defined as dosages greater than 1850 MBq), 13,16,18,19 two administered low dosages of the same radiotracer (defined as dosages less than 1850 MBq), 13,19 and three could not be indicated clearly as either the high-dose or low-dose groups (designated as the mixed-dose group). 7,15,17 Control groups in which 153Sm-SDTMP was administered as the mainstay of treatment were presented in two studies. 7,17,18 Major hematologic toxicity was assessed in six investigations and reported ranging from 0% to 24% among studies. 13 –16,18,19 The other two studies compared the baseline hematologic parameters to the follow-up ones, while stating the general rate of hematotoxicity. 7,17 The studies included were mostly single center and retrospective, not showing high levels of evidence. Data regarding the heterogeneity and the publication bias of the included studies are depicted in Table 3 and Supplementary Figure S1. Details for pooled estimates of VAS, overall response, complete response, KPS, and hematologic adverse events are available in Supplementary Figs. S2–S11)
Summary of Pooled Estimates for Different Variables Assessed in This Meta-Analysis
Assessed by Begg's funnel plot and Egger's test (For more detailed information, refer to the supplemental digital content).
Assessed by mean differences.
ΔVAS, decrease in the visual analog score after treatment with 177Lu-EDTMP compared to the initial scales; ΔKPS, increase in the Karnofsky performance status after treatment with 177Lu-EDTMP; G, Grade; NA, not available for analysis.
Visual analysis score
The meta-analysis depicted significant effect of the 177Lu-EDTMP therapy on the VAS (mean difference [MD]: −4.84, 95% CI: −5.81 to −3.88, p < 0.001). Stratification by the dosage of the radiotracer received indicated statistically significant effect of this mode of therapy on patients' VAS in both the high-dose and low-dose categories (MD: −5.29, 95% CI: −6.89 to −3.70, p < 0.001, and MD: −4.07, 95% CI: −6.31 to −1.83, p < 0.001, respectively).
Overall palliative pain response to treatment
A summary of meta-analysis results concerning frequencies of the overall palliative pain response to 177Lu-EDTMP treatment is demonstrated in Table 3. The meta-analysis revealed significant effect of this mode of treatment on the frequencies of summed overall palliative pain response, as well as in the high-dose and low-dose categories (frequency: 84%, 95% CI: 0.75–0.90, p < 0.001; frequency: 85%, 95% CI: 0.74–0.92, p < 0.001; and frequency: 81%, 95% CI: 0.62–0.91, p = 0.003, respectively).
Complete palliative pain response to treatment
The meta-analysis did not show any significant effect of the 177Lu-EDTMP therapy on the frequency of complete palliative pain response to treatment, with no consideration for the dosage of radiopharmaceutical administered. However, stratification by the dosage indicated the effect of 177Lu-EDTMP therapy on the complete palliative pain response to treatment in patients receiving low dosages of 177Lu-EDTMP (frequency: 13%, 95% CI: 0.04–0.37, p = 0.007), but not the high-dose group.
Karnofsky performance status
Meta-analysis results concerning the effect of treatment with 177Lu-EDTMP on KPS revealed statistically significant results in all the overall, high-dose, and low-dose groups (MD: 21%, 95% CI: 18–24, p < 0.001; MD: 21%, 95% CI: 17–26, p < 0.001; and MD: 20%, 95% CI: 14–27, p < 0.001, respectively).
Anemia
For grade I/II anemia (grade I and II), meta-analyses findings are shown in Table 3. Meta-analysis of the grade I/II anemia revealed significant effect of 177Lu-EDTMP therapy on the frequency of such entities in the overall and high-dose groups (frequency: 24%, 95% CI: 0.14–0.38, p = 0.001, and frequency: 20%, 95% CI: 0.07–0.44, p = 0.02, respectively), but not in the low-dose or mixed-dose categories. On the other hand, meta-analyses of the grade III/IV anemia (grade III and IV) divulged significant effect of 177Lu-EDTMP therapy on the frequency of these grades of anemia in the overall, high-dose, and low-dose groups (frequency: 18%, 95% CI: 0.12–0.27, p < 0.001, frequency: 13%, 95% CI: 0.06–0.25, p < 0.001, and frequency: 22%, 95% CI: 0.09–0.43, p = 0.012, respectively).
