
Abstract
Background:
The retrospective studies that have so far described the outcomes of the sequential use of life-prolonging agents (LPAs) did not include metastatic castration-resistant prostate cancer (mCRPC) patients who received radium-223 (223Ra) as part of their treatment. Consequently, it is not known whether including 223Ra in the therapeutic sequence has an impact on cumulative survival. The aim of this study was to evaluate this impact by comparing the cumulative overall survival (OS) in two series of mCRPC patients sequentially treated with two or three LPAs after first-line docetaxel (DOC), including 223Ra and not.
Materials and Methods:
The authors retrospectively reviewed the records of mCRPC patients with bone involvement alone who received two or three LPAs (including 223Ra) after first-line DOC. The control group was a contemporary series of mCRPC patients with bone involvement alone treated with sequences of two or three LPAs other than 223Ra after first-line DOC.
Results:
Median cumulative OS was 40.6 months in the 223Ra group of 78 patients and 36.2 months in the non-223Ra group of 186 patients (p = 0.08). OS outcomes were significantly influenced by the number of treatment lines, and baseline Eastern Cooperative Oncology Group performance status (PS) and prostate-specific antigen levels.
Conclusions:
To the best of the authors' knowledge, this is the first study designed to evaluate the impact of introducing 223Ra in the treatment sequences for mCRPC patients, and the results show that its use does not negatively affect cumulative OS.
Introduction
Over the last 20 years, the therapeutic landscape of metastatic castration-resistant prostate cancer (mCRPC) has been changed by the availability of a number of life-prolonging agents (LPAs) that have significantly improved overall survival (OS): two chemotherapeutic agents, docetaxel (DOC) 1 and cabazitaxel (CABA) 2 ; two new androgen-receptor targeting agents (ARTAs), abiraterone acetate (AA) and enzalutamide (ENZ) 3 –6 ; and α-emitting radium 223 (223Ra). 7 However, although their sequential use greatly improves the life expectancy of mCRPC patients, 8 –10 the optimal therapeutic sequences are still unclear.
Although a number of retrospective studies have described the outcomes of the sequential use of LPAs, 11 none of them included mCRPC patients who received 223Ra as part of their treatment. Therefore, it is not known whether including the use of 223Ra in the therapeutic sequence has an impact on cumulative survival.
The aim of this study was to explore this impact by comparing cumulative OS in two cohorts of mCRPC patients who sequentially received two or three LPAs after DOC first-line, including 223Ra or not.
Patients and Methods
After the approval of Institutional Review Boards, the authors retrospectively reviewed the records of mCRPC patients who received two or three LPAs (including 223Ra) after first-line DOC sequentially administered in any order in everyday clinical practice; all of the patients had bone disease alone at the time they received 223Ra. The control group was a recently described contemporary series of mCRPC patients treated with sequences of two or three LPAs other than 223Ra after first-line DOC. 12 In an attempt to make the two groups comparable and avoid potential biases, patients with visceral and/or nodal involvement were excluded from the control group.
All of the LPAs were administered at standard doses: up to a maximum of 8–10 intravenous (i.v.) courses of DOC 75 mg/m2 every 3 weeks plus prednisone 10 mg/day in the absence of progression or unacceptable toxicity; CABA 25 mg/m2 i.v. every 3 weeks plus prednisone 10 mg/day until progression; oral AA 1000 mg once daily plus prednisone 10 mg/day until progression; oral ENZ 160 mg once daily until progression; and up to a maximum of six i.v. courses of 223Ra 55 kBq per kilogram of body weight every 4 weeks in the absence of progression or unacceptable toxicity. During treatment, radiographic evaluations and measurements of prostate-specific antigen (PSA) levels were made in accordance with the policy of the individual centers.
Statistical analyses
The authors recorded the patients' demographic data, their medical histories before the development of mCRPC, and their baseline characteristics at the time of starting first-line DOC treatment. They also recorded the type of treatment and its start and end dates for each treatment line. Continuous variables are expressed as median values, and discrete variables as relative frequencies.
The OS of each patient (the primary outcome measure) was calculated from the date of starting first-line treatment to the date of death due to any cause, or was censored on the last date the patient was known to be alive.
The 223Ra-treated and untreated patients and their disease characteristics were compared using the chi-squared test for categorical variables and analysis of variance for continuous variables. The log-rank test was used to compare OS outcomes, and univariate and Cox regression analyses were used to assess the prognostic value of a series of covariates in terms of OS.
The statistical analyses were made using IBM SPSS Statistics software, v. 21.0.
Results
The group of patients who sequentially received two or three LPAs including 223Ra after first-line DOC treatment (the 223Ra group) consisted of a consecutive series of 78 mCRPC patients treated at 12 Italian hospitals between June 2007 and November 2017.