Leukopenia
Leukopenia grade I and II were shown to be affected by the 177Lu-EDTMP therapy, when analyzed overall (frequency: 26%, 95% CI: 0.12–0.47, p = 0.027), but not in the subgroups divided according to the dosage of the radiopharmaceutical received. However, leukopenia grade III and IV occurred as a consequence of the 177Lu-EDTMP therapy in the overall, high-dose, low-dose, and mixed-dose groups (frequency: 40%, 95% CI: 0.01–0.09, p < 0.001, frequency: 40%, 95% CI: 0.01–0.12, p < 0.001, frequency: 30%, 95% CI: 0.00–0.18, p = 0.001, and frequency: 4%, 95% CI: 0.01–0.27, p = 0.004, respectively).
Thrombocytopenia
Meta-analyses found the effect of the 177Lu-EDTMP therapy on thrombocytopenia grade I and II in the overall group (frequency: 21%, 95% CI: 0.08–0.43, p = 0.013); nonetheless, such association was not detected in subgroup analysis. For grade III/IV thrombocytopenia (grade III and IV), meta-analyses findings proved the occurrence of such hematologic toxicities in all the overall, high-dose, low-dose, and mixed-dose patients' categories treated with 177Lu-EDTMP (frequency: 40%, 95% CI: 0.01–0.09, p < 0.001, frequency: 3%, 95% CI: 0.01–0.11, p < 0.001, frequency: 6%, 95% CI: 0.02–0.22, p < 0.001, and frequency: 2%, 95% CI: 0.00–0.27, p = 0.009, respectively).
Discussion
To reach consolidated data and provide the best available evidence required for decision making, herein, the authors conducted a systematic review and meta-analysis to evaluate the efficacy and adverse effects of 177Lu-EDTMP administration in patients with metastatic bone pain. This analysis revealed significant effect of 177Lu-EDTMP therapy on the VAS, overall palliative pain response to treatment, and KPS in the overall, high-dose, and low-dose groups, and complete palliative pain response to treatment in patients receiving low dosages of 177Lu-EDTMP. On the other hand, this therapeutic approach was found to impose certain hematologic toxicities, including grade I/II anemia in the overall and high-dose groups, grade III/IV anemia in the overall, high-dose, and low-dose groups, both the grade I/II leukopenia and thrombocytopenia in the overall group, and grade III/IV leukopenia and thrombocytopenia in the overall group together with all subgroups. Compared to the low dosages of 177Lu-EDTMP, high-dose 177Lu-EDTMP seems to be more effective, while does not pose patients to more serious adverse events; however, this finding should be further evaluated in future studies.
153Sm–EDTMP, a well-known radiopharmaceutical for bone pain palliation, has been widely used since FDA approval in different osteoblastic metastatic lesions, predominantly in prostate and breast cancer, with a well-established standard dose of 37 MBq/kg. 8,20 –22 A palliative pain response rate of 40%–97% with a mean of 70%, a decrease in analgesic consumption. and improved quality of life have been reported in numerous affirmative studies of this radiopharmaceutical. 23 –29 The pain reduction occurs as early as in the first week and lasts for ∼2–3 months after administration. 24,25,27,30 The bone marrow toxicity is usually mild with the lowest platelet and white blood cell counts in 3–5 weeks, resolving in 6–8 weeks after therapy, 24,25,27,28,31 although severe grades of myelotoxicity might be observed in patients with predisposing underlying conditions. including recent chemotherapy, external beam radiation therapy, or malignant bone marrow involvement. 32 The administration of repeated doses of 153Sm-EDTMP can also result in mainly minimal and transient bone marrow toxicity. 33,34 Studies comparing the effect of 177Lu-EDTMP to 153Sm-EDTMP have revealed that they both subject bone metastases to similar radiation doses and lead to the similar pain palliative response rate of ∼75%–80%. 7,18,35 Moreover, the cocktail therapy of 177Lu-/153Sm-EDTMP has depicted safety in administration and pain relief/reduction in 24 out of 25 patients. 36 Given the similar pain response efficacy of 177Lu-EDTMP to that of 153Sm-EDTMP, together with minimal side effects and improved quality of life following the administration of 177Lu-EDTMP, it has been suggested as a feasible and safe alternative to 153Sm-EDTMP for treatment of painful skeletal metastases. Especially, in centers having no nearby access to 153Sm-EDTMP, 177Lu-EDTMP with its longer half-life could stand as a promising alternative. 7,17,18 Furthermore, 177Lu-EDTMP offers a better possibility of post-treatment imaging. Although this option is unlikely to affect the overall outcome of the treatment, it may be an interesting subject for further quantitative studies.