It is worth noting that none of these patient received 223Ra concurrently with abiraterone or enzalutamide.
The control group (the non-223Ra group) consisted of 186 patients treated at 36 Italian hospitals between January 2008 and November 2016. Table 1 shows that the patients' characteristics at the time of the start of sequential treatment were not significantly different, except for the fact that PSA levels were higher in the control group. Thirty-nine patients in the 223Ra group (50%) and 70 (37.6%) in the non-223Ra group received four treatment lines (p = 0.07). In the 223Ra group, 7 patients (9%) received 223Ra in second line, 42 (53.8%) in third line, and 29 (37.2%) in fourth line. Forty-five patients (58.3%) received five or six 223Ra courses. The agents used in the sequences are summarized in the Table 2.
Patient Characteristics at the Start of Sequences Including and Not Including 223Ra
ECOG, Eastern Cooperative Oncology Group; PSA, prostate-specific antigen.
Agents Used in Therapeutic Sequences
After a median follow-up of 35 months (range 9.4–99.2), 185 patients had died (47 in the 223Ra group and 138 in the non-223Ra group). Median cumulative OS from the start of first-line treatment in the population as a whole was 37.8 months: OS was 40.6 months in the 223Ra group and 36.2 months in the non-223Ra group (p = 0.08) (Fig. 1). Considering the study population as a whole (regardless of 223Ra treatment), there was a statistically significant difference in median OS depending on the number of administered treatment lines: it was 34.6 months among the patients who had received three lines and 48.5 months among those who had received four lines (p < 0.0001). No statistically significant differences were observed among the various specific treatment sequences. Median OS from the time of starting first-line treatment was significantly longer in the patients with a baseline Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0–1 than in those with a worse PS (39.0 months vs. 35.3 months; p < 0.0001), and significantly longer in the patients whose baseline PSA levels were ≤69.3 ng/mL than in those with higher levels (40.8 months vs. 31.0 months; p < 0.002). The number of treatment lines, baseline ECOG PS, and PSA levels were significant at univariate and multivariate analysis, whereas the use of 223Ra in the sequence was not significant (Table 3).
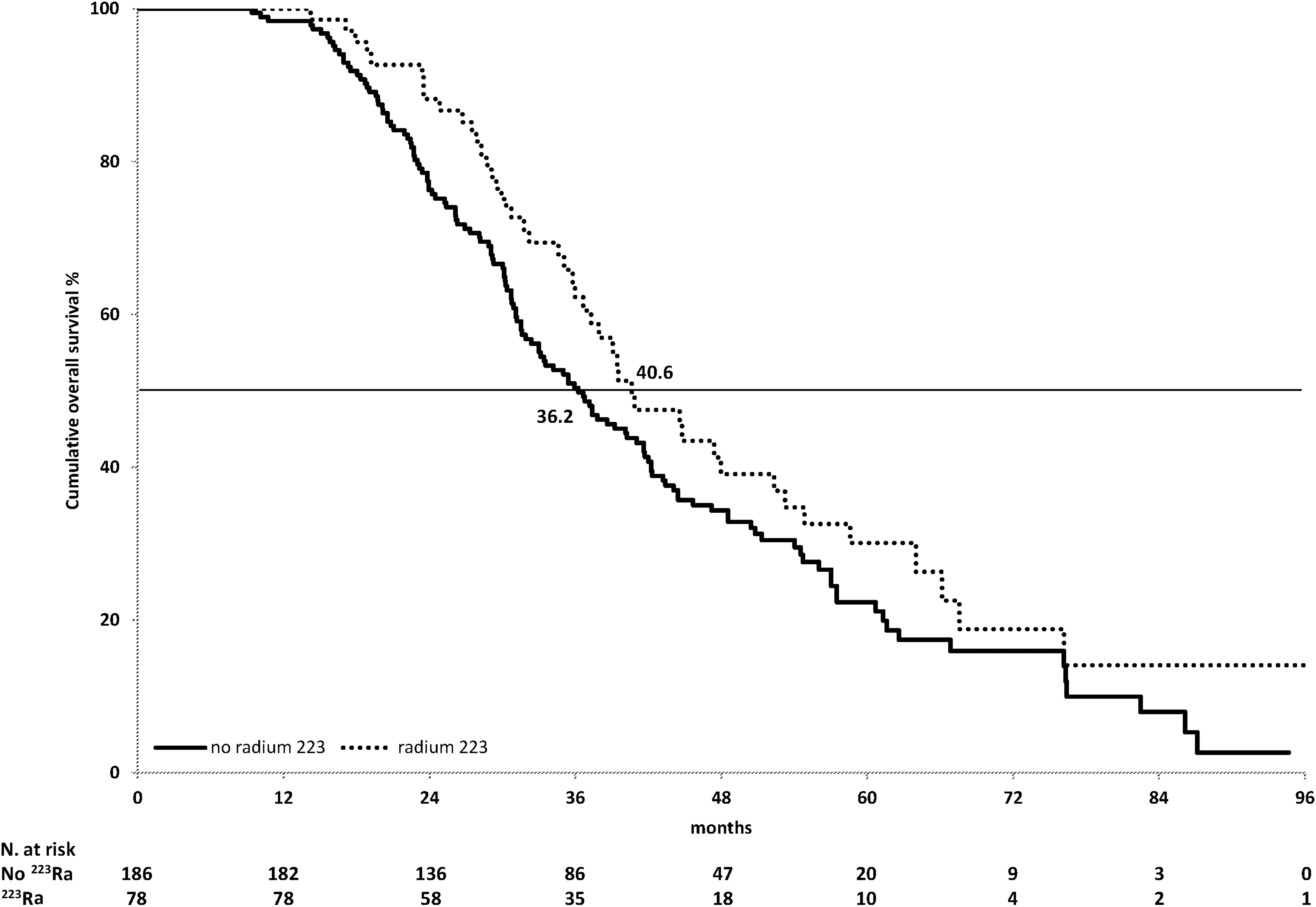
Overall survival from the start of first-line treatment sequences with and without 223Ra. 223Ra, radium 223.
Univariate and Cox Proportional Hazard Analyses of Overall Survival from the Start of First-Line Docetaxel Treatment by Variable of Interest
Reference value.
CI, confidence interval; HR, hazard ratio; OS, overall survival; PS, performance status; PSA, prostate-specific antigen.
Discussion
To the best of our knowledge, this is the first study designed to evaluate the impact of introducing 223Ra into the treatment sequence of mCRPC patients by comparing two cohorts of patients who received sequences with or without 223Ra, and the results suggest that its use does not negatively affect cumulative OS.
Given the availability of five agents capable of prolonging the survival of mCRPC patients in everyday clinical practice, 1 –7 the main challenge facing clinicians is to optimize their sequential use to obtain the longest cumulative survival. Previously published studies of the sequential treatment of mCRPC have evaluated the use of DOC, CABA, AA, and ENZ in every possible order, 11 but none of them considered sequences including 223Ra.
223Ra is an α-emitting radiopharmaceutical with little hematological toxicity because of its low tissue penetration. 13 This specific mechanism of action may be valuable because of the postulated cross-resistance of the other LPAs, all of which directly or indirectly affect androgen receptor machinery, 14 –16 and so the previous administration of one could therefore affect the activity of another. 17 The α-mediated anticancer activity of 223Ra does not interfere with the androgen receptor pathway and could theoretically have the advantage of avoiding cross-resistance with the other LPAs.
The phase III, randomized ALSYMPCA trial compared the effects of 223Ra with those of placebo in symptomatic patients with bone involvement alone (although the presence of lymphadenopathies of up to 3 cm was allowed) who had been previously treated with DOC or were unfit for (or refused) DOC treatment. 7 The results favored the experimental treatment, which led to a statistically significant improvement in OS of 3.6 months; this survival advantage was observed in both chemo-naive and DOC-pretreated patients. 18
The recently published results of the ERA trial, which compared the use of AA plus prednisone plus 223Ra or AA plus prednisone plus placebo in treatment-naive mCRPC patients, found that 29% of the patients in the experimental arm experienced fractures as against 11% in the standard arm, thus leading to a detrimental impact on the patients' OS. 19 On the basis of these findings, the Pharmacovigilance Risk Assessment Committee (PRAC) of the European Medicines Agency (EMA) restricted the use of 223Ra to patients who have received two previous mCRPC treatments, or who cannot receive other treatments. Furthermore, the use of 223Ra was not recommended in patients with a small number of osteoblastic bone metastases. As the present article describes the use of 223Ra in everyday clinical practice before the PRAC pronouncement, the results are valuable in defining the potential effect of 223Ra on OS. Before the recommendation, which was published in July 2018, the use of 223Ra was considered appropriate in symptomatic patients with bone metastases alone, regardless of the number of metastases over the minimum of two. The findings of the observational study, in which 223Ra was administered on the basis of these rules, showed a nonsignificant cumulative OS trend in favor of 223Ra-based sequences.