Beta-emitting bone-seeking radiopharmaceuticals have been used for bone pain palliation for decades, demonstrating acceptable results. Meanwhile, the introduction of α-emitting tracers, with 223RaCl2 at the top, with its promising results in terms of patients' survival cast a shadow over other radiopharmaceuticals. Alpha-emitting radiopharmaceuticals dispense higher linear energy in a shorter range of below 100 μm and mainly induce permanent DNA double-strand breaks, and thus provide a greater degree of toxicity for tumoral cells and less radiation for surrounding normal tissues. 37 –39 Considering the markedly shorter range of 223Ra in tissues, hematological toxicity is anticipated to be less compared to β−-emitting radiopharmaceuticals 40 ; however, mild and reversible myelosuppression can occur with a nadir in 2–4 weeks following their administration resolving in 6 weeks. 41 On the other hand, the palliative pain response rate of 50%–60%, reported for the α-emitter, 223RaCl2, is not beyond the reported range for β−-emitters. 42 The impact of 223RaCl2 on extending survival parameters makes it an appealing agent to be employed 38 ; however, the expensive [223Ra]radium is not globally available. Given the established use of [177Lu]lutetium in radionuclide therapy for neuroendocrine tumors and prostate cancers, it may be more available. In addition, some other characteristics of this relatively inexpensive radioisotope, [177Lu]lutetium, including its favorable half-life, production in high specific activity, efficient therapeutic β−-particles, long effect with a single administration, and sufficient γ-photons for imaging, make it an attractive option in bone pain palliation therapy. 14,43 –45
The comprehensive literature search, and reviewing and appraising the evidence in duplicate so as to protect the study from bias, could be counted as the strengths of this review. However, to put the study within the proper context, important limitations should be acknowledged. First, variable and not always optimum quality of the RCTs included, threatens the interpretability of the authors' findings. Second, substantial heterogeneity across the studies in pooled outcome estimates, despite all their measures taken to account for the heterogeneity across the studies and for the difference within the studies, limits their confidence in the reported estimates. The small number of patients enrolled in some of the included studies stands as the other limitation to be mentioned, making the authors' findings to be interpreted with caution. In addition, the limited number of studies assessing the efficacy and safety of 177Lu-EDTMP for metastatic bone pain palliation could be mentioned as a limitation, signifying the necessity of further studies. Publication bias is the other constraining factor to be notified.
To sum up, considering the imaging possibilities together with the results of this study, systemic administration of 177Lu-EDTMP is an effective, safe, well-tolerated, and feasible alternative treatment option for metastatic bone pain palliation in patients with disseminated skeletal metastases. This agent could stand out among other radiopharmaceuticals used for palliative therapy of metastatic bone pain. However, larger multicenter studies are required to define the exact order of 177Lu-EDTMP among different palliative modalities.
Footnotes
Ethical Approval
This article does not contain any study with human participants or animals performed by any of the authors.
Disclosure Statement
The authors declare that they have no financial or nonfinancial competing interests.
Funding Information
No funding was received.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9
Supplementary Figure S10
Supplementary Figure S11
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.