A number of recently published real-world studies have described large series of patients treated with 223Ra: they confirmed that the use of 223Ra in therapeutic sequencing of mCRPC patients is active regardless of the treatment line, in which it was administered. 20 –23
In particular, Rizzini et al. 21 provided a full description of 223Ra treatment in a cohort of patients who received the radiopharmaceutical in different treatment lines and detailed the changes occurring during its administration. The data concerning the changes in PSA and alkaline phosphatase levels during 223Ra administration are very useful for assessing the clinical benefit of the treatment. Furthermore, the authors evaluated OS from the start of 223Ra administration and found that the difference in OS between the different 223Ra lines was significant only between the third line and fourth lines. The authors' study did not assess OS from 223Ra start, but evaluated the cumulative OS associated with the different treatment sequences from the start of first-line therapy. As there were no statistically significant differences in cumulative OS between the cohorts of patients treated with or without 223Ra, the findings indirectly suggest that the addition of 223Ra does not negatively affect cumulative OS.
The findings of the study indicate that larger number of treatment lines leads to longer cumulative sequence survival, a correlation that retained its statistical significance when it was added to the multivariate analysis. However, this is not surprising because longer survival allows patients to receive more treatment lines. The authors' study has a number of limitations. First of all, the retrospective nature of the data may have affected their validity; however, the main target of the analysis was OS, which is still the most reliable measure of clinical outcome.
Second, the comparison with a contemporary series of patients treated with three or four LPA treatment lines other than 223Ra after having started with DOC may not reflect current everyday clinical practice. In fact, the new hormonal agents, enzalutamide and abiraterone, are now frequently used as first-line treatment. However, as the primary endpoint was cumulative OS, the selection of patients who had received the same first-line treatment clearly allowed us to avoid a potential bias. It would be of course interesting to replicate the study by comparing patients who have received abiraterone or enzalutamide as first-line treatment, but, given the mechanism of action of 223Ra, the authors do not think that its activity would be affected by the type of previous administered agents. They therefore believe that the current findings could support the use of 223Ra in treatment sequence also for mCRPC patients who have not received first-line DOC.
Finally, the authors did not collect data concerning parameters that are known to influence the efficacy and outcomes of 223Ra treatment, such as pain or PSA and alkaline phosphatase levels. However, the study was not intended to evaluate the pros and cons of 223Ra treatment per se, but its potential contribution as another agent to add to those that are already used in the treatment sequences proposed to mCRPC patients. Furthermore, as such parameters can significantly vary at the beginning of each treatment line, they concentrated on some variables known to predict OS in mCRPC patients at the start of the therapeutic sequence and evaluated their impact on cumulative OS.
The indications for 223Ra, that have been modified since the PRAC's pronouncement because of the unfavorable outcomes observed in patients treated with an unapproved combination, have prompted wide-ranging debate in the medical community. 24 The collection of real-world data may therefore not only lead to interesting suggestions for everyday clinical practice, 25 but may also make a valuable contribution to this ongoing debate.
Conclusions
Despite its methodological limitations, the results of this study of patients who sequentially received three or four LPAs (including 223Ra) offer valuable insights into the role of 223Ra in the therapeutic algorithm of mCRPC patients and indicate that it does not negatively affect cumulative OS.
Footnotes
Authors' Confirmation Statement
Conceptualization: O.C.; Methodology: O.C.; Investigation: O.C., V.F., F.M., L.G., R.P.C., C.P., M.T., S.B., G.F., R.B., F.A., P.A., D.D., S.F., A.S., A.M., C.M., C.Z., S.P., E.B., M.S., M.S., U.D.G., G.L.R., E.C., and G.D.V.; Formal analysis: O.C.; Writing-Original draft preparation: O.C.; Writing, Reviewing, and Editing; O.C., V.F., F.M., L.G., R.P.C., C.P., M.T., S.B., G.F., R.B., F.A., P.A., D.D., S.F., A.S., A.M., C.M., C.Z., S.P., E.B., M.S., M.S., U.D.G., G.L.R., E.C., and G.D.V.; O.C. hereby certifies that all coauthors have reviewed and approved of the article before submission.
Disclosure Statement
O.C. received honoraria as advisor and speaker for Astellas, Astra Zeneca, Bayer, Janssen, Pfizer, Sanofi. S.B. received honoraria as advisor and speaker for Bayer, Sanofi. F.M. received honoraria as advisor and speaker for Bayer. M.T. received honoraria as speaker for Astellas, Bayer, Janssen, Sanofi. S.F. received honoraria by Bayer; Blue Earth Diagnostics; Sanofi—Research Funding from Blue Earth Diagnostics—Travel, Accommodations, Expenses from Bayer; Blue Earth Diagnostics; Sanofi. F.A. received Honoraria as speaker for Bayer. D.G. received honoraria as consultant or advisor for Astellas Pharma; Bayer; Bristol-Myers Squibb; Ipsen; Janssen; Merck; Pfizer; Sanofi—Research Funding—AstraZeneca (Inst); Roche (Inst); Sanofi (Inst)—Travel, Accommodations, Expenses—Bristol-Myers Squibb; Ipsen; Janssen; Pfizer. The other authors have no disclosures to be declared.
Funding Information
No funding was received.